

Abstract
Both youngsters and adults with same-sex attraction are at greater risk for negative health outcomes. Despite mounting efforts to determine the biological background, a satisfactory conclusion has not been reached and there is a need to explore alternate factors like functioning of thyroid system during pregnancy. A retrospective chart review was undertaken of 790 eligible children and adolescents who had been admitted to child psychiatry between 2005 and 2013. This population consisted of 520 (65%) males and 270 (35%) females, aged 8 to 17 years. Fifteen mothers (1.8%) were found to have a history of thyroid dysfunction during pregnancy. Sixteen youngsters (2%) had a history of same-sex attraction. Twelve overlapping cases with both same-sex attraction and maternal thyroid dysfunction during pregnancy were identified, which was extremely significant (P<0.0001, by Fisher’s exact test). The association was also significant for each sex (P<0.0001, by Fisher’s exact test). There is evidence that thyroid gland plays a crucial and decisive role in determining sexual orientation in people. Maternal thyroid dysfunctions during pregnancy may result in homosexual orientation in the offspring.
Key words: Sexual orientation, homosexuality, thyroid diseases, prenatal exposure delayed effect, adolescents
Introduction
Despite positive changes in professional definitions, such as removal of homosexuality from DSM in 1973,1 deviations from gender specific heterosexual development still constitute a reason for concern for most of the parents. Unique stressors associated with homosexuality such as stigma, discrimination and bully victimization may adversely affect mental health of young individuals having same-sex attraction.1 Review of relevant literature reveals that people having same-sex attraction are at higher risk of mental disorder, suicidal ideation, substance misuse, and deliberate self-harm than heterosexual people.2 Gay youths are more likely to engage in school refusal, runaway behavior and subsequent homelessness, prostitution and sexually transmitted diseases.3 While it is true that a great majority of people with same-sex attraction do not report any problem relating to their sexual behavior, there is also a significant amount of suffering as well.1,4 It is important to bear in mind that human history is loaded with accounts of severe persecution of individuals with same-sex attraction. It was not until the second half of the 20th century that most influential European countries decriminalized homosexual activity.4 Even today, in at least 76 countries, consensual same-sex relationships are considered as criminal offences punishable by imprisonment and even death, in at least five countries.5 Thus, the medical profession has a duty to alleviate this suffering in all legitimate ways possible. Besides fostering greater tolerance of homosexuality on behalf of society, clinicians are required to prevent negative health outcomes associated with it which may be better addressed by understanding the roots of homosexual behavior.
There is a great deal of research that tries to identify biological factors influencing same-sex orientation. It is suggested that an individual’s sexual orientation is determined by early biological events generated by genes and prenatal sex hormones, both of which hardwire brain morphology.6 In regard to heritable factors, despite several family, twin and molecular studies, much remains to be known about the genetics of human homosexuality.7 Although natural selection favors heterosexuality for transmission of genes from one generation to the next, persistence of homosexuality in a small but consistent percentage of the human population is of question.8
The prenatal androgen model, which has become a cliché in the field, argues that homosexuality in men is due to under-exposure to prenatal androgens and in women, due to over-exposure.9 Attempts to support the model included hormone measurements, animal experimentations and studies of rare disorders (i.e., congenital adrenal hyperplasia and testicular feminization) all of which revealed inconsistent results.10 In the following surge of research in prenatal androgen model, indirect consequences of prenatal hormone impact, such as digit ratio, fingerprint patterns and oto-acoustic emissions have been studied, without reaching definitive conclusions.9 It is warranted that prenatal androgenization is essential for male gender identity development, but apparently not decisive.11 Thus, researchers and clinicians should think about what else may play a role in this puzzling area. The thyroid gland and its hormones merit attention in this regard. The thyroid gland, located in front of the neck, produces two related hormones, thyroxine (T4) and