

Abstract
In the present study, we aimed to verify associations between ambulatory blood pressure (ABP) and pediatric obstructive sleep apnea (OSA) in a hospital-based population.
This was a cross-sectional observational study on children aged 4 to 16 years with OSA-related symptoms from a tertiary referral medical center. All children received overnight polysomnography and 24-hour recording of ABP. Severity of the disease was classified as primary snoring (apnea-hypopnea index, AHI <1), mild OSA (AHI 1–5), and moderate-to-severe OSA (AHI >5).
For 195 children enrolled in this study (mean age, 7.8 ± 3.4 years; 69% boy), ABP increased as severity of OSA increased. During daytime, children with moderate-to-severe OSA had significantly higher systolic blood pressure (BP) (117.0 ± 12.7 vs 110.5 ± 9.3 mmHg), mean arterial pressure (MAP) (85.6 ± 8.1 vs 81.6 ± 6.8 mmHg), and diastolic BP load (12.0 ± 9.6 vs 8.4 ± 10.9 mmHg) compared with children with primary snoring. During nighttime, children with moderate-to-severe OSA had significantly higher systolic BP (108.6 ± 15.0 vs 100.0 ± 9.4 mmHg), MAP (75.9 ± 9.6 vs 71.1 ± 7.0 mmHg), systolic BP load (44.0 ± 32.6 vs 26.8 ± 24.5 mmHg), systolic BP index (0.5 ± 13.1 vs −6.8 ± 8.5 mmHg), and higher prevalence of systolic hypertension (47.6% vs 14.7 %) compared with children with primary snoring. Multiple linear regression analyses revealed an independent association between AHI and nighttime systolic BP and MAP after adjusting for adiposity variables.
This large hospital-based study showed that children with moderate-to-severe OSA had a higher ABP compared with children who were primary snorers. As elevated BP in childhood predicts future cardiovascular risks, children with severe OSA should be treated properly to prevent further adverse cardiovascular outcomes.
INTRODUCTION
Sleep-disordered breathing includes a spectrum of upper airway disorders ranging from primary snoring to obstructive sleep apnea (OSA).1,2 In adults, untreated OSA is associated with hypertension3,4 and other cardiovascular morbidities.5,6 In children, Guilleminault et al7 first described high blood pressure (BP) with OSA in 1976. Since then, several studies have linked OSA with BP in a pediatric population.7–12 Although some studies have reported a trend of elevated BP in children with OSA,7–12 a recent meta-analysis by Zintzaras et al13 reported that evidence of an association between moderate-to-severe childhood OSA and hypertension is insufficient. As the literature show inconsistent results regarding associations between BP and pediatric OSA, further studies are needed to clarify this clinical relevant issue.
Ambulatory blood pressure (ABP) monitoring is a standard diagnostic tool for BP measurements because of high reliability and reproducibility. Monitoring ABP provides an estimate of mean BP level, the diurnal rhythm of BP, and BP variability. Several studies have shown that ABP monitoring, when compared with clinic casual BP measurements, is superior in predicting target organ damage, morbid events, or cardiovascular risk.14 However, few studies have used ABP monitoring to elucidate associations between BP and OSA in children.8–12 Furthermore, obesity increases risk of pediatric OSA.2,15 Obesity in children can also cause hypertension, which ultimately increases cardiovascular risks.16,17 Previous studies have used a small sample size and have not considered the independent role of childhood OSA on BP.8–12,18
The aims of this study were to compare ABP level in children with OSA of varying severity (ie, primary snoring, mild, moderate-to-severe OSA) and to investigate the association between childhood OSA and BP parameters.
MATERIALS AND METHODS
Study Population
Children aged 4 to 16 years with symptoms suggestive of OSA, including snoring, excessive daytime sleepiness, or breathing pauses reported by parents who were referred to the National Taiwan University Hospital, were recruited from the respiratory (P-LL), pediatric (W-CC), and otolaryngologic clinics (W-CH) between September 2012 and March 2015.19 Approval for this study was obtained from the Ethics Committee of National Taiwan University Hospital, and written informed consent was obtained from each participant or their parents. Basic data, clinical history, and physical examination data were obtained by the corresponding author.
The weight and height of each child were measured. Age- and sex-corrected body mass index (BMI) was applied using established guidelines to convert BMI into BMI percentile.20 Obesity was defined as age- and sex-corrected BMI >95th percentile.2,20 Exclusion criteria included the following: children with craniofacial abnormalies, genetic disorders, or neuromuscular diseases; children who had previously received tonsillectomy or adenoidectomy; significant medical illnesses such as respiratory or cardiac disease.
