

Abstract
Hydatid disease remains endemic in some parts of the world. Cardiac hydatidosis with multivisceral involvement is uncommon but potentially fatal. We report the case of a 36-year-old Tunisian woman admitted with chest pain and T-wave inversion in the inferior leads on her electrocardiogram. Transthoracic echocardiography revealed a large hydatid cyst in the epicardium throughout the left ventricle. Thoraco-abdominal computerized tomography (CT) scan showed several hydatid cysts in the left lung, the liver, and in both breasts.
After one week of albendazole treatment, surgical excision of the cardiac cyst on cardiopulmonary bypass was carried out as well as excision of the pulmonary and breast cysts. The postoperative course was uneventful and albendazole treatment was continued for six months. Though hydatid cardiac involvement is very rare, it should be considered in the differential diagnosis of atypical chest pain in young patients, especially those living in regions where hydatid disease is endemic.
Keywords: Hydatid disease, Cardiac hydatid cyst, Chest pain
Introduction
Hydatid disease is a parasitic infection caused by Echinococcus granulosus. It remains endemic in regions such as the Mediterranean, the Middle East, South Africa, America, and Australia. It affects various organs; the most common ones being the liver and lungs [1]. Multivisceral echinococcus with cardiac involvement is exceptional [2]. Cardiac location is an uncommon presentation of hydatid disease and constitutes 0.5–2% of different hydatid disease locations. The most affected areas of cardiac involvement are the left ventricle (60–70%) and right ventricle (10%), while interventricular septum, pericardium, and atria are the least affected [3]. Approximately 10% of patients with cardiac hydatid cysts are symptomatic [4]. Clinical presentation is polymorphic with nonspecific symptoms such as atypical chest pain. Cardiac cysts can rupture and cause anaphylactic reaction, systemic or pulmonary embolization, or pericardial tamponade [4]. We report the case of a young woman with multivisceral hydatidosis revealed by a giant cardiac hydatid cyst treated surgically with success.
Case presentation
A 36-year-old woman with a history of prolonged close proximity to dogs and sheep, reported atypical chest pain and a lack of appetite over three months. Physical examination was unremarkable with normal heart sounds and a normal pulmonary auscultation. Laboratory tests were normal. Her electrocardiogram showed sinus rhythm with negative T-waves in the inferior leads (DII, DIII and aVF). However, trans-thoracic echocardiography (TTE) showed a giant rounded cystic mass with echo-negative contents close to the posterior mitral valve covering the half of the posterior left ventricular wall and measuring 50 × 48 mm without hemodynamic consequences (Fig. 1). Coronary angiography was normal (normal coronary arteries origin, course, and termination). A thoraco-abdominal CT scan revealed a large cystic homogeneous mass related to the atrio-ventricular groove, extending to the left cardiac chambers and measuring 50 × 40 mm, a left pulmonary cyst measuring 15 × 12 mm, two bilateral breast cysts, and a right hepatic cyst (Fig. 2). Mammography confirmed the presence of well-defined right and left heterogeneous cysts with partially calcified edges (Fig. 3). Brain scan was normal. Serological tests performed with enzyme-linked immunosorbent assay (ELISA) were positive for E. granulosus. Ultimately, we retained a diagnosis of multivisceral hydatidosis with cardiac location. After one week of albendazole treatment, uncomplicated excision of the cardiac cyst was performed under cardiopulmonary bypass surgery. Myocardial protection was achieved through intermittent anterograde warm blood cardioplegia. The epicardial cyst was approached directly from the bottom of the heart without opening any cardiac chambers. The cyst was isolated by sponges soaked with hypertonic saline serum in order to prevent local invasion by the parasite. The germinative membrane of the hydatid cyst was completely ablated and cyst contents were totally aspirated. Hypertonic saline solution was injected into the residual cavity to kill any viable daughter vesicles. A capitonnage of the cavity wall was then made by U-shaped interrupted sutures (Fig. 4). Finally, an excision and a capitonnage of the left pulmonary cyst as well as an excision of the right and left breast hydatid cysts were performed. A histopathological exam of the resected tissues was positive for scolices of E. granulosus. Control TTE showed a residual cavity of 2 cm2 (Fig. 5). The postoperative course was uneventful and medical treatment with albendazole was continued over a period of six months.
Figure 1a.

Trans-thoracic echocardiography showing a large cardiac cyst, covering half of the posterior left ventricular wall.
Figure 1b.

Transthoracic echocardiography showing a giant rounded cystic mass measuring 50 × 48 mm on the posterior left ventricular wall.
Figure 2a.

