

Abstract
The primary aim was to compare postoperative radiographic outcomes between sexes among adolescent idiopathic scoliosis (AIS) patients. A total of 162 AIS patients (42 males and 120 females) undergoing pedicle screw instrumentation and posterior fusion were included. Coronal and sagittal curves and flexibilities were measured and calculated. The postoperative correction rate (CR), fulcrum bending correction index (FBCI), and Cincinnati correction index were evaluated to compare the surgical benefits between sexes.
Males were older (16.79 vs 14.79 years, respectively; P < 0.01) and had stiffer curves than females (lateral bending flexibility percentage: 47.77 vs 52.57, respectively, P = 0.21; traction flexibility percentage: 35.48 vs 36.98, respectively, P = 0.98; fulcrum bending flexibility percentage: 56.13 vs 66.57, respectively, P < 0.05). Males and females exhibited similar Lenke classification schemes (P = 0.72), but had different Risser signs (P < 0.01). Although males had greater postoperative curves (20.81° vs 16.83°, respectively; P = 0.009), no obvious differences in the CRs were noted between males and females (FBCI: 145.20% vs 108.37%, respectively; P = 0.92). Smaller preoperative lumbar lordosis was noted in males than in females (40.05° vs 45.72°, respectively; P = 0.03), yet no statistically significant differences in the preoperative and postoperative sagittal curves were observed between the sexes. In conclusion, considering the preoperative flexibilities, the 2 sexes achieved comparable surgical benefits without sacrificing the sagittal balance.
INTRODUCTION
Adolescent idiopathic scoliosis (AIS) is defined as a coronal curvature exceeding 10° on an anteroposterior x-ray image, without any specific etiology, and is one of the most common diseases among children. It is reported that the incidence rate is approximately 0.70% to 1.44% in Mainland China1,2 and 0.47% to 5.2% worldwide.3,4 Sexual dimorphism has been discovered in the course of AIS. The female-to-male ratio is at least 1.5:1 and rises substantially with increased age and Cobb angle.5 In particular, the ratio rises from 2.7 to 8.1 as the Cobb angle increases from 10° to 30°.4 Curve types also differ between sexes. Males have more major thoracic curves, fewer C-modifiers, and less apical lumbar translation in Lenke classification.6 Males usually present with older age and less flexibility,7,8 and sex might not have as much influence on flexibility as age and the Cobb angle.9 In addition, bracing, which has been shown to be notably effective as a conservative treatment,10,11 was found to be less effective in males compared with female patients.12 However, few studies have focused on the surgical outcomes of AIS patients.
Whether there are sex differences regarding these surgical outcomes remains unclear. Sucato13 performed the first retrospective study that focused on radiographic differences after surgery between the sexes. It was found that compared with females, males had larger preoperative primary curves but similar flexibility, in addition to greater postoperative primary curves and a lower correction rate (CR). In a subsequent paired study, although exhibiting similar preoperative primary curves and flexibilities, males had a poorer CR, indicating that sex might affect the surgical outcomes of AIS patients. Ameri14 showed similar findings, but with less flexibility in males. However, no statistically significant differences in the CR were noted in subsequent matched comparisons. Other evidence has failed to verify sex differences in the surgical outcomes of AIS patients. Marks8 conducted a multicenter study including 449 females and 98 males. Males presented with similar primary curves but less flexibility. However, no differences in the postoperative CR or the Cincinnati correction index (CCI) were found between sexes. In a nationwide survey investigating postoperative complications, Patil found that more males experienced in-hospital complications and that the in-hospital death rate was 3 times higher in males.15 Therefore, it remains to be further explored whether males could derive the same surgical benefits as females.
Flexibility could greatly affect the correction results in AIS patients. It has been shown that fulcrum bending film and lateral bending film could effectively predict the coronal Cobb angle after surgery.16–20 The fulcrum bending correction index (FBCI) and CCI have been demonstrated to have valid reliability in assessing radiographic outcomes.17,18,21,22 In addition, it should be noted that when the CR is used and expressed as a percentage, a small change in the measurement will result in a great change in the CR. Therefore, preoperative flexibility should be considered when evaluating surgical outcomes. The primary aim of the present study was to compare radiological outcomes between the sexes among AIS patients.
MATERIALS AND METHODS
Settings and Patient Population
This was a retrospective investigation of all of the consecutive AIS patients undergoing posterior pedicle screw instrumentation at a single spine center from June 2009 to June 2014. The inclusion criteria were adolescent patients requiring a stage-one posterior procedure. The exclusion criteria were congenital scoliosis and suspected neuromuscular scoliosis. Patients with revision surgery or additional flexibility-modifying surgery were also excluded. In all, 268 AIS patients met the inclusion criteria, 65 of whom underwent other procedures for correction of deformity, 25 of whom were lost to follow-up, 8 of whom were not followed up to 3 months, and 8 of whom underwent revision surgery. A total of 162 patients were thus included in the present study. All of the patients underwent pedicle screw instrumentation and posterior fusion by 1 senior surgeon (ML). The specific pedicle screw instrumentation system used was the Moss-Miami system (DePuy Spine, Raynham, MA). The fusion levels were chosen according to the recommendations proposed by Lenke et al.23,24 The study was approved by the local ethics committee.
