

Abstract
Background
Nonspecific interstitial pneumonia (NSIP) is characterized by interstitial infiltration of T lymphocytes, and subpopulations of these cells may be associated with the progression of fibrosis. However, few studies evaluate the correlation of prognosis with this characteristic. Therefore, we performed morphological and quantitative analyses of T lymphocytes in patients with NSIP and evaluated the relationship between T lymphocytes and prognosis.
Methods
Immunohistochemistry was used to detect the presence of CD4+ and CD8+ T lymphocytes in 55 biopsies of patients with NSIP to determine the numbers of these T cell subpopulations in lymphoid follicles as well as in perivascular, interstitial, and peribronchial anatomical compartments. The relationship between CD4+ and CD8+ T lymphocyte populations and prognosis was analyzed.
Results
The mean age of 55 patients was 48.9 ± 10.5 years, and 36 (65 %) of patients were women. All patients were followed for a mean duration of 46 ± 25 months. Thirteen (23.6 %) patients died during follow-up. Perivascular CD4+ lymphocyte infiltration (HR, 0.939; 95 % CI, 0.883–0.999; p = 0.048) was an independent risk factor for survival. Perivascular infiltrates of CD4+ T lymphocytes correlated with survival time (r = 0.270, p = 0.046). Patients with improved forced vital capacity survived longer and had higher numbers of CD4+ T lymphocytes that infiltrated perivascular tissue. The densities of CD4+ and CD8+ T lymphocytes infiltrating other tissues were not significantly associated with survival time.
Conclusions
Perivascular infiltration of CD4+ T lymphocytes in patients with NSIP correlated with prognosis. The underlying mechanisms are unknown and require further studies.
Electronic supplementary material
The online version of this article (doi:10.1186/s12890-015-0122-z) contains supplementary material, which is available to authorized users.
Keywords: T lymphocytes, Nonspecific interstitial pneumonia, Immunohistochemistry, Pathology
Background
Interstitial lung diseases (ILDs) are generally characterized by the accumulation of inflammatory cells within the lung, followed by the progressive deposition of extracellular matrix and subsequent destruction of alveolar airspaces [1]. The precise role of inflammatory cells in the pathogenesis of ILD remains poorly understood [2–4], although evidence indicates that T lymphocytes play an important role in the initiation and development of pulmonary fibrosis [5, 6]. However, few studies evaluate the prognostic significance of T lymphocyte subsets in patients with nonspecific interstitial pneumonia (NSIP) [7]. Therefore, we hypothesized that patients with NSIP who respond successfully to corticosteroid therapy harbor different T lymphocyte subpopulations compared with patients who do not respond.
To test this hypothesis, we evaluated the distribution of T lymphocyte subsets in the lung tissues of patients with NSIP. Using immunohistochemistry, we quantified the T lymphocyte subsets present in lymphoid follicles as well as in perivascular, interstitial, and peribronchial regions and explored the relationship between prognosis and survival.
Methods
Study subjects and diagnostic criteria
Between April 2003 and December 2011, 97 patients from Peking Union Medical College Hospital (PUMCH) were diagnosed with NSIP according to analysis of lung biopsies. Fifty-five patients who completed follow-up by undergoing tests of pulmonary function tests and computed tomography (CT) of the chest were included in this study. NSIP was diagnosed according to the American Thoracic Society (ATS)/European Respiratory Society consensus classification [8, 9]. Patients were not treated with corticosteroids or other immunosuppressants before undergoing a lung biopsy. Connective tissue disease (CTD) was diagnosed according to the criteria of the American College of Rheumatology as follows: autoantibodies against the nucleus (ANA titer >1:320), rheumatoid factor, Sjögren’s-syndrome-related antigens SSA or SSB, Scl-70, Sm, anti-Jo-1, ribonucleoprotein, or cyclic citrullinated peptide [10–13]. Patients with NSIP were classified into the groups as follows: (1) Members of the CTD-NSIP group met the criteria of the American College of Rheumatology for CTD. (2) Members of the NSIP-Ab + group had at least one positive serologic test. (3) Members of the NSIP-Ab– group were autoantibody negative. We extracted clinical characteristics documented at the time of a patient’s first visit as follows: age, ethnicity, sex, symptoms (cough, dyspnea, or wheeze) at the time of lung biopsy, symptoms or signs of CTD, smoking status, physical examination findings, pulmonary function results, serologic results, and chest CT scan.
Informed consent to use medical records was obtained from every patient, their guardian, or both when the patient was admitted to the hospital. The PUMCH Institutional Review Board approved this study (reference number for ethics approval: 2012–10–312).
Pulmonary physiological assessments
Spirometry, total lung capacity determined using plethysmography, forced vital capacity (FVC), and diffusing capacity of the lung for carbon monoxide were measured according to ATS recommendations [14–16], and the results are expressed as the percentage of predicted normal values. Prognosis was described according to FVC 1 year after steroid therapy. We classified patients as follows: FVC-group 1, improvement of FVC >10 %; FVC-group 2, improvement of FVC between 10 % and −10 %; and FVC-group 3, FVC reduced greater than −10 % [17–20].
High-resolution CT
All patients underwent high-resolution CT (HRCT) of the chest upon initial evaluation. A radiologist who specializes in diffuse parenchymal lung disease reviewed the CT scans. The extent and prevalence of abnormalities were measured in the areas as follows: (1) from the lung apex to the carina, (2) from the carina to the upper pulmonary vein, and (3) from the upper pulmonary vein to the base of the lung. HRCT images were assessed to determine the extent of parenchymal abnormalities, including ground-glass opacity (GGO), reticulation, honeycombing, consolidation, and emphysema. The extent of these abnormalities was determined using a 10 % scale for six zones [21]. Prognosis is described according to the manifestations detected using CT 1 year after steroid therapy. Patients with NSIP were classified as follows: CT-group 1, improvement of GGO and reticular opacity >50 %; group, CT-group 2, lesions reduced between 30 % and 50 %, and CT-group 3, lesions reduced by <30 % [21–23].
Histology of lung tissue
Two experienced pathologists reviewed independently the lung biopsy specimens, and the histologic pattern was assigned according to the consensus opinion. The pathologists were unaware of the patients’ clinical information. The histological patterns of the 55 patients were classified further, according to criteria proposed by Katzenstein and Fiorelli [24], as cellular, mixed, or fibrotic. Small airways were defined as those with an internal diameter <2 mm without cartilage in the airway walls [25]. Small blood vessels were defined as those with an internal diameter ≤100 μm [26].