triiodothyronine (T3). These hormones have a critical role in cell differentiation during development and help maintain thermogenic and metabolic homeostasis in the adults.12 Thyroid disorders are highly prevalent in the population and mostly affect women in childbearing age.13 In pregnancy, thyroid gland displays mild to moderate enlargement because of increased physiological demands. Thyroid function is altered by 4 factors in pregnancy: i) the transient increase in human chorionic gonadotropin (hCG) during the first trimester, which cross-reacts with thyroid-stimulating hormone (TSH) receptor; ii) the estrogen-induced rise in thyroxine-binding globulin (TBG) which is the major transport protein for thyroid hormone; iii) increased autoimmunity; and iv) increased urinary iodide clearance, which can cause impaired thyroid hormone production in areas of low iodine supply.12,14-17 Consequently, the levels of both T3 and T4, the major hormones released by the thyroid, increase by ~50% and serum TSH levels decrease in the first trimester and increase in the second and third trimesters.17
Autoimmunity and altered iodine status together account for the majority of abnormalities in pregnancy. Thyroid autoimmunity is present in 5-15% of women of childbearing age.14 Hypothyroidism may affect up to 3% of all pregnant women, while hyperthyroidism is less than 1%. Subclinical forms of thyroid disorders is also a growing concern as undiagnosed cases may result in serious consequences.18 It is a well-established fact that thyroid hormones are essential for both fetal and post-natal neurodevelopment and for the regulation of neuropsychological function in human beings.19 Either due to iodine deficiency or autoimmune thyroid dysfunction, reduction of circulating maternal thyroid hormones has been found to result in lower IQ in infants and young children in several retrospective and prospective studies.15 During gestation, maternal thyroid hormones may also play a role in determining behavior in the offspring.19 This is expected to include behavior relating to sexual attraction, however, there is no study focusing on this issue. In one related study by Ellis and Hellberg,20 fetal exposure to thyroid medications and diet pills was found to be significantly related to homosexual orientation in female offspring. Another recent study mentioned autoimmune thyroid diseases among a group of autoimmune diseases that were found at increased rates in same-sex married Danish individuals.21 In the present study, it was aimed to investigate the association between history of thyroid dysfunction in pregnancy and same-sex attraction/gender nonconformity in the offspring. A child psychiatry cohort was explored to find cases with overlapping conditions.
Materials and Methods
This study was a retrospective chart review of patients evaluated by the author-clinician between 2005 to 2013 in 4 outpatient settings in Istanbul; 2 of them attached to Marmara University and the remaining ones as private clinics. The review of the charts of 2005-2013 period was performed in 2013. Patients were mostly self-referrals and school-referrals. During the reviewed period, all diagnoses had been based on DSM-IV criteria.22 Considering the average age of the onset of same-sex attractions,6 the charts of the children and adolescents aged 8 to 17 years were used in the study. Patients with mental retardation, autism and psychosis were excluded from the review. The excluded children with mental retardation were noted separately in case there was a history of thyroid dysfunction. Children who had a history of sexual abuse and physical abuse were also excluded. Charts with missing perinatal information were not included in the study. Although the study was a retrospective one, the approval of local ethics committee of Marmara University Medical School was obtained. Parents’ consent for treatment involved consent for the use of their data for audit and research purposes provided that their identity not to be disclosed. After the cases with overlapping conditions had been identified (n=12), a second-line consent for the use of their data in a study correlating complaints of the child with pregnancy history, was asked in telephone interviews and none of the mothers refused to participate. More detailed and updated data about the course of their thyroid dysfunction was collected in those interviews. A respectful approach to the subjects has been adopted because of the sensitivity of the topic. In accordance with current clinical practice parameters,1 the term same-sex attraction was reserved for the youngsters who display such behavior whereas the term childhood gender nonconformity was rather indicated for preadolescent cases who had behavior that fell outside gender norms.
