

Abstract
Depression is associated with social dysfunction and maladaptive social environments, but mechanisms through which social relationships affect depressive psychopathology are unclear. We hypothesized that emotion regulation (ER) is such a mechanism, with outcomes of individuals’ ER efforts sensitive to the social context, and individuals’ ER strategy repertoire and use sensitive to social influence. In Study 1, a longitudinal study of community adults (N = 1,319), associations of individuals’ ER strategies with depressive symptoms depended on social connectedness and romantic relationship status (social context hypothesis). Moreover, associations of social connectedness and relationship status with symptoms were accounted for by maladaptive ER concurrently and, for social connectedness, prospectively over 1 year (social influence hypothesis). Study 2a, using a national sample (N = 772), replicated and extended these findings with a broader array of ER strategies, and ruled out alternative explanations regarding social skills and psychological wellbeing. Among participants in romantic relationships (Study 2b; N = 558), intimacy and trust buffered associations of maladaptive ER strategies with symptoms (context), and maladaptive and adaptive ER mediated links between relationship variables and symptoms (influence). Findings suggest that close relationships—and variation in underlying relational processes within relationships— influence the ER strategies people use, and also affect whether individuals’ own ER repertoires contribute to depression when deployed. Results elucidate core social mechanisms of ER in terms of both basic processes and depressive psychopathology, suggest ER is a channel through which social factors affect internal functioning and mental health, and inform relationship pathways for clinical intervention.
Keywords: depression, emotion, emotion regulation, interpersonal processes, close relationships
Major depressive disorder is among the most prevalent mental disorders, with disruptions across cognitive, behavioral, and somatic domains that result in marked suffering, impairment, and cost (Kessler et al., 2005). In recent years, behavioral approaches (e.g., Lewinsohn, 1975) and cognitive approaches (e.g., Beck, 1967) to the etiology and treatment of depression have been augmented by an emphasis on emotion and emotion regulation. A dramatic increase in basic emotion research (Kring & Sloan, 2010) indicates that depression is characterized not only by its characteristic emotion disturbance (e.g., high negative and low positive affect), but also by deficits in the ability to regulate emotion adaptively in response to distress (Aldao, Nolen-Hoeksema, & Schweizer, 2010).
Mirroring basic research on emotion regulation, research on emotion dysregulation in psychopathology has focused squarely on intrapersonal processes. At the same time, however, the social environment—and close relationships in particular—plays a key role in physical and mental health, including depression (Cohen, 2004; Lakey & Cronin, 2008; Uchino, Cacioppo, & Kiecolt-Glaser, 1996). Social isolation, smaller social networks, and low perceived social support are all associated with depression (Cacioppo, Hughes, Waite, Hawkley, & Thisted, 2006; Lakey & Cronin, 2008). Moreover, depressed individuals interact with their social environments in patterns that feed depression, through complex dynamics linking individual pathology to the social context (e.g., stress generation, Hammen, 1991; excessive reassurance-seeking, Joiner, Metalsky, Katz, & Beach, 1999; negative feedback-seeking, Swann, Wenzlaff, Krull, & Pelham, 1992).
However, the mechanisms through which relationships influence individual physical and mental health are poorly understood (Cacioppo & Hawkley, 2003). With respect to depression and other psychopathology, social influences on individual emotion regulation (ER) may represent such a mechanism (Marroquín, 2011). Emotion dysregulation plays a central role in depression, and increasingly, there are reasons to believe that the cognitive and affective mechanisms that underlie ER are susceptible to social influences in adulthood (Rimé, 2009). If so, ER may be one important route through which social relationships affect intrapersonal processes, in both healthy and depressed individuals. The primary goal of the present studies was to elucidate the role of social factors in emotion regulation and dysregulation, with depressive symptoms as a relevant mental health outcome. We sought to examine how social relationships, and romantic relationships in particular, operate as both social contexts in which individuals deploy their own ER strategies when coping with distress, and social influences on how individuals regulate emotion (i.e., their ER strategy repertoire and use).
Emotion Regulation in Depression
Thompson (1994) defined emotion regulation as the “extrinsic or intrinsic processes responsible for monitoring, evaluating, and modifying emotional reactions, especially their intensive and temporal features, to accomplish one’s goals” (pp. 27–28). ER involves responding to internal and external stimuli in a more or less strategic way, to maintain adaptive, goal-oriented functioning given situational demands (Gross, 1998). Individual differences in use of ER strategies have cognitive, emotional, and social consequences in both healthy and disordered populations, and chronic use of maladaptive ER can strongly influence distress and symptomatology (Gross & John, 2003; Nolen-Hoeksema, Wisco, & Lyubomirsky, 2008).
Indeed, emotion dysregulation has been implicated as a transdiagnostic factor in mental health, and in depression specifically (Aldao et al., 2010; Kring & Sloan, 2010). Depressive symptoms are associated with higher use of maladaptive ER strategies such as rumination and expressive suppression, and lower use of adaptive ER such as cognitive reappraisal and acceptance (e.g., Campbell-Sills, Barlow, Brown, and Hofman, 2006; Ehring, Fischer, Schnülle, Bösterling, & Tuschen-Caffier, 2008; Nolen-Hoeksema et al., 2008; see Aldao et al., 2010 for a comprehensive review). Depressive emotion dysregulation appears throughout the cognitive phases of ER, including biased attentional deployment toward negative material, maintenance of such material in memory, biased interpretation of ambiguous stimuli, and elaboration of negative content through repetitive processing and impaired cognitive control (Gotlib & Joormann, 2010).
Social Influences on Emotion Regulation
Clinical science on psychopathology and treatment has benefitted from the rise in basic research on how individuals regulate emotions (Kring & Sloan, 2010). To date, however, basic work on the social context of ER in adulthood has emphasized the influences of intrapersonal ER on social outcomes, rather than influences of social factors on individual ER (e.g., Butler et al., 2003; Richards, Butler, & Gross, 2003). Cross-sectional associations of ER and social functioning are consistent with both causal directions (Bell & Calkins, 2000; Graham, Huang, Clark, & Helgeson, 2008; Srivastava, Tamir, McDonigal, John, & Gross, 2009), and there are several reasons to suspect that individual ER is susceptible to social influences. Most notably, a large body of work on typical and atypical development indicates that the social environment plays a fundamental role in ER during childhood. Parents and family members influence attentional deployment and cognitive control in both adaptive or maladaptive ways across development (see Eisenberg, Spinrad, & Eggum, 2010, for a review). As Rimé (2009) argued, it is highly unlikely that basic mechanisms of ER are so dependent on social influences throughout development and then cease to incorporate interpersonal input in adulthood.
Theoretical and empirical approaches to basic processes in adult ER, and self-regulation more generally, have begun to incorporate the social context (for recent theoretical perspectives, see Butler & Randall, 2013; Fitzsimons & Finkel, 2010, 2011; Zaki & Williams, 2013), emphasizing the complex ways in which two individuals can affect each other’s emotional experience. Adults’ sharing of negative emotion with others serves both affiliative and regulatory functions, including amelioration of stress in the short term (Lepore, Fernandez-Berrocal, Ragan, & Ramos, 2004; Lepore, Ragan, & Jones, 2000; Rimé, 2009), and sharing positive emotion with others can help individuals capitalize on the benefits of positive events (Gable & Reis, 2010). Cognitive reframing by social supporters during support interactions reduces distress (Lepore et al., 2004) and promotes effective coping in response to stress (Holtzman, Newth, & DeLongis, 2004), in ways consistent with interpersonal ER. Indeed, just holding hands with another person attenuates affective reactions to negative stimuli, whether the other is a stranger (Flores & Berenbaum, 2012) or a relationship partner (Coan, Schaefer, & Davidson, 2006).
Together, such findings suggest an important role of social resources in emotion regulation and, potentially, dysregulation. From the perspective of psychopathology, we have previously argued (CITATION MASKED) that a primary benefit of interpersonal ER in adult relationships is that one’s close relationship partners act as “external drives” offering both different sets of ER strategies to supplement the intrapersonal repertoire (i.e., “software”) and additional processing capabilities to supplement implementation (i.e., “hardware”). Such regulatory contributions from others may counter the deficits associated with psychopathology, and contribute to the regulatory flexibility that characterizes healthy ER (Kashdan & Rottenberg, 2010). Indeed, the mere availability of social resources may be a precondition for neurocognitive substrates of self-regulation and ER (Beckes & Coan, 2011).
Here, we use the term “social emotion regulation” to refer to the general concept of an individual as situated in a social world in the broader sense (e.g., within a group or society) as well as in specific social relationships (e.g., romantic partners, family members, friends) that are relevant to his or her intrapersonal emotional and regulatory functioning. We reserve the use of the term “interpersonal emotion regulation” to more precisely describe dyadic or transactional instances in which one individual has a direct effect on another’s emotional state (see Dixon-Gordon, Bernecker, & Christensen, 2015; Marroquín, 2011; Zaki & Williams, 2013), which depending on the definition used, may include unintentional coregulation of emotion between partners (Butler & Randall, 2013), emotional contagion (Hatfield, Cacioppo, & Rapson, 1993), and use of emotion as social information (Van Kleef, 2010). Herein, we focus on social ER, regarding interpersonal ER as a critical subcategory.
The Role of Relationship Factors
Close relationships are a particularly likely context in which social and interpersonal ER exist and, in turn, affect depression. Characteristics of support providers, support recipients, and their unique relationship are key determinants of social support outcomes (Frazier, Tix, & Barnett, 2003; Iida, Seidman, Shrout, Fujita, & Bolger, 2008; Lakey & Scoboria, 2005; Lakey, Orehek, Hain, & VanVleet, 2010). Whether social support leads to beneficial, maladaptive, or benign outcomes—including effects of support on cognition and affect—depends largely on relational features (Lakey & Tanner, 2013; see Lakey & Orehek, 2011, for a review). In different emotional states, people turn to different supporters (Cheung, Gardner, & Anderson, 2015), and evidence that hand-holding attenuates responses to negative stimuli also shows that effects are stronger depending on closeness of the other (spouse versus stranger; Coan et al., 2006), marital quality between spouses (Coan et al., 2006), and the individual’s own desire for closeness (Flores & Berenbaum, 2012).
Although intimate relationships have a positive effect on mental health on average (Dush & Amato, 2005; Kim & McKenry, 2002), variation in relational characteristics relevant to social support appears in both healthy and depressed populations (Lakey, 2010; Lakey, Drew, & Sirl, 1999). In clinical and nonclinical samples, depression and couple discord are highly comorbid and have bidirectional influences over time (for reviews, see Rehman, Gollan, & Mortimer, 2008; Whisman & Baucom, 2012). Moreover, recent approaches to treating individual depression in a couple therapy format show comparable efficacy to individual treatment, as well as stronger effects on relationship discord – an important additional benefit, because discord predicts lower treatment effectiveness and higher post-treatment relapse (Barbato & D’Avanzo, 2008; Baucom, Whisman, & Paprocki, 2012). As yet, however, mechanisms through which relationships affect the psychopathology of depression remain unclear.
Contexts and Mechanisms of Social Emotion Regulation in Depression
How do people in the social environment influence a system organized around regulating internal affective states? We investigate two ways in which social relationships may play a role in ER and, in turn, depression. The first, which we call the social context hypothesis, is that the social world forms an environmental context in which individuals regulate emotions—a context that can either water down or amplify the effects of individuals’ own ER strategies. Thus, relationships act as moderators of links between individual ER and depressive symptoms. The second route, which we call the social influence hypothesis, is that people affect each other’s use of ER strategies. In this latter view (a mediational hypothesis), relationship partners and the social world act not just as an environmental context in which individual ER plays out, but rather directly influence individual ER repertoire and use and, in turn, depressive symptoms.
These two potential influences of social relationships are not mutually exclusive. The distinction between context and influence at the social level maps on to the distinction between ER strategy effectiveness and use at the intrapersonal level. Regarding social context, relationship partners can represent an enriched environment of social support and ER resources that buffer the effects of intrapersonal ER alone. In this account, the availability of external sources of ER (e.g., being surrounded by different strategy repertoires and cognitive capabilities) can dilute the harmful processes characteristic of depressive ER at the individual level. For example, having a daily date to go walking with a supportive friend can provide a socio-environmental buffer against the deleterious effects of an individuals’ own tendency to ruminate. Even if the individual persists in ruminating during and after the walk, the depressogenic effects of this rumination may be diluted by the countervailing effects of the social context (e.g., being forced to leave the house, the friend’s positive affect, the social demand to respond to her questions and statements, her own refusal to engage in ruminative conversation). This friend may or may not affect the individual’s tendency to ruminate, but rather by virtue of her unique characteristics, or merely her presence, forms a social condition that contextually affects the outcome of intrapersonal strategies.
Regarding direct social influence, the content of supportive interactions can include direct intervention on ER that influences precisely the underlying ER difficulties of depression, intentionally or unintentionally. For example, a close other might counter the attentional patterns of depressive ER by encouraging attentional redeployment toward positive stimuli (e.g., “Let’s watch a comedy tonight”). Or a partner’s contribution during supportive interactions can counter the individual’s biases in event interpretation (e.g., “It sounds like your boss appreciated your presentation, even if you thought it went poorly”). Many of the common behaviors of social support—as well as formal techniques in psychotherapy—can be viewed as influencing emotion dysregulation (Marroquín, 2011).
Of course, the social world can exert influences on depression, and likely ER, for better or worse (e.g. Joiner et al., 1999). For example, a partner’s direct influence on ER may be more harmful than helpful when he or she has tendencies to ruminate or is also depressed. Moreover, between any two individuals, interpersonal ER is likely to rely on relational processes (e.g., intimacy and trust) that draw on intrapersonal mechanisms of affect and cognition, vary among relationships, and change within relationships over time. In terms of our “external drive” metaphor for interpersonal ER, in which partners supplement individuals’ systems with different ER repertoires and processing capabilities, such relational factors may serve as “connecting cables” of varying strength, linking external resources to internal processes with more or less efficiency, quality, and power (e.g., high intimacy as a relational condition maximizing the magnitude of interpersonal ER effects within a couple).