Thoracoabdominal CT scan showing a large epicardial cystic mass (50 × 40 mm) close to the posterior left ventricular wall with partially calcified edges.
Figure 2b.
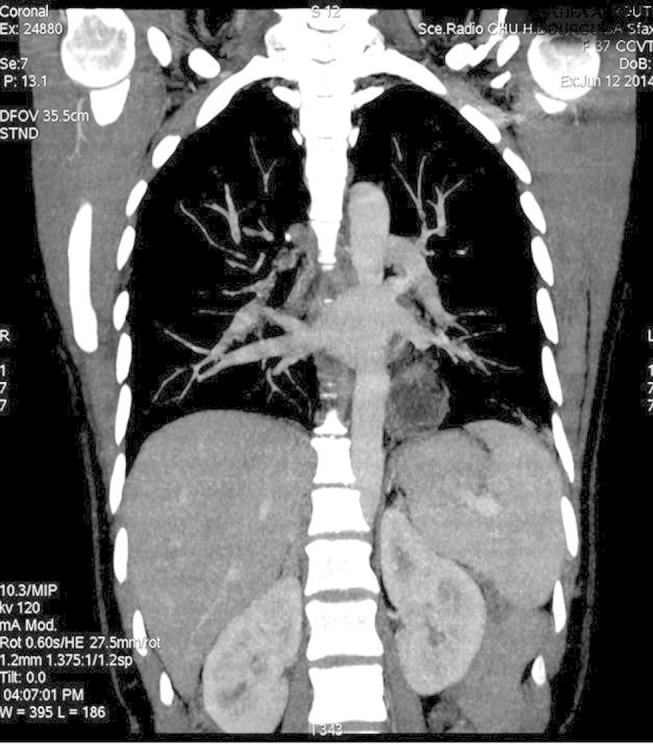
Thoracoabdominal CT scan showing a heterogeneous cyst in the left lung.
Figure 2c.

Thoracoabdominal CT scan showing well-defined cysts in the right liver and the left ventricle.
Figure 3.

Mammography showing bilateral well-defined heterogeneous cysts with partially calcified edges in both breasts.
Figure 4.


Surgical treatment of the cardiac hydatid cyst: a–e. (a) Peroperative view showing a huge epicardial hydatid cyst covering the posterior left ventricular wall. (b) Total ablation of the germinative membrane of the hydatid cyst. (c) Uncompleted excision of the hydatid cyst showing the residual cavity. (d) Capitonnage of the cavity wall made by U-shaped interrupted sutures. (e) The germinative membrane and the content of the cardiac hydatid cyst.
Figure 5.

