

Abstract
Background:
Nutritional status is a critical factor in patient outcomes in a variety of medical contexts. In the surgical fields, there is substantial evidence suggesting that clinical outcomes including infection risk and surgical efficacy may be affected by preoperative nutritional status. The purpose of this study is to evaluate preoperative serum prealbumin levels, the currently preferred serum biomarker of nutritional deficiency, in relation to the risk of developing a surgical site infection.
Methods:
A retrospective case–control series was conducted comparing prospectively collected preadmission serum prealbumin levels to the risk for surgical site infection following elective spine surgery. The analysis was conducted under an approved institutional quality assurance protocol. Patients were identified by querying the department billing codes for deep wound washouts over a 3-year period. A cohort of 32 patients with preoperative prealbumin levels who underwent spine surgery complicated by postoperative deep tissue infection was identified. This was compared against a case–control cohort of 74 patients who underwent spine surgery and did not experience postoperative infection. Clinical variables included demographic information, body mass index, smoking, diabetes, steroid use, length of the procedure, and length of hospital stay. The data were analyzed using multivariate Cox regression.
Results:
Two variables: Preoperative prealbumin < 20 and diabetes were both statistically significant predictors for the risk of developing a postoperative infection with hazard ratios of 2.12 (95% confidence interval [CI]: 1.03–4.37) and 2.22 (95% CI: 1.04–4.75), respectively.
Conclusions:
Our results reinforce the relationship between preoperative nutritional status and outcomes in elective spine surgery. The data indicate that preoperative prealbumin levels may be useful in risk stratification. Further study is needed to determine whether nutritional supplementation may reduce the risk of infection.
Keywords: Malnutrition, nutrition, prealbumin, spinal fusion, spine surgery
INTRODUCTION
Nutritional status is a critical factor in patient outcomes in a variety of medical contexts.[4,7,10,14,15] Surgical outcomes have been linked to patients’ preoperative nutritional status in multiple sub-specialties.[1,5,6,7,8,10,16,19] Currently, transthyretin, more commonly referred to as prealbumin, is the preferred serum biomarker for the assessment of nutritional status due to a shorter half-life than the historically utilized marker, albumin.[2,3,14] Up to 40% of patients over the age of 60 undergoing spinal decompression and fusion are malnourished based upon serum albumin levels;[12] prospective data regarding prealbumin as a nutrition marker in spine surgery are lacking. We recently reported a retrospective link between impaired postoperative nutritional markers (low prealbumin) to deep wound surgical site infection.[20] As a result of that work, we began routinely measuring prealbumin levels preoperatively in patients undergoing elective spine surgery in our institution. The current study evaluates preoperative serum prealbumin levels in relation to the risk of developing a surgical site infection following elective spine surgery.
METHODS
A retrospective case–control series was conducted comparing prospectively collected, preadmission, serum prealbumin levels to the risk for surgical site infection following elective spine surgery. The analysis was conducted under an approved institutional quality assurance protocol. In August of 2009, prealbumin was added to the routine preoperative laboratory panel for all patients undergoing elective spine surgery by the two senior authors at Presbyterian Hospital at the University of Pittsburgh Medical Center. A cohort of patients who experienced postoperative wound infections between 2009 and 2012 was identified. The resulting 292 surgical wound washouts performed during this 3-year period were further narrowed to patients with available preoperative prealbumin levels. Patients with a known cancer diagnosis, with traumatic or infectious pathology, or who underwent minimally invasive or anterior approaches to the spine were further excluded. The above process resulted in 32 patients meeting criteria for inclusion. Subsequently, a case–control cohort of 74 patients who did not experience a postoperative wound infection was assembled from a database of all patients who underwent elective open posterior spinal surgery during the same time interval. Patients were selected based on surgical location, age, number of levels operated, and the availability of preoperative prealbumin levels. The electronic medical record for each patient was then reviewed, and additional clinical and demographic data were collected. Statistical analysis was performed by the department statistician using SPSS (IBM, Armonk, NY, USA). Table 1 summarizes the demographic characteristics for each cohort of patients.
Table 1.