The Present Studies
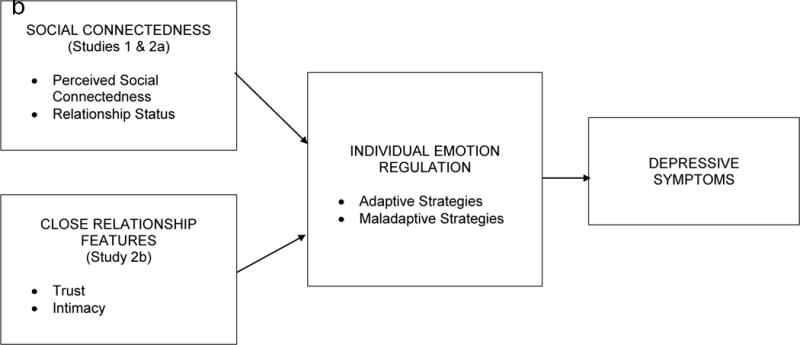
The present studies sought to examine emotion regulation as a route through which social relationships play a role in depression. In three studies with two large samples, we focused on three potential sources of social influence: 1) overall social connectedness; 2) intimate relationship status; and 3) trust and intimacy as varying characteristics within intimate relationships. We tested both the context hypothesis and the influence hypothesis of social ER. Schematics of these models are presented in Figure 1. Analytically, the context hypothesis is a moderator model, in which we predicted that effects of individuals’ own ER strategies on depressive symptoms depend on aspects of social relationships. The influence hypothesis is a mediational model, in which we predicted that effects of social relationships on individual ER would account for their effects on depressive symptoms.
Figure 1.
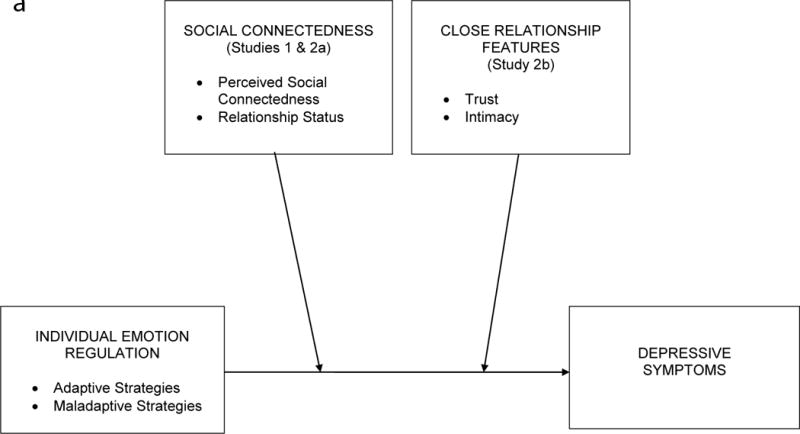
(a) Social Context Hypothesis
(b) Social Influence Hypothesis
Study 1
In Study 1, we first hypothesized an overall benefit of relationships: that individuals embedded in social relationships (i.e., those high in social connectedness, or in an intimate relationship) would endorse less maladaptive ER, more adaptive ER, and fewer depressive symptoms than socially isolated or single individuals. With regard to the context hypothesis, we predicted that individuals’ own ER strategy use would show weaker relations with depressive symptoms among individuals embedded in social relationships, which would suggest that effects of individuals’ strategy use are subject to social effects concurrently and over time. Regarding the influence hypothesis, we hypothesized that relations of social connectedness and relationship status with depressive symptoms, both concurrently and over time, would be attributable to more adaptive and less maladaptive ER.
Method
Participants and Procedure
Participants were recruited through random-digit dialing of telephone numbers in San Francisco, San Jose, and Oakland, California. Of 1,789 individuals who were initially called, 1,319 participated in the first interview, and 1,132 participated in a second interview approximately 1 year later. Trained personnel conducted in-person interviews of approximately 90 minutes, usually at the participant’s home. For each measure, the interviewer read the instructions to the participant aloud; if item responses had multiple options, the interviewer presented a card with response options.
At Time 1, the sample included 625 men (47%) and 694 women (53%) with an average age of 47 years (SD = 15.2, range 24–82). Participants’ self-reported ethno-racial backgrounds were White (70%), Hispanic (9%), African-American (8%), Asian/Pacific Islander (6%), and other/declined to respond (7%). Median income was $40,000–$50,000. Education level completed was high school or less (20%), some college (27%), completed undergraduate degree (26%), some graduate-level education (8%), and graduate degree (20%). Cross-sectional analyses are based on the full Time 1 sample; prospective analyses are based on those individuals who participated in both interviews. Participants who did not participate in the second interview had significantly higher depressive symptoms at Time 1 than those who did participate, p < .05. Due to missing data, sample sizes vary slightly among analyses. For details on methods and sampling, see Nolen-Hoeksema, Larson, & Grayson (1999) and Nolen-Hoeksema (2000).
Measures
Depressive Symptoms
The 13-item Beck Depression Inventory-Short Form (BDI-SF; Beck & Beck, 1972) is a widely-used measure of depression that assesses affective and cognitive symptoms over the past week; scores can range from 0 to 39. Internal consistency was α = .83 at Time 1 and α = .84 at Time 2.
Social Connectedness
The UCLA Loneliness Scale-Revised (Russell, Peplau, & Cutrona, 1980) is a 20-item measure of perceived social isolation (e.g., “There are people I can talk to” and “No one really knows me well”). This measure has strong psychometric properties, including concurrence with time spent alone, fewer social interactions, and fewer close relationships, as well as discriminant validity with respect to measures of personality and depression (Russell et al., 1980). In the present studies, scores were reversed such that higher scores reflect more social connectedness to reflect the theoretical focus on the role of available relationships. Scores had a possible range of 1–81 and good internal consistency at Time 1 (α = .90) and Time 2 (α = .88).
Relationship Status
Participants reported their relationship status at both time points. Relationship status at Time 1 was: 53% married or cohabiting; 18% single/never married; 16% divorced, separated, or single parent; 8% widowed; 4% committed but not cohabiting; 1 declined. Relationship status was considered a dichotomous variable, with married, cohabiting, and committed participants coded as in an intimate relationship (754; 57%) and all others as not in a relationship (564; 43%). Proportions of partnered versus single participants were identical among participants who completed both waves.
Emotion Regulation
To examine individuals’ maladaptive and adaptive ER strategy use, participants completed subscales of the Ruminative Response Scale (RRS; Nolen-Hoeksema & Morrow, 1991), the COPE Inventory-Short Version (Carver, 1997), and additional items measuring suppression. The RRS measures the tendency to respond to distress by focusing passively and repetitively on the causes and consequences of current mood (1 = almost never to 4 = almost always). The present study examined the 5-item brooding subscale (e.g., “Think “What am I doing to deserve this?’”), which does not overlap in content with depressive symptoms (Treynor, Gonzalez, & Nolen-Hoeksema, 2003). Brooding scores were averaged across items, and had good internal consistency at Time 1 (α = .77) and Time 2 (α = .77).
The Brief COPE is a 28-item scale on which participants rated agreement with statements about their how they had coped with stressors over the past year, from 1 (I haven’t been doing this at all) to 4 (I’ve been doing this a lot). We examined the subscales most directly related to ER, as opposed to more general coping strategies. These were behavioral disengagement (e.g., “I’ve been giving up trying to deal with it”), denial (e.g., “I’ve been saying to myself, ‘This problem/situation isn’t real’”), positive reframing (e.g., “I’ve been trying to see things in a different light to make them seem more positive”), active coping (e.g., “I’ve been taking action to try to make the situation better”), and acceptance (e.g., “I’ve been learning to live with the stress”). The COPE has good psychometric properties across a range of populations (Carver, 1997; Carver, Scheier, & Weintraub, 1989). At the time of data collection (1994–1996), there were no well-established measures of suppression as an ER strategy; we thus included 3 additional items measuring emotion and thought suppression (e.g., “I’ve been actively trying to suppress or ignore my emotions about the things that cause me stress”). All scores were averages across constituent items. Internal consistency for individual scales ranged from .51 to .73 at Time 1, and from .60 to .75 at Time 2.
Theoretical and empirical work on coping and ER in healthy functioning and psychopathology has noted that specific intrapersonal ER strategies tend to have adaptive or maladaptive outcomes overall (Aldao et al., 2010; Stanton, Kirk, Cameron, & Danoff-Burg, 2000; Taylor & Stanton, 2007). In a meta-analysis, Aldao et al. (2010) found that specific strategies (avoidance, rumination, and suppression) were reliably positively associated with psychopathology, including depression, whereas others (problem solving and reappraisal) were negatively associated. Importantly, greater use of maladaptive strategies appears to be more problematic for affective psychopathology than lower use of adaptive strategies (Aldao & Nolen-Hoeksema, 2010; Aldao et al., 2010). To reflect this distinction, strategies in the present study were classified as putatively adaptive (positive reframing, active coping, acceptance) or maladaptive (brooding, behavioral disengagement, denial, suppression). Composite variables for maladaptive and adaptive ER were created by standardizing scores on each individual ER variable, and then averaging across constituent scales.
Analytic Approach
Hypotheses regarding descriptive statistics, correlational associations, and group differences were tested first, then the context (moderation) hypothesis, and then the influence (mediation) hypothesis. Within each of these sets of analyses, models were conducted first with perceived social connectedness, and second with intimate relationship status. For all moderation tests revealing a statistically significant interaction, effects were probed by estimating simple slopes at low and high values of the moderator (+/− 1 SD for social connectedness; single versus partnered for relationship status). Mediation models were first tested using hierarchical linear regression to estimate overall effects, and then followed up with bootstrapping mediation analyses indicated for multiple mediator models (Preacher & Hayes, 2008). This analytic approach guided both subsequent studies as well, with relevant changes in variables of interest. In the present study, cross-sectional analyses of moderation and mediation analyses were conducted first with data from Time 1; prospective analyses of moderation and mediation over time were then conducted among participants in both study waves.
Results
Descriptive Statistics
At Time 1, the mean BDI-SF score was 4.56 (SD = 4.29), somewhat above the general population mean of between 2 and 3 (Knight, 1984). Mean social connectedness was 55.68 (SD = 10.98). Because ER composites were standardized, each had a mean of 0 (maladaptive ER SD = 0.68; adaptive ER SD = 0.78). Among participants who participated at both time points, BDI-SF score was 4.45 at Time 1 (SD = 4.14) and 3.96 at Time 2 (SD = 4.08).1
Associations among Study Variables at Time 1
Perceived Social Connectedness
Replicating extant literature, social connectedness was significantly and negatively associated with depressive symptoms (r = −.53, p < .001). Moreover, consistent with our predictions, higher social connectedness was associated with lower maladaptive ER (r = −.36, p < .001) and, to a lesser degree, higher adaptive ER (r = .07, p = .01). Depressive symptoms were positively associated with maladaptive ER (r = .51, p < .001), but were not associated with adaptive ER (r = −.02, p = .48), which was counter to prediction, but consistent with previous findings that high maladaptive strategies play a stronger role in depression than low adaptive strategies (Aldao et al., 2010). Also consistent with such work, adaptive and maladaptive ER were modestly and positively correlated (r = .11, p < .001), indicating that individuals’ repertoires of ER include both adaptive and maladaptive strategies.
Close Relationship Status
Supporting predictions, when compared to single participants, those currently in a relationship reported lower depressive symptoms (M = 4.04, SD = 3.84, versus M = 5.25, SD = 4.75), t(1315) = 5.11, p < .001, d = 0.28, and lower use of maladaptive ER (M = −0.04, SD = 0.66, versus M = 0.06, SD = 0.70), t(1316) = 2.69, p = .007, d = 0.15. Participants in relationships also reported somewhat lower use of adaptive ER (M = −0.03, SD = 0.78, versus M = 0.04, SD = 0.76), t(1315) = 1.76, p = .08, d = 0.09.
Social Relationships as Moderators: The Social Context Hypothesis
Concurrent Context
To test the social context hypothesis, we conducted a series of linear regression analyses, with predictors centered around their means. Results for maladaptive and adaptive ER are presented on the left side of Table 1 for social connectedness and relationship status (the right side of Table 1 presents analogous results from Study 2a).
Table 1.
Social Connectedness and Relationship Status as Moderators of Intrapersonal Emotion Regulation’s Associations with Depressive Symptoms (Studies 1 and 2a)
| Social Connectedness (Outcome: Depressive Symptoms)
|
||||||||
|---|---|---|---|---|---|---|---|---|
| Study 1 (N = 1,319) | Study 2a (N = 772) | |||||||
| b | SE | β | p | b | SE | β | p | |
|
|
|
|||||||
| Maladaptive ER | 2.17 | 0.15 | .34 | <.001 | 6.11 | 0.42 | .41 | <.001 |
| Social Connectedness | −0.15 | 0.01 | −.39 | <.001 | −0.31 | 0.02 | −.42 | <.001 |
| Social Connectedness X Maladaptive ER | −0.06 | 0.01 | −.11 | <.001 | −0.16 | 0.02 | −.15 | <.001 |
| F | 304.54 | <.001 | 404.79 | <.001 | ||||
| Adjusted R2 | .41 | .61 | ||||||
|
|
|
|||||||
| Adaptive ER | 0.10 | 0.13 | .02 | .45 | −1.72 | 0.36 | −.13 | <.001 |
| Social Connectedness | −0.21 | 0.01 | −.54 | <.001 | −0.47 | 0.02 | −.62 | <.001 |
| Social Connectedness X Adaptive ER | 0.001 | 0.01 | .002 | .93 | 0.09 | 0.02 | .10 | <.001 |
| F | 175.54 | <.001 | 264.26 | <.001 | ||||
| Adjusted R2 | .29 | .51 | ||||||
|
| ||||||||
|
Relationship Status (Outcome: Depressive Symptoms)
|
||||||||
| Study 1 (N = 1,319) | Study 2a (N = 772) | |||||||
| b | SE | β | p | b | SE | β | p | |
|
|
|
|||||||
| Maladaptive ER | 3.46 | 0.22 | .55 | <.001 | 11.62 | 0.78 | .79 | <.001 |
| Relationship Status | −0.88 | 0.21 | −.10 | <.001 | −0.98 | 0.63 | −.04 | .12 |
| Relationship Status X Maladaptive ER | −0.57 | 0.30 | −.07 | .06 | −2.19 | 0.91 | −.13 | .02 |
| F | 162.37 | <.001 | 230.87 | <.001 | ||||
|
|
|
|||||||
| Adjusted R2 | .27 | .47 | ||||||
|
|
|
|||||||
| Adaptive ER | −0.26 | 0.24 | −.05 | .27 | −6.10 | 0.77 | −.47 | <.001 |
| Relationship Status | −1.23 | 0.24 | −.14 | <.001 | −3.26 | 0.76 | −.14 | <.001 |
| Relationship Status X Adaptive ER | 0.20 | 0.31 | .03 | .53 | 1.30 | 0.92 | .09 | .16 |
| F | 9.27 | <.001 | 60.72 | <.001 | ||||
| Adjusted R2 | .02 | .19 | ||||||
Outcome variable is depressive symptoms (Study 1: BDI-SF; Beck & Beck, 1972; Study 2a: BDI-II; Beck et al., 1996; for interpretation of unstandardized coefficients, note that the two BDI editions have different ranges). Social Connectedness = reverse-scored UCLA Loneliness Scale-Revised (Russell et al., 1980). Relationship status: 0 = single; 1 = current relationship. Maladaptive and adaptive ER are composites of ER strategies in Studies 1 and 2a: see text for details.