Patient records, kept as electronic office files were reviewed consecutively beginning from the earliest admission until the last one, at the end of October 2013. Besides this, since all files are electronically searchable, all files were explored using relevant search terms in Turkish and English, relating to pregnancy thyroid dysfunction in the mothers and same-sex attraction/gender nonconformity in the children. In order to prevent possible biases while searching for relevant cases, another clinician who had had no responsibility for any of the patients between 2005 to 2013 also reviewed the files. Based on this criteria, only the data of cases on which both clinicians were in agreement were used.
Statistical analysis
The Statistical Package for the Social Sciences version 15 was used for statistical analysis (SPSS 15, Chicago, IL, USA). Fisher’s exact test and T-tests were conducted for the analyses of the data. The prevalence of same-sex attraction/gender nonconformity in the group of children having positive maternal history in pregnancy was compared with the total sample. The comparison was also repeated with smaller control groups derived from the total sample. We also used logistic regression analysis to assess variables predicting same-sex attraction/gender nonconformity. The level P<0.05 was taken as the cut-off value for statistical significance of results.
Results
A total of 790 charts were identified as eligible for further search in this study. This group consisted 520 male children (65%) and 270 (35%) female children, with a mean age of 12.18±2.81.
The review of this archive revealed 39 mothers with thyroid dysfunction either in pregnancy, or currently. From this sample, twenty-four (61%) mothers reported current, 5 (12%) mothers reported only in pregnancy and 10 (25%) mothers reported both in pregnancy and current thyroid problem. In sum, 15 (38%) mothers reported to have thyroid dysfunction during pregnancy. The mean maternal age at delivery was 28.66±4.78. No statistically significant difference existed between the mean delivery age of mothers who had thyroid problem in pregnancy and those who did not. Any thyroid problem was found to affect 4.9% of the entire population (n=790), whereas the rate was 1.8% for pregnancy thyroid problem. The most common principal diagnoses given to the children of mothers in this group were attention deficit hyperactivity disorder (n=14; 35%) and depression (n=10; 25%).
The mothers who had pregnancy thyroid dysfunction (n=15) reported their diagnoses as either hypothyroidism, goiter or Hashimoto disease whereas three mothers could only recall the presence of a thyroid disorder. Among the mothers interviewed, only three reported medication use in pregnancy which were thyroid hormones.
We have identified 16 children and adolescents in the total population who had behavior indicative of same-sex attraction/gender nonconformity. Prevalence rate in the entire population was 2%. Of these children, 13 were males and 3 were females, having a mean age of 13.18±1.83. The sex ratio and mean age were similar to the total sample. Different diagnoses were given to these children, except for three, for whom no diagnosis was applicable. The percentage comparison of same-sex attraction/gender nonconformity in the focus group with other control groups are presented in Figure 1. For each group compared, there was a significant association between the history of thyroid dysfunction in pregnancy and same-sex attraction/gender nonconformity in the children born to these women (P<0.0001, by Fisher’s exact test). The association was also significant for each sex (P<0.0001, by Fisher’s exact test). In logistic regression analysis, no other factor has been found to influence same-sex attraction/gender nonconformity. Table 1 shows some of the main characteristics of the cases with overlapping conditions. Homophobic bullying, which targets children with same-sex attraction/gender nonconformity appeared to be a common problem (n=7; 58%). In Table 1, relevant data regarding children’s thyroid status was also provided.
Figure 1.
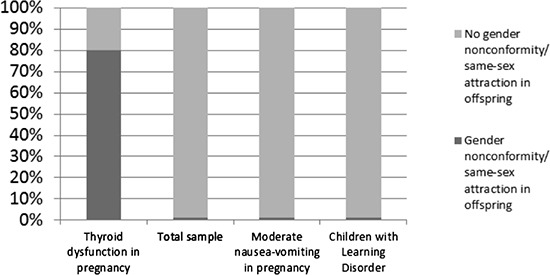
Percentage comparison of same-sex attraction in the focus group with other control groups.
Table 1.