Summary of patient demographics and surgical characteristics by cohort

RESULTS
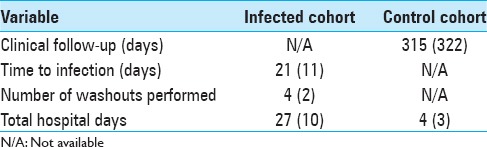
Table 2 summarizes further clinical information for each cohort. Duration of follow-up for the control cohort was 315 ± 322 days ensuring that patients were followed long enough for an infection to manifest. In addition, as expected and indicating the significant cost associated with postoperative wound infections, the total days spent in the hospital was longer in the infected cohort.
Table 2.
Summary of clinical treatment
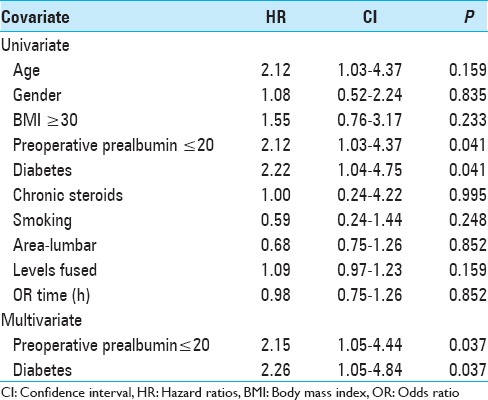
A Chi-squared analysis was used to assess for differences in the basic clinical and demographic parameters found in Table 1 between the infected versus noninfected cohorts. No significant difference was found in the age, male/female ratio, body mass index, operative time, and co-morbidities. This indicates our two groups to be similar in composition. The number of patients with diabetes trended toward but did not reach clinical significance with a P = 0.052. The only difference between groups that was statistically significant was the number of patients considered nutritionally deficient (P = 0.04) preliminarily indicating nutrition status is linked to risk for postoperative infection. A univariate Cox regression model was further utilized to determine the effect of variables on the primary endpoint: Development of infection. Additionally, multivariate regression was subsequently performed on factors with P < 0.1 in the univariate analysis to confirm significance accounting for confounding factors. The results are summarized in Table 3. In the univariate analysis, two variables were significant predictors of infection development: Prealbumin levels ≤20 (P = 0.041, hazard ratios [HR] 2.12) and diabetes (P = 0.041, HR 2.22). Both of these variables remained significant upon multivariate analysis indicating that both are independent risk factors for the development of an infection.
Table 3.
Results of Cox regression analysis
DISCUSSION
The current study demonstrates a link between preoperative nutritional status (low serum prealbumin) and postoperative risk for development of a deep wound infection. We previously reported that decreased prealbumin levels were noted in patients with deep wound infection at the time of re-admission for infection.[20] Prealbumin, however, is known to be lowered in an acute phase response and, therefore, no conclusions could be drawn regarding whether preoperative prealbumin levels could predict the development of an infection.[9] The current analysis, however, demonstrates this link. Diabetes was also found to be an independent risk factor for the development of a postoperative infection; multivariate analysis confirmed that both low serum prealbumin and diabetes were independent risk factors.
Several prior studies have linked nutritional status to postoperative complications in spine surgery utilizing albumin levels as a surrogate marker.[1,12,17,18] For instance, Schoenfeld et al. analyzed 5887 patients who underwent spinal arthrodesis.[17] In a subgroup analysis, patients with serum albumin values <3.5 g/dL were found to have significantly increased risk for mortality (odds ratio [OR] 13.8), complications (OR 3.6), wound infection (OR 2.4), and thromboembolic phenomenon (OR 4.0). Schoenfeld et al. in a prior analysis, also from the National Surgical Quality Improvement Program, of 3475 patients found albumin <3.0 g/dL to be a statistically significant predictor of mortality (OR 9.47), complication (OR 7.68), and major complication including deep wound infection (OR 9.1).[18] While albumin does appear to be a useful predictor of complications, serum prealbumin may be a more sensitive marker. Due to its shorter half-life, prealbumin may better detect early nutritional deficits. A direct comparison would ultimately be needed to compare the sensitivity of these markers.