Immunohistochemical analysis of CD4 and CD8 expression in lung tissue
Lung biopsy specimens were fixed in 10 % neutral-buffered formalin, cut into slices, embedded in paraffin, and cut into 4-μm-thick sections. Paraffin sections were reacted anti-CD4 (clone SP35, Zeta), and anti-CD8 (clone EP1150, Zeta) antibodies using the labeled-streptavidin-biotin complex method. The sections were deparaffinized, rehydrated with Tris-Buffered Saline (TBS) (0.005 M Tris, 0.15 M NaCl, pH 7.6) for 10 min, treated with 3 % hydrogen peroxide for 5 min to inhibit endogenous peroxidase activity, washed in TBS, and incubated with primary antibodies for 1 h. Immunohistochemical analyses of CD4 and CD8 expression were performed using the same tissue sections.
The numbers of dark-brown cells were determined using a NanoZoomer 2.0-RS Slide Scanning System (Hamamatsu Photonics KK; Japan Tokyo) and an Anymicro DSS Pro Image Analysis System (Yu Tian Shi Ji Wei Ye INC; Beijing, China). The follicles as well as perivascular, interstitial, and peribronchial regions were analyzed. The images of CD4+ and CD8+ T lymphocytes were obtained from the same region of the slide. At least six high-power fields (magnification × 200; analysis area, approximately 0.162 mm2) were randomly selected for each region and used to count the stained cells (Fig. 1).
Fig. 1.
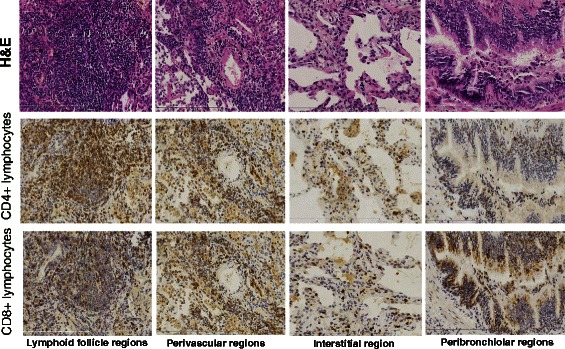
Distribution of T lymphocytes in different regions of lung tissue: CD4+ and CD8 + T lymphocytes decreased gradually in order of Lymphoid follicle, perivascular, interstitial and peribronchiolar regions. Positively stained of CD4+ and CD8 + T lymphocytes with dark brown staining
Treatment and follow up
All patients received a standard initial course of oral prednisone, starting at 0.5 mg/kg/d for 1 month that was tapered every 3 weeks to 5–7.5 mg/d (10 % decrease of the initial dose every 3 weeks), and maintained at 5–7.5 mg/d. Patients were treated for 12–18 months. Cyclophosphamide was administered concurrently with steroid therapy at an oral dose of 100 mg/d administered for 3–6 months to patients diagnosed with CTD-NSIP. Patients underwent routine examinations every 3–6 months after lung biopsy and then once each year at the Interstitial Lung Disease Clinic of PUMCH.
Statistical analysis
All values are expressed as the mean ± standard deviation (SD). Normally distributed data were evaluated using the t test. The Wilcoxon and Kruskal–Wallis tests were used to compare two or more non-normally distributed values, respectively. Fisher’s exact test was used to determine differences between groups. Correlation coefficients were calculated using the Spearman rank method. Cox multivariate regression analysis was used to evaluate risk factors of survival. The times to overall survival were calculated using the Kaplan–Meier method. The probability value was obtained using 2-sided tests, and statistical significance was defined as p < 0.05. SPSS 15.0 (SPSS for Windows, version 15.0; SPSS Inc., Chicago, IL, USA) was used for statistical analysis.
Results and discussion
Clinical features and laboratory findings
The clinical, radiological, and physiological measurements obtained at the time of the initial visit are shown in Table 1. The mean age of 55 patients was 48.9 ± 10.5 years (range, 23–68 years), and 36 patients (65 %) were women. There were 47 nonsmokers, six former smokers, and two current smokers. The mean duration of respiratory symptoms from onset to lung biopsy was 6 months (20.2 ± 50.9 months; range, 0.8–360 months). All patients were followed for a mean duration of 64.3 ± 26.7 months (range, 14–120 months).
Table 1.
Clinical features and laboratory findings of patients with NSIP
| NSIP (n = 55) | |
|---|---|
| Clinical manifestations, N (%) | |
| Dyspnea | 40 (72.7) |
| Cough | 47(85.5) |
| Chest pain | 4(7.3) |
| Dry eyes or dry mouth | 3(5.5) |
| Fever | 7 (12.7) |
| Arthralgia | 9(16.4) |
| Skin rash | 6(10.9) |
| Raynaud’s phenomenon | 3(5.5) |
| Weight loss | 4(7.3) |
| Crackles | 41(74.6) |
| Clubbing | 21(38.2) |
| Laboratory tests | |
| ESR, mm/h | 21.2 ± 19.2 |
| PaO2, mmHg | 77.8 ± 12.9 |
| PCO2, mmHg | 37.9 ± 8.4 |
| Serological results, N (%) | |
| Anti-nuclear antibody | 14 (25.5) |
| Anti-SSA antibody | 3 (5.5) |
| Anti-neutrophil cytoplasmic antibody | 3 (5.5) |
| Anti-Jo-1 antibody | 1 (1.8) |
| Anti-Scl-70 antibody | 1 (1.8) |
| PFT | |
| TLC, % predicted | 76.8 ± 14.1 |
| DLCO, % predicted | 56.4 ± 16.8 |
| Baseline chest CT findings, N (%) | |
| Ground glass opacity | 34 (61.8) |
| Patchy opacity | 40 (72.7) |
| Irregular reticular opacity | 35 (63.6) |
| Traction bronchiectasis | 17 (30.9) |
| Pleural thickness | 5 (14.6) |
The patients were diagnosed as follows: 21 with CTD-NSIP (including seven with polymyositis/dermatomyositis; seven with rheumatoid arthritis; four with of Sjögren syndrome; two with systemic sclerosis, and one with microscopic polyangiitis), 14 with NSIP-Ab (+), and 20 with NSIP-Ab (−). There were no differences among the three groups according to age, sex, cough, and dyspnea. Symptoms of arthralgia, Raynaud’s phenomenon, skin rash, and dry eye or mouth were highly associated with the CTD-NSIP and NSIP-Ab + groups compared with the NSIP-Ab- group (Table 2). No differences among the three groups were noted in arterial blood gas and HRCT findings. Abnormalities of pulmonary function were similar among the three groups and were characterized by restrictive defects with impairment of diffusion (Table 3). During follow-up, three patients (15 %) with cellular NSIP died (two from lung infections, one from liver failure), and six (21 %) and four (80 %) patients with mixed or fibrotic NSIP, respectively, died from progression of lung disease.