Maladaptive ER significantly interacted with social connectedness, but adaptive ER did not. Simple slopes analyses at low (−1SD) and high (+1SD) levels of social connectedness (Hayes & Matthes, 2009) indicated that maladaptive ER was more strongly associated with depressive symptoms when individuals were lower in social connectedness (b = 2.77, SE = 0.17, p < .001) than when they were higher in social connectedness (b = 1.56, SE = 0.20, p < .001), supporting the hypothesis that one’s perception of available social relationships buffers the consequences of ER for depressive symptoms.
A similar pattern emerged for relationship status (lower half of Table 1). At a marginal level of statistical significance, maladaptive ER’s association with symptoms depended on relationship status (p = .06), whereas adaptive ER’s did not (p = .53). Maladaptive ER had a stronger association with depressive symptoms among single participants (b = 3.46, SE = 0.22, p < .001) than among participants in intimate relationships (b = 2.89, SE = 0.20, p < .001).2, 3
Prospective Context
All prospective analyses adjusted for depressive symptoms at Time 1, which were highly correlated with symptoms at Time 2 (r = .60, p < .001). The interaction between maladaptive ER and social connectedness was nonsignificant (b = −0.005, SE = 0.012, p = .67), indicating that the simple effect of maladaptive ER on symptoms over time (b = 0.61, SE = 0.17, p < .001) was not moderated by connectedness (simple effect b = −0.03, SE = 0.01, p = .01), F(4, 1126) = 168.83, p < .001, Adjusted R2 = .37. By contrast, the simple effects of adaptive ER (b = 0.29, SE = 0.13, p = .02) and social connectedness (b = −0.03, SE = 0.01, p = .001) were qualified by an interaction (b = −0.03, SE = 0.01, p = .02), F(4, 1125) = 166.47, p < .001, Adjusted R2 = .37. Controlling for depressive symptoms at Time 1, adaptive ER was associated with increased symptoms at Time 2 among individuals low in social connectedness (b = 0.56, SE = 0.19, p = .003), but was unassociated with Time 2 symptoms among individuals high in social connectedness (b = 0.01 SE = 0.16, p = .94).
Similar to concurrent findings at Time 1, the prospective association of maladaptive ER with symptoms was moderated by relationship status (maladaptive ER b = 0.26, SE = 0.23, p = .26; relationship status b = −0.15, SE = 0.20, p = .44; interaction b = 0.71, SE = 0.29, p = .01), F(4, 1126) = 168.94, p < .001, Adjusted R2 = .38. However, effects were in the opposite direction: adjusting for Time 1 symptoms, maladaptive ER predicted increased depressive symptoms among individuals in romantic relationships (b = 0.97, SE = 0.20, p < .001) but not among single individuals (b = 0.26, SE = 0.23, p = .26). Consistent with cross-sectional findings, adaptive ER did not interact with relationship status in prospective analyses (adaptive ER b = 0.15, SE = 0.20, p = .45; relationship status b = −0.13, SE = 0.20, p = .52; interaction b = 0.11, SE = 0.26, p = 0.66), F(4, 1125) = 160.76, p < .001, Adjusted R2 = .36.
Emotion Regulation as a Mediator: The Social Influence Hypothesis
Concurrent Influence
To test the social influence hypothesis, we first conducted two hierarchical regressions to test mediation. In the first step of each regression, either social connectedness or relationship status was entered as a predictor of depressive symptoms, with maladaptive and adaptive ER entered simultaneously in a second step (see left side of Table 2).
Table 2.
Emotion Regulation as a Mediator of Cross-Sectional Associations of Social Connectedness and Relationship Status with Depressive Symptoms (Studies 1 and 2a)
| Predictor | Outcome: Depressive Symptoms
|
|||||
|---|---|---|---|---|---|---|
| Study 1 (N =1319) | Study 2a (N= 772) | |||||
| β | p | Adj R2 | β | p | Adj R2 | |
| Step 1 | ||||||
| Social Connectedness | −.54 | <.001 | .40 | −.70 | <.001 | .48 |
| Step 2 | ||||||
| Social Connectedness | −.40 | <.001 | .40 | −.41 | <.001 | .60 |
| Maladaptive ER | .37 | <.001 | .40 | <.001 | ||
| Adaptive ER | −.03 | .16 | −.09 | <.001 | ||
|
| ||||||
| Step 1 | ||||||
| Relationship Status | −.14 | <.001 | .02 | −.17 | <.001 | .03 |
| Step 2 | ||||||
| Relationship Status | −.11 | <.001 | .27 | −.05 | .04 | .50 |
| Maladaptive ER | .51 | <.001 | .61 | <.001 | ||
| Adaptive ER | −.08 | .001 | −.19 | <.001 | ||
Outcome variable is depressive symptoms (Study 1: BDI-SF; Beck & Beck, 1972; Study 2: BDI-II; Beck et al., 1996). Social Connectedness = reverse-scored UCLA Loneliness Scale-Revised (Russell et al., 1980). Relationship status is coded with single as the reference group; all other variables are centered around their means. Maladaptive and adaptive ER are composite variables: see text for details.
When ER was added in the second step, the direct effect of social connectedness on symptoms decreased from β = −.54, p < .001, to β = −.40, p < .001, suggesting partial mediation, and the full model accounted for significantly more variance in depressive symptoms, Adjusted R2 = .40, ΔF(2, 1313) = 125.09, p < .001. Similarly, the main effect of being in a relationship decreased from β = −.14, p < .001, to β = −.11, p < .001, after the addition of maladaptive and adaptive ER to the model. The amount of symptom variance accounted for increased substantially, from Adjusted R2 = .02 to .27, ΔF(2, 1312) = 229.87, p < .001.
To test mediation formally, we employed the bootstrapping method recommended by Preacher and Hayes (2008) for multiple mediators. Point estimates of indirect effects represent the multiplicative ab path of independent variables (social connectedness or relationship status) through mediators (maladaptive and adaptive ER). These are reported as unstandardized coefficients with associated standard errors. Estimates were based on 5,000 bootstrapping resamples and are reported with 95% bias-corrected and accelerated confidence intervals; they are considered statistically significant when their confidence intervals do not include 0.
Social connectedness had statistically significant indirect effects on depressive symptoms through maladaptive ER, ab = −0.05, SE = 0.01, 95% CI [−0.07, −0.04], but not through adaptive ER, ab = −0.001, SE = 0.001, 95% CI [−0.003, 0.0001]. Similarly, the association between being in a relationship and lower depressive symptoms was partially accounted for by indirect effects through maladaptive ER, ab = −0.34, SE = 0.12, 95% CI [−0.59, −0.11], but not through adaptive ER, ab = 0.03, SE = 0.02, 95% CI [−0.001, 0.09].
Prospective Influence
To examine social connectedness as a prospective predictor, we first computed partial correlations between social connectedness at Time 1 and ER (or symptoms) at Time 2, partialling out the Time 1 score for ER (or symptoms). Adjusting for Time 1 depressive symptoms, Time 1 social connectedness was associated with lower Time 2 depressive symptoms (pr = −.09, p = .002). Adjusting for Time 1 ER, social connectedness was associated with lower maladaptive ER (pr = −.13, p < .001), but not with adaptive ER (pr = −.01, p = .63). Therefore, being higher in social connectedness prospectively predicted decreases in both maladaptive ER and depressive symptoms over the course of a year.
To test whether social connectedness’ effects on ER over time accounted for its effects on depressive symptoms over time, we conducted a hierarchical regression predicting Time 2 depressive symptoms, entering Time 1 social connectedness in Step 1, Time 1 depressive symptoms, maladaptive ER, and adaptive ER as covariates in Step 2, and Time 2 maladaptive and adaptive ER in step 3. The prospective association of social connectedness with Time 2 symptoms, β = −.38, p < .001, remained statistically significant with the inclusion of Time 1 ER and symptoms, β = −.08, p = .008. The addition of Time 2 ER to the model decreased the effect of social connectedness on Time 2 symptoms, β = −.05, p = .07, indicating mediation, and significantly improved the variance accounted for, ΔR2 = .07, ΔF(2, 1121) = 69.47, p < .001. Bootstrapping analyses controlling for Time 1 predictors revealed a significant indirect effect of social connectedness prospectively through maladaptive ER, ab = −0.009, SE = 0.004, 95% CI [−0.019, −0.001], but not adaptive ER, ab = −0.001, SE = 0.001, 95% CI [−0.004, 0.001]. The full model is presented in Figure 2.4
Figure 2.
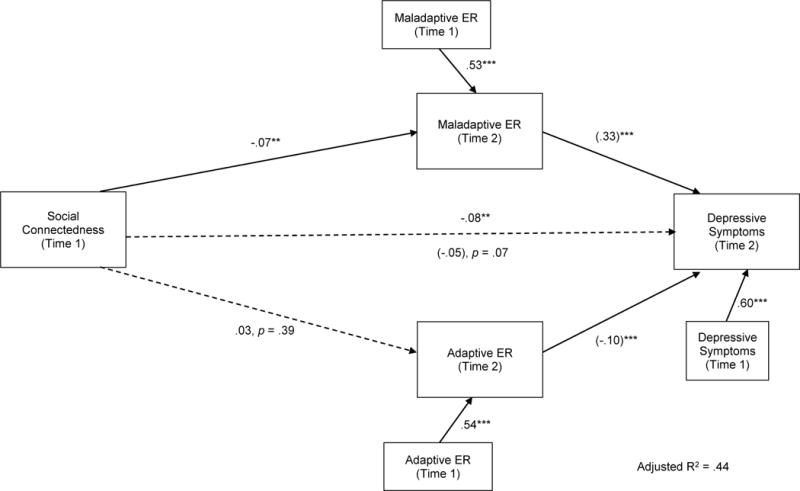
Prospective effects of social connectedness on depressive symptoms through emotion regulation over one year (Study 1).
Coefficients are standardized betas; coefficients in parentheses are after entering mediators into model. Model controls for Time 1 ER and depressive symptoms. N = 1132. ** p < .01; *** p < .001
Cross-sectional results regarding relationship status did not hold over time. Univariate ANCOVAs predicting either depressive symptoms or ER at Time 2 from relationship status at Time 1, controlling for the outcome variable at Time 1, were all statistically nonsignificant, lowest p = .47. Bootstrapping analyses accounting for Time 1 predictors indicated nonsignificant effects of relationship status through Time 2 maladaptive ER, ab = 0.002, SE = 0.07, 95% CI [−0.13, 0.13], and adaptive ER, ab < 0.001, SE = 0.02, 95% CI [−0.04, 0.04].
Discussion
Study 1 provides support for the hypothesis that social relationships play a role in individual ER and depression. Cross-sectionally, the strength of association between an individual’s ER strategies and depressive symptoms depended on how embedded in social relationships he or she was, supporting the social context hypothesis. Specifically, maladaptive ER strategies had weaker associations with depressive symptoms among more socially connected people than among more socially isolated people, and among people in close relationships versus single people, indicating that intrapersonal effects are diluted by social factors. This pattern was specific to maladaptive strategies: whereas social connectedness and relationship status buffered the negative effects of maladaptive strategies, they did not moderate effects of adaptive strategies cross-sectionally.
Moreover, social connectedness and being in a romantic relationship were positively linked with adaptive ER strategy use and negatively linked with maladaptive ER strategy use. Thus, in addition to a buffering quality against the effects of maladaptive intrapersonal ER (the context hypothesis), social relationships were also related to ER strategy use (influence hypothesis). Indeed, as hypothesized, links between social connectedness and relationship status with depressive symptoms were partially accounted for by links with maladaptive intrapersonal ER use. Importantly, social connectedness also prospectively predicted decreases in depressive symptoms over the year, and this effect was partially mediated through decreases in maladaptive ER.
Several differences emerged between concurrent and longitudinal findings. First, whereas the influence of social connectedness through maladaptive ER was supported over time, the influence of close relationship status was not. Second, with regard to the context hypothesis, adaptive ER was prospectively associated with increased symptoms among people low in social connectedness, even though concurrent associations of adaptive ER with symptoms did not depend on connectedness. This finding may indicate that beyond broadly amplifying effects of intrapersonal ER, low social connectedness can confer risk for detrimental effects of even one’s adaptive ER strategies (i.e., backfiring). Third, whereas socially connected and partnered individuals showed weaker associations of their maladaptive ER strategies with depressive symptoms cross-sectionally, prospective findings indicated that connectedness and close relationships may not buffer against effects of maladaptive ER on changes in depression over time. In fact, maladaptive ER predicted longitudinal increases in symptoms only among partnered individuals. This finding is inconsistent with a directional hypothesis that, overall, relationships buffer against maladaptive ER effects and facilitate adaptive ER effects on depression.
However, taken together, these prospective findings are fully consistent with the notion that relationships provide context for both maladaptive and adaptive ER, and can play beneficial or detrimental roles depending on relational processes. The present findings support both the social context hypothesis and the social influence hypothesis, with regard to maladaptive ER especially. However, several aspects of this study limit interpretation. First, when the data in this study were collected (1994–1996), ER was in development as a theoretical and empirical construct (e.g., Gross, 1998). As such, a limited range of ER strategies was tapped. A primary goal of Studies 2a and 2b was to improve the measurement of ER by employing contemporary measures that better capture a more diverse set of ER constructs more strongly grounded in current empirical and theoretical work.
In addition, alternative explanations exist for the observed relations between social connectedness, ER, and symptoms. First, both perceived social connectedness and use of ER strategies are associated with general psychological wellbeing (e.g., Gross & John, 2003; Mellor, Stokes, Firth, Hayashi, & Cummins, 2008), which might more parsimoniously account for depressive symptoms. Second, people who report more social connectedness and who maintain close relationships may differ in relevant social characteristics from people who report more social isolation. Highly connected individuals are more socially skilled and engage differently with people in their social network (Riggio, Watring, & Throckmorton, 1993); perhaps it is not the interpersonal influence that matters, but rather that personality characteristics and social abilities in the individual are confounded with having relationships. In Study 2a we sought to rule out these potential alternative explanations.5
Study 1 also raises important questions of how partners and social supporters influence individuals’ ER and symptoms. Although perceived social connectedness and relationship status provide good indices of the role of social relationships, they do not address underlying relational features, and do not tap the inner workings of specific primary support relationships, such as romantic partnerships. The present findings suggest that a full understanding of social factors requires understanding relationships as playing positive or negative roles in intrapersonal ER and depression, rather than conferring wholesale benefits, consistent with the hypothesis that variability in relationship processes contributes healthy or unhealthy effects. Moreover, relationship status per se overlooks a wide range of variation in both singlehood experiences and romantic partnerships. If individual ER is sensitive to social influences as a system, relationship partners and characteristics should affect individual ER for better or worse, within relationships, in a way that global social connectedness and relationship status cannot capture. In Studies 2a and 2b, we sought to address the limitations of Study 1, while extending our focus to the romantic relationship as a primary context of social ER.