Polysomnography
Overnight polysomnography (PSG) study (Embla N7000, Reykjavik, Iceland) was performed in the sleep center of the National Taiwan University Hospital.2,15,18,19,21–26 The sleep parameters were scored according to the 2007 American Academy of Sleep Medicine standards.27 Briefly, apnea was defined as ≥90% decrease in airflow and hypopnea was a ≥50% decrease in airflow associated with reduced arterial oxygen saturation in ≥3% or an arousal for duration of ≥2 breaths. Disease severity in children was further characterized as primary snoring (apnea-hypopnea index, AHI <1/h), mild OSA (AHI 1–5/h), and moderate-to-severe OSA (AHI ≥5/h).21–26
24-Hour ABP
All participants received 24-hour ABP monitoring using the Oscar 2 oscillometric monitor (SunTech Medical, Model 222, Morrisville, NC), which has been validated by the International Protocol of the European Society of Hypertension and British Hypertension Society.28,29 Measurements were obtained with the appropriately sized cuff on the nondominant arm. Participants were asked to maintain their usual activity but to remain still during daytime measurements. The monitors were programmed for daytime (7 am to 10 pm) measurements of BP at 15-minute intervals and for nighttime (10 pm to 7 am) measurements of BP at 30-minute intervals. The cutoff for daytime and nighttime was defined according to the sleep diary derived from parents or children. Extreme outlier BP readings were assumed to be invalid and were discarded as artifacts. Therefore, visual inspections of grossly inconsistent readings were made before interpretation, and only measurements with systolic BP <240 and >70 mmHg, diastolic BP <140 and >40 mmHg, heart rate <125 beats/min, and pulse pressure >40 but <100 mmHg with a diastolic BP <systolic BP were considered valid.30
Mean systolic, diastolic BP, and mean arterial pressure (MAP) were calculated for daytime and nighttime. The BP load was defined as percentage of valid BP measurements >95th percentile of BP for age and sex. Different age and sex groups were compared by applying the BP index.30 The BP index was calculated by using the following formula: BP index = (measured BP – 95th percentile)/95th percentile × 100.12 Hypertension was defined as mean SBP or DBP values > 95th percentile of the ABP norm.30
Nocturnal dipping of systolic and diastolic BP was calculated as the difference between mean daytime and nighttime BP and expressed as a percentage of dipping. Subjects with nocturnal BP dipping <10% were defined as nondippers.
Statistical Analysis
Data were analyzed using IBM SPSS Statistics 20.0 (IBM Corporation, New York, NY). Continuous data were expressed as the mean and standard deviation, and categorical data were expressed as the number and percentage. The distribution of continuous variables among the disease severity groups was compared by Kruskal-Wallis test with Bonferroni post hoc multiple comparison when the overall test was significant. Differences in proportions between groups were examined with the Fisher exact test. The association between the sleep parameter (ie, AHI) and BP measurements was investigated by multivariable linear regression analysis. The AHI values were logarithmically transformed (natural log [x +0.1]) because its distribution was skewed and contained zero. Several models were constructed to evaluate associations between AHI and BP parameters with adjustment for age, sex, height, and adiposity (ie, BMI, BMI percentile, and obesity). A P value <0.05 was considered statistically significant.
RESULTS
Demographics
From September 2012 to March 2015, children with symptoms suggestive of OSA were invited to participate. The final analysis included 195 subjects who had overnight PSG data and ABP measurements. Mean age was 7.8 ± 3.4 years; 69.0% (134/195) were male. For OSA groups, 17.4% (34/195) had primary snoring (AHI <1), 39.5% (77/195) had mild OSA (5 ≥ AHI >1), and 43.1% (84/195) had moderate-to-severe OSA (AHI >5). Table 1 compares the basic characteristics and PSG data among children with different disease severity. Children with moderate-to severe OSA had a higher BMI, BMI percentile, and the prevalence of obesity than that of primary snoring children. Children with mild OSA had a higher BMI percentile than that of primary snorers. Not surprisingly, children with higher AHI levels also had a significantly higher oxygen desaturation index, arousal index, and lower mean and minimum oxygen saturation.
TABLE 1.
Demographic, Anthropometric, and Polysomnographic Data

BP During Daytime
During daytime, children with moderate-to-severe OSA had significantly higher systolic BP (117.0 ± 12.7 vs 110.5 ± 9.3 mmHg), mean arterial pressure (MAP) (85.6 ± 8.1 vs. 81.6 ± 6.8 mmHg), and diastolic BP load (12.0 ± 9.6 vs. 8.4 ± 10.9 mmHg) compared with children with primary snoring. However, systolic and diastolic BP index did not significantly differ among OSA subgroups. Additionally, the daytime prevalence of systolic and diastolic hypertension did not significantly differ among the OSA subgroups (Table 2) (Figs. 1–3).
TABLE 2.