The current study has several limitations.First, the study is a retrospective cohort analysis and is, therefore, subject to the limitations inherent to the study design. This is also a single institution analysis that was limited in selecting patients based on the availability of preoperative prealbumin levels. Thus, the patients in this study represent a small segment of those who have undergone spinal fusion at our institution. Further study is needed in this area to prove that nutritional status is a definitively useful tool for risk stratifying patients for postoperative complications. The ultimate goal would be to reduce postoperative infections through preoperative nutritional supplementation. While there have been several small trials of perioperative supplementation with total parenteral nutrition in deformity surgeries with largely negative results, there has been minimal work performed in this regard and represents a potentially inexpensive, noninvasive avenue by which complications may be reduced.[11,13]
CONCLUSION
Prealbumin is a useful marker of nutritional status that predicts patients who are at an increased risk of developing postoperative deep wound infections following spine surgery. This has changed our practice pattern to include further education regarding preoperative nutrition. Ultimately, further study is needed to determine whether the risk of developing an infection may be mitigated by preoperative nutritional supplementation.
Footnotes
Contributor Information
David J. Salvetti, Email: salvettidj@upmc.edu.
Zachary J. Tempel, Email: tempelzj@upmc.edu.
Gurpreet S. Gandhoke, Email: gandhokegs@upmc.edu.
Philip V. Parry, Email: parrypv@upmc.edu.
Ramesh M. Grandhi, Email: rameshmgrandhi@gmail.com.
Adam S. Kanter, Email: kanteras@upmc.edu.
David O. Okonkwo, Email: okonkwodo@upmc.edu.
REFERENCES
- 1.Adogwa O, Martin JR, Huang K, Verla T, Fatemi P, Thompson P, et al. Preoperative serum albumin level as a predictor of postoperative complication after spine fusion. Spine (Phila Pa 1976) 2014;39:1513–9. doi: 10.1097/BRS.0000000000000450. [DOI] [PubMed] [Google Scholar]
- 2.Beck FK, Rosenthal TC. Prealbumin: A marker for nutritional evaluation. Am Fam Physician. 2002;65:1575–8. [PubMed] [Google Scholar]
- 3.Bernstein LH, Ingenbleek Y. Transthyretin: Its response to malnutrition and stress injury. Clinical usefulness and economic implications. Clin Chem Lab Med. 2002;40:1344–8. doi: 10.1515/CCLM.2002.232. [DOI] [PubMed] [Google Scholar]
- 4.Bower RH, Cerra FB, Bershadsky B, Licari JJ, Hoyt DB, Jensen GL, et al. Early enteral administration of a formula (Impact) supplemented with arginine, nucleotides, and fish oil in intensive care unit patients: Results of a multicenter, prospective, randomized, clinical trial. Crit Care Med. 1995;23:436–49. doi: 10.1097/00003246-199503000-00006. [DOI] [PubMed] [Google Scholar]
- 5.Braga M, Gianotti L, Nespoli L, Radaelli G, Di Carlo V. Nutritional approach in malnourished surgical patients: A prospective randomized study. Arch Surg. 2002;137:174–80. doi: 10.1001/archsurg.137.2.174. [DOI] [PubMed] [Google Scholar]
- 6.Burden S, Todd C, Hill J, Lal S. Pre-operative nutrition support in patients undergoing gastrointestinal surgery. Cochrane Database Syst Rev. 2012;11:CD008879. doi: 10.1002/14651858.CD008879.pub2. [DOI] [PubMed] [Google Scholar]
- 7.de la Cruz KI, Bakaeen FG, Wang XL, Huh J, LeMaire SA, Coselli JS, et al. Hypoalbuminemia and long-term survival after coronary artery bypass: A propensity score analysis. Ann Thorac Surg. 2011;91:671–5. doi: 10.1016/j.athoracsur.2010.09.004. [DOI] [PubMed] [Google Scholar]