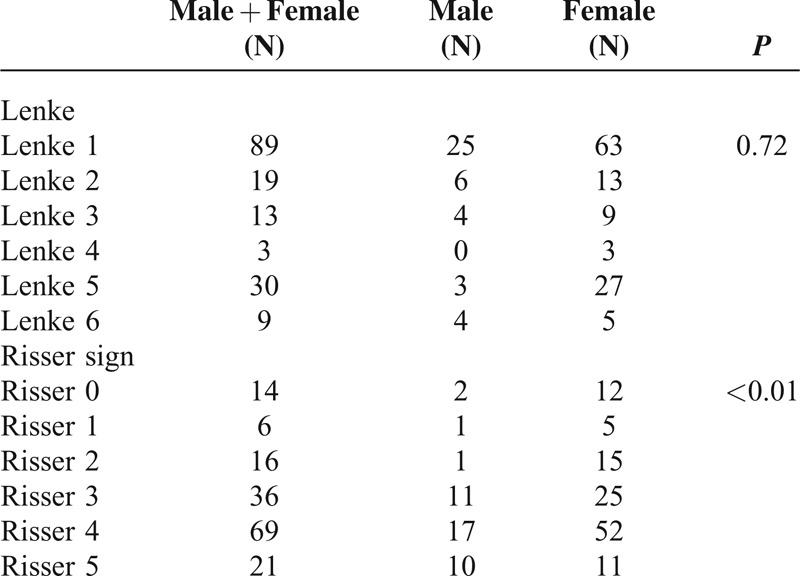
According to the Lenke classification scheme,23 there were 89 patients with a Lenke 1 curve, 19 patients with a Lenke 2 curve, 13 patients with a Lenke 3 curve, 3 patients with a Lenke 4 curve, 30 patients with a Lenke 5 curve, and 9 patients with a Lenke 6 curve. The Risser sign was used to assess bone maturity. There were 14 patients with a Risser sign of 0, 6 patients with a Risser sign of 1, 16 patients with a Risser sign of 2, 36 patients with a Risser sign of 3, 69 patients with a Risser of sign 4, and 21 patients with a Risser sign of 5.
Clinical and Radiographic Assessment
All of the demographic data were retrieved from the medical records. Radiographic measurements were performed on scanned radiographs. Blood loss and blood transfusion during the perioperative period as well as major complications were recorded. Films were measured using a standard technique and were obtained from long-cassette radiographs during the preoperative period and follow-up radiographs during the postoperative period (3 months). An experienced spine surgeon (YB) reviewed the medical records and plain radiographs of all of the patients. Coronary flexibility was assessed based on bending radiographs, traction radiographs, and fulcrum bending radiographs. Lateral bending radiographs were performed by asking patients to maximally bend while in the supine position. Fulcrum bending films were obtained according to the protocol of Cheung and Luk.16,17 The thoracic fulcrum was placed at the rib of the corresponding apical vertebra, with the shoulder away from the table. In patients with lumbar curves, fulcrums were placed at the apical vertebra, with the pelvis away from the table. Supine traction films were measured according to the Takahashi method.25 Although the patient was supine, the traction rope was placed around the lower jaw and occiput, and the caudal traction rope was placed around the pelvis; the traction force was set as half of the body weight, with 30 kg as the maximum. The Cobb angle was measured in pre- and postoperative posterior-anterior; lateral standing radiographs; and preoperative supine lateral bending, supine traction, and fulcrum bending radiographs.
The CR, lateral bending flexibility (LBF), supine traction bending flexibility, fulcrum bending flexibility (FBF), FBCI, and CCI were calculated as follows:
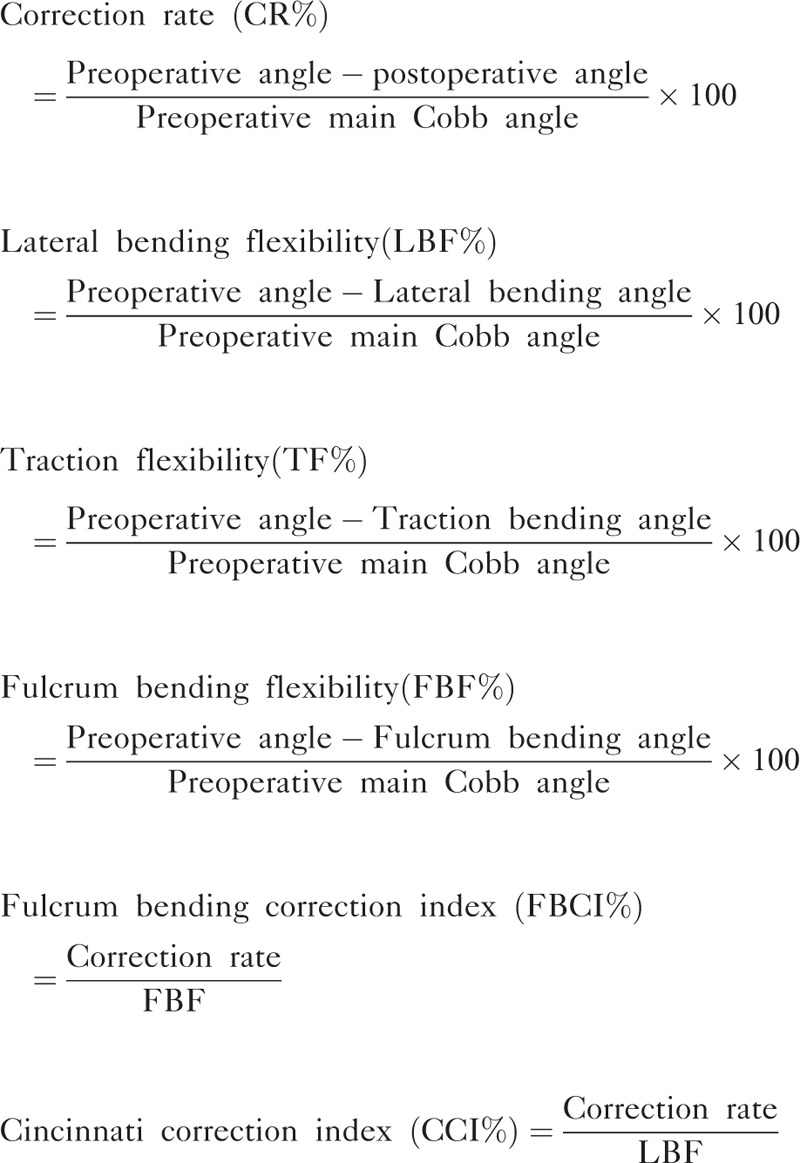 |
Statistical Analysis