Table 2.
Clinical features of patients classified as CTD-NSIP, NSIP-Ab (+), or NSIP-Ab (−)
| Characteristics | CTD-NSIP (n = 21) | NSIP-Ab (+) (n = 14) | NSIP-Ab (−) (n = 20) | p value |
|---|---|---|---|---|
| Age (years) | 50.48 ± 11.73 | 44.57 ± 8.81 | 50.50 ± 9.99 | 0.197 |
| Male (%) | 15/21 (71.4 %) | 10/14 (71.4 %) | 11/20 (55.0 %) | 0.468 |
| Duration (months) | 12.21 ± 18.06 | 18.06 ± 30.99 | 30.20 ± 78.73 | 0.528 |
| Follow-up time (months) | 43.14 ± 23.90 | 53.43 ± 29.07 | 44.40 ± 24.01 | 0.467 |
| Symptoms | ||||
| Dyspnea | 15/21 (71.4 %) | 13/14 (92.9 %) | 19/20 (95 %) | 0.067 |
| Cough | 14/21 (66.7 %) | 10/14 (71.4 %) | 16/20 (80 %) | 0.627 |
| Chest pain | 2/21 (9.5 %) | 1/14 (7.1 %) | 1/20 (5 %) | 0.856 |
| Dry eyes or dry mouth | 2/21 (9.5 %) | 1/14 (7.1 %) | 0 | 0.386 |
| Fever | 2/21 (9.5 %) | 2/14 (14.3 %) | 3/20 (15 %) | 0.853 |
| Arthralgia | 6/21 (28.6 %) | 3/14 (21.4 %) | 1/20 (5 %) | 0.138 |
| Rash | 5/21 (23.8 %) | 1/14 (7.1 %) | 0 | 0.044 |
| Raynaud’s phenomenon | 3/21 (14.3 %) | 0 | 0 | 0.077 |
| Weight loss | 2/21 (9.5 %) | 1/14 (7.1 %) | 1/20 (5.0 %) | 0.856 |
| Signs | ||||
| Crackles | 19/21 (90.5 %) | 13/14 (92.9 %) | 15/20 (75 %) | 0.246 |
| Clubbing | 7/21 (33.3 %) | 5/14 (35.7 %) | 5/20 (25 %) | 0.765 |
Table 3.
Laboratory values of patients classified as CTD-NSIP, NSIP-Ab (+) and NSIP-Ab (−)
| Laboratory tests | CTD-NSIP (n = 21) | Ab (+)-NSIP (n = 14) | Ab (−)-NSIP (n = 20) | p value |
|---|---|---|---|---|
| ESR, mm/h | 16.33 ± 7.69 | 19.50 ± 12.70 | 27.45 ± 28.32 | 0.167 |
| PaO2, mmHg | 76.28 ± 14.25 | 80.67 ± 9.77 | 77.47 ± 13.52 | 0.614 |
| PCO2, mmHg | 40.20 ± 11.94 | 36.24 ± 5.57 | 36.74 ± 4.52 | 0.292 |
| TLC, % predicted | 77.17 ± 15.82 | 74.42 ± 10.37 | 77.01 ± 12.70 | 0.844 |
| DLCO, % predicted | 53.54 ± 14.06 | 56.62 ± 20.86 | 55.79 ± 8.60 | 0.893 |
| Chest CT findings at biopsy | ||||
| Ground glass opacity | 15/21 (71.4 %) | 6/14 (42.9 %) | 13/20 (65.0 %) | 0.219 |
| Patchy | 16/21 (76.2 %) | 10/14 (71.4 %) | 14/20 (70.0 %) | 0.899 |
| Reticular opacity | 12/21 (57.1 %) | 11/14 (78.6 %) | 12/20 (60.0 %) | 0.397 |
| Bronchiectasis | 4/21 (19.0 %) | 5/14 (35.7 %) | 8/20 (40.0 %) | 0.315 |
| Pleural thickness | 1/21 (4.8 %) | 4/14 (28.6 %) | 3/20 (15.0 %) | 0.147 |
Distribution of T lymphocyte subsets among different regions of lung tissue
The distribution of CD4+ T lymphocytes is shown in Fig. 2A. The number of CD4+ T lymphocytes per 0.1 mm2 in the follicle, perivascular, interstitial, and peribronchial regions were 161.4 ± 89.0, 61.4 ± 30.6, 40.9 ± 12.0, and 25.9 ± 14.2, respectively. The numbers of CD4+ T cells decreased gradually in the order of the follicle, perivascular, interstitial, and peribronchial regions. The differences in cell counts between each of two different regions were statistically significant (p < 0.001).
Fig. 2.
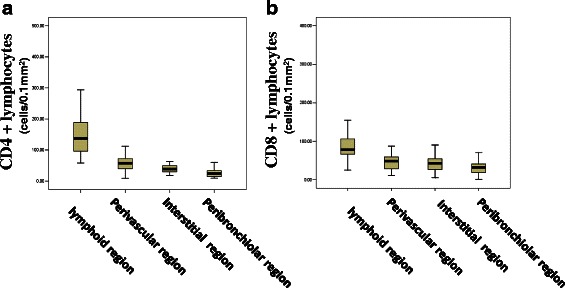
a Distribution of CD4+ T lymphocytes in different regions of lung tissue. The different in CD4+ cell counts between any two regions were statistically significant (p < 0.001). b Distribution of CD8 + T lymphocytes in different regions of lung tissue. CD8+ cell in follicles were much more than those in each of the other three regions (p < 0.001)
The distribution of CD8+ T lymphocytes (Fig. 2B) was similar to that of CD4+ T lymphocytes. The numbers of CD8+ T lymphocytes per 0.1 mm2 in perivascular (47.6 ± 22.7), interstitial (45.7 ± 30.1), and peribronchial (32.5 ± 19.3) regions were not significantly different (p = 0.561). The number of lymphocytes in follicles (96.3 ± 58.4) were much greater than those in each of the other three regions (all p < 0.001).
Distribution of CD4+ and CD8+ T lymphocytes among NSIP subtypes
We analyzed NSIP subtypes as follows: 22 cellular, 28 mixed, and five fibrotic. The distribution of CD4+ and CD8+ T lymphocytes in these subtypes is summarized in Table 4. Perivascular infiltration with CD4+ T lymphocytes was more prominent in patients with the cellular pattern compared with those with the mixed or fibrotic pattern. There was no significant difference in the number of infiltrating CD8+ T lymphocytes among the four anatomical regions.