Study 2a: Replication and Extension
Method
Participants and Procedure
Participants were recruited for this study from Amazon’s Mechanical Turk (mTurk.com), an online platform where individuals register to complete a range of tasks and receive monetary compensation. mTurk has been shown to be an efficient method to collect reliable and valid data in basic and clinical psychological research (Buhrmester, Kwang, and Gosling, 2011; Shapiro, Chandler, & Mueller, 2013). The study was described as being about “personality, mood, and social relationships,” and completers received monetary compensation. Participants were directed to a secure online platform, where they provided informed consent and completed a battery of questionnaires before reading a debriefing form and being provided with a link to local mental health resources. Recruitment was limited to the United States; no other inclusion or exclusion criteria were applied other than required minimum age of 18 years.
In total, 772 participants completed the study, 558 (72%) of whom reported a current romantic relationship. The full sample was used, as we sought first to replicate and extend the findings of Study 1 pertaining to social connectedness and relationship status. The full sample included 470 women (61%) and 300 men (39%; 2 declined), with an average age of 34.1 years (SD = 12.0, range = 18–75; 1 declined). Self-reported ethno-racial group was White (77%), Black/African-American (6%), Asian/Asian-American (6%), Hispanic/Latino (6%), multiracial (3%), and other (2%; 1 declined).
Depression Measure
Depressive Symptoms
Depressive symptoms were measured with the 21-item Beck Depression Inventory-II (BDI-II; Beck, Steer, & Brown, 1996), which has good reliability and validity in clinical and nonclinical samples. Scores have a possible range of 0–63, with scores of 14 or higher indicating at least mild symptomatology. Internal consistency in this sample was α = .93.
Social Connectedness and Alternative Explanation Measures
Social Connectedness
As in Study 1, participants completed the UCLA Loneliness Scale (Russell et al., 1980), reversed such that higher scores indicate higher connectedness. Scores in the present study had a possible range of 1–61 (because the measure included the typical 4 scale points, compared to 5 scale points used in Study 1). Internal consistency was α = .95.
Psychological Wellbeing
General psychological wellbeing was measured with the 5-item Satisfaction with Life Scale (SWLS; Diener, Emmons, Larsen, & Griffin, 1985) developed to assess global life satisfaction (e.g., “In most ways my life is close to my ideal”) without tapping loneliness or affect. It has a possible range of 5–35 and good reliability and validity (Diener et al., 1985); in the present study, internal consistency was α = .93.
Social Skills
The Emotional Expressivity and Emotional Sensitivity scales from the self-report Social Skills Inventory (Riggio & Carney, 2003) are linked with objectively skilled behavior and social network quality. In the present study we used 4-item versions of each scale, selecting the highest-loading items on the original scales (Oldmeadow, Quinn, & Kowert, 2012), and averaged across constituent items for possible ranges of 1–5. The expressivity scale (e.g., “I often touch my friends when talking to them”) showed poor reliability (α = .53), but the sensitivity scale (e.g., “I can easily tell what a person’s character is by watching his or her interactions with others”) showed very good reliability (α = .86).
Emotion Regulation Measures
We sought to capture a range of putatively maladaptive and adaptive ER strategies that have been linked with depression. Putatively maladaptive strategies included rumination (measured in two ways), experiential avoidance, expressive suppression, thought suppression, and catastrophizing. Putatively adaptive strategies included cognitive reappraisal, positive refocusing (i.e., attentional deployment toward positive things outside the situation), refocus on planning, positive reappraisal (i.e., focus on positive aspects of the situation), and putting into perspective. Maladaptive ER and adaptive ER composite variables were created by averaging standardized values of these variables, measured as follows.
As in Study 1, rumination was measured with the brooding subscale of the RRS (Treynor et al., 2003; α = .78). Experiential avoidance (e.g., “I worry about not being able to control my worries and feelings”) was measured with the Acceptance and Action Questionnaire (AAQ-II; Bond et al., 2011; α = .94). Cognitive reappraisal (e.g., “When I want to feel less negative emotion, I change the way I’m thinking about the situation”) and expressive suppression (e.g., “I control my emotions by not expressing them”) were measured with the Emotion Regulation Questionnaire (ERQ; Gross & John, 2003; reappraisal α = .89; suppression α = .80). Thought suppression (e.g., “Sometimes I stay busy just to keep thoughts intruding on my mind”) was measured with a 6-item version of the White Bear Suppression Inventory (WBSI; Wegner & Zanakos, 1996) validated by Palm and Strong (2007; α = .90). The Cognitive Emotion Regulation Questionnaire (CERQ; Garnefski & Kraaij, 2007) measured the maladaptive strategies of catastrophizing (e.g., “I often think that what I have experienced is the worst that can happen to a person”) and rumination (e.g., “I am preoccupied with what I think and feel about what I have experienced”), and the adaptive strategies of positive refocusing (e.g., “I think of something nice instead of what has happened”), refocus on planning (e.g., “I think about how I can best cope with the situation”), positive reappraisal (e.g., “I look for the positive sides to the matter”), and putting into perspective (e.g., “I tell myself there are worse things in life”). Internal consistencies for CERQ scales ranged from α = .69 to α = .91. All ER measures have strong psychometric properties, as well as associations with depression and other affective psychopathology (see Aldao et al., 2010).
Results
Descriptive Statistics and Correlations
The mean BDI-II score was 12.06 (SD = 10.49), higher than the community mean in past research (e.g., Dozois, Dobson, & Ahnberg, 1998). The sample included 276 people (36%) with a score of 14 or more, corresponding to at least mild depressive symptoms (Beck et al., 1996). Of the full sample, 106 (14%) scored in the mild range (BDI = 14–19), 100 (13%) scored in the moderate range (BDI = 20–28), and 70 (9%) scored in the severe range (BDI ≥ 29). These rates are higher than in the general population; studies using similar online samples have shown elevated rates of distress and symptoms (Shapiro et al., 2013).
Mean social connectedness was 38.23 (SD = 13.96). Maladaptive and adaptive ER means were both 0 (maladaptive SD = 0.71; adaptive SD = 0.82). Maladaptive and adaptive ER were negatively correlated (r = −.36, p < .001). Means and standard deviations for other variables were: psychological wellbeing M = 20.26, SD = 8.39; emotional expressivity M = 3.07, SD = 0.82; emotional sensitivity M = 3.38, SD = 0.91.
As predicted, depressive symptoms significantly correlated with lower social connectedness, r = −.69, higher maladaptive ER, r = .68, and lower adaptive ER, r = −.41, all p’s < .001. As expected given its potential explanatory value, psychological wellbeing was associated with depressive symptoms (r = −.61), social connectedness (r = .66), maladaptive ER (r = −.51) and adaptive ER (r = .41), all p’s < .001. Similarly, social skills were associated with fewer symptoms (expressivity r = −.34, p < .001, sensitivity r = −.02, p = .58), higher social connectedness (expressivity r = .44, p < .001; sensitivity r = .15, p < .001), less maladaptive ER (expressivity r = −.44, p < .001; sensitivity r = .05, p = .20), and more adaptive ER (expressivity r = .28, p < .001; sensitivity r = .23, p < .001).
Social Connectedness
As predicted, social connectedness was negatively associated with maladaptive ER strategies (r = −.61, p < .001), and positively associated with adaptive ER strategies (r = .43, p < .001). These correlations replicated the associations in Study 1, and were notably stronger.
Moderation: Social Connectedness as Context of ER
To test the context hypothesis, we conducted a series of multiple regression analyses predicting depressive symptoms from social connectedness, ER, and their interaction (with variables centered around their means). Results are presented on the right side of Table 1.6 Replicating cross-sectional findings from Study 1, the main effects of maladaptive ER (β = .41, p < .001) and social connectedness (β = −.42, p < .001) on depressive symptoms were qualified by a statistically significant interaction (β = −.15, p < .001). As predicted, maladaptive ER had a stronger association with symptoms at low levels of social connectedness (−1SD; b = 8.28, SE = 0.53, p < .001) than at high levels (+1SD, b = 3.94, SE = 0.54, p < .001).
In the analysis with adaptive ER, main effects of adaptive ER (β = −.13, p < .001) and social connectedness (β = −.62, p < .001) were qualified by a significant interaction (β = .10, p < .001). Adaptive ER was associated with fewer depressive symptoms at low levels of social connectedness (b = −2.92, SE = 0.46, p < .001), but was not associated with symptoms at high levels of social connectedness (b = −0.53, SE = 0.49, p = .28). Thus, social connectedness diluted effects of adaptive ER.
We also examined the possibility that the apparent role of social connectedness in depressive ER could be due to characteristics of the individual that are likely associated with both social connectedness and depression. Both of the interactions of social connectedness with ER remained when including either life satisfaction (as an index of psychological wellbeing), or emotion sensitivity or expressivity (as indices of social skills), indicating they do not account for the results.
Mediation: Social Connectedness as an Influence on ER
We tested whether the associations between social connectedness and symptoms were attributable to associations with ER (see Table 2, right side). When maladaptive and adaptive ER were entered in the second step of a hierarchical regression, the effect of social connectedness decreased from β = −.70, p < .001, to β = −.41, p < .001, suggesting partial mediation, and the variance accounted for was significantly improved, ΔR2 = .12, ΔF(2, 768) = 110.62, p < .001. Bootstrapping analyses indicated that social connectedness’ effects on depressive symptoms was partially accounted for by both lower maladaptive ER (ab = −0.18, SE = .015, 95% CI [−0.21, −0.15]) and higher adaptive ER (ab = −0.03, SE = 0.01, 95% CI: [−0.05, −0.01]).
Relationship Status
Participants in a relationship were significantly lower in depressive symptoms than single participants (relationship M = 10.97, SD = 9.75; single M = 14.91, SD = 11.78; t(770) = 4.73, p < .001, d = −0.38). They were also significantly higher in social connectedness (M = 40.87, SD = 13.20, versus M = 31.35, SD = 13.56; t(770) = 8.90, p < .001, d = 0.71), psychological wellbeing (M = 21.95, SD = 8.00, versus M = 15.85, SD = 7.76; t(770) = 9.57, p < .001, d = 0.77), emotional expressivity (M = 3.15, SD = 0.81, versus M = 2.85, SD = 0.81; t(762) = 4.66, p < .001, d = 0.37), and emotional sensitivity (M = 3.44, SD = 0.86, versus M = 3.24, SD = 1.00; t(762) = 2.69, p = .007, d = 0.22). Moreover, participants in relationships reported significantly lower levels of maladaptive ER (relationship M = −0.07, SD = 0.71; single M = 0.20, SD = 0.67; t(770) = 4.78, p < .001, d = −0.39), and marginally higher levels of adaptive ER (relationship M = 0.03, SD = 0.81; single M = −0.09, SD = 0.84, t(770) = 1.94, p = .052, d = .15).
Moderation: Relationships as Contexts of ER
The association of maladaptive ER with symptoms (β = .79, p < .001) was moderated by relationship status (interaction β = −.13, p = .02), such that maladaptive ER was associated with higher depressive symptoms among single participants (b = 11.62, SE = 0.78, p < .001) than among participants in relationships (b = 9.43, SE = 0.45, p < .001; see Table 1, right side). By contrast, the effects of adaptive ER (β = −.47, p < .001) and relationship status (β = −.14, p < .001) were not qualified by an interaction (β = .09, p = .16). These findings replicate cross-sectional findings in Study 1.
Mediation: Relationships as Influences on ER
When maladaptive and adaptive ER were added to the second step of a hierarchical regression (Table 2, right side), the direct effect of relationship status decreased from β = −.17, p < .001, to β = −.05, p = .04, suggesting mediation, and the variance explained significantly improved, from R2 = .03 to .50, ΔF(2, 768) = 363.85, p < .001. The beneficial effect of being in a close relationship was partially explained by both lower maladaptive ER (ab = −2.41, SE = .50, 95% CI [−3.42, −1.46]) and higher adaptive ER (ab = −.31, SE = .17, 95% CI [−0.68, −0.01].
Discussion
Study 2a—examining a wider range of ER strategies, as well as a more current measure of depressive symptoms—largely replicated findings in Study 1, with notable differences. We first replicated findings from Study 1 that social connectedness plays a role in whether individuals’ own ER strategies are associated with depressive symptoms, extending these findings to a more comprehensive set of contemporary ER strategies that are linked with depression. The hypothesis that social relationships are implicated in adaptive ER, as well as maladaptive ER, also received more substantial support than in Study 1. Moreover, this study also ruled out the alternative explanations that the role of social connectedness is better explained by general psychological wellbeing or individuals’ social skills, providing stronger support for the notion that relationships themselves influence the role of individual ER in depression.
Findings indicate that when an individual is embedded in social relationships, his or her ER strategies—both adaptive and maladaptive—have weaker associations with symptoms, consistent with the dilution notion of social influences on ER in depression. This finding, contrary to that of Study 1, suggests that the social context hypothesis may involve general dilution across ER in general, rather than specifically buffering maladaptive ER and facilitating adaptive ER. Importantly, this pattern implies that the effect of relationships on symptoms depends in part on the individual’s own specific ER repertoire. However, adaptive ER did not have differential associations with symptoms depending on relationship status. As in Study 1, only the relation between maladaptive ER and symptoms depended on relationship status.
The finding that social connectedness “waters down” effects of individuals’ ER strategies regardless of their adaptiveness is consistent with our hypothesis that relationship resources play a dynamic role in ER that depends on mechanisms at the individual, partner, and relationship levels, rather than providing a wholesale benefit. The present pattern—an effect of social relationships diluting individual ER effects across the board—is exactly what we would expect at the level of social connectedness and relationship status, if the more specific influences of social ER depend mechanistically on characteristics that vary across partners, relationships, and interpersonal interactions.7
Similarly, the present study augmented Study 1′s cross-sectional findings regarding the social influence hypothesis, although it did not allow a prospective test comparable to Study 1. First, results replicated the finding that the beneficial associations of both social connectedness and being in a close relationship with depressive symptoms are partially accounted for by their relations with lower maladaptive ER. Second, they extended these findings to adaptive ER, indicating that even when they do not facilitate effectiveness of individuals’ own adaptive ER, social connections (including romantic partners) may influence use of a range of maladaptive and adaptive ER strategies, with beneficial effects for depression.