- 8.Del Savio GC, Zelicof SB, Wexler LM, Byrne DW, Reddy PD, Fish D, et al. Preoperative nutritional status and outcome of elective total hip replacement. Clin Orthop Relat Res. 1996;326:153–61. doi: 10.1097/00003086-199605000-00018. [DOI] [PubMed] [Google Scholar]
- 9.Fuhrman MP, Charney P, Mueller CM. Hepatic proteins and nutrition assessment. J Am Diet Assoc. 2004;104:1258–64. doi: 10.1016/j.jada.2004.05.213. [DOI] [PubMed] [Google Scholar]
- 10.Gianotti L. Nutrition and infections. Surg Infect (Larchmt) 2006;7(Suppl 2):S29–32. doi: 10.1089/sur.2006.7.s2-29. [DOI] [PubMed] [Google Scholar]
- 11.Hu SS, Fontaine F, Kelly B, Bradford DS. Nutritional depletion in staged spinal reconstructive surgery.The effect of total parenteral nutrition. Spine (Phila Pa 1976) 1998;23:1401–5. doi: 10.1097/00007632-199806150-00019. [DOI] [PubMed] [Google Scholar]
- 12.Klein JD, Hey LA, Yu CS, Klein BB, Coufal FJ, Young EP, et al. Perioperative nutrition and postoperative complications in patients undergoing spinal surgery. Spine (Phila Pa 1976) 1996;21:2676–82. doi: 10.1097/00007632-199611150-00018. [DOI] [PubMed] [Google Scholar]
- 13.Lapp MA, Bridwell KH, Lenke LG, Baldus C, Blanke K, Iffrig TM. Prospective randomization of parenteral hyperalimentation for long fusions with spinal deformity: Its effect on complications and recovery from postoperative malnutrition. Spine (Phila Pa 1976) 2001;26:809–17. doi: 10.1097/00007632-200104010-00023. [DOI] [PubMed] [Google Scholar]
- 14.Lourenço P, Silva S, Friões F, Alvelos M, Amorim M, Couto M, et al. Low prealbumin is strongly associated with adverse outcome in heart failure. Heart. 2014;100:1780–5. doi: 10.1136/heartjnl-2014-305747. [DOI] [PubMed] [Google Scholar]
- 15.Marik PE, Zaloga GP. Meta-analysis of parenteral nutrition versus enteral nutrition in patients with acute pancreatitis. BMJ. 2004;328:1407. doi: 10.1136/bmj.38118.593900.55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Moskovitz DN, Kim YI. Does perioperative immunonutrition reduce postoperative complications in patients with gastrointestinal cancer undergoing operations? Nutr Rev. 2004;62:443–7. doi: 10.1111/j.1753-4887.2004.tb00016.x. [DOI] [PubMed] [Google Scholar]
- 17.Schoenfeld AJ, Carey PA, Cleveland AW, 3rd, Bader JO, Bono CM. Patient factors, comorbidities, and surgical characteristics that increase mortality and complication risk after spinal arthrodesis: A prognostic study based on 5,887 patients. Spine J. 2013;13:1171–9. doi: 10.1016/j.spinee.2013.02.071. [DOI] [PubMed] [Google Scholar]
- 18.Schoenfeld AJ, Ochoa LM, Bader JO, Belmont PJ., Jr Risk factors for immediate postoperative complications and mortality following spine surgery: A study of 3475 patients from the National Surgical Quality Improvement Program. J Bone Joint Surg Am. 2011;93:1577–82. doi: 10.2106/JBJS.J.01048. [DOI] [PubMed] [Google Scholar]
- 19.Stableforth WD, Thomas S, Lewis SJ. A systematic review of the role of immunonutrition in patients undergoing surgery for head and neck cancer. Int J Oral Maxillofac Surg. 2009;38:103–10. doi: 10.1016/j.ijom.2008.12.008. [DOI] [PubMed] [Google Scholar]
- 20.Tempel Z, Grandhi R, Maserati M, Panczykowski D, Ochoa J, Russavage J, et al. Prealbumin as a serum biomarker of impaired perioperative nutritional status and risk for surgical site infection after spine surgery. J Neurol Surg A Cent Eur Neurosurg. 2015;76:139–43. doi: 10.1055/s-0034-1394188. [DOI] [PubMed] [Google Scholar]