Characteristics of the cases presenting with same-sex attraction/gender nonconformity and history of maternal thyroid dysfunction in pregnancy.
| Case | Sex | Age | Principal psychiatric diagnosis | Records relating to same-sex attraction/gender non-conformity | Reported pregnancy thyroid dysfunction in pregnancy | Medication used for thyroid dysfunction | Additional notes |
|---|---|---|---|---|---|---|---|
| 1 | M | 15 | No diagnosis | Effeminate behavior; plucking eyebrows; subject to homophobic bullying at school | Goiter | No - |
- |
| 2 | M | 14 | Major depression | Effeminate behavior; in love with a male friend; subject to homophobic bullying at school | Hashimoto thyroiditis | No | - |
| 3 | M | 10 | Anxiety disorder | Shaving body hair; subject to homophobic bullying at school | Hypothyroidism | Yes | - |
| 4 | M | 11 | Learning disorder | Effeminate behavior; subject to homophobic bullying at school | Hashimoto thyroiditis | Yes | - |
| 5 | M | 11 | Asperger disorder | Effeminate behavior; subject to homophobic bullying at school | Hypothyroidism | No | History of postnatal thyroid hormone use for 2 months |
| 6 | M | 9 | ADHD | Parental concerns regarding sexuality; seen peeping other boys’ genitals on several occasions | Hashimoto thyroiditis | Yes | - |
| 7 | M | 17 | No diagnosis | Sexual activity with a male friend; admits same-sex orientation | Goiter | No | - |
| 8 | M | 13 | No diagnosis | Sexual play with a male friend; admits same-sex orientation | Hypothyroidism | No | Anti-thyroid medication use before pregnancy |
| 9 | M | 11 | Anxiety disorder | Sexual play with other boys; subject to homophobic bullying at school | Hypothyroidism | No | - |
| 10 | M | 17 | Major depression | Effeminate behavior; in love with a male friend; previously subject to homophobic bullying at school | Hypothyroidism | No | - |
| 11 | F | 16 | Anxiety disorder | An affair with a masculine girl | Hashimoto thyroiditis | No | Also had Hashimoto thyroiditis |
| 12 | F | 17 | ADHD | Sexual activity with a female friend; admits bisexual orientation | Hashimoto thyroiditis | No | Also had Hashimoto thyroiditis |
No child was identified as having both mental retardation and perinatal history of thyroid dysfunction. In excluded cases, no child with same-sex attraction existed.
Discussion and Conclusions
In this study, a significant association between thyroid dysfunction in pregnancy and same-sex attraction/gender nonconformity in the offspring was found. Several implications may be derived from this finding. To the best of my knowledge, this study is the only one that explored this association with a focused objective and found positive results.
An initial point of note is that the prevalence of thyroid disorders in the study population, both currently and in pregnancy, is far less than the reported prevalence rates that may be expected.14-17 It is possible to hypothesize that only certain patients had received medical attention in pregnancy. Current case-finding procedures are estimated to fail to identify many pregnant women with subclinical and overt hypothyroidism.17 Thus, there may be additional cases who remain undiagnosed.
Also, a significant rate of children and adolescents with same-sex attraction may remain to be identified. First of all, same-sex interest may manifest later than the mean age we found in this population. Second, sexual behavior understandably may be kept private and secret. Third, as can be seen in Table I, most subjects were male children who assume a feminine role. Active or manly same-sex attraction was not a reason for referral.
Similarly, behavioral manifestations of same-sex attraction in girls were lower than population estimates in this study. This finding of sex difference in referral rates is in line with previous reports of gender issues.23 Despite these difficulties, there existed sufficient cases to show the magnitude of underlying pathology.
The assumption that same-sex interest is caused by child sexual abuse is no longer supported.24 Situational homosexuality, which occurs when heterosexual partner is inaccessible, like in prisons, constitutes only a small group.4 Therefore, it is likely that the index group in our study represents general characteristics of individuals with same-sex attraction in a population. As 3 children had not received any psychiatric diagnosis and the remaining children’s disorders were either temporary or common ones seen in child psychiatry practice, this may call for further research about the generalizability of the present findings to general population. On the other hand, although the statistical association we found in this study is such strong, there were 3 cases who had no sex attraction/gender nonconformity despite maternal thyroid history dysfunction in pregnancy. Depending on the timing, duration, severity and type of maternal thyroid dysfunction, there may be a group of children who could survive the negative impact on behavior.