24-Hour Ambulatory Blood Pressure in OSA Subgroups

FIGURE 1.
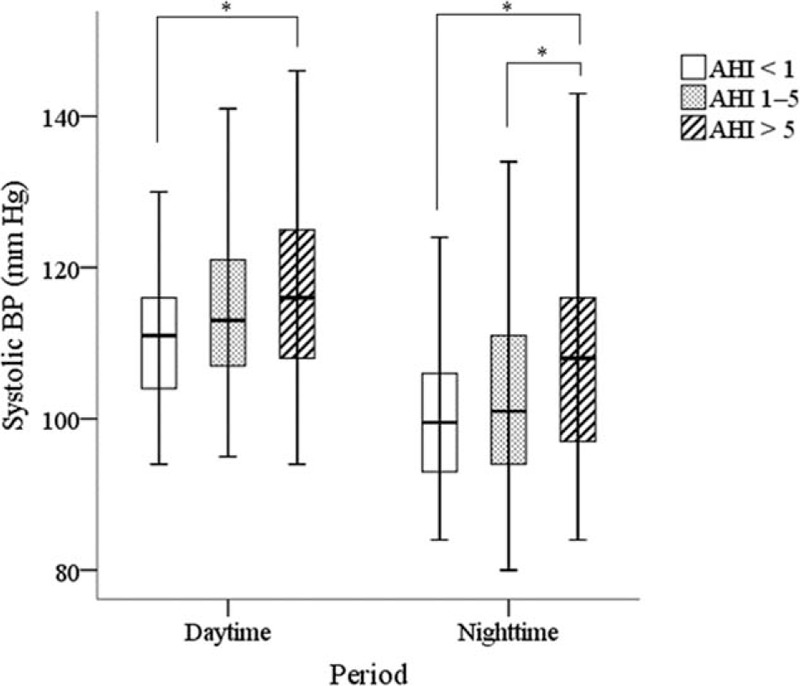
Systolic BP during different periods for OSA subgroups. ∗Post hoc test, P < 0.05. BP = blood pressure, OSA = obstructive sleep apnea.
FIGURE 3.
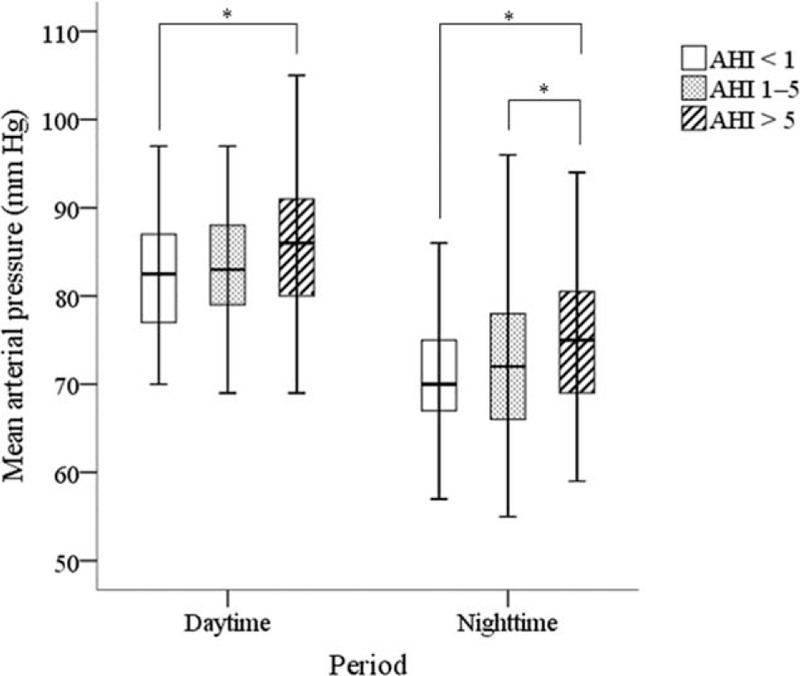
Mean arterial pressure during different periods for OSA subgroups. ∗Post hoc test, P < 0.05. BP = blood pressure, OSA = obstructive sleep apnea.
FIGURE 2.