Statistical analysis was performed using SPSS 16.0 software (SPSS, Inc, Chicago, IL) and SAS 9.1.3 (SAS Institute, Cary, NC). Descriptive data are presented as the mean and standard deviation for quantitative variables and as the median for qualitative variables. An independent-sample t test was used to compare preoperative radiographic outcomes between males and females if homogeneity of variance was obtained. Otherwise, the Wilcoxon signed-rank sum test was used. Both a t test and analysis of covariance were conducted to compare postoperative radiographic outcomes. The CR, FBCI, and CCI were compared using the Wilcoxon signed-rank sum test. Lenke-type classification and the Risser sign distribution were analyzed using the Cochran–Mantel–Haenszel (CMH) test via SAS. Statistical significance was defined as a P value <0.05.
RESULTS
A total of 162 patients were included in the study, with 42 males and 120 females. All of the patients were from Mainland China. Most of the patients (156/162) were of Han descent. The males were significantly older than the females (16.79 vs 14.79 years, respectively; P < 0.01). Males and females demonstrated similar flexibility, with the exception of lower FBF in males than in females (LBF%, 47.77 vs 52.57, respectively, P = 0.21; TF%, 35.48 vs 36.98, respectively, P = 0.98; FBF%, 56.13 vs 66.57, respectively, P < 0.05; Table 1). No significant differences were found in the Lenke classification schemes between males and females, with Lenke 1 accounting for the highest percentages (60% vs 53%, respectively) and Lenke 4 accounting for the lowest percentages (0% vs 3%, respectively; Table 2). Thoracic curves were dominant in both males and females (83% vs 73%, respectively). Overall differences were noted in the Risser sign analysis (P < 0.01 for the CMH test; Table 2). It was demonstrated that more males than females had mature bones (25% vs 9%, respectively). However, fewer males were found to have ceased progression of scoliosis compared with females (25% vs 53%, respectively).
TABLE 1.
Preoperative Characteristics of AIS Patients
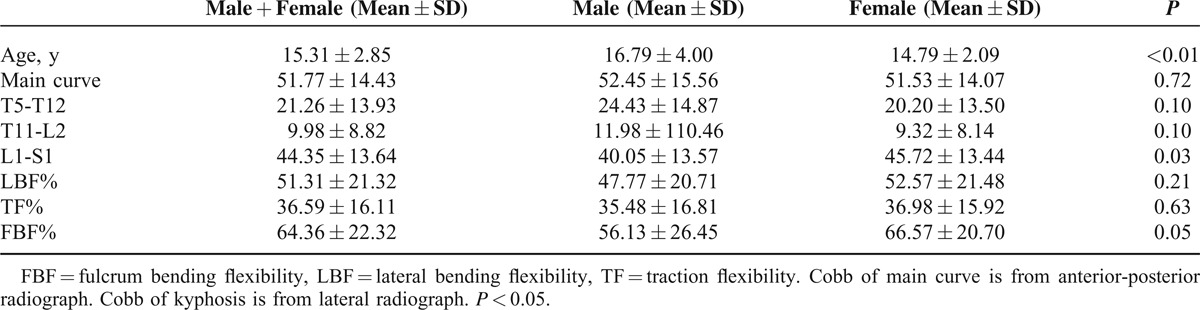
TABLE 2.
Lenke Classification and Risser Sign in Male and Female AIS Patients
During surgery, males were prone to losing more blood than females (857 vs 607 mL, respectively; P < 0.05; Table 3). However, the amount of blood transfusion was similar in males and females (685 vs 673 mL, respectively; P = 0.91). No mortality or revision surgeries were recorded.
TABLE 3.