As described in the Methods section in accordance with current clinical practice parameters,1 although two different terms, gender nonconformity and same-sex attraction were used to identify the explored behavior, all cases have been merged in a single group as can be seen in Table 1. There is agreement that gender nonconformity often is a developmental precursor of homosexuality in males and it is also associated with negative health outcomes.1 The present study provides further evidence that both conditions are developmentally linked. On the other hand, in all youngsters in Table 1, the extent of same-sex attraction was beyond the limits of sexual experimentation which is a feature of adolescent development.6
A particular point is that, no case had been diagnosed as having gender identity disorder, which is a different developmental pathway. However, gender identity disorder in the offspring should also be considered among the behavioral consequences of prenatal thyroid dysfunction and may be explored in further research.
In contrast to what may be expected, no case was identified as having low IQ because of early thyroid dysfunction, which is a well-established consequence. It is evident that the impact of early thyroid dysfunction on developing neurons produces more common but not less serious results which manifest later in life at a behavioral level.
It is worth thinking why the association identified in this study remained undetected before. First of all, as different specialties are involved in this model, namely endocrinology, obstetrics, pediatrics, child and adult psychiatry, grasping the whole picture may be elusive. However, unlike other disciplines, child psychiatry has a unique advantage of being able to collect data for both parents and offspring. Secondly, the impact of thyroid dysfunction on sexual behavior unfolds after so many years, even after a couple of decades. This is in contrast to developmental disorders which become evident earlier in life. Thirdly, because of understandable sexual privacy and secrecy in the context of strong moral, cultural and religious values, even very close relatives of an individual with same-sex attraction may be unaware of the condition. Fourth, a significant rate of pregnant women with thyroid dysfunction may go undiagnosed, or may have subclinical forms of thyroid dysfunction. All of these factors may contribute to the issue remain unsolved.
All possible explanations of the findings will be based on thyroid dysfunction during pregnancy, as it is the most likely predictor of same-sex attraction in the majority of cases. Either present before pregnancy or developed afterwards, thyroid diseases may result in diminished supply of thyroid hormones which are crucial for optimal brain development. Developing brain areas, which will be responsible for determining heterosexual orientation remain undifferentiated without the influence of essential thyroid hormones. As the timing, duration, severity and type of insult during development determine the specific consequence,25 the characteristics of same-sex attraction (i.e., bisexual or entirely homosexual) in the offspring are expected to be shaped by these factors. Once the timely effects of specific hormones are missed, these functions may have been never recovered in a lifetime. Besides, these areas may also be overly sensitive to the availability of the thyroid hormones. We should also consider whether there is such a mechanism in the brain that in case thyroid hormones are low, less vital neurons are sacrificed to save more crucial ones to preserve optimal intelligence. Further to these explanations, we need to think about the possible role of autoimmunity in the generation of deviant sexual orientation, as Hashimoto thyroiditis was quite common in the index group. It is known that, in Hashimoto thyroiditis, TSH receptor blocking antibodies are capable of crossing the placenta and affecting the fetal thyroid.16 It is possible to hypothesize that besides lowering thyroid hormone levels, various antibodies may attack sensitive areas in the developing fetal brain and may produce permanent effects. Finally, there is also possibility that maternal thyroid dysfunction may impact prenatal androgen system and generate permanent consequences. All of these issues require further extensive research.