Control trans-thoracic echocardiography showing the residual cavity (a and b).
Discussion
Hydatid disease, commonly known as echinococcus or hydatidosis, remains endemic in some areas of the world. This parasitic disease is a significant public health problem in these countries. It is a tissue infestation frequently caused by the larva of E. granulosus [4]. Humans are accidental hosts in the cycle of E. granulosus and are infected by handling dogs or ingesting cyst-containing meat from an intermediate host [2]. The most common localizations of hydatid cysts are the liver (in 50–70% of cases) and lungs (in 5–30% of cases). But other parts of the body can also be affected [1]. Multivisceral hydatidosis inside thoracic and abdominal compartments with cardiac hydatid cyst as first presentation is exceptional [2]. A literature review did not reveal reports of multivisceral hydatidosis involving liver, lung, both breasts, or heart with chest pain as a revealing symptom. In our case, this was diagnosed using imaging techniques. Cardiac involvement is an uncommon presentation of hydatid cyst disease, accounting for approximately 0.5–2% of all hydatidosis cases, and mainly occurring as part of a systemic infection [3]. Areas of cardiac involvement in hydatid disease include the left ventricle (60% of cases), the right ventricle (10%), the pericardium (7%), the pulmonary artery (6%), the left atrial appendage (6%), and the interventricular septum (4%) [3]. Echinococcus larvae necessarily get through two filters (liver and lung) and then reach the heart mainly through the coronary circulation [4,5]. The second route of infestation is the pulmonary vein due to the rupture of pulmonary echinococcal cysts in the vein. The heart can also be secondarily affected by direct contact with hydatid cysts originating from the liver or the lungs [5]. The left ventricle is the most frequently involved site of cardiac hydatid cysts due to the rich coronary blood supply and the good perfusion of the left ventricular myocardial mass [4,5]. Cardiac cysts grow toward the weaker side of the ventricular wall; either the epicardium or endocardium [6]. Clinical manifestations vary according to the cyst site, size, and number and are due to related complications. Symptoms are mostly nonspecific and include atypical chest pain, breath shortness, asthenia, and palpitations. Left ventricular hydatid cysts are usually located subepicardially and may compress the small coronary arteries. Hence, chest pain can be the symptom revealing hydatid cysts and mimicking the coronary artery disease [7]. Cardiac hydatid cysts may result in serious consequences such as rupture into the pericardial cavity or the cardiac chambers. Rupture into the pericardial cavity is a rare complication of the subepicardial hydatid cysts. It may be silent or cause an acute tamponade, constrictive pericarditis, or pericardial cysts. Rupture of subendocardial cysts into the circulation can cause anaphylactic reaction and may be fatal [6]. The diagnosis of a subepicardial hydatid cyst revealed through chest pain was made in our case. However, there were no complications, and the angiography did not reveal compression of the coronary arteries.
Various serological tests are available for the diagnosis and postoperative follow-up of hydatid cyst recurrence, such as immunoelectrophoresis, ELISA, latex agglutination, and the indirect hemagglutination (IHA) test [8]. However, previous reports have shown that serologic tests can have false-negative results, and therefore imaging modalities such as ultrasonography, CT scan, and magnetic resonance imaging (MRI) have been the methods of choice [9]. For cardiac involvement, TTE is the exam of choice thanks to its availability, high sensitivity, good resolution, and the ability to detect hemodynamic repercussion. CT scan and MRI can help localize the lesion, and detect multiple lesions and multi-organ involvement [5]. In our case, the diagnosis of cardiac hydatid cyst was made by TTE and ELISA tests which were positive for hydatid disease. Other multiple lesions including lung, bilateral breast and liver involvement were detected by CT scan.
Due to their localization in the myocardium or pericardium and the risk of life-threatening complications, hydatid cardiac cysts should be operated on as soon as diagnosis is made [10]. Surgical treatment depends on the size, location, and number of the cysts. The main principle of surgical treatment is to empty the cyst, remove daughter cysts and the germinative membrane, excise the pericyst, and then obliterate the residual cavity with sutures (capitonnage). The use of local scolicidal solution such as hypertonic saline solution is obligatory after cysto-pericystectomy in order to minimize the risk of dispersion of cystic content [10]. Supplemental medical therapy with albendazole is recommended, which has better results in preventing recurrence of hydatid disease. The duration of anti-parasitic postoperative treatment depends on intra-operative findings and the presence of complications.
Conclusion
Multivisceral hydatidosis with cardiac involvement is an uncommon entity and has nonspecific clinical presentation. Chest pain may be a revealing symptom. Diagnosis of hydatid disease of the heart depends on a series of tests including hydatid serology, echocardiography, MRI, and CT scan. Cardiac hydatidosis should be considered in the differential diagnosis of tumoral and cystic masses. The treatment of choice is surgical excision, even in asymptomatic patients.
Disclosure: Authors have nothing to disclose with regard to commercial support.
Footnotes
Peer review under responsibility of King Saud University.
References
- 1.Kireşi D.A., Karabacakoğlu A., Odev K., Karaköse S. Uncommon locations of hydatid cysts. Acta Radiol. 2003;44(6):622–636. doi: 10.1080/02841850312331287749. [DOI] [PubMed] [Google Scholar]
- 2.Grozavu C., Ilias M., Pantile D. Multivisceral echinococcosis: concept, diagnosis, management. Chirurgia (Bucur) 2014;109(6):758–768. [PubMed] [Google Scholar]
- 3.Ulgen M.S., Alan S., Karadede A., Aydinalp O., Toprak N. Cardiac hydatid cysts located in both the left ventricular apex and the intraventricular septum: case report. Heart Vessels. 2000;15(5):243–244. doi: 10.1007/pl00007271. [DOI] [PubMed] [Google Scholar]
- 4.Ipek G., Omeroglu S.N., Goksedef D., Balkanay O.O., Kanbur E., Engin E. Large cardiac hydatid cyst in the interventricular septum. Tex Heart Inst J. 2011;38(6):719–722. [PMC free article] [PubMed] [Google Scholar]
- 5.Younis S.N., Faraj A.A. Cardiac hydatid disease, case report, and review of literature. Acta Clin Belg. 2014;69(1):66–68. doi: 10.1179/0001551213Z.0000000003. [DOI] [PubMed] [Google Scholar]
- 6.Tuncer E., Tas S.G., Mataraci I., Tuncer A., Donmez A.A., Aksut M. Surgical treatment of cardiac hydatid disease in 13 patients. Tex Heart Inst J. 2010;37(2):189–193. [PMC free article] [PubMed] [Google Scholar]
- 7.Gocen U., Atalay A., Basturk Y., Topcuoglu M.S., Yaliniz H., Salih O.K. Urgent surgery for cardiac hydatid cyst located in interventricular septum. Asian Cardiovasc Thorac Ann. 2014;22(8):965–967. doi: 10.1177/0218492313489562. [DOI] [PubMed] [Google Scholar]
- 8.Abu-Eshy S.A. Some rare presentations of hydatid cyst (Echinococcus granulosus) J R Coll Surg Edinb. 1998;43(5):347–352. [PubMed] [Google Scholar]
- 9.Dahniya M.H., Hanna R.M., Ashebu S., Muhtaseb S.A., El-Beltagi A., Badr S. The imaging appearances of hydatid disease at some unusual sites. Br J Radiol. 2001;74(879):283–289. doi: 10.1259/bjr.74.879.740283. [DOI] [PubMed] [Google Scholar]
- 10.Salih O.K., Celik S.K., Topcuoğlu M.S., Kisacikoğlu B., Tokcan A. Surgical treatment of hydatid cysts of the heart: a report of 3 cases and a review of the literature. Can J Surg. 1998;41(4):321–327. [PMC free article] [PubMed] [Google Scholar]