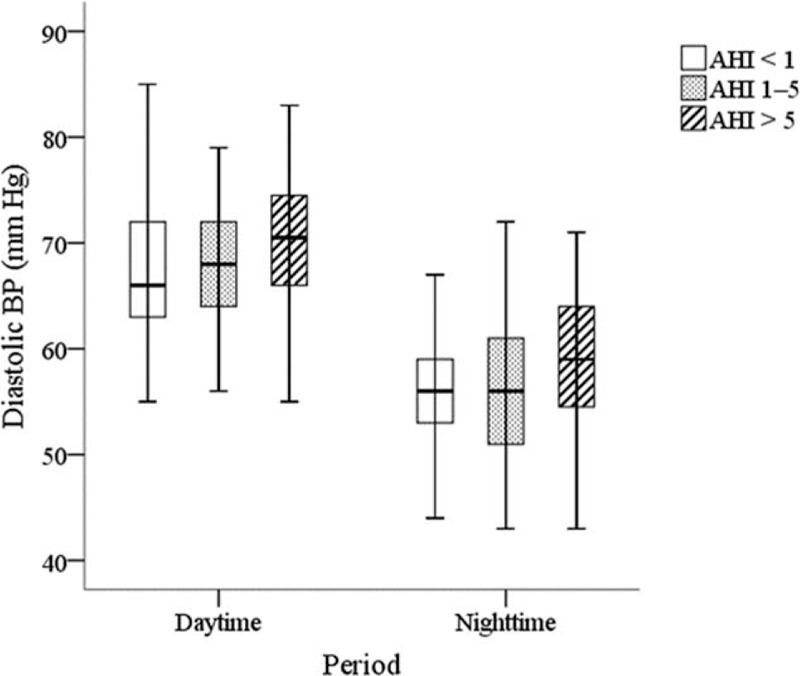
Diastolic BP during different periods for OSA subgroups. ∗Post hoc test, P < 0.05. BP = blood pressure, OSA = obstructive sleep apnea.
Blood Pressure During Nighttime
During nighttime, children with moderate-to-severe OSA had significantly higher systolic BP (108.6 ± 15.0 vs 100.0 ± 9.4 mmHg), MAP (75.9 ± 9.6 vs 71.1 ± 7.0 mmHg), pulse pressure (49.2 ± 10.4 vs 43.4 ± 6.1 mmHg), systolic BP load (44.0 ± 32.6 vs 26.8 ± 24.5 mmHg), systolic BP index (0.5 ± 13.1 vs −6.8 ± 8.5 mmHg), and prevalence of systolic hypertension (47.6 vs. 14.7 %) compared to primary snoring children. Table 2 shows that children with moderate-to-severe OSA had significantly higher systolic BP (108.6 ± 15.0 vs 103.0 ± 13.3 mmHg), MAP (75.9 ± 9.6 vs 72.3 ± 9.2 mmHg), systolic BP load (44.0 ± 32.6 vs 30.6 ± 29.3 mmHg), and systolic BP index (0.5 ± 13.1 vs −4.2 ± 12.4 mmHg) compared with children with mild OSA (Figs. 1–3).
Nocturnal BP Dipping
Compared with those with mild OSA, children with moderate-to-severe OSA had significantly lower systolic nocturnal BP dipping (7.1 ± 8.6 vs 10.0 ± 7.8 mmHg). However, diastolic nocturnal BP and the proportion of nondippers did not significantly differ among the 3 OSA subgroups (Table 2).
Multivariable Linear Regression Analyses
Multiple linear regression models were used to explore associations between AHI and BP parameters after adjusting for possible confounders (ie, age, sex, height, and adiposity variables) (Table 3). Unadjusted analysis showed the AHI was positively correlated with daytime systolic BP, daytime MAP, nighttime systolic BP, nighttime diastolic BP, and nighttime MAP. Associations between AHI and daytime BP parameters were partially affected by adiposity, whereas AHI correlated positively with nighttime systolic BP and MAP after adjusting possible confounders.
TABLE 3.
Multivariable Linear Regression Analyses of the Association Between AHI (in Log Scale) and BP Parameters After Adjustment of Possible Confounders

DISCUSSION
This large, hospital-based study elaborates associations between ABP and OSA in children. Analytical results show that children with OSA had elevated ABP with increased disease severity. In this study cohort, children with moderate-to-severe OSA had significantly higher daytime systolic BP and diastolic BP load compared with primary snorers. In children with moderate-to-severe OSA, nighttime systolic BP, systolic BP load, and systolic BP index were also significantly higher compared with primary snorers. The effect of OSA on nighttime BP is independent of obesity. These findings provide robust evidence that, in children with OSA, BP is higher in those who are primary snorers. From a clinical perspective, elevated BP in childhood predicts future cardiovascular risks.31–32 Therefore, children with severe OSA require monitoring of cardiovascular parameters and proper treatment to prevent further adverse cardiovascular consequences.