In Table 1, there are cases having same-sex attraction/gender nonconformity despite medication history addressing thyroid dysfunction during pregnancy. Although more detailed medication histories were not available, thyroid hormone use during pregnancy in the index cases will be discussed in two ways that i) medication use rate is low and ii) simple supply of thyroid medication may be ineffective in altering the pathogenesis if basic underlying factor is autoimmunity. At this point, I am going to refer to the study by Ellis and Hellberg, cited above.20 The most significant finding in that study was increased prenatal use of thyroid hormone and diet pills in the mothers of young females with homosexual/bisexual orientation. According to the authors, thyroid and dieting medications may trigger immune reactions that may result in homosexual/bisexual orientation in the female offspring. However, correction of hypothyroidism with synthetic levothyroxine is known to be safe,26 and in the present study there was no history of medication use in the majority of the cases. Thus, it appears that it is not the medication use that leads to same-sex attraction, but the basic thyroid dysfunction itself. Definitely, as there may be several cases who never come into medical attention, the subjects with medication use represent only a sub-group. I will also argue that a broad spectrum of thyroid disorders should be considered rather than only immune conditions. Finally, failure to find significant results in male subjects may stem from methodology: both sexes are affected in the present study as might be expected. Finally, a recent study that reported increased rates of certain autoimmune diseases in homosexual individuals but no increased overall risk can best be explained with the mechanism presented in our study.21
From a child psychiatry point of view, it is clearly visible that there is a new kid in the playground. What was found in the present study is obviously a challenge to pre-existing theories about homosexuality and there’s sufficient ground to introduce a new model. The prenatal androgen model, which refers to rare disorders such as congenital adrenal hyperplasia and testicular feminization for explanation, is going to be affected by the decisive role of thyroid hormones in sexual orientation. The genetic model is also under scrutiny. It is not surprising to find significant results for homosexuality in genetic studies as prevalent thyroid disorders (i.e., Hashimoto thyroiditis) have a very strong genetic background. In the search for possible factors for the persistence of homosexuality in human populations, thyroid disorders provide a reasonable explanation as they are prevalent and more common in women.12 Fraternal birth order effect, which refers to increasing odds of homosexuality in having older brothers,27 may simply reflect continuously decreasing capacity in thyroid disorders in subsequent pregnancies. In sum, the findings of this study and review of the preexisting views indicate the birth of prenatal thyroid theory to explain the underlying dynamics of same-sex attraction in human beings.
There is a need to add relevant statements for the ethical position of this study and manuscript, as it is known that there exist views that oppose scientific study on the causes of same-sex attraction. We believe that clinicians as researchers do not have an option to suppress data, experience or insight gained in their practice. If there is a medical risk factor that may highly predict certain behaviors, clinical researchers cannot remain silent and cannot keep it hidden, which apparently constitutes an ethical violation. Individuals with same-sex attraction have the right to know the possible origins of their behavior which cannot be denied by making decisions on behalf of them. Apparently, in this age of information, this right extends to any individual who would like to be interested. People at childbearing age, for instance, may not be accepting homosexuality, because they don’t want offspring that is likely to be persecuted and susceptible to negative health sequelae. On the other hand, we are well aware that abuse of scientific knowledge is always a potential risk and we must be prepared to struggle against it at all times.
A number of limitations exist in this study. First, the prenatal medical data relied on parental recall. However, as thyroid disorders are chronic in nature, the mothers may be pretty bright in reporting about this. Also, the parents and the children had not been questioned systematically about issues of sexual behavior. The retrospective design allows only use of data collected for clinical management. However, such limitations are inevitable in investigating an issue in which cause and effect are apart in time.