Comparison of Blood Loss and Transfusion After Surgery Between Sex

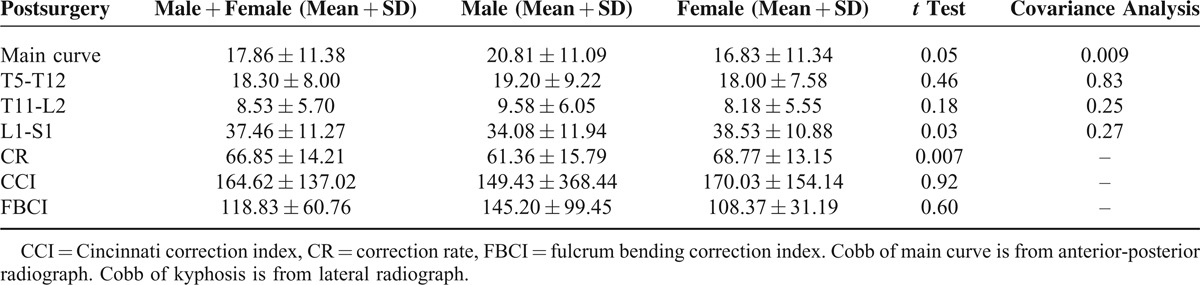
Preoperatively, males and females had similarly sized main curves (52.45° vs 51.53°, respectively; P = 0.72; Table 1). However, greater mean main curves were noted for males than for females after surgery (20.81° vs 16.83°, respectively; P = 0.05). Analysis of covariance also revealed a statistically significant difference in the postoperative main curve between males and females (P = 0.009). CR analysis showed that males had a poorer CR than females (61.36% vs 66.85%, respectively; P = 0.007; see representative pre-/postoperative AP films, with Figure 1A and B for a male patient and Figure 2A and B for a female patient). However, when flexibility was considered, no obvious differences were observed because both the FBCI and the CCI were comparable between males and females (FBCI%, 145.20 vs 108.37, respectively, P = 0.60; CCI%, 170.03 vs 149.43, respectively, P = 0.28; Table 4).
FIGURE 1.
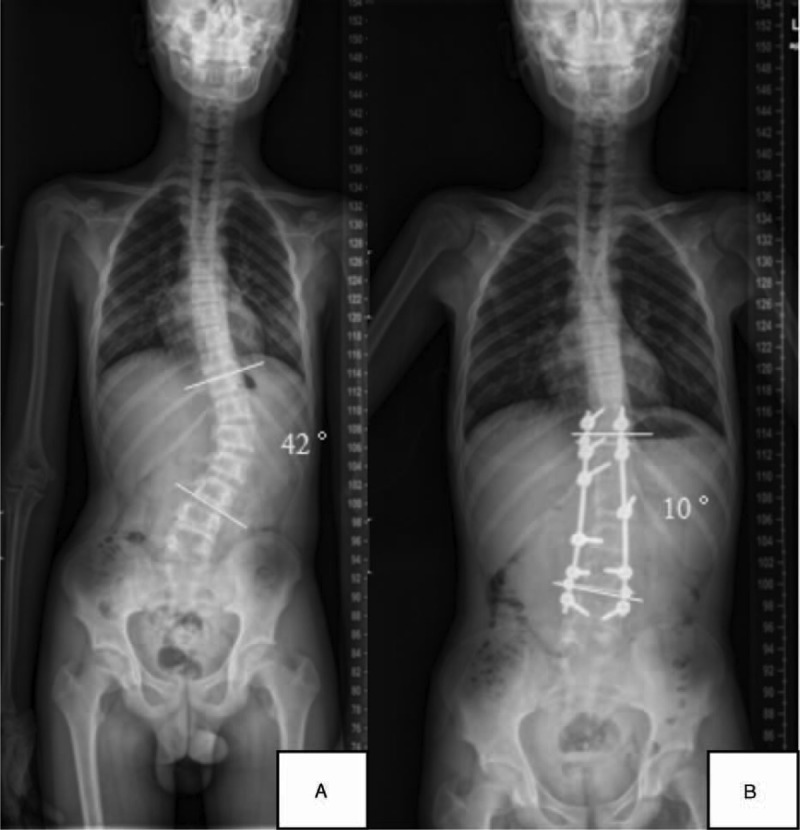
Representative pre-/postoperative AP films of a male patient. The preoperative Cobb angle is 42° (A), and the postoperative Cobb angle is 10° (B).
FIGURE 2.
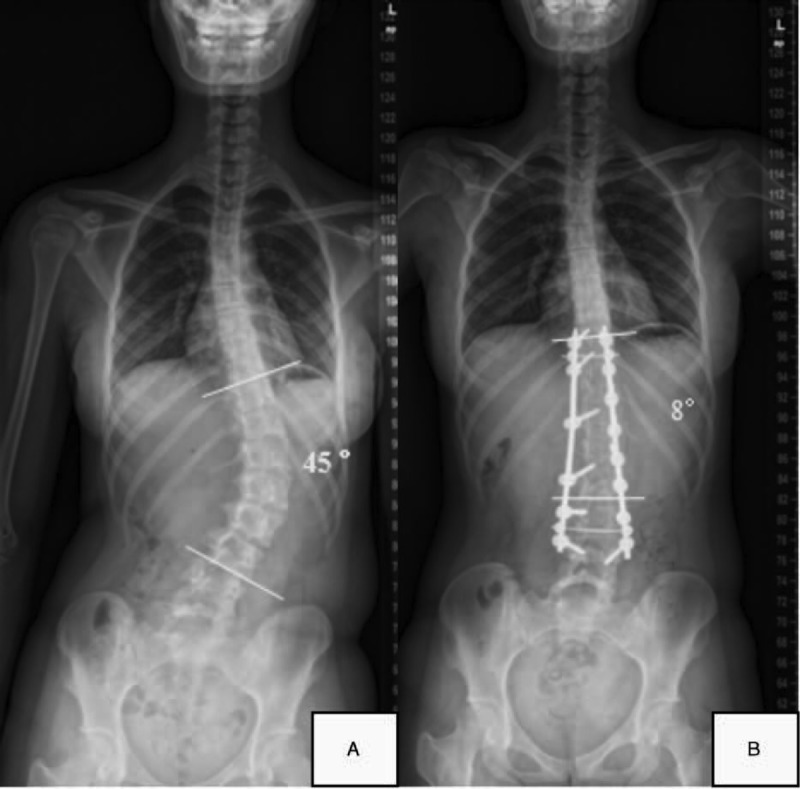
Representative pre-/postoperative AP films of a female patient. The preoperative Cobb angle is 45° (A), and the postoperative Cobb angle is 8° (B).