In children, Guilleminault et al7 first linked OSA to elevated BP.7–12 However, a meta-analysis by Zintzaras et al13 offered insufficient evidence that moderate-to-severe OSA was associated with hypertension, a finding that may be confounded by a small sample size and large heterogeneity among studies. In contrast, many recent studies demonstrated a trend of elevated BP in children with OSA.8–12,33–35 Li et al8 and Xu et al12 reported a dose-response relationship between OSA and BP in children. Horne et al35 indicated that pediatric OSA increased BP during sleep more than in control, regardless of OSA severity. Weber et al11 showed that children with OSA had higher diastolic and mean BP compared with those of primary snoring. The present study found that moderate-to-severe OSA was associated with elevated BP during daytime and nighttime. In children, OSA also had a strong correlation with systolic BP during nighttime, and the correlation was independent of obesity. These findings indicate that childhood OSA is associated with elevated BP. Interestingly, the prevalence of non-dippers in this study did not significantly differ among OSA subgroups. However, children with moderate-to-severe OSA had less systolic nocturnal dipping. Previously, Li et al, Horne et al, and Nisbet et al observed that nocturnal dipping is preserved in young children with OSA.8,36,37 But Weber et al11 demonstrated children with OSA had decreased degree of nocturnal dipping. In these children, exposure to the effects of OSA was sufficiently long or the disease severity was sufficiently high to affect nocturnal dipping profiles. Therefore, OSA and cardiovascular effects may be resolved when appropriate treatment is administrated.
Impacts of pediatric OSA on cardiovascular effects have received increasing attention.31–43 Evidence of autonomic dysfunction was found in children with OSA during both wakefulness and sleep.33–35 Moreover, BP dysregulation, elevated sympathetic activity and impairment of autonomic reflexes occur in school-aged children and adolescents with OSA.39–42 Notably, cardiovascular consequences of OSA occur not only in children with OSA, but also in children with primary snoring.43 This hospital-based study recruited participants with clinical symptoms. Therefore, cardiovascular comparisons between children with OSA and normal controls were not obtained.
High BP in adulthood is a well-established risk factor for early disability and death.44 Although BP levels in childhood cannot be directly linked with cardiovascular events in adults, a number of studies have reported that intermediate markers of target organ damage, including left ventricular hypertrophy, atherosclerosis, or cognitive dysfunction, are detectable in children and adolescents with elevated BP.31,32,45–47 Importantly, elevated BP in children continues into adulthood and is often associated with modifiable risk factors such as lack of physical activity, obesity, and sleep problems.31,32,48,49 If the diagnosis of high BP is not made, associated risk factors are unlikely to decrease. This study highlighted correlations between increased BP and OSA in children, implying early awareness and proper treatment should be considered in this category of patients to prevent further cardiovascular complications.
This study has certain limitations. First, this study lacked a normal control group.50 In this hospital-based study, primary snorers were the comparison group. However, children who are primary snorers are not considered innocent anymore,51 and evidence exists that children with primary snoring had higher BP levels compared with normal controls.43 Second, this study was a cross-sectional study. Further longitudinal, prospective studies are needed to elucidate long-term changes of OSA and its association with BP.52–55 Third, this study did not link BP with other cardiovascular measurements, and evidence of early target-organ damage in children with OSA was not obtained.56 Finally, because of the lack of normal BP reference in Taiwanese children, this study used normative data for the US population.30 Future studies should examine effect of treatment on BP in children with sleep disturbances.18,57–60
CONCLUSIONS
This large, hospital-based study shows that daytime and nighttime BP levels elevated with increased severity of OSA in children. Compared with children with primary snoring, those with moderate-to-severe OSA had a significantly higher BP. This study identified a correlation between OSA severity and nighttime BP, and the correlation was independent of obesity. Since elevated BP in childhood predicts future cardiovascular risks, children with OSA and hypertension should receive proper treatment to prevent further adverse cardiovascular consequences. Further studies are needed to elucidate the impacts of surgery or other treatment strategies on BP parameters in children with obstructive sleep disorders.
Acknowledgments
The authors thank Staff of the Center of Sleep Disorder, National Taiwan University Hospital for their technical support; M-JW and W-CY for their assistance in BP machine setting and data collection. We are grateful for the cooperation and participation of all of the children and their parents.
This study was supported by grant MOST 103-2511-S-002-002-MY2 from Ministry of Science and Technology, R.O.C. (Taiwan). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. No additional external funding was received for this study.
Footnotes
Abbreviations: ABP = ambulatory blood pressure, AHI = apnea-hypopnea index, BMI = body mass index, BP = blood pressure, MAP = mean arterial pressure, OSA = obstructive sleep apnea, PSG = polysomnography.
Author contributions: K-TK, study concept and design, acquisition of data, analysis and interpretation of data, drafting of the manuscript, statistical analysis; S-NC, acquisition of data, analysis and interpretation of data, statistical analysis, revising manuscript critically for important intellectual content; W-CW, acquisition of data, critical revision of the manuscript for important intellectual content; P-LL, acquisition of data, critical revision of the manuscript for important intellectual content; W-CH, takes responsibility for the content of the article, study concept and design, acquisition of data, analysis and interpretation of data, drafting of the manuscript, critical revision of the manuscript for important intellectual content.
