

Abstract
Background
Agenesis of the internal carotid artery (ICA) is a rare congenital abnormality, sporadically reported to be associated with a combined congenital hypopituitarism. Nevertheless, only a few cases have been extensively described, and none of these have been characterized by an isolated growth hormone (GH) deficiency.
Case presentation
Here, we describe a 17-year old boy referred to our hospital for fatigue, decreased muscle strength and severe headache reported after the cessation of rhGH treatment for a GH deficiency diagnosed at the age of 2 years and 3 months. Magnetic resonance imaging (MRI) showed an adenohypophyseal hypoplasia with a lack of posterior pituitary hyperintensity, whereas MRI angiography indicated the absence of a normal flow void in the left ICA. Endocrinological tests confirmed the GH deficiency (GH peak after growth-hormone-releasing hormone (GHRH) + arginine: 2.42 ng/mL) with a very low IGF-I value (31 ng/mL) and normal function of other pituitary axes.
Conclusion
To the best of our knowledge this is the first confirmed case of an isolated GH deficiency in a patient with ICA agenesis. The presence of an isolated pituitary deficit is unlike to be considered only as an effect of hemodynamic mechanism, suggesting a role for genetic factor(s) as a common cause of these two rare birth defects. Further studies could clarify this issue and the underlying mechanisms to better understand the etiopathogenetic characteristics of this disorder.
Electronic supplementary material
The online version of this article (doi:10.1186/s12902-015-0037-y) contains supplementary material, which is available to authorized users.
Background
Agenesis, aplasia and hypoplasia of the internal carotid artery (ICA) are rare congenital vascular malformations [1]. Of these, agenesis of the ICA is an extremely rare vascular anomaly occurring in less than 0.01 % of the population [2]. A 3:1 left side predominance in the ICA agenesis has been reported [1].
Agenesis of the ICA is rarely associated with congenital hypopituitarism (CH) [3]. CH is also a very rare congenital manifestation presenting either as an isolated hormone deficiency—the most common of which is isolated growth hormone deficiency (IGHD)—or multiple pituitary hormone involvement (combined pituitary hormone deficiencies (CPHD)) [4].
The etiology of this association is not clear: even if the blocking of a unilateral blood supply might cause the pituitary hypoplasia, a possible genetic cause, such as complex neural crest differentiation and/or migration disorders, cannot be excluded.
To the best of our knowledge, no more than 12 cases of CPHD associated with ICA have been reported [2, 5–14] (Table 1). However, a case of transient IGHD has been also described even though it may be caused by a reduced flow because of a focal stenosis in the right distal internal carotid artery and right middle cerebral artery due to a moyamoya [15]. Given the rarity of these two conditions, the association is unlikely to be causal, although this possibility cannot be excluded. In this report, we describe for the first time a 17-year-old boy with a confirmed diagnosis of IGHD and we review the literature and discuss the etiology of this association.
Table 1.
Review of endocrinological and anatomical characteristics of patients with congenital hypopituitarism and internal carotid malformations
| Sex | Age | Pituitary MRI | Internal carotid RMI | Other characteristics | Molecular studies | References | |
|---|---|---|---|---|---|---|---|
| 1 | N | N | Not specified (except for normal posterior pituitary). | Absence of ICA and carotid canal. | Not specified. | NP | [14] |
| 2 | M | 18 m | Pituitary hypoplasia. | Anomaly of right ICA. | TSH, GH, ACTH deficiency. Central diabetes insipidus. Possible hypogonadism. | NP | [13] |
| 3 | F | 5 m | Absence of anterior pituitary and ectopic pituitary posterior lobe. | Absence of right common carotid artery, right ICA, right anterior cerebral artery. | TSH, ACTH and GH deficiency. No evidence of diabetes insipidus. Genitalia were normal. Single central maxillary incisor. | NP | [7] |