Table 4.
Distribution of T lymphocytes in patients with different histological patterns
| Tissue | Cellular NSIP (n = 22) | Mixed NSIP (n = 28) | fibrotic NSIP (n = 5) | p value |
|---|---|---|---|---|
| CD4+ T lymphocytes (number/0.1 mm2) | ||||
| Follicle region | 163.37 ± 89.58 | 159.69 ± 94.36 | 161.93 ± 68.14 | 0.990 |
| Perivascular region | 78.12 ± 34.79 | 49.74 ± 22.42 | 53.10 ± 18.17 | 0.003* |
| Interstitial region | 40.85 ± 12.66 | 39.54 ± 11.52 | 38.48 ± 13.97 | 0.894 |
| Peribronchial region | 27.53 ± 15.60 | 25.70 ± 13.82 | 20.10 ± 8.84 | 0.575 |
| CD8+ T lymphocytes (number/0.1 mm2) | ||||
| Follicle region | 123.11 ± 77.81 | 72.62 ± 26.37 | 110.74 ± 36.94 | 0.006 |
| Perivascular region | 57.51 ± 23.43 | 38.91 ± 17.50 | 52.60 ± 29.89 | 0.011 |
| Interstitial region | 57.96 ± 39.81 | 36.26 ± 17.53 | 43.83 ± 18.69 | 0.037 |
| Peribronchial region | 39.11 ± 22.52 | 27.80 ± 16.27 | 29.40 ± 12.50 | 0.111 |
The numbers of CD4+ and CD8+ T lymphocytes cells in the CTD-NSIP (n = 21), NSIP-Ab (+) (n = 14), and NSIP-Ab (−) (n = 20) groups were not significantly different in each of the four anatomical regions (Table 5).
Table 5.
Distribution of T lymphocytes in the CTD-NSIP, NSIP-Ab (+) and NSIP-Ab (−) groups
| CTD-NSIP group (n = 21) | NSIP-Ab (+) group (n = 14) | NSIP-Ab (−) group (n = 20) | P value | |
|---|---|---|---|---|
| CD4+ T lymphocytes (number/0.1 mm2) | ||||
| Follicle region | 181.5 ± 87.2 | 155.4 ± 110.7 | 144.4 ± 73.1 | 0.401 |
| Perivascular region | 70.2 ± 26.8 | 54.5 ± 25.4 | 51.2 ± 27.0 | 0.061 |
| Interstitial region | 42.9 ± 12.5 | 38.2 ± 10.9 | 38.15 ± 12.20 | 0.372 |
| Peribronchial region | 28.8 ± 13.4 | 25.6 ± 13.3 | 26.3 ± 16.1 | 0.989 |
| CD8+ T lymphocytes (number/0.1 mm2) | ||||
| Follicle region | 107.9 ± 72.2 | 102.4 ± 26.1 | 107.8 ± 50.9 | 0.139 |
| Perivascular region | 59.5 ± 23.7 | 46.6 ± 17.4 | 42.7 ± 19.8 | 0.115 |
| Interstitial region | 45.7 ± 23.9 | 33.3 ± 19.5 | 54.2 ± 39.0 | 0.139 |
| Peribronchial region | 36.0 ± 21.6 | 30.2 ± 15.7 | 30.4 ± 19.4 | 0.579 |
T lymphocyte subsets in lung tissue and improved CT findings
After undergoing therapy for 1 year, 25 patients (20 cellular and five mixed patterns) achieved a 50 % improvement in GGO and reticular opacity (CT-group 1). The lesions of 14 patients (all mixed pattern) decreased between 30 % and 50 % (CT-group 2). The lesions of 14 patients (nine mixed and five fibrotic patterns) were reduced by <30 % (CT-group 3). The number of CD4+ T lymphocytes in perivascular tissue in the CT-group 1 was significantly greater compared with those of other two CT-groups (76.5 ± 33.9 vs 49.5 ± 17.3, p = 0.009; 76.5 ± 33.9 vs 43.9 ± 18.4, p = 0.002) (Fig. 3), but not in the other anatomical regions. There was no correlation between the number of CD8+ T lymphocytes and the improvement HRCT findings.
Fig. 3.
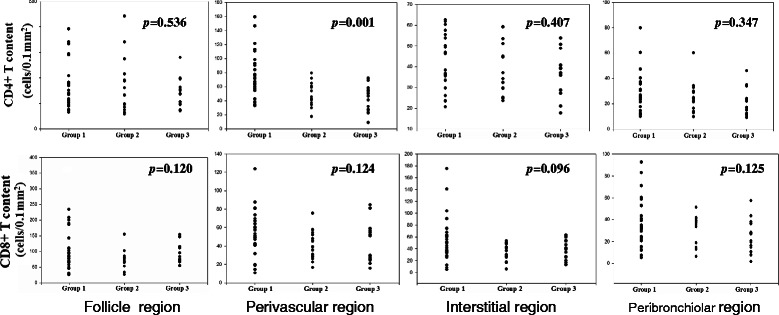
Correlation of T lymphocytes in different regions of tissue and prognosis of NSIP. Group 1: an improvement of ground-glass opacity and reticular opacity over 50 % on HRCT; Group 2: the lesions were still present but decreased between 30–50 % on HRCT; Group 3: the lesions were reduced less than 30 % on HRCT. There is statistical significance of CD4+ lymphocytes perivascular infiltrates among three groups (p = 0.001)
T lymphocyte subsets of lung tissue and pulmonary function tests
Cox multivariate regression analysis revealed that after 12 months of follow-up, FVC was an independent factor for survival (HR, 0.828; 95 % CI, 0.692–0.992; p = 0.040) (Additional file 1: Table S1). There was a marginal correlation of FVC with the number of perivascular CD4 cells (Fig. 4). Among 55 patients, 21 (11 cellular and 10 mixed patterns) achieved an improvement of FVC >10 % (FVC-group 1). No correlation between perivascular CD4 infiltration and DLCO at first visit (p=0.642, r=-0.064) (Additional file 2: Figure s2) and DLCO after 12 months follow up (p=0.134, r=-0.205) (Additional file 3: Figure S2).
Fig. 4.