The authors declare no conflicts of interest.
REFERENCES
- 1.Marcus CL, Brooks LJ, Draper KA, et al. American Academy of Pediatrics Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2012; 130:e714–e755. [DOI] [PubMed] [Google Scholar]
- 2.Kang KT, Lee PL, Weng WC, et al. Body weight status and obstructive sleep apnea in children. Int J Obes (Lond) 2012; 36:920–924. [DOI] [PubMed] [Google Scholar]
- 3.Peppard PE, Young T, Palta M, et al. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med 2000; 342:1378–1384. [DOI] [PubMed] [Google Scholar]
- 4.Marin JM, Agusti A, Villar I, et al. Association between treated and untreated obstructive sleep apnea and risk of hypertension. JAMA 2012; 307:2169–2176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Yaggi HK, Concato J, Kernan WN, et al. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med 2005; 353:2034–2041. [DOI] [PubMed] [Google Scholar]
- 6.Loke YK, Brown JW, Kwok CS, et al. Association of obstructive sleep apnea with risk of serious cardiovascular events: a systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes 2012; 5:720–728. [DOI] [PubMed] [Google Scholar]
- 7.Guilleminault C, Eldridge FL, Simmons FB, et al. Sleep apnea in eight children. Pediatrics 1976; 58:23–30. [PubMed] [Google Scholar]
- 8.Li AM, Au CT, Sung RY, et al. Ambulatory blood pressure in children with obstructive sleep apnoea: a community based study. Thorax 2008; 63:803–809. [DOI] [PubMed] [Google Scholar]
- 9.Amin RS, Carroll JL, Jeffries JL, et al. Twenty-four-hour ambulatory blood pressure in children with sleep-disordered breathing. Am J Respir Crit Care Med 2004; 169:950–956. [DOI] [PubMed] [Google Scholar]
- 10.Leung LC, Ng DK, Lau MW, et al. Twenty-four-hour ambulatory BP in snoring children with obstructive sleep apnea syndrome. Chest 2006; 130:1009–1017. [DOI] [PubMed] [Google Scholar]
- 11.Weber SA, Santos VJ, Semenzati Gde O, et al. Ambulatory blood pressure monitoring in children with obstructive sleep apnea and primary snoring. Int J Pediatr Otorhinolaryngol 2012; 76:787–790. [DOI] [PubMed] [Google Scholar]
- 12.Xu Z, Li B, Shen K. Ambulatory blood pressure monitoring in chinese children with obstructive sleep apnea/hypopnea syndrome. Pediatr Pulmonol 2013; 48:274–279. [DOI] [PubMed] [Google Scholar]
- 13.Zintzaras E, Kaditis AG. Sleep-disordered breathing and blood pressure in children: a meta-analysis. Arch Pediatr Adolesc Med 2007; 161:172–178. [DOI] [PubMed] [Google Scholar]
- 14.Pickering TG, Shimbo D, Haas D. Ambulatory blood-pressure monitoring. N Engl J Med 2006; 354:2368–2374. [DOI] [PubMed] [Google Scholar]
- 15.Hsu WC, Kang KT, Weng WC, et al. Impacts of body weight after surgery for obstructive sleep apnea in children. Int J Obes (Lond) 2013; 37:527–531. [DOI] [PubMed] [Google Scholar]
- 16.Friedemann C, Heneghan C, Mahtani K, et al. Cardiovascular disease risk in healthy children and its association with body mass index: systematic review and meta-analysis. BMJ 2012; 345:e4759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rosner B, Cook NR, Daniels S, et al. Childhood blood pressure trends and risk factors for high blood pressure: the NHANES experience 1988–2008. Hypertension 2013; 62:247–254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kuo YL, Kang KT, Chiu SN, et al. Blood pressure after surgery among obese and non-obese children with obstructive sleep apnea. Otolaryngol Head Neck Surg 2015; 152:931–940. [DOI] [PubMed] [Google Scholar]
- 19.Kang KT, Weng WC, Lee CH, et al. Detection of pediatric obstructive sleep apnea syndrome: history or anatomical findings? Sleep Med 2015; 16:617–624. [DOI] [PubMed] [Google Scholar]
- 20.Chen W, Chang MH. New growth charts for Taiwanese children and adolescents based on World Health Organization standards and health-related physical fitness. Pediatr Neonatol 2010; 51:69–79. [DOI] [PubMed] [Google Scholar]
- 21.Kang KT, Weng WC, Yeh TH, et al. Validation of the Chinese version OSA-18 quality of life questionnaire in Taiwanese children with obstructive sleep apnea. J Formos Med Assoc 2014; 113:454–462. [DOI] [PubMed] [Google Scholar]
