

Abstract
[Purpose] Medial knee osteoarthritis, a degenerative joint disease, affects adults. The external knee adduction moment, a surrogate knee-loading measure, has clinical implications for knee osteoarthritis patients. Tai Chi is a promising intervention for pain alleviation in knee osteoarthritis; however, the characteristics of external knee adduction moment during Tai Chi have not been established. [Subjects and Methods] During normal and Tai Chi walking, a gait analysis was performed to compare the external knee adduction moment moment-arm characteristics and paired t-tests to compare moment-arm magnitudes. [Results] A significant difference was observed in the average lateral direction of moment-arm magnitude during Tai Chi walking (−0.0239 ± 0.011 m) compared to that during normal walking (−0.0057 ± 0.004 m). No significant difference was found between conditions in average medial direction of moment-arm magnitude (normal walking: 0.0143 ± 0.010 m; Tai Chi walking: 0.0098 ± 0.014 m). [Conclusion] Tai Chi walking produced a larger peak lateral moment-arm value than normal walking during the stance phase, whereas Tai Chi walking and normal walking peak medial moment-arm values were similar, suggesting that medial knee joint loading may be avoided during Tai Chi walking.
Key words: Tai Chi gait, External knee adduction moment arm, Walking
INTRODUCTION
Knee osteoarthritis (OA) is a common degenerative joint disorder affecting older adults. The external knee adduction moment (EKAM) is a surrogate medial knee joint loading measure linked with the severity1) and progression2) of medial compartment knee OA. The EKAM is the product of frontal plane ground reaction force (GRF) and frontal plane moment arm (the perpendicular distance from the frontal plane GRF vector to the center of the knee joint). Individuals with knee OA have significantly greater than normal EKAM compared with measures of knee joint loading in other planes of motion, such as knee flexion and extension moments3). Thus, EKAM has become a variable of great interest in knee OA research.
Tai Chi is an ancient Chinese martial art, involving slow and sequential patterns of movement. It has been shown to alleviate patient-reported pain and improve physical function in patients with chronic conditions, including knee OA4, 5). However, few biomechanical studies exist to support such conclusions. Biomechanical analyses of Tai Chi are imperative in order to understand the underlying mechanisms associated with improvements in movement function and attenuation of symptoms related to chronic joint conditions such as knee OA.
Although previous studies have described various biomechanical characteristics of Tai Chi gait6,7,8), no investigations to date have looked at specific EKAM characteristics during Tai Chi gait. In a study by Hunt et al.9), a higher correlation was found between the peak EKAM moment arm and peak EKAM outcome than between peak frontal plane GRF and peak EKAM. This finding suggests that EKAM moment arm characteristics are a critical component for understanding EKAM outcomes during the stance phase and should be the subject of further analysis in studies examining medial knee joint loading responses during walking tasks.
Describing EKAM moment-arm characteristics during the Tai Chi gait of asymptomatic healthy individuals is the first step toward understanding the EKAM response to Tai Chi interventions within the medial compartment of the knee in the OA population. The purpose of this study was to quantify the EKAM moment-arm characteristics during the stance phase of normal walking (NW) and Tai Chi walking (TW) in healthy individuals. The working hypothesis was that moment-arm characteristics would differ between TW and NW stance phases.
SUBJECTS AND METHODS
A total of 10 subjects, 5 males and 5 females were enrolled in this study. Their mean age was 58.4 ± 13.1 years (mean ± SD); weight, 73.57 ± 18.54 kg; and height, 1.73 ± 0.08 m. None of the subjects had a history of musculoskeletal and/or neurological condition or injury to either lower extremity. This study was approved by the university’s Institutional Review Board, and informed consent was obtained from each participant prior to data collection.
A 7-camera optical motion capture system (VICON Technology, Los Angeles, CA, USA), capturing at 100 Hz, was used to obtain kinematic measurements during each trial performed within a capture area. Two force platforms capturing at 1,000 Hz (Advanced Mechanical Technology, Inc., Watertown, MA, USA) were embedded in a walkway (3 m wide × 10 m long) inside the capture area and used to obtain GRF measurements. Kinematic and kinetic data were simultaneously collected using Nexus software (VICON Technology, Los Angeles, CA, USA).
Subjects underwent gait analysis as part of the experimental protocol. Reflective markers were placed on both right and left sides of bony landmarks of the pelvis, thigh, shank, foot, shoulder, and trunk. In addition, subjects wore compression attire and performed each trial barefoot. Static calibration trials of each subject standing in the center of the capture area with arm abducted were recorded prior to capturing dynamic motion trials. These trials are necessary for documenting the position of each marker for subsequent analysis procedures. After the static calibration trials, subjects performed 4 motion trials of both NW and TW conditions.