Study 2b: Intimacy and Trust within Romantic Relationships
What is it about social relationships that drives these effects on ER and depressive symptoms? If social ER plays a mechanistic role in mental health distinct from other influences of social relationships (e.g., providing instrumental resources, influencing health decision-making; Cacioppo & Hawkley, 2003; Cohen, 2004), we should expect core relational mechanisms of close relationships to be especially important (Lakey et al., 2010; Marroquín, 2011). In particular, because intrapersonal ER involves complex interactions of cognition and affect, we should expect those features of relationships that promote cognitive and affective interdependence between individuals to play foundational roles in social ER, by allowing internal systems of affect and cognition to access interpersonal resources in times of need (and, viewed in a complementary way, by allowing relationship partners to access individuals’ intrapersonal systems when they seek to aid in regulation). Consistent with this hypothesis, Randall and Schoebi (2015) showed that effects of relationship partners on one another’s emotion and psychological distress (i.e., coregulation) depend on individual differences in susceptibility to partners’ affect. We suggest that intimacy and trust between relationship partners are key to this process.
Intimacy is an interpersonal process through which relationship partners express feelings, engage in self-disclosure, and respond to one another’s disclosures and needs, and it largely defines the “closeness” of close relationships (Laurenceau, Barrett, & Pietromonaco, 1998; Reis, Clark, & Holmes, 2004). Trust involves an individual’s ability to take on risk, with a sense of confidence and security in the partner’s reliability, dependability, and predictability (Rempel, Holmes, & Zanna, 1985; Simpson, 2007). Intimacy and trust within relationships may essentially lay the foundations for interpersonal ER by creating the contextual conditions required for interpersonal ER to operate. Just as intrapersonal ER is facilitated by identifying one’s own emotions, and believing one can regulate them (Barrett, Gross, Christensen, & Benvenuto, 2001; Tamir, John, Srivastava, & Gross, 2007), so too is interpersonal ER likely to be facilitated by shared understanding of the individual’s current emotional experience, and the individual’s perception that the partner’s contribution is relevant, safe, and goal-consistent. For partners to be valuable sources of regulatory support, they need to be perceived as able to accurately appraise the individual’s view of the situation and the emotion at hand (which involves intimacy), and as competent and dependable as a source of influence (which involves trust).
Our primary hypothesis in Study 2b was that high trust and high intimacy within a romantic relationship form a foundational context for social ER effects, and promote healthier ER, whereas low trust and intimacy provide a backdrop for individuals’ increased reliance on their own existing ER strategies, and promote less healthy ER. By focusing on people in romantic relationships, we essentially controlled for relevant structural and psychosocial variables connected with relationship status in and of itself (e.g., availability of a close other; dispositional desire for intimate affiliation) and focused on process-oriented conditions and mechanisms of social ER.
Method
Participants and Procedure
Participants in this study were the subset of 558 participants from Study 2a who reported currently being in a committed, romantic relationship; they completed the measures below during the same study session. The sample included 374 women (67%) and 182 men (33%; 2 declined), with an average age of 34.4 years (SD = 11.8, range = 18–70; 1 declined). Ethnoracial group was White (80%), Asian/Asian-American (5%), Hispanic/Latino (5%), Black/African-American (5%), multiracial (3%), and other (2%; 1 declined). Participants self-identified as heterosexual (89%), gay/lesbian (2%), or bisexual (9%).
Participants reported their relationship status: casually dating (4%); committed dating relationship (e.g. boyfriend/girlfriend; 28%); engaged to be married/partnered (8%); married, partnered, or living as if married/partnered (58%); and other (2%). Length of the relationship varied: less than 3 months (3%); 3 to 6 months (3%); 6 months to 1 year (8%); 1 year to 3 years (23%); 3 years to 5 years (15%); 5 years to 10 years (19%); 10 years to 20 years (18%); more than 20 years (12%). Most (77%) reported cohabiting.
Relationship Measures
Intimacy
The 30-item Personal Assessment of Intimacy in Relationships (PAIR; Schaefer & Olson, 1981) adopts a conceptualization of intimacy consistent with Reis and Shaver’s (1988) emphasis on transactional experiences of disclosure and responsiveness (see also Laurenceau et al., 1998; Reis et al., 2004). Participants completed the 6 emotional intimacy items (e.g., My partner can really understand my hurts and joys) and 6 intellectual intimacy items (e.g., When it comes to having a serious discussion, it seems that we have little in common). The scales have good internal consistency and convergent validity with marital satisfaction and conflict, as well as validity across diverse relationship types (Schaefer & Olson, 1981). We computed a total intimacy score (α = .94) by summing the two scales, which were highly correlated (r = .89, p < .001).
Trust
The Trust Scale (Rempel et al., 1985) measures 3 components of interpersonal trust: predictability, faith, and dependability. We examined the 5-item dependability subscale, which taps the degree to which one’s partner is seen as reliable in the face of risk or distress, and captures the lay definition of trust with respect to an individuals’ global assessment of their partner’s reliability based on personal characteristics and past actions (e.g., I can rely on my partner to keep the promises he/she makes to me). This subscale has good internal consistency and construct validity with dating and married couples (Holmes, 1991; Rempel et al., 1985); internal consistency in the present study was α = .86.
Results
Descriptive Statistics
The mean BDI-II score among individuals in relationships was 10.97 (SD = 9.75; range = 0–46), mean maladaptive ER was −0.07 (SD = 0.71; range = −1.60 to 1.96), and mean adaptive ER was 0.03 (SD = 0.81; range = −2.20 to 1.88). Mean intimacy was 47.19 (SD = 11.50; range = 12–60) and trust M = 7.69 (SD = 6.89; range = −15 to 15). Both intimacy and trust had skewed distributions (such that very low scores were infrequent), and were log-transformed for analyses.
Correlations among Variables
Depressive symptoms among individuals in romantic relationships were associated with both maladaptive ER (r = .69, p < .001) and adaptive ER (r = −.40, p < .001). Higher intimacy and trust were significantly associated with lower maladaptive ER (intimacy r = −.36; trust r = −.23), higher adaptive ER (intimacy r = .29; trust r = .26), and lower depressive symptoms (intimacy r = −.41; trust r = −.35), consistent with the hypothesis that relationships higher in these qualities confer benefits for both ER and mental health (all p’s < .001).
Intimacy and Trust as Relational Contexts of ER
Table 3 presents moderation analyses for intimacy and trust. Intimacy significantly moderated the relation between maladaptive ER and symptoms, but not between adaptive ER and symptoms. Individuals’ maladaptive ER had stronger effects on depressive symptoms when they were in low-intimacy relationships (−1SD; b = 10.02, SE = 0.58, p < .001) than when they were in high-intimacy relationships (b = 6.79, SE = 0.61, p < .001). Similarly, maladaptive ER was more strongly related to symptoms in low-trust (b = 9.92, SE = 0.58, p < .001) than in high-trust relationships (b = 7.74, SE = 0.57, p < .001). The relation between adaptive ER and symptoms was not moderated by trust.
Table 3.
Intimacy and Trust within Relationships as Moderators of Intrapersonal Emotion Regulation’s Associations with Depressive Symptoms in Study 2b (N = 558)
| Intimacy | Outcome: Depressive Symptoms
|
|||
|---|---|---|---|---|
| b | SE | β | p | |
| Maladaptive ER | 8.40 | 0.44 | .61 | <.001 |
| Intimacy | −4.63 | 0.68 | −.22 | <.001 |
| Intimacy X Maladaptive ER | −3.46 | 0.88 | −.12 | <.001 |
| F | 197.63 | <.001 | ||
| Adjusted R2 | .52 | |||
|
| ||||
| Adaptive ER | −3.61 | 0.46 | −.30 | <.001 |
| Intimacy | −6.98 | 0.81 | −.33 | <.001 |
| Intimacy X Adaptive ER | 1.37 | 0.95 | .05 | .15 |
| F | 63.79 | <.001 | ||
| Adjusted R2 | .25 | |||
|
| ||||
| Trust | ||||
|
| ||||
| Maladaptive ER | 8.83 | 0.42 | 0.64 | <.001 |
| Trust | −5.11 | 0.73 | −.21 | <.001 |
| Trust X Maladaptive ER | −2.67 | 0.97 | −.08 | .01 |
| F | 198.94 | <.001 | ||
| Adjusted R2 | .52 | |||
|
| ||||
| Adaptive ER | −3.92 | 0.47 | −.32 | <.001 |
| Trust | −6.37 | 0.94 | −.27 | <.001 |
| Trust X Adaptive ER | 0.43 | 1.08 | .02 | .69 |
| F | 52.27 | <.001 | ||
| Adjusted R2 | .22 | |||
Outcome variable is depressive symptoms (BDI-II; Beck et al., 1996). Maladaptive and adaptive ER are composites of ER strategies: see text for details. Intimacy = log-transformed sum of emotional and intellectual intimacy subscales of Personal Assessment of Intimacy in Relationships (PAIR; Schaefer & Olson, 1981). Trust = log-transformed dependability subscale of Trust Scale (Rempel et al., 1985). All variables centered around their means.
Intimacy and Trust as Relational Influences on ER
We conducted analyses testing maladaptive and adaptive ER as mediators of the effects of intimacy and trust on symptoms (see Figure 3). The addition of maladaptive ER and adaptive ER to the intimacy model attenuated the main effect of intimacy (from β = −.41, p < .001, to β = −.16, p < .001) and increased the model’s ability to account for variance in depressive symptoms, ΔR2 = .35, ΔF(2, 553) = 203.81, p < .001. Tests of mediation revealed that the effect of relationship intimacy on symptoms was mediated by both maladaptive ER (ab = −4.34, SE = 0.55, 95% CI [−5.46, −.3.31]) and adaptive ER (ab = −0.89, SE = 0.24, 95% CI [−1.42, −0.47]).
Figure 3.
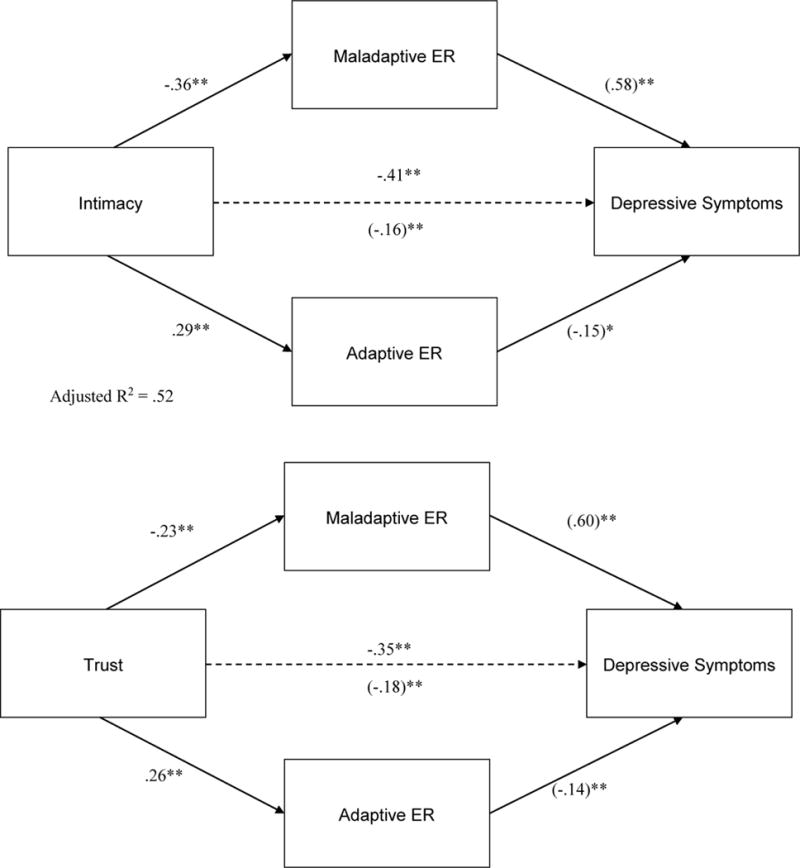
Associations of intimacy and trust with depressive symptoms are partially accounted for by links to emotion regulation (Study 2b).
Coefficients are standardized betas; coefficients in parentheses are after entering mediators into model. N = 558.
** p < .01
The main effect of trust in Step 1, β = −.35, p < .001, decreased to β = −.18, p < .001 when maladaptive and adaptive ER were added in Step 2, and the variance explained increased, ΔR2 = .41, ΔF(2, 552) = 238.44, p < .001. Both maladaptive ER (b = −3.25, SE = 0.64, 95% CI [−4.52, −2.04]) and adaptive ER (b = −0.89, SE = 0.26, 95% CI [−1.44, −0.44]) significantly mediated the relation between relationship trust and depressive symptoms.
Discussion
Primary findings in Study 2b support the hypothesis that with regard to depression, social aspects of ER are not based solely on the perception of available others or the existence of close relationship partners per se, but also on characteristics of those relationships. Among people in romantic relationships, the association between their maladaptive ER strategies and depressive symptoms depended on intimacy and trust. These findings support the notion that romantic relationships represent a context for social ER, and that this role depends specifically on relational conditions that facilitate interpersonal ER through affective connection between partners (see Fruzzetti & Iverson, 2004). Notably, the findings were specific to maladaptive ER, and not adaptive ER, suggesting that within relationships, these characteristics buffer individuals from the effects of their less healthy strategies, without impacting the effectiveness of their healthier strategies.
Extending findings from Studies 1 and 2a, we also found that, in addition to moderating relations between ER strategies and depressive symptoms, intimacy and trust within relationships were also associated with individuals’ use of ER strategies. Moreover, this association statistically accounted for the relations of intimacy and trust with symptoms. In this case, both maladaptive and adaptive ER accounted for social influences. This pattern supports the social influence hypothesis within relationships—that relationship qualities involving emotional connectedness are linked with implementation of a range of maladaptive and adaptive ER strategies.
The present study thus provides added support for the view that relationships are a context in which social influences on individual ER and depressive symptoms occur, and that unique characteristics of relationships can affect the degree to which individuals’ own ER strategies are related to depression. In particular, we provide evidence for the notion that intimacy and trust—long considered crucial components of intimate relationships—also act as buffers against maladaptive ER in the case of depressive symptoms. The present findings advance the idea that ER is a specific mechanism through which relationships and relationship partners influence adaptive functioning and mental health.
Several study limitations deserve mention. First, the study was cross-sectional and cannot speak to causal direction. This is especially important because social relationships and ER have bidirectional effects (Bell & Calkins, 2000), as do relationships and depression (Whisman, 2001). Importantly, only one partner provided data. Our examination of relational variables taps individuals’ perceptions of their relationships and of partners’ support efforts, not objective behavioral measures, and these can differ meaningfully in the case of support (Haber, Coheen, Lucas, & Baltes, 2007). Nevertheless, given our interest in external influences on individuals’ own ER and symptoms, participants’ own assessment of these variables—including relationship phenomena—are likely quite relevant. This is especially the case for questions of psychopathology. What people see as supportive does not always match what their partners see as supportive (Verhofstadt, Ickes, & Buysse, 2010), and perceived support is far more predictive of depression than enacted support (Lakey & Cronin, 2008). Although we hypothesize that objectively measurable, external factors in the social environment affect the individual ER system, we also suspect, for example, that a partner’s objective dependability is a relatively weak facilitator of healthy ER if the individual perceives the partner as undependable.