- 22.Chou CH, Kang KT, Weng WC, et al. Central sleep apnea in obese children with sleep disordered breathing. Int J Obes (Lond) 2014; 38:27–31. [DOI] [PubMed] [Google Scholar]
- 23.Kang KT, Chou CH, Weng WC, et al. Associations between Adenotonsillar hypertrophy, age, and obesity in children with obstructive sleep apnea. PLoS One 2013; 8:e78666. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kang KT, Weng WC, Lee CH, et al. Discrepancy between objective and subjective outcomes after adenotonsillectomy in children with obstructive sleep apnea syndrome. Otolaryngol Head Neck Surg 2014; 151:150–158. [DOI] [PubMed] [Google Scholar]
- 25.Lee CH, Kang KT, Weng WC, et al. Quality of life after adenotonsillectomy for children with sleep-disordered breathing: a linear mixed model analysis. Int J Pediatr Otorhinolaryngol 2014; 78:1374–1380. [DOI] [PubMed] [Google Scholar]
- 26.Lee CH, Kang KT, Weng WC, et al. Quality of life after adenotonsillectomy in children with obstructive sleep apnea: short-term and long-term results. Int J Pediatr Otorhinolaryngol 2015; 79:210–215. [DOI] [PubMed] [Google Scholar]
- 27.Iber C, Ancoli-Israel S, Chesson AL, Jr, et al. The AASM Manual for the scoring of sleep and associated events. Darien, IL:American Academy of Sleep Medicine; 2007. [Google Scholar]
- 28.Jones SC, Bilous M, Winship S, et al. Validation of the OSCAR 2 oscillometric 24-hour ambulatory blood pressure monitor according to the International Protocol for the validation of blood pressure measuring devices. Blood Press Monit 2004; 9:219–223. [DOI] [PubMed] [Google Scholar]
- 29.Goodwin J, Bilous M, Winship S, et al. Validation of the Oscar 2 oscillometric 24-h ambulatory blood pressure monitor according to the British Hypertension Society protocol. Blood Press Monit 2007; 12:113–117. [DOI] [PubMed] [Google Scholar]
- 30.Urbina E, Alpert B, Flynn J, et al. Ambulatory blood pressure monitoring in children and adolescents: recommendations for standard assessment–a scientific statement from the American Heart Association Atherosclerosis, Hypertension, and Obesity in Youth Committee of the Council on Cardiovascular Disease in the Young and the Council for High Blood Pressure Research. Hypertension 2008; 52:433–451. [DOI] [PubMed] [Google Scholar]
- 31.Aglony M, Acevedo M, Ambrosio G. Hypertension in adolescents. Expert Rev Cardiovasc Ther 2009; 7:1595–1603. [DOI] [PubMed] [Google Scholar]
- 32.Falkner B, Lurbe E, Schaefer F. High blood pressure in children: clinical and health policy implications. J Clin Hypertens (Greenwich) 2010; 12:261–276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Amin R, Somers VK, McConnell K, et al. Activity-adjusted 24-hour ambulatory blood pressure and cardiac remodeling in children with sleep disordered breathing. Hypertension 2008; 51:84–91. [DOI] [PubMed] [Google Scholar]
- 34.Kirk V, Midgley J, Giuffre M, et al. Hypertension and obstructive sleep apnea in Caucasian children. World J Cardiol 2010; 2:251–256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Horne RS, Yang JS, Walter LM, et al. Elevated blood pressure during sleep and wake in children with sleep-disordered breathing. Pediatrics 2011; 128:e85–e92. [DOI] [PubMed] [Google Scholar]
- 36.Horne RS, Yang JS, Walter LM, et al. Nocturnal dipping is preserved in children with sleep disordered breathing regardless of its severity. Pediatr Pulmonol 2013; 48:1127–1134. [DOI] [PubMed] [Google Scholar]
- 37.Nisbet LC, Nixon GM, Yiallourou SR, et al. Sleep-disordered breathing does not affect nocturnal dipping, as assessed by pulse transit time, in preschool children: evidence for early intervention to prevent adverse cardiovascular effects? Sleep Med 2014; 15:464–471. [DOI] [PubMed] [Google Scholar]
- 38.Tan HL, Gozal D, Kheirandish-Gozal L. Obstructive sleep apnea in children: a critical update. Nat Sci Sleep 2013; 5:109–123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Nisbet LC, Yiallourou SR, Walter LM, et al. Blood pressure regulation, autonomic control and sleep disordered breathing in children. Sleep Med Rev 2014; 18:179–189. [DOI] [PubMed] [Google Scholar]