TABLE 4.
Postoperative Characteristics of AIS Patients Between Sex
Males had nonsignificantly larger curves in preoperative and postoperative thoracic kyphosis and thoracolumbar lordosis while having significantly smaller preoperative lumbar lordosis (Table 1). Postoperatively, a t test revealed that males had smaller lumbar lordosis than females (34.08° vs 38.53°, respectively; P = 0.03). However, analysis of covariance showed no statistically significant differences (P = 0.27) in the preoperative and postoperative changes between males and females when the preoperative Cobb angle imbalance was controlled (Table 4).
DISCUSSION
Whether males can achieve similar surgical outcomes has attracted growing interest from surgeons because of sexual dimorphism in the course of AIS.6,8,13,14,26,27 Although numerous studies have focused on the evaluation of surgical outcomes and relevant factors affecting surgical correction,28–30 few have paid attention to sex differences. It has been noted that males present with older age, stiffer curves, and poorer brace treatment results.8,12,13,14,26 Therefore, speculation that males achieve a lower CR in the course of scoliosis has naturally arisen. Indeed, Sucato and Ameri found that males presented with larger main curves and achieved a poorer CR than females.13,14 However, other studies failed to replicate these results.8,26 In the present study, it was demonstrated that males had larger postoperative main curves than females, although they derived similar surgical benefits when assessed via a correction index.
In our study, males presented with older age, as described in other studies.8,13,14 Lenke classification analysis revealed that the main thoracic curves were prevalent in both sexes and that triple major curves were the least prevalent. Differences in bone maturity were noted between the sexes. Males were found to have more Risser sign 5 than females, indicating that males presented with more mature bones. However, more males than females were found to have scoliosis progression; studies have found that scoliosis ceases to progress in females once Risser 4 is reached, whereas in males, Risser 5 must be reached. Marks also found that the 2 sexes had similar Lenke classification schemes, whereas Ameri and Helenius used the King classification system.
Compared with females, males had similarly sized main curves as well as thoracic kyphosis and thoracolumbar curves; however, males had smaller lumbar lordosis. These results were similar to those of the Marks study,8 with the main curves being approximately 50°. However, Sucato and Ameri both found that males presented with a larger Cobb angle before surgery, with mean Cobb angles >60° 13,14 (Table 5). Owing to the relatively small number of patients in the Sucato and Ameri studies, it is reasonable to believe that males could present with similar Cobb angles to those of females before surgery. The cause of the difference may be partly that parents pay more attention to their children's appearance now than they did 10 years ago. Therefore, parents will take their children to the hospital as soon as they identify any imbalance in the spine.3,4
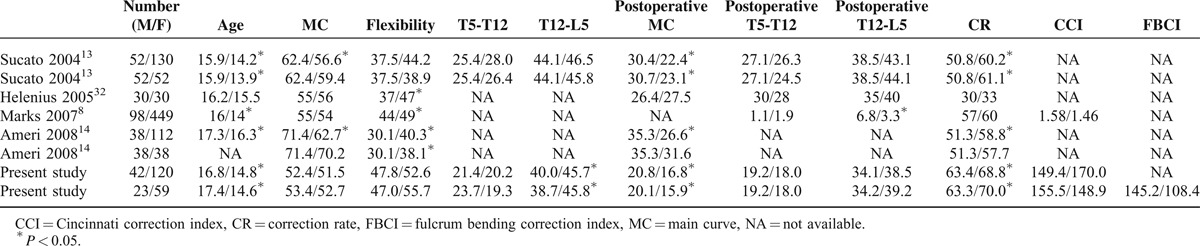
TABLE 5.
Summary of Studies on Radiological Differences Between Males and Females in AIS Patients
Flexibilities were thoroughly evaluated before surgery. Lateral bending films, traction films, and fulcrum bending films were used. In lateral bending films and traction films, males and females demonstrated similar flexibilities. However, in fulcrum bending films, males showed poorer flexibility than females. Sucato, Marks, Helenius, and Ameri only used lateral bending films to test flexibility.8,13,14,32 Sucato found that males and females had similar flexibilities, whereas Helenius, Marks, and Ameri found that males had significantly stiffer curves compared with females. Ameri reported poorer flexibility, and the present study reported greater flexibility.14 The cause of the difference may be that most patients had larger curves in the Ameri study and smaller curves in the present study. In addition, the patients included in the Ameri study were older than those in other studies. Studies have found that flexibility is closely associated with the Cobb angle and age in AIS patients.7–9 Fulcrum bending films have been shown to be superior in predicting the postoperative Cobb angle and CR, which are also 2 of the key factors in determining the surgical strategies for thoracic curve patients.16–18 Recently, it has been demonstrated that fulcrum bending films have a similar predictive effect in patients with lumbar and superior thoracic curves.21 Therefore, it is necessary to use fulcrum bending films in evaluating flexibility in AIS patients.