| 4 | M | 23 year | Absence of anterior pituitary and ectopic pituitary posterior lobe. | Absence of right ICA and carotid canal and A1 segment of the right anterior cerebral artery. | Congenital microphthalmia with cataract and coloboma of the right eye, encephalocele. Hormonal substitution treatments not specified. | NP | [5] |
| 5 | M | 37 year | Absence of anterior pituitary. | Hypoplasia of right ICA and carotid canal. | Amblyopia of the left eye caused by an optic nerve coloboma, encephalocele. Hormonal substitution treatments not specified. | NP | [5] |
| 6 | F | 29 year | Pituitary hypoplasia and ectopic pituitary posterior lobe. | Absence of right ICA, carotid canal, and A1 segment of the right anterior cerebral artery. | TSH, ACTH, and GH deficiency. No evidence of diabetes insipidus. Hypogonadism. Chiari I malformation with syringomyelia. | NP | [9] |
| 7 | M | 5 year | Absence of anterior pituitary and ectopic pituitary posterior lobe. | Absence of left ICA and carotid canal, A1 segment of the left anterior cerebral artery and the anterior communicating artery. | Retrognathia, microphallus, and cryptorchidism. TSH, ACTH, GH deficiency, but no evidence of diabetes insipidus. Possibile hypogonadism. | NP | [10] |
| 8 | M | 11 year | Pituitary hypoplasia | Absence of left ICA and carotid canal; hypoplasia of A1 segment of left anterior cerebral artery | TSH, ACTH, GH deficiency. Central diabetes insipidus. Microphallus with possible hypogonadism. | NP | [6] |
| 9 | F | 10 year | Hypoplastic anterior pituitary, flat sella turcica, absent pituitary stalk | Agenesis of the left ICA and the left carotid canal | GH, TSH, gonadotropin deficiency. No evidence of diabetes insipidus. Born out of a consanguineous marriage. | No HESX1, LHX4, OTX2 mutations | [8] |
| 10 | F | 7 month | Adenohypophyseal hypoplasia with a lack of posterior pituitary hyperintensity | Absence of the left ICA | Desaturation episodes, recurrent respiratory infections. Short hands and feet. GH, ACTH and TSH deficiency. | 17q24.2 deletion | [3] |
| 11 | F | 2 year | Adenohypophyseal hypoplasia with a lack of posterior pituitary hyperintensity | Absence of the right ICA | GH, TSH, and gonadotropin deficiency. No clinical evidence of diabetes insipidus. | NP | [11] |
| 12 | M | 3 week | Absence of anterior pituitary with ectopic posterior pituitary | Absence of the left ICA and carotid canal | GH, TSH, ACTH and gonadotropin deficiency. Microphallus. | NP | [12] |
| 13 | M | 17 year | Adenohypophyseal hypoplasia with a lack of posterior pituitary hyperintensity | Agenesis of the left ICA | GH deficiency. No other pituitary deficiencies. No clinical evidence of diabetes insipidus. | Normal array-CGH | Our case |
NP not performed
Case report
The patient was a 17-year-old boy on rhGH therapy for 14 years because of a GH deficiency that was diagnosed at the age of 2 years and 3 months. Therapy was stopped 9 months before the beginning of symptoms—fatigue, decreased muscle strength and severe headache. However, the patient had not come for retesting one month after discontinuation of rhGH treatment.
The propositus was the first child of non-consanguineous Italian parents. The mother was in treatment for post-partum depression. The maternal grandfather was in treatment for autoimmune hyperthyroidism.
The mother’s height was 152 cm and she had menarche at the age of 13; the father’s height was 168 cm and he had a normal development. The target height was 166.0 ± 6.0 cm (−1.70 SDS). All auxological data were normalized for chronological age by conversion to standard deviation scores (SDS) that were calculated according to the following formula: patient value - mean of age-related reference value/standard deviation of the age-related reference value [16].
The child was born at 40 weeks of gestation with an uncomplicated delivery. The birth weight was 2970 g (−1.15 SDS), length at birth was 50 cm (−0.30 SDS), and his occipito-frontal head circumference (OFC) was 34 cm (−0.61 SDS). He had neonatal jaundice requiring phototherapy. The child’s neuromotor development was normal: he sat at 6 months, walked independently at 12 months, and began to use language at 14 months.