General Discussion
The present studies tested the hypothesis that social factors in ER strategy use and effectiveness serve as routes through which the social environment, and close relationships in particular, affect intrapersonal ER and depression. Across three studies of two large community samples, our findings provide support for this hypothesis. As such, they address open questions of both basic mechanisms through which social relationships influence health (e.g., Cacioppo & Hawkley, 2003) and routes through which the core psychopathology of depression is affected by its social context (e.g., Lakey & Cronin, 2008; Whisman & Baucom, 2012). Findings support the increasing recognition that ER, typically conceptualized and investigated as an intrapersonal system, is intimately connected to the social world.
Findings also provide new evidence that such influence has a role in psychopathology. Across the studies, we found evidence for both the social context hypothesis—that social relationships moderate the relations between individual ER and symptoms—and the social influence hypothesis, that they affect individuals’ ER in ways that account for depression. That is, with respect to depression, the effectiveness of individuals’ own ER strategies can be diluted or amplified by social and relationship resources, and these resources also affect ER strategy repertoire and use. Although we have examined these routes separately, they are not mutually exclusive. The processes of ER relevant to psychopathology, involving both what people do in the face of distress, and what becomes of their efforts, may be as deeply embedded in multiple, interacting social mechanisms in adulthood as they are in child and adolescent development.
Findings also indicate that romantic relationships’ role in ER can be for better or worse depending on within-relationship factors, integrating prior research on overall benefits of relationships on mental health (Dush & Amato, 2005; Kim & McKenry, 2002) with the role of relationship dysfunction in depression (Whisman & Baucom, 2012). Within relationships, the unique characteristics of close relationships themselves—specifically, intimacy and trust—were not only associated with depressive symptoms through their association with ER strategy use, they also diluted the strength of the link between individuals’ maladaptive ER and symptoms. It appears it is not just the presence of close others that matters for social ER, but also those particular features of close relationships that are tied to affective interdependence.
Social relationships are often considered to be adaptive influences on physical and mental health, including depression (e.g., Cacioppo et al., 2006; Cohen, 2004), whereas social approaches to depressive psychopathology have emphasized maladaptive social patterns (e.g., Hammen, 1991; Joiner et al., 1999). The present findings support social ER as a route through which relationships have both adaptive and maladaptive effects linking the social world with individuals’ symptoms. These social influences were more often due to relations with maladaptive ER strategies than with adaptive strategies, and findings suggest that close relationships characterized by high affective connectedness may play a more focused role in buffering individuals from the harmful effects of their own maladaptive strategies, while allowing adaptive ER to do its helpful work. If so, this is precisely the relational pattern to address individual depression, where individuals’ overuse of maladaptive strategies is more strongly implicated than underuse of adaptive strategies (Aldao & Nolen Hoeksema, 2010).
However, the finding in Study 2a that a comprehensive set of both maladaptive and adaptive ER strategies had weaker associations with depressive symptoms depending on social factors supports the idea that in general, availability of social relationships dilutes the role of individual ER in depression as an overall system, rather than exerting a uniformly helpful influence of buffering maladaptive and amplifying adaptive ER. Future work is needed to examine just how perceived and actual social resources, acting as contexts, dilute or amplify intrapersonal effects once ER strategies are deployed. Effective partners may notice maladaptive ER use and prevent its consequences by, for example, making sure the individual stays active that day, or supporters might introduce beneficial non-ER contributions, such as instrumental support, that by enacting their own effects, dilute the power of ER.
Findings support the hypothesis that relationship partners help shape individuals’ regulatory responses and affect the outcomes of intrapersonal regulation. However, the present studies cannot fully address an additional possibility—that relationships might affect not only use and effectiveness of ER, but also exposure to events that require ER. Indeed, exploratory analyses in Study 1 indicated that lower social connectedness was linked with more stressful life events, which themselves were associated with greater use of overall ER. This pattern remains consistent with the view of ER as a proximal process implicated in broader social-environmental factors in depression. Indeed, one might consider social effects on stress exposure as another type of social ER itself, targeting the situation selection phase of ER (Gross, 1998) and buffering against symptomatology by decreasing demands for the intrapersonal strategies emphasized here, which occur at subsequent cognitive and affective stages of ER. Covarying stressful life events did not account for our findings, but future research should examine social effects on event exposure and regulatory demands, in addition to intrapersonal ER use and effectiveness.
Such a perspective is consistent with Coan and colleagues’ social baseline theory, which proposes that it is not just actual social provisions (e.g., advice or soothing) that affect self-regulation, but rather that intrapersonal neural and psychological processes have evolved to assume the existence of social resources in the environment, and are hampered when such resources are not present (Beckes & Coan, 2011; Coan & Maresh, 2014; Coan & Sbarra, 2015). The conditions of low social connectedness, lack of intimate relationships, and low intimacy and trust within romantic relationships observed in the present studies may confer vulnerability to emotional distress and impair effective ER not just through the social-regulatory actions of others (i.e., interpersonal ER), but also through greater internal processing challenges in the absence of optimal social resources.
Moreover, ER is only one mechanism through which supporters, and social factors more generally, may affect depression and other psychopathology. Although findings supporting the influence hypothesis showed mediation of social effects on symptoms through ER, a substantial portion of the direct effects of social connectedness, relationship status, intimacy, and trust was left unaccounted for by ER. Social factors play roles in depression through other, potentially more distal routes, including stress generation (Hammen, 1991), maladaptive social behavior (Joiner et al., 1999), and relationship conflict (Whisman, 2001), as well as through the multi-domain processes that link relationships and health (Cacioppo & Hawkley, 2003). We suspect ER is a relevant proximal process for mental health outcomes in particular, in light of the central role of emotion dysregulation in psychopathology (Aldao et al., 2010; Kring & Sloan, 2010). To the extent that ER represents an intrapersonal mechanism of social effects, it may play an important proximal role in a broad range of processes typically construed at the “external” levels of interpersonal, relational, or social processes. Indeed, emotion dysregulation at the heart of depression may be affected from the outside not only by dyadic and transactional processes of interpersonal ER, but also by environmental factors that represent more macro-social context and influence (e.g., culture; poverty; institutional discrimination).
Research at a more behavioral and mechanistic level is needed to understand what partners and supporters actually do that “targets” general and disorder-specific ER processes (effectively or ineffectively). It is worth noting that many maladaptive ER strategies in depression—including those tapped in the present studies—involve behavioral, cognitive, and emotional avoidance of distressing experiences, whereas the more adaptive involve an active approach orientation (Stanton et al., 2000). It may be that the cognitive processes and behaviors required to sustain relationships both day-to-day among nondepressed individuals (e.g., responding to a partner asking how your day was) and in the context of depression or emotional disturbance (e.g., explaining your inability to fall asleep) discourage avoidance and encourage emotional and cognitive approach in the social domain that, in turn, undergird basic processes of healthy intrapersonal regulation. Dyadic and experimental paradigms are essential to future work illuminating the individual, partner, and relationship factors proximally and causally involved in interpersonal ER and depression. It will be a critical next step to include both self and partner reports to capture truly dyadic processes, tease apart intrapersonal and interpersonal effects, reduce potential biases in reporting based on one individual’s depression, and more effectively model relationship processes (e.g., using actor-partner independence models; Cook & Kenny, 2005).
Several limitations should be addressed in future work. First, our measure of social connectedness captures individuals’ global sense of available relationships, but more objective measurement of social networks can further elucidate how relationships affect ER. This is especially relevant in depression, where perceptions of support availability and relationship partners can be biased. Second, relationship status in the present studies captures the availability of romantic partners, but obscures variation in a range of psychosocial, demographic, and interpersonal domains that may be relevant to social ER in meaningful ways (e.g., by collapsing never-partnered, divorced, and widowed participants into a “single” category). Relatedly, although romantic relationships are primary sources of social support for many people, they are only one of many relationship types that we suspect influence ER. Different social connections in one’s life can serve different social ER needs, and a “diverse portfolio” of supporters may be especially beneficial (Cheung et al., 2015).
Even as our research supports prospective social effects on ER and depression, it is important to note that intrapersonal processes also affect relational outcomes over time. Alternative longitudinal mediation models in Study 1 indicated that effects of social connectedness over time may involve two routes: (1) affecting maladaptive ER and, in turn, depression (as we emphasize), and (2) affecting depression and, in turn, ER. Moreover, in mediational models examining change in social connectedness over time as the outcome, maladaptive ER mediated effects of depressive symptoms, and vice versa. These models are consistent with reciprocal links between ER and depression, as well as evidence that both depression and ER have social and relationship consequences (e.g. Butler et al., 2003; Whisman, 2001).
We argue that ER plays a central, proximal role in these multidirectional social, emotional, and clinical processes, and future research should examine these pathways. It is important that future work tease apart prospective effects that are not fully addressed in the present studies. Indeed, differences among concurrent and prospective findings in Study 1 highlight the need to disentangle social effects on ER and depression over time. At the same time, however, we note Lakey and Orehek’s (2011) caution that whereas longitudinal designs optimally test effects of stable social factors on psychological outcomes, hypotheses regarding immediate effects of partners and social interactions on intrapersonal outcomes (as in interpersonal ER) may be best tested cross-sectionally. In this vein, experimental investigations may most clearly demonstrate causal effects of supporters on immediate ER.
The studies presented here focused on depression dimensionally, rather than as a clinical diagnosis. Still, it is important to note that in both samples, depressive symptoms were elevated relative to community means, and these samples captured a range that included clinically significant symptomatology (e.g., 36% reporting at least mild symptoms in Study 2a). Future research should examine social influences on ER in clinically depressed individuals, and in particular, whether they incorporate interpersonal influences in different ways at higher levels of severity. In particular, truly dyadic processes of social ER likely depend heavily on the individuals’ own behavior which, in depression, can involve withdrawal or hostility that drive away support or block out its effects (e.g., Joiner et al., 1999; Rehman et al., 2008). Moreover, in severe depression, neurocognitive deficits (e.g., attention, memory, and cognitive flexibility) can reach such significant levels that internal ER processes may simply be unresponsive to external intervention through social routes. It is possible that the normative processes linking the social world with ER break down just when they could be most beneficial.
The present studies support the hypothesis that ER is one mechanism through which social relationship partners—and variation in fundamental qualities of close relationships—affect individual mental health, and may have implications for treatment. For example, clinicians might consider a couple therapy approach to individual depression specifically in cases where the individual lacks important ER capabilities, is in a discordant relationship that hampers ER, or has shown limited progress on ER skills in individual work (see Beach & Whisman, 2012). By far, however, the dominant treatment modality for depression is at the individual level. In such intervention, it is important to consider patients’ social environment as not just a backdrop (e.g., as a psychosocial stressor), but rather as an active contributor to underlying mechanisms—one with the ability to help or hinder. In approaching intervention, clinicians might also consider the possibility that at higher levels of depressive pathology, features of individuals’ regulatory systems that might typically incorporate valuable social resources are limited, presenting supporters, relationship partners, and psychotherapists themselves with formidable barriers.
More fundamentally, the present studies indicate that ER is one route through which social influences “get under the skin” to affect health outcomes, and situate the evolving links between ER and healthy versus maladaptive functioning within the relatively underexplored social context of relationships. Both ER and interpersonal dysfunction are implicated in other mental disorders and in physical health; future work might examine a transdiagnostic role of social ER, as well as how different patterns of social ER may be linked with distinct psychopathologies. Increased attention to the social context of emotion regulation has the potential to advance understanding of the basic mechanisms through which close relationships affect individual health for better or worse.
Acknowledgments
This research was supported in part by an American Psychological Association Dissertation Research Award to Brett Marroquín, and by National Institute of Mental Health grant 5 T32 MH 015750. This article is dedicated to the memory of Susan Nolen-Hoeksema, with gratitude for the generous feedback and advice of Annette Stanton, Margaret Clark, and Thomas Bradbury.
Footnotes
Several demographic differences emerged among the study variables. Women reported significantly more depressive symptoms than men (male M = 4.12, SD = 4.01; female M = 4.95, SD = 4.50; t(1316) = 3.50, p < .001), but higher social connectedness (male M = 54.34, SD = 10.63; female M = 56.89, SD = 11.15; t(1317) = 4.25, p < .001). Women also reported higher use of both maladaptive ER (male M = −0.05, SD = 0.64; female M = 0.05, SD = 0.71; t(1317) = 2.60, p = .009), and adaptive ER (male M = −0.09, SD = 0.80; female M = 0.08, SD = 0.74; t(1316) = 4.02, p < .001). Older age was associated with lower depressive symptoms (r = −.09, p = .001), higher social connectedness (r = .14, p < .001), and lower use of both maladaptive ER (r = −.10, p < .001) and adaptive ER (r = −.14, p < .001). White participants endorsed lower use of maladaptive ER strategies (M = −0.08, SD = 0.61) compared to participants of Asian/Pacific Islander (M = 0.14, SD = 0.66), African-American (M = 0.20, SD = 0.87), Hispanic (M = 0.25, SD = 0.84), and other ethnicity (M = 0.15, SD = .77), F (4, 1314) = 11.91, p < .001. All analyses were conducted with and without including sex, age, and ethnicity as covariates; the pattern of results remained the same, and thus models are reported here without demographic variables included. In light of known gender differences in relationship variables and social support (e.g., Rehman et al., 2008), we also tested gender as a moderator of all analyses. All such interactions were statistically nonsignificant except as noted in the text.
We also tested five alternative longitudinal mediation models representing all other possible orders of predictor, mediator, and outcome. The only alternative model seeking to explain depression (i.e., effects of ER through social connectedness) was not supported. However, in models predicting social connectedness, ER and depression each mediated effects of the other, and in models predicting ER, social connectedness and depression each mediated effects of the other, consistent with the notion that relationships, intrapersonal ER, and depression have complex and multidirectional dynamics over time (see General Discussion).
Another important alternative possibility is that ER plays a more direct role in mental health for individuals who are at risk for other reasons (e.g., dispositional or environmental vulnerabilities) that require them to deploy ER strategies more often, leading depression outcomes to depend more on ER among higher-risk than less vulnerable individuals. We approached this possibility in two ways. First, we compared subgroups of high versus low depression in Studies 1 and 2a, based on recommended cutoff criteria for mild depression (BDI-SF ≥ 5 in Study 1; BDI-II ≥ 14 in Study 2a), and compared correlations between ER and depressive symptoms. In one case (Study 1, Time 1), maladaptive ER was more strongly cross-sectionally correlated with symptoms among higher-BDI participants (r = .42) than among lower-BDI participants (r = .15). Otherwise, cross-sectional and prospective correlations of maladaptive and adaptive ER with symptoms were comparable across risk levels in both samples. Thus, even if lower-risk individuals encounter less frequent demands to use ER compared to higher-risk individuals, it appears that in general, the effects of their ER strategies when deployed are similar.