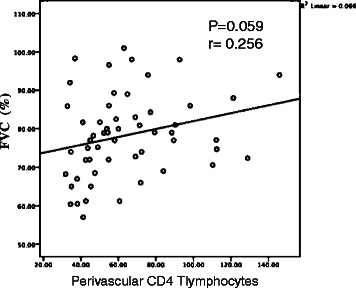
The relationship between perivascular CD4 infiltration and 12 months Follow-up FVC (p = 0.059, r = 0.256)
Nineteen patients (eight cellular, nine mixed, and two fibrotic patterns) achieved improved FVC between 10 % and −10 % (FVC-group 2). The FVC values of 15 patients (three cellular, nine mixed, and three fibrotic patterns) decreased greater than −10 % (FVC-group 3). The number of CD4+ T lymphocytes that infiltrated perivascular tissue in FVC-group 1 was significantly greater than those of the other two groups (77.9 ± 31.5 vs 63.0 ± 23.1, p = 0.056; 77.9 ± 31.5 vs 46.5 ± 12.5, p = 0.001) (Fig. 5).
Fig. 5.
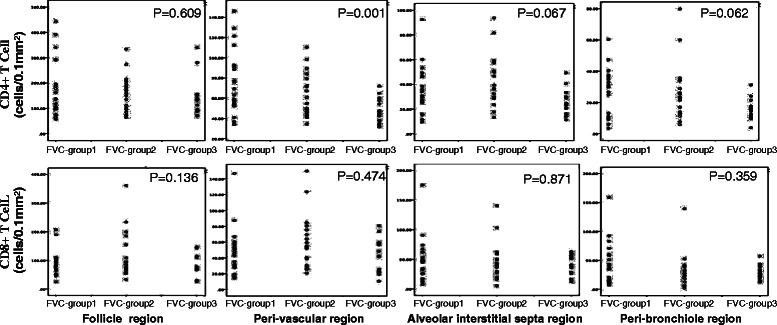
The relationship between CD4 T lymphocytes in perivascular regions of tissue and prognosis of FVC in NSIP patients. There are significant difference among three groups, p = 0.001.FVC-Group1 vs FVC-Group2 p = 0.056; FVC-Group1 vs FVC-Group3 p = 0.000; FVC-Group2 vs FVC-Group3 p = 0.054. FVC-group 1: an improvement of FVC over 10 % after 12 months treatment. FVC-group 2: FVC improved between 10 and −10 % after 12 months treatment. FVC-group 3: FVC worsen over −10 % after 12 months treatment
The densities of CD4+ and CD8+ T lymphocytes T that infiltrated other anatomical compartments was not significantly associated with pulmonary function tests.
The number of CD4+ T lymphocytes infiltrating perivascular tissue influences survival
Cox multivariate regression analysis considered age, sex, and numbers of CD4+ and CD8+ T lymphocytes infiltrating the lungs, and lung function tests (first visit and after 1 year of follow-up). The results revealed that perivascular infiltration of CD4+ T lymphocytes (HR, 0.939; 95 % CI, 0.883–0.999; p = 0.048) was an independent factor for survival (Additional file 1: Table S1).
The densities CD4+ T lymphocytes infiltrating perivascular tissues of all patients were significantly associated with survival time (r = 0.270, p = 0.046) (Fig. 6) compared with those in other anatomical compartments. Further, patients with a much higher density of CD4+ T lymphocytes (≥61 cells/0.1 mm2) in the perivascular compartment survived longer (log-rank test, 4.58; p = 0.040) (Fig. 7). The cutoff value was determined using the ROC curve, and the AUC for patients’ survival was 0.79 (sensitivity 0.615, specificity 0.710).The densities of CD4+ and CD8+ T lymphocytes infiltrating other anatomical compartments were not significantly associated with survival time.
Fig. 6.
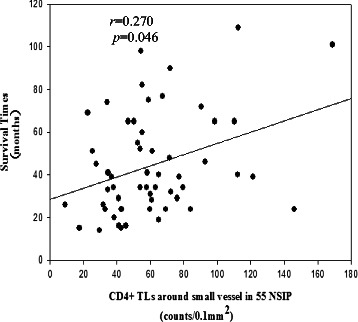
CD4+ T lymphocytes perivascular infiltration were closely related to survival time in NSIP patients. Correlation coefficients were calculated using the Spearman rank method
Fig. 7.
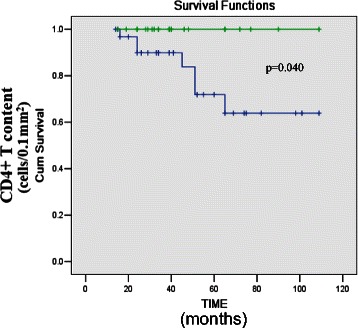
Kaplan-Meier survival curve for 55 NSIP patients grouped by the cell density of CD4 in small vessel region. Green line: ≥61 cells/0.1 mm2. Blue line: < 61 cells/0.1 mm2. There is a significant difference (log-rank test: 4.58, p = 0.04) between the groups
The most important finding of the present study was that the number of CD4+ T lymphocytes that infiltrated perivascular tissue correlated significantly with the prognosis of NSIP.
Immunohistochemical analyses revealed the T lymphocyte subsets infiltrated not only lymphoid follicles and interstitial regions, but perivascular and peribronchial regions as well, which is consistent with the findings of our previous study [7]. In this study, we did not detect a significant difference in T lymphocyte density among cellular, mixed, and fibrotic patterns among the same tissues analyzed here. The small number of patients with the fibrotic pattern might account for these findings, although we show here that there were more lymphocytes in patients with the cellular than with the fibrotic pattern. In contrast, in the present study, we found a correlation between the infiltration of perivascular tissue with CD4+ T cells with prognosis.
The predictors of prognosis of patients with ILD are the results of the pulmonary function test [18–20] and all-cause mortality [27–31]. In the present study, we combined them [29] to analyze perivascular CD4+ T lymphocyte infiltration and clinical prognosis. FVC consistently predicts the mortality of patients with IPF [17–20, 32] and is considered the best marker of chronic disease progression. FVC data now serve as the preferred primary endpoint in trials of therapies IPF [33].
In the present study, we show that FVC was an independent predictor of survival, which is consistent with the results of previous studies [32, 34–37]. When we classified patients according to the change of FVC after the 12-month follow-up, we found that higher numbers of perivascular CD4+ T lymphocytes correlated with improved FVC.
In the present study, all-cause mortality was 23.6 %. Cox multivariate regression analysis revealed that perivascular CD4+ T lymphocyte infiltration was an independent predictor of survival. Survival time correlated with the number of perivascular CD4+ T lymphocytes. Patients with higher numbers of perivascular T lymphocytes in the perivascular region have a better prognosis.