At 6 months, the patient exhibited very deficient growth (Fig. 1a and b). At 2 years and 3 months, he was admitted to our Paediatric Endocrine Unit for an endocrinological evaluation. His height, evaluated according the growth charts compiled by Cacciari et al. [17], was 78.6 cm (−2.79 SDS). His weight was 9.830 kg (−2.78 SDS), and his BMI was 15.91 (−0.28 SDS) (Fig. 1a-d). Extensive biochemical, endocrinological and metabolic examinations did not reveal any abnormalities with the exception of plasma concentrations of IGF-I and IGFBP-3 that were low for his age and sex: 27 ng/mL and 1.38 μg/mL, respectively. Thus, GH stimulation tests were performed and showed a reduced response after the clonidine (GH peak of 5.2 ng/mL) and insulin (glucose nadir 2.0 mmol/L at 30 min; GH peak of 3.9 ng/mL) tests. This revealed a GH deficiency (GHD). Bone age was assessed according to the Greulich and Pyle method [18], and it was delayed (1 year and 2 months versus a chronological age of 2 years and 3 months). Brain MRI of the hypophyseal region showed the presence of a pituitary hypoplasia (height 1.8 mm and width 2.7 mm). Consequently, hGH therapy (0.22 mg/kg/wk) was started.
Fig. 1.

Length (a), weight (b), height (c) and body mass index (BMI; d) growth charts of the patient. The growth charts of the length and weight refer to the first 3 years 4 months of life. The arrows indicate the age at which growth hormone treatment was initiated (black arrow). The length and the weight were evaluated according the growth charts compiled by de Onis et al. [37]. The height and BMI were evaluated according the growth charts compiled by Cacciari et al. [17]
The child responded very well to rhGH treatment (Fig. 1c) and at 3 years and 4 months old, his height was 94.5 cm (−1.14 SDS), weight 12.450 kg (−2.10 SDS), height velocity 15.06 cm/yr (5.05 SDS), and BMI 13.94 (−1.75 SDS). At 4 years and 3 months old, his height was 101.9 cm (−0.82 SDS), his weight was 15.300 kg (−1.24 SDS), his height velocity was 8.05 cm/yr (1.12 SDS), and his BMI was 14.73 (−0.82 SDS).
The onset of puberty occurred at 12 years old with normal onset, timing, tempo, and magnitude of pubertal changes [19]. He stopped rhGH treatment at 16 years and 3 months old when he reached the definitive stature [16]: his height was 170.8 cm (−0.64 SDS) and his weight was 51.800 kg (−1.56 SDS) with a BMI of 17.76 (−1.63 SDS) (Fig. 1c and d).
At 17 years old, his GH secretion was re-tested by the growth-hormone-releasing hormone (GHRH) + arginine test, which is a reliable test of ITT in retesting patients who had undergone GH treatment in childhood [20]. The test confirmed a severe GH deficiency (basal GH value of 0.18 ng/mL; GH peak of 2.42 ng/mL).
MRI angiography was performed because of the severe growth hormone deficiency (GHD) and headache; it confirmed the presence of adenohypophyseal hypoplasia (height 2.5 mm and width 3.5 mm) with a lack of posterior pituitary hyperintensity. The MRI angiography also showed the absence of a normal flow void in the left ICA (Fig. 2).
Fig. 2.
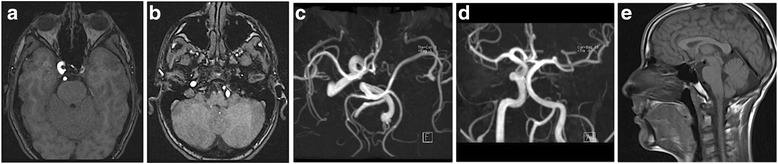
A MRI angiography time-of-flight (TOF) three-dimensional (3D) technique through the circle of Willis revealed agenesis of the intracranial portion of the left internal carotid artery (ICA). a. 3D TOF in the axial plane at the carotid siphon level shows agenesis of the left ICA. b. 3D TOF in the axial plane for the vertebrobasilar system shows the left vertebral artery and the compensatory hypertrophy. c. MRI angiography maximum intensity projection (MIP) reconstruction in the axial plane reveals agenesis of the intracranial portion of the left ICA. d. MRI angiography MIP reconstruction in the coronal plane highlights hypertrophy in the left vertebral collateral blood flow. e. Sagittal T1W TSE sequence shows adenohypophyseal hypoplasia (height 2.5 mm and width 3.5 mm) with a lack of posterior pituitary hyperintensity
No abnormal findings were noted in the electrocardiogram. Chromosomal studies of the peripheral lymphocyte cultures revealed a 46,XY normal male karyotype. An array of CGH analyses on the patient’s DNA was performed with an Agilent 60 K array platform with a resolution of approximately 100 kb. No genomic imbalances were detected. A complete examination was performed with particular attention to neurology, metabolism, and endocrinology (Table 2). The only abnormal result was a very low IGF-I value (31 ng/mL). In light of these results, the patient restarted rhGH therapy, and his symptoms at the time of referral disappeared.