In the present study, it was discovered that males had greater main curves after surgery, indicating that males might derive limited benefits from surgery compared with females. Similar results were found in other studies.8,13,14 Males had curves that were 5° to 10° larger on average than those of females after surgery, regardless of whether they had similar curve sizes before surgery. However, in a multicenter study, similarly sized main curves were found in the 2 sexes after surgery.8 To control for the differences between preoperative main curves, both Sucato and Ameri conducted a paired study to eliminate the preoperative differences.13,14 However, Sucato found a poorer CR in males, whereas Ameri failed to discover any differences after surgery when controlling for the main curve. The cause of the difference may be that flexibility and surgical techniques essentially influence the surgical outcomes. In the Sucato study,13 males and females demonstrated similar flexibility, whereas males had stiffer curves in the Ameri study 14 (Table 5). Marks found that males and females could benefit from a similar surgical correction effect when the CR was used.8 However, other studies found that the CR in males was 5% to 10% lower than that in females.
In our study, males derived similar surgical benefits. No statistically significant differences were observed regarding the correction indexes (FBCI, 145.20 vs 108.37, P = 0.60; CCI, 155.50 vs 148.92, P = 0.28). Lateral bending film was designed to assess spinal flexibility to predict the correction achieved by Harrington instrumentation. It has a limited ability to reflect the outcomes of the modern segmental spinal instrumentation commonly used today.19,31 The FBCI has been demonstrated to have superior advantages in assessing thoracic curves, with similar results in lumbar curve patients.21 Therefore, males and females derived comparable benefits from surgery in the present study. This finding may be attributable to the pedicle screw instrumentation used in our study, which offers an enhanced three-dimensional deformity correction and preserves motion segments,32,33 as popularized by Roy-Camille et al.34 Systematic reviews have concluded that pedicle screw instrumentation yields a significantly larger percentage of angle correction than hooks and hybrid instrumentation.35,36 It should be noted that different surgical strategies were used in the above-mentioned studies,8,13,14 which may have significantly affected the surgical outcomes. In addition, cumulative surgical experience is an important factor influencing surgical outcomes, as evidenced by lower complication rates today than 10 to 20 years ago.15,37
In addition, no loss of sagittal balance was noticed in the present study, indicating that pedicle screw instrumentation did not endanger the stability of the spine. There were no statistically significant differences in thoracic kyphosis or lumbar lordosis between sexes. Sucato also noted that males and females had similar acceptable thoracic kyphosis and lumbar lordosis before and after surgery.13 Marks and Ameri did not report sagittal balance before and after surgery. It should be noted that the CR is not improved at the expense of sagittal balance. Although minimal loss of thoracic kyphosis and lumbar lordosis was noted after surgery (kyphosis, 21.26° vs 18.30° pre- and postsurgery, respectively; lordosis, 44.35° vs 37.46° pre- and postsurgery, respectively), both postoperative kyphosis and lordosis had normal values (kyphosis, 10°–40°; lordosis, 20°–60°), without endangering sagittal balance.23,38 Meanwhile, the thoracolumbar curve was also in the normal range, with mean values of <10° in both sexes, indicating no obvious imbalance in the thoracolumbar area.23
Our findings may serve as a valuable reference for clinical practice. Although males may present with older age, stiffer curves and higher Risser signs, they can derive similar surgical benefits as females. Posterior pedicle screw instrumentation is an effective surgical procedure for correction of deformity in both male and female AIS patients. Our results suggest that correction indexes (the FBCI and CCI) are effective for assessing surgical outcomes compared with the CR. Although in certain male cases, the postoperative Cobb angle may be larger than that in female counterparts, males can achieve comparable surgical benefits because of their stiffer curves. The FBCI and CCI are effective parameters for assessing the surgical outcomes of deformity correction.
There were several advantages of the present study. First, the subjects were homogeneous because all of the patients underwent modern posterior pedicle screw instrumentation under the guidance of Lenke strategies,23,27 whereas other studies included patients who had undergone different surgical procedures, such as posterior or anterior instrumentation, Harrington instrumentation, and Texas Scottish Rite Hospital instrumentation. A lack of such homogeneity would add another important compounding factor to the surgical results, beyond sex and flexibility.8,13,14 Second, appropriate statistical analysis methods were used in the present study. Analysis of covariance was used to examine the postoperative Cobb angle because the preoperative Cobb angle can significantly affect the postoperative Cobb angle. Although a t test was used in the Sucato study13 and nonparametric analysis was used in the Marks8 and Ameri14 studies, not all of the studies excluded the effect of the preoperative Cobb angle. For example, in the present study, a t test revealed statistically significant differences in lumbar lordosis between sexes, whereas analysis of covariance showed no difference between the sexes after controlling for preexisting differences. Therefore, it is more appropriate to use analysis of covariance for postoperative parameters. In addition, the CMH test was used to test the differences in Lenke classification and Risser sign distribution in the present study, whereas other studies failed to use reasonable statistical methods to test the differences.8,13,14 More importantly, correction indexes, rather than the CR, were used in the present study. The FBCI and CCI were shown to be effective and consistent in assessing surgical outcomes. In addition, fulcrum bending films can better predict the postoperative Cobb angle after surgery.17,18,21,22
The limitations of this study were relatively few compared with those in the Marks study. However, the Marks study enrolled more patients than other studies did,13,14 indicating that the results were reliable. In addition, there may be rater bias when measuring the Cobb angles of x-ray films.