The accumulation of T lymphocytes in tissue is considered a cell-mediated immune reaction to bodily injury [38], particularly in patients with immune dysfunction [39]. The accumulation of perivascular CD4+ T lymphocytes occurs in patients with cutaneous lichen planus [40] and in the muscle tissue of patients with dermatomyositis [41]. Some studies found that T cells might be involved in the pathogenesis of interstitial lung disease. For example, the levels of CXCL9, CXCL10, and CXCL11 in bronchoalveolar lavage fluid indicate that lung fibroblasts induce a Th1-type immune response in patients with NSIP [42].
In an animal model of lung injury, perivascular CD4+ T lymphocytes accumulate in lung tissue [43, 44]. In patients with interstitial pneumonia caused by graft-versus-host disease, interstitial pneumonitis develops primarily from the dissemination of perivascular CD4+ T lymphocytes infiltrates [45]. Immunosuppressive agents such as cyclophosphamide suppress inflammation caused by perivascular T lymphocytes by reducing the T lymphocyte population and ameliorating T lymphocyte function [46]. These findings, taken together with those of the present study, suggest that perivascular infiltration of CD4+ T lymphocytes contributes to the pathogenesis of NSIP. If CD4+ T cells are involved in ILD, treating patients with anti-T cell-specific immunosuppressants such as FK506 and anti-TNF-α antibodies may be justified. For example, patients with ILD, particularly those with CTD-ILD, respond to these agents, [47, 48].
It is very unlikely that lung biopsies will be performed solely to count T-cells when pulmonary function tests and other less invasive measures are available. The implication of our findings related to therapy is that they provide an answer to the question of why anti-T cell treatment is beneficial for patients with ILD.
We recognize that our study is limited by its retrospective design, and B lymphocyte and other inflammatory cells were not investigated. However, to our knowledge, this is the first study to evaluate the relationship between perivascular infiltration of CD4+ T cells and the prognosis of patients with NSIP.
In conclusion, we show here that perivascular infiltration of CD4+ T cells correlated significantly with prognosis and survival. The underlying mechanisms require further study.
Acknowledgments
The authors thank the physicians and supporting staff of the Division of Pulmonary Disease, PUMCH who cared for these patients between 2003 and 2011 and Drs Cartin-ceba Ridrigo and Jay H. Ryu, Division of Pulmonary and Critical Care Medicine, Mayo Clinic for their helpful suggestions for writing the manuscript and discussions about our research. This study was supported by the Ministry of Science and Technology of China’s “Key Projects in the National Science & Technology Pillar Program during the Twelfth Five-year Plan Period” 2011BA11B17.
Abbreviations
- CBC
Complete blood count
- CTD
Connective tissue disease
- DLCO
Diffusing capacity of the lung for carbon monoxide
- ESR
Erythrocyte sedimentation rate
- FVC
Forced vital capacity
- HRCT
High-resolution computed tomography
- ILD
Interstitial lung diseases
- NSIP
Nonspecific interstitial pneumonia
- TLC
Total lung capacity
Additional files
Table S1. The prognostic factors study with multivariate analysis. (DOCX 406 kb)
Figure S1. The relationship between perivascular CD4 infiltration and DLCO (p = 0.642, r = −0.064). (PPT 98 kb)
Figure S2.The relationship between perivascular CD4 infiltration and 12 months follow-up DLCO (p = 0.134, r = −0.205). (PPT 43 kb)
Footnotes
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
Study conceptualization and design: Dr. JHS. Dr. JHS takes responsibility for the content of the manuscript, including the data and analysis. Data collection: Drs LQ, and WZW. Pathological review and immunohistochemical analysis: Drs HRL and WZW. Statistical analyses: Dr. LQ. Manuscript preparation: Drs. JHS and YX. Advice on rheumatologic disease: Dr. WJZ. Advice on radiology: Dr. MWQ. All authors read and approved the final version.
Contributor Information
Ling Qin, Email: qinlingpumch@126.com.
WenZe Wang, Email: wwzvssxy@hotmail.com.
HongRui Liu, Email: lhr1936@163.com.
Yi Xiao, Email: Xy_pumch@sina.com.
MingWei Qin, Email: Qingmingwei@hotmail.com.
WenJie Zheng, Email: wenjiezh@gmail.com.
JuHong Shi, Phone: 86-10-69155028, Email: ShiJH@pumch.cn.
References
- 1.Katzenstein AL, Myers JL. Idiopathic pulmonary fibrosis: clinical relevance of pathologic classification. Am J Respir Crit Care Med. 1998;157(4 Pt 1):1301–1315. doi: 10.1164/ajrccm.157.4.9707039. [DOI] [PubMed] [Google Scholar]
- 2.Selman M, King TE, Pardo A. Idiopathic pulmonary fibrosis: prevailing and evolving hypotheses about its pathogenesis and implications for therapy. Ann Intern Med. 2001;134(2):136–151. doi: 10.7326/0003-4819-134-2-200101160-00015. [DOI] [PubMed] [Google Scholar]
- 3.Gross TJ, Hunninghake GW. Idiopathic pulmonary fibrosis. N Engl J Med. 2001;345(7):517–525. doi: 10.1056/NEJMra003200. [DOI] [PubMed] [Google Scholar]
- 4.Ishii H, Mukae H, Kadota J, Fujii T, Abe K, Ashitani J, et al. Increased levels of interleukin-18 in bronchoalveolar lavage fluid of patients with idiopathic nonspecific interstitial pneumonia. Respiration; international review of thoracic diseases. 2005;72(1):39–45. doi: 10.1159/000083399. [DOI] [PubMed] [Google Scholar]
- 5.Hu H, Stein-Streilein J. Hapten-immune pulmonary interstitial fibrosis (HIPIF) in mice requires both CD4+ and CD8+ T lymphocytes. J Leukoc Biol. 1993;54(5):414–422. doi: 10.1002/jlb.54.5.414. [DOI] [PubMed] [Google Scholar]