Table 2.
Laboratory results at left ICA agenesis diagnosis
| Value | Reference values | Value | Reference values | ||
|---|---|---|---|---|---|
| FreeT4, pmol/L | 12.4 | 10.3–19.4 | HbA1c, % | 4.4 | <5.5 |
| TSH, mIU/L | 1.20 | 0.40–4.0 | Na+, mEq/L | 138 | 135–145 |
| Cortisol, μg/dL | 16.8 | 5.0–19.0 | K+, mEq/L | 4.2 | 3.5–5.0 |
| ACTH, ng/L | 25.7 | 9.0–52.0 | Cl−, mEq/L | 101 | 95–105 |
| Prolactin, mIU/L | 271 | 87.0–392.0 | Plasma osmolality, mOsm/kg | 295 | 280–300 |
| Total testosterone, ng/mL | 378 | 270.0–1070.0 | Urine Osmolality, mOsm/kg | 1037 | 400–1100 |
TSH thyroid-stimulating hormone, ACTH adrenocorticotrophic hormone
Discussion
ICA agenesis is a rare congenital abnormality that is very rarely associated with CH. All reported cases refer to patients with CPHD and ICA agenesis although many of these reports did not describe—or only poorly described—the possible associated endocrinological abnormalities and treatments. This had led many to hypothesize a vascular cause of pituitary disorders. Two different theories involving the hemodynamic mechanisms or disorders of differentiation and/or migration of the neural crest have been reported [2].
The ICA originates from the third aortic arch during embryogenesis. However, it is controversial whether the common and external carotids really originate from the same third aortic arch or from the aortic sac [21]. In patients presenting a vascular anomaly of the ICA, the blood supply of the affected side is partially or completely compensated by the vertebrobasilar or contralateral ICA system. This is characterized by the enlargement of a normally existing segment or presence of abnormal or persisting fetal arteries [22]. In most patients, this vascular anomaly is asymptomatic [23], and the rarity of a pediatric ICA agenesis diagnosis suggests that the arterial collateral pathways are initially sufficient to support cerebral perfusion [24]. However, some patients may experience recurrent headaches, blurred vision, hemiparesis, and hypopituitarism [25, 26] likely due to cerebrovascular insufficiency, compression by collateral vessels, or associated cerebral aneurysms [21]. Moreover, the symptoms reported by our patient were probably the result of both GHD (fatigue, decreased muscle strength, etc.) and ICA agenesis (headache).
Only one of the 13 patients previously described in the literature had MRI evidence of associated vascular defects. This patient had transient GH deficiency and was described by Quah et al. [15]. This patient’s pituitary defects and neurological symptoms may have been caused by reduced flow due to a focal stenosis of the other distal internal carotid artery and right middle cerebral artery due to a moyamoya [15]. However, the presence of a defect in the vascular perfusion is difficult to reconcile with the pituitary anatomical abnormalities and with the variability of the endocrinological defects reported including isolated GH deficiency or central diabetes insipidus (described only rarely) [6, 15].
The ICA is formed in embryos during the fourth week from the third aortic arch arteries and during the fifth and sixth weeks from the terminal segments of the dorsal aorta [27]. Conversely, the pituitary gland fully develops due to merging of the Rathke pouch and the infundibulum by the eighth week of gestation. The blood supply of the anterior and posterior pituitary gland comes from the bilateral superior and inferior hypophyseal arteries arising from the ICA [28]. It is not clear why pituitary hypoplasia would result from blocking of a unilateral blood supply and from abnormalities of the hypophyseal anatomy such as adenohypophysis hypoplasia and aplasia. However, the presence of ectopic neurophypophysis, which has been described in some patients, or other hypophyseal abnormalities, may also suggest a genetic etiology.