Second, we examined stressful life events as an index of individuals’ different situational demands for both social support and ER. Using a version of the Stressful Life Circumstances Index of the Health and Daily Living Form (Moos, Cronkite, Billings, & Finney, 1986), we examined both overall number of life events and number of negative events experienced over the course of the past year. Consistent with differential ER demands, social connectedness was cross-sectionally associated with fewer life events overall (r = −.11), and fewer negative events (r = −.15), and life events were associated with more use of both maladaptive ER (overall r = .14, negative r = .17) and adaptive ER (overall r = .26, negative r = .23), all p’s < .001. We then examined stressful life events at Time 1 as a moderator of all prospective analyses (i.e., testing whether context and influence findings differed depending on level of environmental stress or frequency of occasions to regulate emotion) as well as life events as a covariate (i.e., as a more parsimonious account for social and ER effects on depressive symptoms). With regard to the context hypothesis, all findings remained when life events were covaried, and no three-way interactions including life events with either social connectedness or relationship status were statistically significant. With regard to the influence hypothesis, the primary finding that maladaptive ER mediated the effect of social connectedness on symptoms was significantly moderated by life events, such that mediation was not statistically significant at high levels of stressful life events (above the 75th percentile), although patterns were in the same direction. Primary findings that adaptive ER did not mediate effects were not qualified by an interaction with life events.
However, a gender X relationship status X adaptive ER interaction emerged (p = .018) such that among women, adaptive ER was associated with lower symptoms if they were in a relationship (b = −0.64, SE = 0.31, p = .037) but not if they were single (b = −.02, SE = 0.30, p = .95). This gender interaction did not emerge for corresponding analyses in Study 2a.
In all studies, analyses involving relationship status were also conducted adjusting for social connectedness, to address potential effects of their overlap. In all cases, the pattern of findings remained the same, with the single exception being that the marginally-significant interaction between relationship status and maladaptive ER became statistically significant when adjusting for social connectedness, indicating effects of objective relationship status across studies were not due to higher perceived connectedness.
For clarity in interpretation of the unstandardized coefficients, we note that depressive symptoms were measured with the BDI-SF in Study 1, and BDI-II in Study 2, which differ in their ranges.
A potential contributor to the more substantial role of adaptive ER in Study 2a than in Study 1 is that maladaptive and adaptive ER were moderately negatively correlated, whereas in Study 1 they were only modestly (and positively) correlated. A primary aim in Study 2 was to measure ER strategies more specifically, rather than broader coping; the negative correlation may indicate that the selected ER strategies indeed show more adaptive/maladaptive specificity and thus evidenced less overlap attributable to coping in general. In addition, all adaptive and almost all maladaptive strategies in Study 1 were from the COPE (i.e., items from a single measure with common instructions and response set), whereas strategies in Study 2 came from a wider array of measures, mostly designed to tap specific strategies. Thus, greater divergence between adaptive and maladaptive ER in Study 2 versus Study 1 may also reflect differences in measurement variance.
Contributor Information
Brett Marroquín, Department of Psychology, University of California, Los Angeles.
Susan Nolen-Hoeksema, Department of Psychology, Yale University.
References
- Aldao A, Nolen-Hoeksema S. Specificity of cognitive emotion regulation strategies: A transdiagnostic examination. Behaviour Research and Therapy. 2010;48(10):974–983. doi: 10.1016/j.brat.2010.06.002. [DOI] [PubMed] [Google Scholar]
- Aldao A, Nolen-Hoeksema S. When are adaptive strategies most predictive of psychopathology? Journal of Abnormal Psychology. 2012;121(1):276–281. doi: 10.1037/a0023598. [DOI] [PubMed] [Google Scholar]
- Aldao A, Nolen-Hoeksema S, Schweizer S. Emotion-regulation strategies across psychopathology: A meta-analytic review. Clinical Psychology Review. 2010;30(2):217–237. doi: 10.1016/j.cpr.2009.11.004. [DOI] [PubMed] [Google Scholar]
- Barbato A, D’Avanzo B. Efficacy of couple therapy as a treatment for depression: A meta-analysis. Psychiatric Quarterly. 2008;79(2):121–132. doi: 10.1007/s11126-008-9068-0. [DOI] [PubMed] [Google Scholar]
- Barrett LF, Gross J, Christensen TC, Benvenuto M. Knowing what you’re feeling and knowing what to do about it: Mapping the relation between emotion differentiation and emotion regulation. Cognition & Emotion. 2001;15(6):713–724. doi: 10.1080/02699930143000239. [DOI] [Google Scholar]
- Baucom DH, Whisman MA, Paprocki C. Couple-based interventions for psychopathology. Journal of Family Therapy. 2012;34(3):250–270. doi: 10.1111/j.1467-6427.2012.00600.x. [DOI] [Google Scholar]
- Beach SRH, Whisman MA. Affective disorders. Journal of Marital and Family Therapy. 2012;38:201–219. doi: 10.1111/j.1752-0606.2011.00243.x. [DOI] [PubMed] [Google Scholar]
- Beck AT. Depression: Clinical, experimental and theoretical aspects. New York, NY: Harper & Row; 1967. [Google Scholar]
- Beck AT, Beck RW. Screening depressed patients in family practice: A rapid technique. Postgraduate Medicine. 1972;52:81–85. doi: 10.1080/00325481.1972.11713319. [DOI] [PubMed] [Google Scholar]
- Beck AT, Steer RA, Brown GK. Beck Depression Inventory-II manual. New York, NY: Harcourt Brace Janovich; 1996. [Google Scholar]
- Beckes L, Coan JA. Social baseline theory: The role of social proximity in emotion and economy of action. Social and Personality Psychology Compass. 2011;5:976–988. [Google Scholar]
- Bell KL, Calkins SD. Relationships as inputs and outputs of emotion regulation. Psychological Inquiry. 2000;11(3):160–163. [Google Scholar]
- Bodenmann G, Plancherel B, Beach SR, Widmer K, Gabriel B, Meuwly N, Schramm E. Effects of coping-oriented couple therapy on depression: A randomized clinical trial. Journal of Consulting and Clinical Psychology. 2008;76:944–954. doi: 10.1037/a0013467. [DOI] [PubMed] [Google Scholar]
- Bond FW, Hayes SC, Baer RA, Carpenter KM, Guenole N, Orcutt HK, Zettle RD. Preliminary psychometric properties of the acceptance and action questionnaire–II: A revised measure of psychological inflexibility and experiential avoidance. Behavior Therapy. 2011;42(4):676–688. doi: 10.1016/j.beth.2011.03.007. [DOI] [PubMed] [Google Scholar]
- Buhrmester M, Kwang T, Gosling SD. Amazon’s Mechanical Turk: A new source of inexpensive, yet high-quality, data? Perspectives on Psychological Science. 2011;6(1):3–5. doi: 10.1177/1745691610393980. [DOI] [PubMed] [Google Scholar]
- Butler EA, Egloff B, Wilhelm FH, Smith NC, Erickson EA, Gross JJ. The social consequences of expressive suppression. Emotion. 2003;3(1):48–67. doi: 10.1037/1528-3542.3.1.48. [DOI] [PubMed] [Google Scholar]
- Butler EA, Randall AK. Emotional coregulation in close relationships. Emotion Review. 2013;5(2):202–210. doi: 10.1177/1754073912451630. [DOI] [Google Scholar]
- Cacioppo JT, Hawkley LC. Social isolation and health, with an emphasis on underlying mechanisms. Perspectives in Biology and Medicine. 2003;46(3):S39–S52. [PubMed] [Google Scholar]
- Cacioppo JT, Hughes ME, Waite LJ, Hawkley LC, Thisted RA. Loneliness as a specific risk factor for depressive symptoms: Cross-sectional and longitudinal analyses. Psychology and Aging. 2006;21:140–151. doi: 10.1037/0882-7974.21.1.140. [DOI] [PubMed] [Google Scholar]
- Campbell-Sills L, Barlow DH, Brown TA, Hofmann SG. Acceptability and suppression of negative emotion in anxiety and mood disorders. Emotion. 2006;6(4):587–595. doi: 10.1037/1528-3542.6.4.587. [DOI] [PubMed] [Google Scholar]
- Carver CS. You want to measure coping but your protocol’s too long: Consider the brief COPE. International Journal of Behavioral Medicine. 1997;4(1):92–100. doi: 10.1207/s15327558ijbm0401_6. [DOI] [PubMed] [Google Scholar]
- Carver CS, Scheier MF, Weintraub JK. Assessing coping strategies: A theoretically based approach. Journal of Personality and Social Psychology. 1989;56:267–283. doi: 10.1037//0022-3514.56.2.267. [DOI] [PubMed] [Google Scholar]
- Cheung EO, Gardner WL, Anderson JF. Emotionships: Examining people’s emotion-regulation relationships and their consequences for well-being. Social Psychology and Personality Science. 2015;6:407–414. Doi: http://dx.doi.org/10.1177/1948550614564223. [Google Scholar]
- Coan JA. Adult attachment and the brain. Journal of Social and Personal Relationships. 2010;27:210–217. doi: 10.1177/0265407510368966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coan JA, Maresh EL. Social baseline theory and the social regulation of emotion. In: Gross J, editor. Handbook of Emotion Regulation. 2nd. New York: Guilford; 2014. pp. 221–236. [Google Scholar]
- Coan JA, Sbarra DA. Social baseline theory: The social regulation of risk and effort. Current Opinion in Psychology. 2015;1:87–91. doi: 10.1016/j.copsyc.2014.12.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coan JA, Schaefer HS, Davidson RJ. Lending a hand: Social regulation of the neural response to threat. Psychological Science. 2006;17(12):1032–1039. doi: 10.1111/j.1467-9280.2006.01832.x. [DOI] [PubMed] [Google Scholar]
- Cohen S. Social relationships and health. American Psychologist. 2004;59:676–684. doi: 10.1037/0003-066X.59.8.676. [DOI] [PubMed] [Google Scholar]
- Cook WL, Kenny DA. The Actor-Partner Interdependence Model: A model of bidirectional effects in developmental studies. International Journal of Behavioral Development. 2005;29:101–109. [Google Scholar]
- Diener E, Emmons RA, Larsen RJ, Griffin S. The satisfaction with life scale. Journal of Personality Assessment. 1985;49(1):71–75. doi: 10.1207/s15327752jpa4901_13. [DOI] [PubMed] [Google Scholar]
- Dixon-Gordon KL, Bernecker SL, Christensen K. Recent innovations in the field of interpersonal emotion regulation. Current Opinion in Psychology. 2015;3:6–42. [Google Scholar]
- Dozois DJA, Dobson KS, Ahnberg JL. A psychometric evaluation of the Beck Depression Inventory-II. Psychological Assessment. 1998;10:83–89. [Google Scholar]
- Dush CM, Amato PR. Consequences of relationship status and quality for subjective well-being. Journal of Social & Personal Relationships. 2005;22:607–627. [Google Scholar]
- Ehring T, Fischer S, Schnülle J, Bösterling A, Tuschen-Caffier B. Characteristics of emotion regulation in recovered depressed versus never depressed individuals. Personality and Individual Differences. 2008;44:1574–1584. [Google Scholar]
- Eisenberg N, Spinrad TL, Eggum ND. Emotion-related self-regulation and its relation to children’s maladjustment. Annual Review of Clinical Psychology. 2010;6(1):495–525. doi: 10.1146/annurev.clinpsy.121208.131208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fitzsimons GM, Finkel EJ. Interpersonal influences on self-regulation. Current Directions in Psychological Science. 2010;19(2):101–105. doi: 10.1177/0963721410364499. [DOI] [Google Scholar]
- Fitzsimons GM, Finkel EJ. The effects of self-regulation on social relationships. In: Vohs KD, Baumeister RF, editors. Handbook of self-regulation. Research, theory and applications. 2. New York, NY: Guilford; 2011. pp. 407–421. [Google Scholar]
- Flores LE, Berenbaum H. Desire for emotional closeness moderates the effectiveness of the social regulation of emotion. Personality and Individual Differences. 2012;53(8):952–957. doi: 10.1016/j.paid.2012.07.009. [DOI] [Google Scholar]
- Frazier PA, Tix AP, Barnett CL. The relational context of social support: Relationship satisfaction moderates the relations between enacted support and distress. Personality and Social Psychology Bulletin. 2003;29(9):1133–1146. doi: 10.1177/0146167203254545. [DOI] [PubMed] [Google Scholar]
- Fruzzetti AE, Iverson KM. Mindfulness, acceptance, validation, and “individual” psychopathology in couples. In: Hayes SC, Follette VM, Linehan MM, editors. Mindfulness and acceptance: Expanding the cognitive-behavioral tradition. New York, NY: Guilford Press; 2004. pp. 168–191. [Google Scholar]
- Fruzzetti AE, Worrall JM. Accurate expression and validating responses: A transactional model for understanding individual and relationship distress. In: Sullivan KT, Davila J, editors. Support processes in intimate relationships. New York, NY: Oxford University Press; 2010. pp. 121–150. [Google Scholar]
- Gable SL, Reis HT. Good news! Capitalizing on positive events in an interpersonal context. In: Zanna MP, editor. Advances in Experimental Social Psychology. Vol. 42. San Diego, CA: Elsevier Academic Press; 2010. pp. 195–257. [Google Scholar]
- Garnefski N, Kraaij V. The Cognitive Emotion Regulation Questionnaire. European Journal of Psychological Assessment. 2007;23(3):141–149. doi: 10.1027/1015-5759.23.3.141. [DOI] [Google Scholar]
- Gotlib IH, Joormann J. Cognition and depression: Current status and future directions. Annual Review of Clinical Psychology. 2010;6(1):285–312. doi: 10.1146/annurev.clinpsy.121208.131305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Graham SM, Huang JY, Clark MS, Helgeson VS. The positives of negative emotions: Willingness to express negative emotions promotes relationships. Personality and Social Psychology Bulletin. 2008;34(3):394–406. doi: 10.1177/0146167207311281. [DOI] [PubMed] [Google Scholar]