In conclusion, males and females achieve comparable surgical benefits without sacrificing the sagittal balance. In addition, males have a greater main curve size after surgery than females. However, the preoperative sex differences do not compromise the radiological outcomes of pedicle screw treatment.
Footnotes
Abbreviations: AIS = adolescent idiopathic scoliosis, CCI = Cincinnati correction index, CR = correction rate, FBCI = fulcrum bending correction index.
The authors, their immediate families, and any research foundation with which they are affiliated did not receive any financial payments or other benefits from any commercial entity related to the subject of this article.
XX, FW, XZ, and YC contributed equally to this article.
The authors have no conflicts of interest to disclose.
REFERENCES
- 1.Ma X, Zhao B, Lin QK. Investigation on scoliosis incidence among 24,130 school children. Zhonghua Liu Xing Bing Xue Za Zhi 1995; 16:109–110. [PubMed] [Google Scholar]
- 2.Huang NQ, Guo HS, Liu J, et al. A survey on adolescent scoliosis in Guangzhou. Zhonghua Liu Xing Bing Xue Za Zhi 2011; 32:138–141. [PubMed] [Google Scholar]
- 3.Ueno M, Takaso M, Nakazawa T, et al. A 5-year epidemiological study on the prevalence rate of idiopathic scoliosis in Tokyo: school screening of more than 250,000 children. J Orthop Sci 2011; 16:1–6. [DOI] [PubMed] [Google Scholar]
- 4.Luk KD, Lee CF, Cheung KM, et al. Clinical effectiveness of school screening for adolescent idiopathic scoliosis: a large population-based retrospective cohort study. Spine (Phila Pa 1976) 2010; 35:1607–1614. [DOI] [PubMed] [Google Scholar]
- 5.Konieczny MR, Senyurt H, Krauspe R. Epidemiology of adolescent idiopathic scoliosis. J Child Orthop 2013; 7:3–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sponseller PD, Flynn JM, Newton PO, et al. The association of patient characteristics and spinal curve parameters with Lenke classification types. Spine (Phila Pa 1976) 2012; 37:1138–1141. [DOI] [PubMed] [Google Scholar]
- 7.Hoashi JS, Cahill PJ, Bennett JT, et al. Adolescent scoliosis classification and treatment. Neurosurg Clin N Am 2013; 24:173–183. [DOI] [PubMed] [Google Scholar]
- 8.Marks M, Petcharaporn M, Betz RR, et al. Outcomes of surgical treatment in male versus female adolescent idiopathic scoliosis patients. Spine (Phila Pa 1976) 2007; 32:544–549. [DOI] [PubMed] [Google Scholar]
- 9.Chen ZQ, Zhao YF, Bai YS, et al. Factors affecting curve flexibility in skeletally immature and mature idiopathic scoliosis. J Orthop Sci 2011; 16:133–138. [DOI] [PubMed] [Google Scholar]
- 10.Carragee EJ, Lehman RA., Jr Spinal bracing in adolescent idiopathic scoliosis. N Engl J Med 2013; 369:1558–1560. [DOI] [PubMed] [Google Scholar]
- 11.Maruyama T, Grivas TB, Kaspiris A. Effectiveness and outcomes of brace treatment: a systematic review. Physiother Theory Pract 2011; 27:26–42. [DOI] [PubMed] [Google Scholar]
- 12.Karol LA. Effectiveness of bracing in male patients with idiopathic scoliosis. Spine (Phila Pa 1976) 2001; 26:2001–2005. [DOI] [PubMed] [Google Scholar]
- 13.Sucato DJ, Hedequist D, Karol LA. Operative correction of adolescent idiopathic scoliosis in male patients. A radiographic and functional outcome comparison with female patients. J Bone Joint Surg Am 2004; 86-A:2005–2014. [DOI] [PubMed] [Google Scholar]
- 14.Ameri E, Behtash H, Mobini B, et al. Radiographic outcome of surgical treatment of adolescent idiopathic scoliosis in males versus females. Scoliosis 2008; 3:12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Patil CG, Santarelli J, Lad SP, et al. Inpatient complications, mortality, and discharge disposition after surgical correction of idiopathic scoliosis: a national perspective. Spine J 2008; 8:904–910. [DOI] [PubMed] [Google Scholar]
- 16.Luk KD, Don AS, Chong CS, et al. Selection of fusion levels in adolescent idiopathic scoliosis using fulcrum bending prediction: a prospective study. Spine (Phila Pa 1976) 2008; 33:2192–2198. [DOI] [PubMed] [Google Scholar]
- 17.Cheung WY, Lenke LG, Luk KD. Prediction of scoliosis correction with thoracic segmental pedicle screw constructs using fulcrum bending radiographs. Spine (Phila Pa 1976) 2010; 35:557–561. [DOI] [PubMed] [Google Scholar]
- 18.Luk KD, Cheung WY, Wong Y, et al. The predictive value of the fulcrum bending radiograph in spontaneous apical vertebral derotation in adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 2012; 37:E922–E926. [DOI] [PubMed] [Google Scholar]