Pituitary gland development and function depend on the sequential temporal and spatial expression of multiple transcription factor genes such as POU1F1 (POU class 1 homeobox 1; OMIM 173110), PROP1 (prophet of PIT1; OMIM 601538), HESX1 (homeobox gene expressed in ES cells; OMIM 601802), LHX3 (LIM homeobox gene 3; OMIM 600577), LHX4 (LIM homeobox gene 4; OMIM 602146), SOX3 (SRY-related HMG-box gene 3; OMIM 313430), and OTX2 (orthodenticle homolog 2; OMIM 600037) [4]. However, these defects may cause a deficiency in one or more pituitary hormones. Its clinical features vary in both severity and time of presentation, and onset may occur in the neonatal period or develop later in life [29–31]. In some patients, the hormonal deficiencies may present as a part of a syndrome with patients manifesting abnormalities in structures that share a common embryological origin with the pituitary gland [29–31].
In our review 6 patients, in addition to our, had a pituitary hypoplasia [3, 6, 8, 9, 11, 13]. This abnormality was isolated in two cases [6, 13], associated with ectopic neurohypophysis [9], absent pituitary stalk [8], or associated with a lack of posterior pituitary hyperintensity [3, 11]. However 5 patients had an absent adenohypophysis [5, 7, 10, 12] and 4 associated of these showed an ectopic neurohypophysis [5, 7, 10, 12].
Moreover, ectopic neurohypophysis may be accompanied by midline brain defects [32] supporting an embryological defect due to genetic factors [32, 33]. This has been reported in idiopathic GH deficiency or in subjects with HESX1, LHX4, and SOX3 gene mutations [34]. For example, both the SOX3 under- and over-expression may result in CPHD or IGHD in males, associated with infundibular hypoplasia, ectopic/undescended posterior pituitary, and abnormalities of the corpus callosum [35]. In these patients, congenital abnormalities of the ICA or other vessels have not been reported [35]. However, the associated midline anomalies (coloboma, single central maxillary tooth, transsphenoidal encephalocele, and Chiari I malformation) reported in some cases [5, 7, 9, 15] may support this hypothesis.
Of the patients in our review, one case had unilateral agenesis of the internal carotid artery associated with CPHD without HESX1, LHX4, or OTX2 mutations [8]. Moreover, Savasta et al. [3] recently reported a CNV (copy number variant) i.e. a paternally inherited 200-kb deletion in 17q24.2. Thus, we performed array-CGH in our patient, but discovered no genomic imbalances. However, we indicate the need for further molecular analysis by NGS techniques to discover possible molecular abnormalities associated with this syndrome.
Given the rarity of the two conditions, the association is unlikely to be causal, although this cannot be excluded [36]. So, we hypothesize that an unknown gene mutation is the most likely explanation for the anatomical defects seen in these patients, suggesting a role for genetic factor(s) as a common cause of these two birth defects.
Conclusions
Here were report the first case of a confirmed isolated GH deficiency in a patient with ICA agenesis. Our experience suggests the opportunity to carefully evaluate possible vascular abnormalities in case of IGHD or CPHD. The presence of an isolated pituitary deficit, and the rare association between the two conditions, suggest a genetic rather than a hemodynamic mechanism. Further studies, especially with NGS-based molecular analysis, could clarify this issue and the underlying mechanisms to better understand the etiopathogenetic characteristics of this disorder.
Consent
Parents of the patient provided written informed consent for publication of this Case Report and any accompanying images. A copy of the written consent is available for review by the Editor of this Journal.
Acknowledgements
The authors would like to thank the patient’s family.
Abbreviations
- ACTH
Adrenocorticotrophic hormone
- CH
Congenital hypopituitarism
- CPHD
Combined pituitary hormone deficiencies
- GH
Growth hormone
- GHD
Growth hormone deficiency
- GHRH
Growth-hormone-releasing hormone
- ICA
Internal carotid artery
- IGHD
Isolated growth hormone deficiency
- MRI
Magnetic resonance image
- TSH
Thyroid-stimulating hormone
Additional file
CARE guidelines checklist of our Case Report. (DOCX 14 kb)
Footnotes
Competing interests
Stefano Stagi (SStagi), Giovanna Traficante (GT), Elisabetta Lapi (EL), Marilena Pantaleo (MP), Sabrina Becciani (SB), Marzia Mortilla (MM), Salvatore Seminara (SSeminara) and Maurizio de Martino (MdM) have no financial interests to disclose and no conflict of interest to declare.