- 6.Fireman E, Vardinon N, Burke M, Spizer S, Levin S, Endler A, et al. Predictive value of response to treatment of T-lymphocyte subpopulations in idiopathic pulmonary fibrosis. Eur Respir J. 1998;11(3):706–711. [PubMed] [Google Scholar]
- 7.Qin L, Wang WZ, Liu HR, Xu WB, Qin MW, Zhang ZH, et al. CD4+ and CD8+ T lymphocytes in lung tissue of NSIP: correlation with T lymphocytes in BALF. Respir Med. 2013;107(1):120–127. doi: 10.1016/j.rmed.2012.09.021. [DOI] [PubMed] [Google Scholar]
- 8.American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus Classification of the Idiopathic Interstitial Pneumonias This joint statement of the American Thoracic Society (ATS), and the European Respiratory Society (ERS) was adopted by the ATS board of directors, June 2001 and by the ERS Executive Committee, June 2001. Am J Respir Crit Care Med. 2002;165(2):277–304. doi: 10.1164/ajrccm.165.2.ats01. [DOI] [PubMed] [Google Scholar]
- 9.Travis WD, Costabel U, Hansell DM, King TE, Jr, Lynch DA, Nicholson AG, et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. 2013;188(6):733–748. doi: 10.1164/rccm.201308-1483ST. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO, 3rd, et al. Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010;62(9):2569–2581. doi: 10.1002/art.27584. [DOI] [PubMed] [Google Scholar]
- 11.Vitali C, Bombardieri S, Jonsson R, Moutsopoulos HM, Alexander EL, Carsons SE, et al. Classification criteria for Sjogren’s syndrome: a revised version of the European criteria proposed by the American-European Consensus Group. Ann Rheum Dis. 2002;61(6):554–558. doi: 10.1136/ard.61.6.554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lonzetti LS, Joyal F, Raynauld JP, Roussin A, Goulet JR, Rich E, et al. Updating the American College of Rheumatology preliminary classification criteria for systemic sclerosis: addition of severe nailfold capillaroscopy abnormalities markedly increases the sensitivity for limited scleroderma. Arthritis Rheum. 2001;44(3):735–736. doi: 10.1002/1529-0131(200103)44:3<735::AID-ANR125>3.3.CO;2-6. [DOI] [PubMed] [Google Scholar]
- 13.Medsger TA, Jr, Oddis CV. Classification and diagnostic criteria for polymyositis and dermatomyositis. J Rheumatol. 1995;22(4):581–585. [PubMed] [Google Scholar]
- 14.Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. The European respiratory journal: official journal of the European Society for Clinical Respiratory Physiology. 2005;26(2):319–338. doi: 10.1183/09031936.05.00034805. [DOI] [PubMed] [Google Scholar]
- 15.Wanger J, Clausen JL, Coates A, Pedersen OF, Brusasco V, Burgos F, et al. Standardisation of the measurement of lung volumes. The European respiratory journal : official journal of the European Society for Clinical Respiratory Physiology. 2005;26(3):511–522. doi: 10.1183/09031936.05.00035005. [DOI] [PubMed] [Google Scholar]
- 16.Macintyre N, Crapo RO, Viegi G, Johnson DC, van der Grinten CP, Brusasco V, et al. Standardisation of the single-breath determination of carbon monoxide uptake in the lung. The European respiratory journal : official journal of the European Society for Clinical Respiratory Physiology. 2005;26(4):720–735. doi: 10.1183/09031936.05.00034905. [DOI] [PubMed] [Google Scholar]
- 17.Collard HR, King TE, Jr, Bartelson BB, Vourlekis JS, Schwarz MI, Brown KK. Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2003;168(5):538–542. doi: 10.1164/rccm.200211-1311OC. [DOI] [PubMed] [Google Scholar]
- 18.Flaherty KR, Mumford JA, Murray S, Kazerooni EA, Gross BH, Colby TV, et al. Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia. Am J Respir Crit Care Med. 2003;168(5):543–548. doi: 10.1164/rccm.200209-1112OC. [DOI] [PubMed] [Google Scholar]
- 19.Jegal Y, Kim DS, Shim TS, Lim CM, Do Lee S, Koh Y, et al. Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia. Am J Respir Crit Care Med. 2005;171(6):639–644. doi: 10.1164/rccm.200403-331OC. [DOI] [PubMed] [Google Scholar]
- 20.King TE, Jr, Safrin S, Starko KM, Brown KK, Noble PW, Raghu G, et al. Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis. Chest. 2005;127(1):171–177. doi: 10.1378/chest.127.1.171. [DOI] [PubMed] [Google Scholar]
- 21.Kim MY, Song JW, Do KH, Jang SJ, Colby TV, Kim DS. Idiopathic nonspecific interstitial pneumonia: changes in high-resolution computed tomography on long-term follow-up. J Comput Assist Tomogr. 2012;36(2):170–174. doi: 10.1097/RCT.0b013e31823ed437. [DOI] [PubMed] [Google Scholar]
- 22.Arakawa H, Yamada H, Kurihara Y, Nakajima Y, Takeda A, Fukushima Y, et al. Nonspecific interstitial pneumonia associated with polymyositis and dermatomyositis: serial high-resolution CT findings and functional correlation. Chest. 2003;123(4):1096–1103. doi: 10.1378/chest.123.4.1096. [DOI] [PubMed] [Google Scholar]
- 23.Zhao Z, Liang C, Zhang J, Zhang R, He H. Clinical and imaging findings in patients with severe acute respiratory syndrome. Chin Med J (Engl) 2003;116(7):1104–1105. [PubMed] [Google Scholar]
- 24.Katzenstein AL, Fiorelli RF. Nonspecific interstitial pneumonia/fibrosis. Histologic features and clinical significance. Am J Surg Pathol. 1994;18(2):136–147. doi: 10.1097/00000478-199402000-00003. [DOI] [PubMed] [Google Scholar]
- 25.Ranga V, Kleinerman J. Structure and function of small airways in health and disease. Arch Pathol Lab Med. 1978;102(12):609–617. [PubMed] [Google Scholar]
- 26.Vinay Kumar, Nelso Fausto, Abul Abbas. Robbins & Cotran Pathologic Basis of Disease. 7th ed. Saunders (Amsterdam Holland); 2004:512–3.