- Gross JJ. The emerging field of emotion regulation: An integrative review. Review of General Psychology. 1998;2(3):271–299. [Google Scholar]
- Gross JJ, John OP. Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. Journal of Personality and Social Psychology. 2003;85(2):348–362. doi: 10.1037/0022-3514.85.2.348. [DOI] [PubMed] [Google Scholar]
- Haber MG, Cohen JL, Lucas T, Baltes BB. The relationship between self-reported received and perceived social support: A meta-analytic review. American Journal of Community Psychology. 2007;39(1–2):133–144. doi: 10.1007/s10464-007-9100-9. [DOI] [PubMed] [Google Scholar]
- Hammen C. Generation of stress in the course of unipolar depression. Journal of Abnormal Psychology. 1991;100(4):555–561. doi: 10.1037//0021-843x.100.4.555. [DOI] [PubMed] [Google Scholar]
- Hatfield E, Cacioppo JL, Rapson RL. Emotional contagion. Current Directions in Psychological Science. 1993;2:96–99. [Google Scholar]
- Hayes AF, Matthes J. Computational procedures for probing interactions in OLS and logistic regression: SPSS and SAS implementations. Behavior Research Methods. 2009;41(3):924–936. doi: 10.3758/brm.41.3.924. [DOI] [PubMed] [Google Scholar]
- Holmes JG. Trust and the appraisal process in close relationships. In: Jones WH, Perlman D, editors. Advances in Personal Relationships. Vol. 3. London: Sage; 1991. pp. 187–220. [Google Scholar]
- Holtzman S, Newth S, DeLongis A. The role of social support in coping with daily pain among patients with rheumatoid arthritis. Journal of Health Psychology. 2004;9(5):677–695. doi: 10.1177/1359105304045381. [DOI] [PubMed] [Google Scholar]
- Iida M, Seidman G, Shrout PE, Fujita K, Bolger N. Modeling support provision in intimate relationships. Journal of Personality and Social Psychology. 2008;94:460–478. doi: 10.1037/0022-3514.94.3.460. [DOI] [PubMed] [Google Scholar]
- Joiner TE, Metalsky GI, Katz J, Beach SRH. Depression and excessive reassurance-seeking. Psychological Inquiry. 1999;10(4):269–278. [Google Scholar]
- Kashdan TB, Rottenberg J. Psychological flexibility as a fundamental aspect of health. Clinical Psychology Review. 2010;30(7):865–878. doi: 10.1016/j.cpr.2010.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Archives of General Psychiatry. 2005;62:593–602. doi: 10.1001/archpsyc.62.6.593. [DOI] [PubMed] [Google Scholar]
- Kim HK, McKenry PC. The relationship between marriage and psychological well-being: A longitudinal analysis. Journal of Family Issues. 2002;23(8):885–911. doi: 10.1177/019251302237296. [DOI] [Google Scholar]
- Knight RG. Some general population norms for the short form Beck Depression Inventory. Journal of Clinical Psychology. 1984;40:751–753. doi: 10.1002/1097-4679(198405)40:3<751::aid-jclp2270400320>3.0.co;2-y. [DOI] [PubMed] [Google Scholar]
- Kring AM, Sloan DM. Emotion regulation in psychopathology: A transdiagnostic approach to etiology and treatment. New York, NY: Guilford; 2010. [Google Scholar]
- Lakey B. Social support: Basic research and new strategies for intervention. In: Maddux JE, Tangney JP, editors. Social Psychological Foundations of Clinical Psychology. NY: Guilford; 2010. pp. 177–194. [Google Scholar]
- Lakey B, Cronin A. Low social support and major depression: Research, theory and methodological issues. In: Dobson KS, Dozois DJA, editors. Risk factors in depression. Academic Press; 2008. pp. 385–408. [Google Scholar]
- Lakey B, Drew JB, Sirl K. Clinical depression and perceptions of supportive others: A generalizability analysis. Cognitive Therapy and Research. 1999;23:511–533. [Google Scholar]
- Lakey B, Orehek E, Hain KL, VanVleet M. Enacted support’s links to negative affect and perceived support are more consistent with theory when social influences are isolated from trait influences. Personality & Social Psychology Bulletin. 2010;36(1):132–142. doi: 10.1177/0146167209349375. [DOI] [PubMed] [Google Scholar]
- Lakey B, Orehek E. Relational regulation theory: A new approach to explain the link between perceived social support and mental health. Psychological Review. 2011;118(3):482–495. doi: 10.1037/a0023477. [DOI] [PubMed] [Google Scholar]
- Lakey B, Scoboria A. Trait and social influences in the links between perceived social support and mental health. Journal of Personality. 2005;73:361–388. doi: 10.1111/j.1467-6494.2005.00312.x. [DOI] [PubMed] [Google Scholar]
- Lakey B, Tanner SM. Social influences in negative thinking and affect. Cognitive Therapy and Research. 2013;37(1):160–172. [Google Scholar]
- Laurenceau JP, Barrett LF, Pietromonaco PR. Intimacy as an interpersonal process: The importance of self-disclosure, partner disclosure, and perceived partner responsiveness in interpersonal exchanges. Journal of Personality and Social Psychology. 1998;74(5):1238–1251. doi: 10.1037//0022-3514.74.5.1238. [DOI] [PubMed] [Google Scholar]
- Lepore SJ, Fernandez-Berrocal P, Ragan J, Ramos N. It’s not that bad: Social challenges to emotional disclosure enhance adjustment to stress. Anxiety, Stress & Coping. 2004;17(4):341–361. doi: 10.1080/10615800412331318625. [DOI] [Google Scholar]
- Lepore SJ, Ragan JD, Jones S. Talking facilitates cognitive-emotional processes of adaptation to an acute stressor. Journal of Personality and Social Psychology. 2000;78(3):499–508. doi: 10.1037//0022-3514.78.3.499. [DOI] [PubMed] [Google Scholar]
- Lewinsohn PM. The behavioral study and treatment of depression. Progress in behavior modification. 1975;1:19–64. [Google Scholar]
- Marroquín B. Interpersonal emotion regulation as a mechanism of social support in depression. Clinical Psychology Review. 2011;31(8):1276–1290. doi: 10.1016/j.cpr.2011.09.005. [DOI] [PubMed] [Google Scholar]
- Mellor D, Stokes M, Firth L, Hayashi Y, Cummins R. Need for belonging, relationship satisfaction, loneliness, and life satisfaction. Personality and Individual Differences. 2008;45(3):213–218. doi: 10.1016/j.paid.2008.03.020. [DOI] [Google Scholar]
- Moos RH, Cronkite RC, Billings AG, Finney JW. Health and Daily Living Form manual. Social Ecology Laboratory, Department of Psychiatry and Behavioral Sciences, Veterans Administration and Stanford University Medical Centers; Palo Alto, CA: 1986. [Google Scholar]
- Nolen-Hoeksema S. The role of rumination in depressive disorders and mixed anxiety/depressive symptoms. Journal of Abnormal Psychology. 2000;109:504–511. [PubMed] [Google Scholar]
- Nolen-Hoeksema S, Davis CG. Thanks for sharing that: Ruminators and their social support networks. Journal of Personality and Social Psychology. 1999;77:801–814. doi: 10.1037//0022-3514.77.4.801. [DOI] [PubMed] [Google Scholar]
- Nolen-Hoeksema S, Larson J, Grayson C. Explaining the gender difference in depressive symptoms. Journal of Personality and Social Psychology. 1999;77(5):1061–1072. doi: 10.1037//0022-3514.77.5.1061. [DOI] [PubMed] [Google Scholar]
- Nolen-Hoeksema S, Morrow J. A prospective study of depression and posttraumatic stress symptoms after a natural disaster: The 1989 Loma Prieta earthquake. Journal of Personality and Social Psychology. 1991;61(1):115–121. doi: 10.1037//0022-3514.61.1.115. [DOI] [PubMed] [Google Scholar]
- Nolen-Hoeksema S, Wisco BE, Lyubomirsky S. Rethinking rumination. Perspectives on Psychological Science. 2008;3(5):400–424. doi: 10.1111/j.1745-6924.2008.00088.x. [DOI] [PubMed] [Google Scholar]
- Oldmeadow JA, Quinn S, Kowert R. Attachment style, social skills, and Facebook use amongst adults. Computers in Human Behavior. 2013;29(3):1142–1149. doi: 10.1016/j.chb.2012.10.006. [DOI] [Google Scholar]
- Palm KM, Strong DR. Using item response theory to examine the White Bear Suppression Inventory. Personality and Individual Differences. 2007;42(1):87–98. doi: 10.1016/j.paid.2006.06.023. [DOI] [Google Scholar]
- Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods. 2008;40:879–891. doi: 10.3758/brm.40.3.879. [DOI] [PubMed] [Google Scholar]
- Randall AK, Schoebi D. Lean on me: Susceptibility to partner affect attenuates psychological distress over a 12-month period. Emotion. 2015;15:201–10. doi: 10.1037/emo0000043. [DOI] [PubMed] [Google Scholar]
- Rehman U, Gollan J, Mortimer A. The marital context of depression: Research, limitations, and new directions. Clinical Psychology Review. 2008;28(2):179–198. doi: 10.1016/j.cpr.2007.04.007. [DOI] [PubMed] [Google Scholar]
- Reis HT, Shaver P. Intimacy as an interpersonal process. In: Duck S, editor. Handbook of Personal Relationships: Theory, Research, and Interventions. New York, NY: Wiley; 1988. pp. 367–389. [Google Scholar]
- Reis HT, Clark MS, Holmes JG. Perceived partner responsiveness as an organizing construct in the study of intimacy and closeness. In: Mashek D, Aron A, editors. The handbook of closeness and intimacy. Mahwah, NJ: Lawrence Erlbaum Associates; 2004. pp. 201–225. [Google Scholar]
- Rempel JK, Holmes JG, Zanna MP. Trust in close relationships. Journal of Personality and Social Psychology. 1985;49(1):95–112. [PubMed] [Google Scholar]
- Richards JM, Butler EA, Gross JJ. Emotion regulation in romantic relationships: The cognitive consequences of concealing feelings. Journal of Social and Personal Relationships. 2003;20(5):599–620. doi: 10.1177/02654075030205002. [DOI] [Google Scholar]
- Riggio RE, Carney DR. Social Skills Inventory manual. Second. Redwood City, CA: MindGarden; 2003. [Google Scholar]
- Riggio RE, Watring KP, Throckmorton B. Social skills, social support, and psychological adjustment. Personality and Individual Differences. 1993;15(3):275–280. [Google Scholar]
- Rimé B. Emotion elicits the social sharing of emotion: Theory and empirical review. Emotion Review. 2009;1:60–85. [Google Scholar]
- Russell DW, Peplau L, Cutrona CE. The Revised UCLA Loneliness Scale: Concurrent and discriminant validity evidence. Journal of Personality and Social Psychology. 1980;39:472–480. doi: 10.1037//0022-3514.39.3.472. [DOI] [PubMed] [Google Scholar]
- Schaefer MT, Olson DH. Assessing intimacy: The PAIR inventory. Journal of Marital and Family Therapy. 1981;7(1):47–60. [Google Scholar]
- Shapiro DN, Chandler J, Mueller PA. Using mechanical turk to study clinical populations. Clinical Psychological Science. 2013;1(2):213–220. doi: 10.1177/2167702612469015. [DOI] [Google Scholar]
- Simpson JA. Psychological foundations of trust. Current Directions in Psychological Science. 2007;16(5):264–268. [Google Scholar]
- Spasojevic J, Alloy LB. Rumination as a common mechanism relating depressive risk factors to depression. Emotion. 2001;1:25–37. doi: 10.1037/1528-3542.1.1.25. [DOI] [PubMed] [Google Scholar]
- Spinrad TL, Eisenberg N, Gaertner B, Popp T, Smith CL, Kupfer A, Hofer C. Relations of maternal socialization and toddlers’ effortful control to children’s adjustment and social competence. Developmental Psychology. 2007;43(5):1170–1186. doi: 10.1037/0012-1649.43.5.1170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Srivastava S, Tamir M, McGonigal KM, John OP, Gross JJ. The social costs of emotional suppression: A prospective study of the transition to college. Journal of Personality and Social Psychology. 2009;96(4):883–897. doi: 10.1037/a0014755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stanton AL, Kirk SB, Cameron CL, Danoff-Burg S. Coping through emotional approach: Scale construction and validation. Journal of Personality and Social Psychology. 2000;78:1150–1169. doi: 10.1037/0022-3514.78.6.1150. [DOI] [PubMed] [Google Scholar]
- Swann WB, Jr, Wenzlaff RM, Krull DS, Pelham BW. Allure of negative feedback: Self-verification strivings among depressed persons. Journal of Abnormal Psychology. 1992;101(2):293–306. doi: 10.1037/0021-843x.101.2.293. [DOI] [PubMed] [Google Scholar]
- Tamir M, John OP, Srivastava S, Gross JJ. Implicit theories of emotion: Affective and social outcomes across a major life transition. Journal of Personality and Social Psychology. 2007;92(4):731–744. doi: 10.1037/0022-3514.92.4.731. [DOI] [PubMed] [Google Scholar]
- Taylor SE, Stanton AL. Coping resources, coping processes, and mental health. Annual Review of Clinical Psychology. 2007;3:377–401. doi: 10.1146/annurev.clinpsy.3.022806.091520. [DOI] [PubMed] [Google Scholar]
- Thompson RA. Emotion regulation: A theme in search of a definition. Monographs of the Society for Research in Child Development. 1994;59:25–52. [PubMed] [Google Scholar]
- Treynor W, Gonzalez R, Nolen-Hoeksema S. Rumination reconsidered: A psychometric analysis. Cognitive Therapy and Research. 2003;27(3):247–259. [Google Scholar]
- Uchino BN, Cacioppo JT, Kiecolt-Glaser JK. The relationship between social support and physiological processes: A review with emphasis on underlying mechanisms and implications for health. Psychological Bulletin. 1996;119(3):488–531. doi: 10.1037/0033-2909.119.3.488. [DOI] [PubMed] [Google Scholar]
- Van Kleef GA. The emerging view of emotion as social information. Social and Personality Psychology Compass. 2010;4:331–343. [Google Scholar]
- Verhofstadt LL, Ickes W, Buysse A. I know what you need right now: Empathic accuracy and support provision in marriage. In: Sullivan JDKT, editor. Support processes in intimate relationships. New York, NY: Oxford University Press; 2010. pp. 71–88. [Google Scholar]
- Wegner DM, Zanakos S. Chronic thought suppression. Journal of Personality. 1996;62(4):615–640. doi: 10.1111/j.1467-6494.1994.tb00311.x. [DOI] [PubMed] [Google Scholar]
- Whisman MA. The association between depression and marital dissatisfaction. In: Beach S, editor. Marital and family processes in depression: A scientific approach. Washington, DC: American Psychological Association; 2001. pp. 3–24. [Google Scholar]
- Whisman MA, Baucom DH. Intimate relationships and psychopathology. Clinical Child and Family Psychology Review. 2012;15(1):4–13. doi: 10.1007/s10567-011-0107-2. [DOI] [PubMed] [Google Scholar]
- Zaki J, Williams WC. Interpersonal emotion regulation. Emotion. 2013;13:803–810. doi: 10.1037/a0033839. [DOI] [PubMed] [Google Scholar]