- 40.Ng DK, Chan C, Chow AS, et al. Childhood sleep-disordered breathing and its implications for cardiac and vascular diseases. J Paediatr Child Health 2005; 41:640–646. [DOI] [PubMed] [Google Scholar]
- 41.Kwok KL, Ng DK, Chan CH. Cardiovascular changes in children with snoring and obstructive sleep apnoea. Ann Acad Med Singapore 2008; 37:715–721. [PubMed] [Google Scholar]
- 42.Walter LM, Yiallourou SR, Vlahandonis A, et al. Impaired blood pressure control in children with obstructive sleep apnea. Sleep Med 2013; 14:858–866. [DOI] [PubMed] [Google Scholar]
- 43.Li AM, Au CT, Ho C, et al. Blood pressure is elevated in children with primary snoring. J Pediatr 2009; 155:362–368. [DOI] [PubMed] [Google Scholar]
- 44.Mancia G, Fagard R, Narkiewicz K, et al. Task Force Members 2013 ESH/ESC Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens 2013; 31:1281–1357. [DOI] [PubMed] [Google Scholar]
- 45.Drukteinis JS, Roman MJ, Fabsitz RR, et al. Cardiac and systemic hemodynamic characteristics of hypertension and prehypertension in adolescents and young adults: the Strong Heart Study. Circulation 2007; 115:221–227. [DOI] [PubMed] [Google Scholar]
- 46.Raitakari OT, Juonala M, Kähönen M, et al. Cardiovascular risk factors in childhood and carotid artery intima-media thickness in adulthood: the Cardiovascular Risk in Young Finns Study. JAMA 2003; 290:2277–2283. [DOI] [PubMed] [Google Scholar]
- 47.Lande MB, Kaczorowski JM, Auinger P, et al. Elevated blood pressure and decreased cognitive function among school-age children and adolescents in the United States. J Pediatr 2003; 143:720–724. [DOI] [PubMed] [Google Scholar]
- 48.Baker JL, Olsen LW, Sørensen TI. Childhood body-mass index and the risk of coronary heart disease in adulthood. N Engl J Med 2007; 357:2329–2337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Bibbins-Domingo K, Coxson P, Pletcher MJ, et al. Adolescent overweight and future adult coronary heart disease. N Engl J Med 2007; 357:2371–2379. [DOI] [PubMed] [Google Scholar]
- 50.Marcus CL, Moore RH, Rosen CL, et al. Childhood Adenotonsillectomy Trial (CHAT) A randomized trial of adenotonsillectomy for childhood sleep apnea. N Engl J Med 2013; 368:2366–2376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Li AM, Zhu Y, Au CT, et al. Natural history of primary snoring in school-aged children: a 4-year follow-up study. Chest 2013; 143:729–735. [DOI] [PubMed] [Google Scholar]
- 52.Nisbet LC, Yiallourou SR, Biggs SN, et al. Preschool children with obstructive sleep apnea: the beginnings of elevated blood pressure? Sleep 2013; 36:1219–1226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Vlahandonis A, Nixon GM, Davey MJ, et al. Improvement of sleep-disordered breathing in children is associated with a reduction in overnight blood pressure. Sleep Med 2013; 14:1295–1303. [DOI] [PubMed] [Google Scholar]
- 54.Vlahandonis A, Yiallourou SR, Sands SA, et al. Long-term changes in blood pressure control in elementary school-aged children with sleep-disordered breathing. Sleep Med 2014; 15:83–90. [DOI] [PubMed] [Google Scholar]
- 55.Li AM, Au CT, Ng C, et al. A 4-year prospective follow-up study of childhood OSA and its association with BP. Chest 2014; 145:1255–1263. [DOI] [PubMed] [Google Scholar]
- 56.National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics 2004; 114 (2 Suppl 4th Report):555–576. [PubMed] [Google Scholar]
- 57.Ng DK, Wong JC, Chan CH, et al. Ambulatory blood pressure before and after adenotonsillectomy in children with obstructive sleep apnea. Sleep Med 2010; 11:721–725. [DOI] [PubMed] [Google Scholar]
- 58.Lee LA, Li HY, Lin YS, et al. Severity of childhood obstructive sleep apnea and hypertension improved after adenotonsillectomy. Otolaryngol Head Neck Surg 2015; 152:553–560. [DOI] [PubMed] [Google Scholar]
- 59.Teo DT, Mitchell RB. Systematic review of effects of adenotonsillectomy on cardiovascular parameters in children with obstructive sleep apnea. Otolaryngol Head Neck Surg 2013; 148:21–28. [DOI] [PubMed] [Google Scholar]
- 60.Vlahandonis A, Walter LM, Horne RS. Does treatment of SDB in children improve cardiovascular outcome? Sleep Med Rev 2013; 17:75–85. [DOI] [PubMed] [Google Scholar]