

Abstract
Kaatsu training is an exercise method involving the application of pressure to the target muscle, and is being increasingly used in rehabilitation programs for heart disease patients in some hospitals. This method restricts blood flow to the muscles during exercise, and the resultant hypoxia effectively causes muscle hypertrophy and strengthening. However, no medical guidelines or risk factors for its use have been established.
We report a case involving a 45-year-old man who suffered from 2 episodes of central retinal vein occlusion (CRVO), both occurring on the day following a Kaatsu training session.
As a characteristic of the CRVO and its subsequent complications, the affected eye lost vision despite treatment. The patient had a history of hypertension and diabetes, and thus was at an increased risk of CRVO. Kaatsu training, which changes the heart rate and serum growth hormone levels, may have triggered the onset of CRVO.
This case highlights that underlying medical conditions such as hypertension, diabetes, and the consequent inflammation, could be risk factors for vascular side effects resulting from Kaatsu training. Further studies are required before the medical and recreational use of Kaatsu training become widespread.
INTRODUCTION
To achieve effective muscle hypertrophy with less exercise, a training method involving application of pressure to the target muscle, named Kaatsu training, was developed, and is now used in rehabilitation programs for heart disease patients in some hospitals. In this method, the muscles are tightly wrapped during exercise, thereby restricting blood flow, and the resultant hypoxia causes hypertrophy and a gain in strength.1 Several societies, including the American College of Sports Medicine, have published guidelines for the Kaatsu training program to effectively obtain efficient muscle hypertrophy and strength.2 However, there are presently no medical guidelines or published risk factors for its use.
Kaatsu training is a low-intensity resistant training method that is combined with restricted venous blood flow from the working muscle achieved by compressing the vasculature proximal to the exercising muscles using a dedicated device.1 The belt pressure reaches over 200 mmHg during this training. This pressure has been suggested to restrict venous blood flow and cause pooling of the blood in the capacitance vessels distal to the belt, while simultaneously restricting arterial blood flow.3,4 Under this condition, the muscle-bone cross-sectional area measured in magnetic resonance imaging was found to be increased compared with control training without applying pressure to the target muscle.1 However, at the same time, the heart rate was significantly increased immediately after starting the Kaatsu training compared with the control training.1 Thus, Kaatsu training may cause unexpected adverse events in organs and/or tissues other than the target muscle.
To highlight the potential risks of the application of Kaatsu training in some specific cases, we here report a case of central retinal vein occlusion (CRVO), a vision-threatening retinal disease, that occurred following Kaatsu training. CRVO often occurs in patients with hypertension5 and is associated with an increased risk of cardiovascular diseases.6 The main findings associated with CRVO are widespread retinal hemorrhage, resulting in edema in the central part of the retina (macular edema), and retinal ischemia. The ischemic change may cause abnormal vessel proliferation, which often subsequently causes intraocular massive hemorrhage and/or neovascular glaucoma as the most severe complications of CRVO.
CASE REPORT
A 45-year-old man, who had been seen by us previously for diabetic retinopathy follow-up (Figure 1A), presented with sudden impairment of best-corrected visual acuity (BCVA) in his left eye due to CRVO (Figure 1B). Severe edema and ischemic changes, as well as hemorrhage in the macula, induced a sudden loss in vision from 20/20 to 20/200. The patient was given a local steroid injection to reduce the macular edema and pan-retinal photocoagulation to prevent neovascularization and related eye complications. He gradually recovered his visual acuity as the macular edema decreased; however, 2 months later, he complained of further visual impairment (BCVA, 6/200) due to a recurrence of CRVO (Figure 1C). At this point, the hemorrhage was more severe than the first event, and he subsequently suffered from severe vitreous hemorrhage. Pars plana vitrectomy and additional extensive pan-retinal photocoagulation were administered; however, in spite of the treatment, the intraocular pressure elevated to 45 mmHg due to secondary neovascular glaucoma to CRVO, which was uncontrollable both with medications and surgery for glaucoma (trabeculectomy). Finally, his visual acuity was further reduced to only light perception.
FIGURE 1.
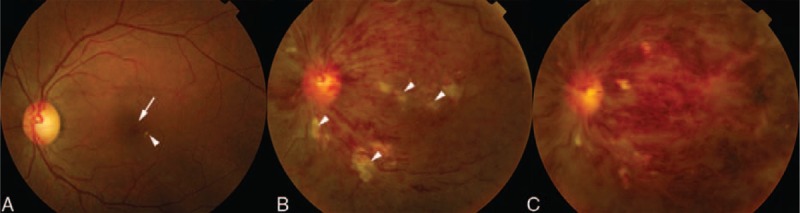
Central retinal vein occlusion (CRVO) photographs of the fundus. (A) Before the onset of CRVO. Simple diabetic retinopathy indicated by a small retinal hemorrhage and hard exudates (arrowhead) was observed. The arrow shows the macular region. (B) CRVO. Retinal hemorrhage spread throughout the retina. Soft exudates (arrowheads), indicating retinal ischemia, were obvious. Edema could be seen in the macular region. (C) Recurrence of CRVO. The retinal hemorrhage and macular edema increased.