For the NW condition, subjects began at the determined starting point at one end of the capture area and were instructed to walk across the area at a self-selected pace so that the right foot fully contacted the first force platform, and the left foot fully contacted the second force platform. For the TW condition, subjects were instructed to walk across the same area using TW gait movements so that the sequence of foot contacts with the force platform matched that of the NW condition. Data from the motion trials were obtained from the right lower extremity during right foot stance phase. Stance phase was determined by the onset of GRF at heel strike and dissolution of GRF at toe off.
Three-dimensional marker data were filtered using a 4th order, low-pass Butterworth digital filter with a cutoff of 6 Hz. Segmental Euler angles (x-y-x sequence) were computed based on the rotation matrix between global and local coordinate systems of each segment. Inverse dynamics principles were employed to calculate the EKAM using kinematic and GRF data10). EKAM moment-arm calculations were made by dividing the EKAM by the frontal plane GRF, resulting in either medial (positive) or lateral (negative) moment-arm projections. Individual trials were normalized to the time of the stance phase.
Peak medial and lateral EKAM moment-arm magnitudes, from both the NW and TW conditions, were obtained for each trial and averaged across trials for each subject. Separate paired samples t-tests were used to measure differences in peak medial and lateral moment-arm magnitudes between NW and TW. The probability value of significance was set at 0.05.
RESULTS
A significantly greater average lateral EKAM moment-arm magnitude was observed in TW (−0.0239 ± 0.011 m) compared with that in NW (−0.0057 ± 0.004 m) (p < 0.01). No significant difference was found between conditions in average medial EKAM moment-arm magnitude (NW: 0.0143 ± 0.010 m; TW: 0.0098 ± 0.014 m; p = 0.305) (Table 1).
Table 1. Medial and Lateral moment-arm means (standard deviation) during normal walking and Tai Chi walking.
| Moment-arm projection | Group moment-arm means (standard deviation) | |
|---|---|---|
| NW# | TW# | |
| Medial moment arm | 0.0143 (0.010) | 0.0098 (0.014) |
| Lateral moment arm* | −0.0057 (0.004) | −0.0239 (0.011) |
#NW: normal walking, TW: Tai Chi walking. *Lateral moment-arm magnitude was significantly less during the stance phase of Tai Chi walking than during that of normal walking.
DISCUSSION
A comparison of NW and TW moment-arm characteristics was made during the stance phase of the respective gait cycles. Results of this study showed that TW exhibited a significantly greater average lateral EKAM moment-arm magnitude compared with that of NW. Although the average medial EKAM moment-arm magnitude was greater during NW compared with that during TW, this difference was not statistically significant. These findings demonstrate that TW induced a medial to lateral EKAM moment-arm shift throughout the stance phase (Fig. 1).
Fig. 1.
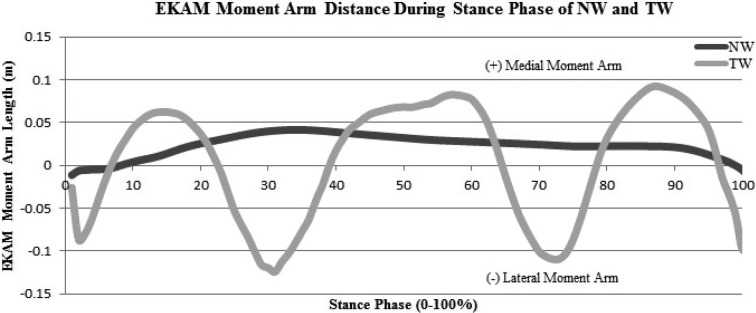
Single representative subject pattern of EKAM moment-arm length during the stance phase of normal and Tai Chi walking
Differences in EKAM moment-arm characteristics between NW and TW could be attributed to several factors. First, TW involves motion occurring in primarily the sagittal and frontal planes. The Tai Chi step occurs more lateral from the line of progression than NW, requiring greater hip abduction and overall greater lateral motion of the ankle, knee, hip, and shoulder6). Similarly, during transition from single-leg stance to heel strike of the contralateral foot, the line of progression occurs anterior-laterally, requiring further hip abduction of the target limb. This reduces the likelihood for adduction at the knee joint to occur.