- 19.Aronsson DD, Stokes IA, Ronchetti PJ, et al. Surgical correction of vertebral axial rotation in adolescent idiopathic scoliosis: prediction by lateral bending films. J Spinal Disord 1996; 9:214–219. [PubMed] [Google Scholar]
- 20.Debanné P, Pazos V, Labelle H, et al. Evaluation of reducibility of trunk asymmetry in lateral bending. Stud Health Technol Inform 2010; 158:72–77. [PubMed] [Google Scholar]
- 21.Vora V, Crawford A, Babekhir N, et al. A pedicle screw construct gives an enhanced posterior correction of adolescent idiopathic scoliosis when compared with other constructs: myth or reality. Spine (Phila Pa 1976) 2007; 32:1869–1874. [DOI] [PubMed] [Google Scholar]
- 22.Li J, Dumonski ML, Samartzis D, et al. Coronal deformity correction in adolescent idiopathic scoliosis patients using the fulcrum-bending radiograph: a prospective comparative analysis of the proximal thoracic, main thoracic, and thoracolumbar/lumbar curves. Eur Spine J 2011; 20:105–111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Lenke LG, Betz RR, Harms J, et al. Adolescent idiopathic scoliosis: a new classification to determine extent of spinal arthrodesis. J Bone Joint Surg Am 2001; 83-A:1169–1181. [PubMed] [Google Scholar]
- 24.Lenke LG, Betz RR, Clements D, et al. Curve prevalence of a new classification of operative adolescent idiopathic scoliosis: does classification correlate with treatment? Spine (Phila Pa 1976) 2002; 27:604–611. [DOI] [PubMed] [Google Scholar]
- 25.Takahashi S, Passuti N, Delécrin J. Interpretation and utility of traction radiography in scoliosis surgery. Analysis of patients treated with Cotrel-Dubousset instrumentation. Spine (Phila Pa 1976) 1997; 22:2542–2546. [DOI] [PubMed] [Google Scholar]
- 26.Raggio CL. Sexual dimorphism in adolescent idiopathic scoliosis. Orthop Clin North Am 2006; 37:555–558. [DOI] [PubMed] [Google Scholar]
- 27.Helenius I, Remes V, Yrjönen T, et al. Does gender affect outcome of surgery in adolescent idiopathic scoliosis? Spine (Phila Pa 1976) 2005; 30:462–467. [DOI] [PubMed] [Google Scholar]
- 28.Wilson PL, Newton PO, Wenger DR, et al. A multicenter study analyzing the relationship of a standardized radiographic scoring system of adolescent idiopathic scoliosis and the Scoliosis Research Society outcomes instrument. Spine (Phila Pa 1976) 2002; 27:2036–2040. [DOI] [PubMed] [Google Scholar]
- 29.Rushton PR, Grevitt MP. Do vertebral derotation techniques offer better outcomes compared to traditional methods in the surgical treatment of adolescent idiopathic scoliosis? Eur Spine J 2014; 23:1166–1176. [DOI] [PubMed] [Google Scholar]
- 30.Kepler CK, Meredith DS, Green DW, et al. Long-term outcomes after posterior spine fusion for adolescent idiopathic scoliosis. Curr Opin Pediatr 2012; 24:68–75. [DOI] [PubMed] [Google Scholar]
- 31.Cheung KM, Luk KD. Prediction of correction of scoliosis with use of the fulcrum bending radiograph. J Bone Joint Surg Am 1997; 79:1144–1150. [DOI] [PubMed] [Google Scholar]
- 32.Suk SI, Lee CK, Kim WJ, et al. Segmental pedicle screw fixation in the treatment of thoracic idiopathic scoliosis. Spine (Phila Pa 1976) 1995; 20:1399–1405. [PubMed] [Google Scholar]
- 33.Suk SI, Lee SM, Chung ER, et al. Selective thoracic fusion with segmental pedicle screw fixation in the treatment of thoracic idiopathic scoliosis: more than 5-year follow-up. Spine (Phila Pa 1976) 2005; 30:1602–1609. [DOI] [PubMed] [Google Scholar]
- 34.Roy-Camille R, Saillant G, Mazel C. Internal fixation of the lumbar spine with pedicle screw plating. Clin Orthop 1986; 203:7–17. [PubMed] [Google Scholar]
- 35.Crawford AH, Lykissas MG, Gao X, et al. All-pedicle screw versus hybrid instrumentation in adolescent idiopathic scoliosis surgery: a comparative radiographical study with a minimum 2-year follow-up. Spine (Phila Pa 1976) 2013; 38:1199–1208. [DOI] [PubMed] [Google Scholar]
- 36.Ledonio CG, Polly DW, Jr, Vitale MG, et al. Pediatric pedicle screws: comparative effectiveness and safety: a systematic literature review from the Scoliosis Research Society and the Pediatric Orthopaedic Society of North America task force. J Bone Joint Surg Am 2011; 93:1227–1234. [DOI] [PubMed] [Google Scholar]
- 37.Hicks JM, Singla A, Shen FH, et al. Complications of pedicle screw fixation in scoliosis surgery: a systematic review. Spine (Phila Pa 1976) 2010; 35:E465–E470. [DOI] [PubMed] [Google Scholar]
- 38.Bernhardt M, Bridwell KH. Segmental analysis of the sagittal plane alignment of the normal thoracic and lumbar spines and thoracolumbar junction. Spine (Phila Pa 1976) 1989; 14:717–721. [DOI] [PubMed] [Google Scholar]