Authors’ contributions
SStagi carried out the endocrinological evaluation, conceived of the study, and participated in its design. GT performed the clinical genetic evaluation, conceived of the study, and participated in its design. EL performed the clinical genetic evaluation, and revised critically the manuscript. MP performed the molecular genetic studies, participated in the acquisition of data, and was involved in drafting the manuscript. SB performed the endocrinological evaluation, participated in the acquisition of data, and was involved in drafting the manuscript. MM performed the neuroradiological evaluation, was involved in drafting, and revised critically the manuscript. SSeminara performed the endocrinological evaluation and revised critically the manuscript. MdM participated in the endocrinological evaluation and participated in its coordination. All authors read and approved the final manuscript.
Contributor Information
Stefano Stagi, Phone: +39-055-5662585, Email: stefano.stagi@yahoo.it.
Giovanna Traficante, Email: giovanna.traficante@meyer.it.
Elisabetta Lapi, Email: elisabetta.lapi@meyer.it.
Marilena Pantaleo, Email: marilena.pantaleo@meyer.it.
Sabrina Becciani, Email: beccianisabrina@hotmail.it.
Marzia Mortilla, Email: marzia.mortilla@meyer.it.
Salvatore Seminara, Email: seminara@unifi.it.
Maurizio de Martino, Email: maurizio.demartino@unifi.it.
References
- 1.Clarós P, Bandos R, Gilea I, Clarós A, Jr, Capdevila A, García Rodríguez J, et al. Major congenital anomalies of the internal carotid artery: agenesis, aplasia and hypoplasia. Int J Pediatr Otorhinolaryngol. 1999;49:69–76. doi: 10.1016/S0165-5876(99)00012-9. [DOI] [PubMed] [Google Scholar]
- 2.Lee JH, Oh CW, Lee SH, Han DH. Aplasia of the internal carotid artery. Acta Neurochir (Wien) 2003;145:117–125. doi: 10.1007/s00701-002-1046-y. [DOI] [PubMed] [Google Scholar]
- 3.Savasta S, Merli P, Introzzi F, Strocchio L, Lanati G, Incorpora G, et al. Agenesis of internal carotid artery and hypopituitarism: case report and review of literature. J Clin Endocrinol Metab. 2012;97:3414–3420. doi: 10.1210/jc.2011-3389. [DOI] [PubMed] [Google Scholar]
- 4.Kelberman D, Rizzoti K, Lovell-Badge R, Robinson IC, Dattani MT. Genetic regulation of pituitary gland development in human and mouse. Endocr Rev. 2009;30:790–829. doi: 10.1210/er.2009-0008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Blustajn J, Netchine I, Frédy D, Bakouche P, Piekarski JD, Meder JF. Dysgenesis of the internal carotid artery associated with transsphenoidal encephalocele: a neural crest syndrome? AJNR Am J Neuroradiol. 1999;20:1154–1157. [PMC free article] [PubMed] [Google Scholar]
- 6.Inamo Y, Harada K. Agenesis of the internal carotid artery and congenital pituitary hypoplasia: proposal of a cause of congenital hypopituitarism. Eur J Pediatr. 2003;162:610–612. doi: 10.1007/s00431-003-1272-1. [DOI] [PubMed] [Google Scholar]
- 7.Kjellin IB, Kaiserman KB, Curran JG, Geffner ME. Aplasia of right internal carotid artery and hypopituitarism. Pediatr Radiol. 1999;29:586–588. doi: 10.1007/s002470050654. [DOI] [PubMed] [Google Scholar]
- 8.Lamine F, Kanoun F, Chihaoui M, Saveanu A, Menif E, Barlier A, et al. Unilateral agenesis of internal carotid artery associated with congenital combined pituitary hormone deficiency and pituitary stalk interruption without HESX1, LHX4 or OTX2 mutation: a case report. Pituitary. 2012;15(Suppl 1):S81–S86. doi: 10.1007/s11102-012-0411-y. [DOI] [PubMed] [Google Scholar]