- 27.Raghu G, Anstrom KJ, King TE, Jr, Lasky JA, Martinez FJ. Prednisone, azathioprine, and N-acetylcysteine for pulmonary fibrosis. N Engl J Med. 2012;366(21):1968–1977. doi: 10.1056/NEJMoa1113354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Wells AU, Behr J, Costabel U, Cottin V, Poletti V, Richeldi L. Hot of the breath: mortality as a primary end-point in IPF treatment trials: the best is the enemy of the good. Thorax. 2012;67(11):938–940. doi: 10.1136/thoraxjnl-2012-202580. [DOI] [PubMed] [Google Scholar]
- 29.Corte TJ, Goh NS, Glaspole IN, Zappala CJ, Hopkins PM, Wilsher ML. Idiopathic pulmonary fibrosis: is all-cause mortality a practical and realistic end-point for clinical trials? Thorax. 2013;68(5):491–492. doi: 10.1136/thoraxjnl-2012-203114. [DOI] [PubMed] [Google Scholar]
- 30.King TE, Jr, Albera C, Bradford WZ, Costabel U, Hormel P, Lancaster L, et al. Effect of interferon gamma-1b on survival in patients with idiopathic pulmonary fibrosis (INSPIRE): a multicentre, randomised, placebo-controlled trial. Lancet. 2009;374(9685):222–228. doi: 10.1016/S0140-6736(09)60551-1. [DOI] [PubMed] [Google Scholar]
- 31.Noth I, Anstrom KJ, Calvert SB, de Andrade J, Flaherty KR, Glazer C, et al. A placebo-controlled randomized trial of warfarin in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2012;186(1):88–95. doi: 10.1164/rccm.201202-0314OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Latsi PI, du Bois RM, Nicholson AG, Colby TV, Bisirtzoglou D, Nikolakopoulou A, et al. Fibrotic idiopathic interstitial pneumonia: the prognostic value of longitudinal functional trends. Am J Respir Crit Care Med. 2003;168(5):531–537. doi: 10.1164/rccm.200210-1245OC. [DOI] [PubMed] [Google Scholar]
- 33.Raghu G, Collard HR, Anstrom KJ, Flaherty KR, Fleming TR, King TE, Jr, et al. Idiopathic pulmonary fibrosis: clinically meaningful primary endpoints in phase 3 clinical trials. Am J Respir Crit Care Med. 2012;185(10):1044–1048. doi: 10.1164/rccm.201201-0006PP. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Corte TJ, Wort SJ, MacDonald PS, Edey A, Hansell DM, Renzoni E, et al. Pulmonary function vascular index predicts prognosis in idiopathic interstitial pneumonia. Respirology. 2012;17(4):674–680. doi: 10.1111/j.1440-1843.2011.02121.x. [DOI] [PubMed] [Google Scholar]
- 35.Schmidt SL, Nambiar AM, Tayob N, Sundaram B, Han MK, Gross BH, et al. Pulmonary function measures predict mortality differently in IPF versus combined pulmonary fibrosis and emphysema. Eur Respir J. 2011;38(1):176–183. doi: 10.1183/09031936.00114010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Zappala CJ, Latsi PI, Nicholson AG, Colby TV, Cramer D, Renzoni EA, et al. Marginal decline in forced vital capacity is associated with a poor outcome in idiopathic pulmonary fibrosis. Eur Respir J. 2010;35(4):830–836. doi: 10.1183/09031936.00155108. [DOI] [PubMed] [Google Scholar]
- 37.du Bois RM, Weycker D, Albera C, Bradford WZ, Costabel U, Kartashov A, et al. Ascertainment of individual risk of mortality for patients with idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2011;184(4):459–466. doi: 10.1164/rccm.201011-1790OC. [DOI] [PubMed] [Google Scholar]
- 38.Berndt A, Muller G. Occurrence of T lymphocytes in perivascular regions of the lung after intratracheal infection of swine with Pasteurella multocida. Vet Immunol Immunopathol. 1995;49(1–2):143–159. doi: 10.1016/0165-2427(95)05457-H. [DOI] [PubMed] [Google Scholar]
- 39.Hvas J, McLean C, Justesen J, Kannourakis G, Steinman L, Oksenberg JR, et al. Perivascular T cells express the pro-inflammatory chemokine RANTES mRNA in multiple sclerosis lesions. Scand J Immunol. 1997;46(2):195–203. doi: 10.1046/j.1365-3083.1997.d01-100.x. [DOI] [PubMed] [Google Scholar]
- 40.Rana S, Gupta R, Singh S, Mohanty S, Gupta K, Kudesia M. Localization of T-cell subsets in cutaneous lichen planus: an insight into pathogenetic mechanism. Indian J Dermatol Venereol Leprol. 2010;76(6):707–709. doi: 10.4103/0378-6323.72452. [DOI] [PubMed] [Google Scholar]
- 41.Dalakas MC, Hohlfeld R. Polymyositis and dermatomyositis. Lancet. 2003;362(9388):971–982. doi: 10.1016/S0140-6736(03)14368-1. [DOI] [PubMed] [Google Scholar]
- 42.Sumida A, Hasegawa Y, Okamoto M, Hashimoto N, Imaizumi K, Yatsuya H, et al. TH1/TH2 immune response in lung fibroblasts in interstitial lung disease. Arch Med Res. 2008;39(5):503–510. doi: 10.1016/j.arcmed.2008.02.005. [DOI] [PubMed] [Google Scholar]
- 43.Bruder D, Westendorf AM, Geffers R, Gruber AD, Gereke M, Enelow RI, et al. CD4 T Lymphocyte-mediated lung disease: steady state between pathological and tolerogenic immune reactions. Am J Respir Crit Care Med. 2004;170(11):1145–1152. doi: 10.1164/rccm.200404-464OC. [DOI] [PubMed] [Google Scholar]
- 44.Cuttica MJ, Langenickel T, Noguchi A, Machado RF, Gladwin MT, Boehm M. Perivascular T-cell infiltration leads to sustained pulmonary artery remodeling after endothelial cell damage. Am J Respir Cell Mol Biol. 2011;45(1):62–71. doi: 10.1165/rcmb.2009-0365OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Workman DL, Clancy J., Jr Phenotypic analysis of pulmonary perivascular mononuclear infiltrates that occur as a direct result of acute lethal graft-versus-host disease describes the onset of interstitial pneumonitis. Am J Pathol. 1995;147(5):1350–1360. [PMC free article] [PubMed] [Google Scholar]
- 46.Jonsson CA, Erlandsson M, Svensson L, Molne J, Carlsten H. Mycophenolate mofetil ameliorates perivascular T lymphocyte inflammation and reduces the double-negative T cell population in SLE-prone MRLlpr/lpr mice. Cell Immunol. 1999;197(2):136–144. doi: 10.1006/cimm.1999.1570. [DOI] [PubMed] [Google Scholar]
- 47.Takada K, Nagasaka K, Miyasaka N. Polymyositis/dermatomyositis and interstitial lung disease: a new therapeutic approach with T-cell-specific immunosuppressants. Autoimmunity. 2005;38(5):383–392. doi: 10.1080/08916930500124023. [DOI] [PubMed] [Google Scholar]
- 48.Brunasso AM, Aberer W, Massone C. New onset of dermatomyositis/polymyositis during anti-TNF-alpha therapies: a systematic literature review. Sci World J. 2014;2014:179180. doi: 10.1155/2014/179180. [DOI] [PMC free article] [PubMed] [Google Scholar]