The patient had asymptomatic simple diabetic retinopathy, although his blood glucose level was moderately controlled at his first visit (HbA1c, 6.4%), as well as high blood pressure (145 mmHg [systolic]/105 mmHg [diastolic]), although he had not received a diagnosis of hypertension or any medicine for this condition. We eventually learned that the patient had taken up the habit of Kaatsu training, and had undergone a training session on the day before both his first onset and the recurrence. This study followed the tenets of the Declaration of Helsinki and was approved by the Ethics Committee of Keio University School of Medicine. Informed consent was given by the patient.
DISCUSSION
Both of the events in this case were preceded by a session of Kaatsu training. This training regimen tends to drastically increase the heart rate and blood pressure at the peak of exercise.7 This may be at least partly due to the fact that Kaatsu training immediately causes an increased serum level of growth hormone, which is a pressure-raising hormone.7 Thus, substantial changes to the systemic condition occur during Kaatsu training, although compression is only applied to a specific target muscle. Even under resting conditions, the patient's blood pressure met the criteria for hypertension, and it may have been elevated further during Kaatsu training. The patient also had diabetes, which causes hyperviscosity induced by high glucose and diabetic microangiopathy, and can easily induce abnormal turbulent flow, thereby increasing the risk factor for endoluminal thrombus formation.8 In fact, the major risk factors for retinal vein occlusion are a high hematocrit level as well as hypertension.5 In addition, various inflammatory cytokines that induce the abnormal adhesion of leukocytes and/or platelets may have been upregulated owing to the patient's diabetes and hypertension. Under these conditions, the repeated circulatory changes caused by Kaatsu training may have exacerbated deep vein thrombosis, and ultimately triggered serious vein occlusions.
Kaatsu training is now used as a rehabilitative program for heart disease patients or as a general training program. The risk of injury related to the high-intensity resistance training required for achieving muscle hypertrophy and strength gain may be reduced by using Kaatsu training, which involves low-intensity resistance training.1 However, as the present case demonstrates, Kaatsu training may also cause side effects in distant tissues and/or organs by inducing circulatory changes. This case illustrates that underlying medical conditions such as hypertension, diabetes, and the inflammation associated with these diseases could be risk factors for vascular side effects during Kaatsu training.
We propose that people who practice Kaatsu training should carefully monitor their general condition, including their blood pressure, during and after training, and that a person with a chronic underlying disease should carefully consider whether or not to use Kaatsu. This case clearly demonstrates that the influence of Kaatsu training should be further studied from various medical viewpoints before its medical and recreational use becomes more widespread.
Acknowledgements
The authors thank all the medical staff in our clinic for technical assistance.
Footnotes
Abbreviations: BCVA = best-corrected visual acuity, CRVO = central retinal vein occlusion.
This case was reported according to the tenets of the Declaration of Helsinki.
The authors report no conflicts of interest.
REFERENCES
- 1.Abe T, Kearns CF, Sato Y. Muscle size and strength are increased following walk training with restricted venous blood flow from the leg muscle, Kaatsu-walk training. J Appl Physiol 2006; 100:1460–1466. [DOI] [PubMed] [Google Scholar]
- 2.American College of Sports Medicine Position Stand. The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness, and flexibility in healthy adults. Med Sci Sports Exerc 1998; 30:975–991. [DOI] [PubMed] [Google Scholar]
- 3.Burgomaster KA, Moore DR, Schofield LM, et al. Resistance training with vascular occlusion: metabolic adaptations in human muscle. Med Sci Sports Exerc 2003; 35:1203–1208. [DOI] [PubMed] [Google Scholar]
- 4.Takarada Y, Takazawa H, Sato Y, et al. Effects of resistance exercise combined with moderate vascular occlusion on muscular function in humans. J Appl Physiol 2000; 88:2097–2106. [DOI] [PubMed] [Google Scholar]
- 5.Takarada Y, Takazawa H, Ishii N. Applications of vascular occlusion diminish disuse atrophy of knee extensor muscles. Med Sci Sports Exerc 2000; 32:2035–2039. [DOI] [PubMed] [Google Scholar]
- 6.Takarada Y, Nakamura Y, Aruga S, et al. Rapid increase in plasma growth hormone after low-intensity resistance exercise with vascular occlusion. J Appl Physiol (1985) 2000; 88:61–65. [DOI] [PubMed] [Google Scholar]
- 7.Takano H, Morita T, Iida H, et al. Hemodynamic and hormonal responses to a short-term low-intensity resistance exercise with the reduction of muscle blood flow. Eur J Appl Physiol 2005; 95:65–73. [DOI] [PubMed] [Google Scholar]
- 8.Hayreh SS, Zimmerman B, McCarthy MJ, et al. Systemic diseases associated with various types of retinal vein occlusion. Am J Ophthalmol 2001; 131:61–77. [DOI] [PubMed] [Google Scholar]