- 9.Mellado JM, Merino X, Ramos A, Salvadó E, Saurí A. Agenesis of the internal carotid artery with a trans-sellar anastomosis: CT and MRI findings in late-onset congenital hypopituitarism. Neuroradiology. 2001;43:237–241. doi: 10.1007/s002340000460. [DOI] [PubMed] [Google Scholar]
- 10.Moon WJ, Porto L, Lanfermann H, Weis R, Zanella FE. Agenesis of internal carotid artery associated with congenital anterior hypopituitarism. Neuroradiology. 2002;44:138–142. doi: 10.1007/s002340100678. [DOI] [PubMed] [Google Scholar]
- 11.Seixas D, Ayres-Basto M, Fontoura M, Silva ML, Fonseca J. Agenesis of the internal carotid artery and hypogenesis of the pituitary gland: cause, consequence or coincidence? Neuroradiol J. 2006;19:629–632. doi: 10.1177/197140090601900512. [DOI] [PubMed] [Google Scholar]
- 12.Shulman DI, Martinez CR. Association of ectopic posterior pituitary and anterior pituitary hypoplasia with absence of the left internal carotid. J Pediatr Endocrinol Metab. 1996;9:539–542. doi: 10.1515/JPEM.1996.9.5.539. [DOI] [PubMed] [Google Scholar]
- 13.Tanaka R, Tokuda M, Shinakawa S, Okasora K, Suzuki S, Konishi K. A multiple pituitary hormone deficiency patient with anomaly of internal carotid artery. 1996. [Google Scholar]
- 14.Triulzi F, Scotti G, di Natale B, Pellini C, Lukezic M, Scognamiglio M, et al. Evidence of a congenital midline brain anomaly in pituitary dwarfs: a magnetic resonance imaging study in 101 patients. Pediatrics. 1994;93:409–416. [PubMed] [Google Scholar]
- 15.Quah BL, Hamilton J, Blaser S, Héon E, Tehrani NN. Morning glory disc anomaly, midline cranial defects and abnormal carotid circulation: an association worth looking for. Pediatr Radiol. 2005;35:525–528. doi: 10.1007/s00247-004-1345-y. [DOI] [PubMed] [Google Scholar]
- 16.Stagi S, Galli L, Cecchi C, Chiappini E, Losi S, Gattinara CG, et al. Final height in patients perinatally infected with the human immunodeficiency virus. Horm Res Paediatr. 2010;74:165–171. doi: 10.1159/000281018. [DOI] [PubMed] [Google Scholar]
- 17.Cacciari E, Milani S, Balsamo A, Spada E, Bona G, Cavallo L, et al. Italian cross-sectional growth charts for height, weight and BMI (2 to 20 year) J Endocrinol Invest. 2006;29:581–593. doi: 10.1007/BF03344156. [DOI] [PubMed] [Google Scholar]
- 18.Greulich WW, Pyle SI. Radiographic Atlas of Skeletal Development of the Hand and Wrist. Stanford, CA: Stanford University Press; 1959. [Google Scholar]
- 19.Tanner JM, Whitehouse RH. Clinical longitudinal standards for height, weight, height velocity, weight velocity, and stages of puberty. Arch Dis Child. 1976;51:170–179. doi: 10.1136/adc.51.3.170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Aimaretti G, Baffoni C, Bellone S, Di Vito L, Corneli G, Arvat E, et al. Retesting young adults with childhood-onset growth hormone (GH) deficiency with GH-releasing-hormone-plus-arginine test. J Clin Endocrinol Metab. 2000;85:3693–3699. doi: 10.1210/jcem.85.10.6858. [DOI] [PubMed] [Google Scholar]
- 21.Quint DJ, Boulos RS, Spera TD. Congenital absence of the cervical and petrous internal carotid artery with intercavernous anastomosis. AJNR Am J Neuroradiol. 1989;10:435–439. [PMC free article] [PubMed] [Google Scholar]
- 22.Midkiff RB, Boykin MW, McFarland DR, Bauman JA. Agenesis of the internal carotid artery with intercavernous anastomosis. AJNR Am J Neuroradiol. 1995;16:1356–1359. [PMC free article] [PubMed] [Google Scholar]
- 23.Elazab NE, Riel-Romero RM, Gonzalez-Toledo E. Internal carotid artery agenesis and basilar artery aneurysm with third nerve palsy. Pediatr Neurol. 2010;42:451–454. doi: 10.1016/j.pediatrneurol.2010.02.002. [DOI] [PubMed] [Google Scholar]