Second, the single-leg stance phase exhibits a longer duration during TW, for which the subject must stabilize the lower extremity to reduce the center of mass sway. Such action is needed to reduce excess motion at the ankle, knee, and hip joints to allow smooth transition to the contralateral heel strike. Wu & Hitt7) noted that the foot center of pressure (COP) had significant media-lateral displacement during TW, with the tendency of the COP to remain toward the lateral side of the foot during the stance phase. This finding suggests that the frontal plane GRF vector would shift mediolaterally as the center of mass moves more directly over the base of support, as indicated by the mediolateral fluctuation in EKAM moment-arm projection seen in this study. Furthermore, a medial to lateral shift in moment-arm projection points to an alteration in the EKAM throughout the stance phase of TW compared with that of NW8).
Evidence of differences in the EKAM moment-arm during TW compared with those during NW supports the notion of altered motor control of the lower extremity and concurs with previous literature that noted changes in lower extremity spatiotemporal and muscle activation characteristics6). Ultimately, lower extremity muscle activation patterns during TW would likely affect the position of the limb, and thereby the position of the moment arms that contribute to external knee joint moments. These control strategies during TW could be enhanced with training11, 12) and feedback on limb positioning in space or the magnitude of loading experienced throughout the stance phase.
The limitations of this study should be noted. First, factors associated with altered medial knee joint loading during NW, such as static and dynamic knee joint alignment, body composition, and gender, should be considered during TW; these were not considered in the present study. In addition, moment-arm characteristics were not assessed in knee OA patients; thus, the results of the present study can only be generalized to adults who do not show knee OA symptoms. More studies employing TW should be conducted to better understand the biomechanical knee joint loading response in people with knee OA and assess the impact of TW as an intervention for these patients.
This is the first study to demonstrate characteristics of the frontal plane moment arm during TW in healthy populations. The results of this study confirm the hypothesis that EKAM moment-arm characteristics differ between TW and NW in healthy individuals. Medial to lateral changes in EKAM moment-arm projection suggest possible mitigation of medial knee joint loading during TW; however, further analysis is needed to better understand this relationship. The findings of this study provide a platform for future investigations of the biomechanical knee joint loading characteristics of TW, with potential clinical implications for knee OA populations.
REFERENCES
- 1.Sharma L, Hurwitz DE, Thonar EJ, et al. : Knee adduction moment, serum hyaluronan level, and disease severity in medial tibiofemoral osteoarthritis. Arthritis Rheum, 1998, 41: 1233–1240. [DOI] [PubMed] [Google Scholar]
- 2.Miyazaki T, Wada M, Kawahara H, et al. : Dynamic load at baseline can predict radiographic disease progression in medial compartment knee osteoarthritis. Ann Rheum Dis, 2002, 61: 617–622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Baliunas AJ, Hurwitz DE, Ryals AB, et al. : Increased knee joint loads during walking are present in subjects with knee osteoarthritis. Osteoarthritis Cartilage, 2002, 10: 573–579. [DOI] [PubMed] [Google Scholar]
- 4.Wang C, Schmid CH, Hibberd PL, et al. : Tai Chi is effective in treating knee osteoarthritis: a randomized controlled trial. Arthritis Rheum, 2009, 61: 1545–1553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ye J, Cai S, Zhong W, et al. : Effects of tai chi for patients with knee osteoarthritis: a systematic review. J Phys Ther Sci, 2014, 26: 1133–1137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wu G, Liu W, Hitt J, et al. : Spatial, temporal and muscle action patterns of Tai Chi gait. J Electromyogr Kinesiol, 2004, 14: 343–354. [DOI] [PubMed] [Google Scholar]
- 7.Wu G, Hitt J: Ground contact characteristics of Tai Chi gait. Gait Posture, 2005, 22: 32–39. [DOI] [PubMed] [Google Scholar]
- 8.Wu G, Millon D: Joint kinetics during Tai Chi gait and normal walking gait in young and elderly Tai Chi Chuan practitioners. Clin Biomech (Bristol, Avon), 2008, 23: 787–795. [DOI] [PubMed] [Google Scholar]
- 9.Hunt MA, Birmingham TB, Giffin JR, et al. : Associations among knee adduction moment, frontal plane ground reaction force, and lever arm during walking in patients with knee osteoarthritis. J Biomech, 2006, 39: 2213–2220. [DOI] [PubMed] [Google Scholar]
- 10.Winter DA: Biomechanics and Motor Control of Human Movement, 3rd ed. New York: John Wiley & Sons, 2005. [Google Scholar]
- 11.Jacobson BH, Chen HC, Cashel C, et al. : The effect of T’ai Chi Chuan training on balance, kinesthetic sense, and strength. Percept Mot Skills, 1997, 84: 27–33. [DOI] [PubMed] [Google Scholar]
- 12.Kim HD, Je HD, Jeong JH, et al. : Effects of Tai Chi training on obstacle avoidance and gait initiation by older people. J Phys Ther Sci, 2013, 25: 193–198. [Google Scholar]