- 24.Mayer PL, Leon Kier E. The ontogenetic and phylogenetic basis of cerebrovascular anomalies and variants. In: Apuzzo MLJ, editor. Brain Surgery: Complications, avoidance and management. 1. New York: Churchill and Livingstone; 1993. pp. 741–747. [Google Scholar]
- 25.Florio F, Balzano S, Nardella M, Strizzi V, Cammisa M, Bozzini V, et al. Congenital absence of the internal carotid artery. Cardiovasc Intervent Radiol. 1999;22:74–78. doi: 10.1007/s002709900334. [DOI] [PubMed] [Google Scholar]
- 26.Harps E, Helmke K. Diagnosis of congenital absence of internal carotid artery by power angio sonography. Eur Radiol. 1998;8:1245–1247. doi: 10.1007/s003300050542. [DOI] [PubMed] [Google Scholar]
- 27.Padget DH. The development of the cranial arteries in the human embryo. Contrib Embryol Carnegie Inst. 1948;32:205–261. [Google Scholar]
- 28.Lasjaunias P, Santoyo-Vazquez A. Segmental agenesis of the internal carotid artery: angiographic aspects with embryological discussion. Anat Clin. 1984;6:133–141. doi: 10.1007/BF01773165. [DOI] [PubMed] [Google Scholar]
- 29.Kelberman D, Dattani MT. Hypopituitarism oddities: congenital causes. Horm Res. 2007;68(Suppl 5):138–144. doi: 10.1159/000110610. [DOI] [PubMed] [Google Scholar]
- 30.Alatzoglou KS, Dattani MT. Genetic forms of hypopituitarism and their manifestation in the neonatal period. Early Hum Dev. 2009;85:705–712. doi: 10.1016/j.earlhumdev.2009.08.057. [DOI] [PubMed] [Google Scholar]
- 31.Romero CJ, Pine-Twaddell E, Radovick S. Novel mutations associated with combined pituitary hormone deficiency. J Mol Endocrinol. 2011;46:R93–R102. doi: 10.1530/JME-10-0133. [DOI] [PubMed] [Google Scholar]
- 32.Ultmann MC, Siegel SF, Hirsch WL, Finegold DN, Foley TP., Jr Pituitary stalk and ectopic hyperintense T1 signal on magnetic resonance imaging. Implications for anterior pituitary dysfunction. Am J Dis Child. 1993;147:647–652. doi: 10.1001/archpedi.1993.02160300053022. [DOI] [PubMed] [Google Scholar]
- 33.Chen S, Léger J, Garel C, Hassan M, Czernichow P. Growth hormone deficiency with ectopic neurohypophysis: anatomical variations and relationship between the visibility of the pituitary stalk asserted by magnetic resonance imaging and anterior pituitary function. J Clin Endocrinol Metab. 1999;84:2408–2413. doi: 10.1210/jcem.84.7.5849. [DOI] [PubMed] [Google Scholar]
- 34.di Iorgi N, Secco A, Napoli F, Calandra E, Rossi A, Maghnie M. Developmental abnormalities of the posterior pituitary gland. Endocr Dev. 2009;14:83–94. doi: 10.1159/000207479. [DOI] [PubMed] [Google Scholar]
- 35.Stagi S, Lapi E, Pantaleo M, Traficante G, Giglio S, Seminara S, de Martino M. A SOX3 (Xq26.3-27.3) duplication in a boy with growth hormone deficiency, ocular dyspraxia, and intellectual disability: a long-term follow-up and literature review. Hormones (Athens) 2014;13:552–560. doi: 10.14310/horm.2002.1523. [DOI] [PubMed] [Google Scholar]
- 36.Thomas M, Massa G, Craen M, de Zegher F, Bourguignon JP, Heinrichs C, et al. Prevalence and demographic features of childhood growth hormone deficiency in Belgium during the period 1986–2001. Eur J Endocrinol. 2004;151:67–72. doi: 10.1530/eje.0.1510067. [DOI] [PubMed] [Google Scholar]
- 37.de Onis M, Onyango AW, Borghi E, Garza C, Yang H, WHO Multicentre Growth Reference Study Group Comparison of the World Health Organization (WHO) Child Growth Standards and the National Center for Health Statistics/WHO international growth reference: implications for child health programmes. Public Health Nutr. 2006;9:942–947. doi: 10.1017/phn20062005. [DOI] [PubMed] [Google Scholar]