Based on the insight gained from this work, further studies may be conducted with attention to methodology. Following phase of research is expected to focus on confirmation of present findings. Then, neurobiology of fetal impact and improvement of endocrinological care during pregnancy may be studied. Using current case-finding procedures, many pregnant women with subclinical and overt hypothyroidism may remain undetected.17 On the other hand, neither targeted case finding nor universal screening have been shown to lead to improved outcomes in population-based studies.17 In light of this study, screening for thyroid dysfunction in pregnancy should be rethought, which is controversial in current guidelines.17 Outcome criteria for intervention studies should be redefined considering same-sex attraction unfolding much later. Newer intervention strategies may be needed as same-sex attraction is a special kind of consequence. Principles of endocrine counseling to couples before conception may be established. Psychological effects and therapeutic management of awareness of thyroid impact in affected individuals, either as mother or as offspring, may become a field of highest priority. A final note is that medical implications should always be developed with multi-disciplinary consensus. More convincing neurobiological evidence will be a positive step towards social acceptance and greater adaptation of young and adult people with same-sex orientation. Violence and prejudice against individuals with same-sex attraction will inevitably lose part of its ground. With further medical understanding and awareness, all medical specialties have to do their best to help all affected people in their potential problems. There is a real need to review all relevant cultural, legal, political and even historical aspects of the topic from the medical standpoint explained in this article. It is only with the rule of science and knowledge that certain misconceptions and misperceptions will be cleared up and humankind will benefit.
References
- 1.Adelson SL, American Academy of Child and Adolescent Psychiatry (AACAP), Committee on Quality Issues (CQI). Practice parameter on gay, lesbian, or bisexual sexual orientation, gender nonconformity, and gender discordance in children and adolescents. J Am Acad Child Adolesc Psychiatry 2012;51:957-74. [DOI] [PubMed] [Google Scholar]
- 2.King M, Semlyen J, Tai SS, et al. A systematic review of mental disorder, suicide, and deliberate self harm in lesbian, gay and bisexual people. BMC Psychiatry 2008;8:70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wells SA. The health beliefs, values, and practices of gay adolescents. Clin Nurse Spec 1999;13:69-73. [DOI] [PubMed] [Google Scholar]
- 4.Pickett BL. Historical dictionary of homosexuality. Lanham: The Scarecrow Press Inc.; 2009. [Google Scholar]
- 5.The Office of the United Nations High Commissioner for Human Rights. Fact sheet: criminalization. Available from: https://unfe-uploads-production.s3.amazonaws.com/unfe-34-UN_Fact_Sheets_v6_-_Criminalization.pdf [Google Scholar]
- 6.Perrin EC, Cohen KM, Gold M, et al. Gay and lesbian issues in pediatric health care. Curr Probl Pediatr Adolesc Health Care 2004;34:355-98. [DOI] [PubMed] [Google Scholar]
- 7.Rodríguez-Larralde A, Paradisi I. [Influence of genetic factors on human sexual orientation. Review]. Invest Clin 2009;50:377-91. [Article in Spanish]. [PubMed] [Google Scholar]
- 8.Muscarella F, Fink B, Grammer K, Kirk-Smith M. Homosexual orientation in males: evolutionary and ethological aspects. Neuro Endocrinol Lett 2001;22:393-400. [PubMed] [Google Scholar]
- 9.Rahman Q. The neurodevelopment of human sexual orientation. Neurosci Biobehav Rev 2005;29:1057-66. [DOI] [PubMed] [Google Scholar]
- 10.Banks A, Gartrell NK. Hormones and sexual orientation: a questionable link. J Homosex 1995;28:247-68. [DOI] [PubMed] [Google Scholar]
- 11.Gooren L. The biology of human psycho-sexual differentiation. Horm Behav 2006;50:589-601. [DOI] [PubMed] [Google Scholar]
- 12.Jameson IJ, Weetman AP. Disorders of the thyroid gland. Kasper DL, Braunwald E, Fauci AS, et al. eds. Harrison’s principles of ınternal medicine. 16th ed. New York: McGraw-Hill Book Company; 2005. pp 2104-2127. [Google Scholar]
- 13.Wang C, Crapo LM. The epidemiology of thyroid disease and implications for screening. Endocrinol Metab Clin North Am 1997;26:189-218. [DOI] [PubMed] [Google Scholar]
- 14.Kennedy RL, Malabu UH, Jarrod G, et al. Thyroid function and pregnancy: before, during and beyond. J Obstet Gynaecol 2010;30:774-83. [DOI] [PubMed] [Google Scholar]
- 15.Lazarus JH. Thyroid function in pregnancy. Br Med Bull 2011;97:137-48. [DOI] [PubMed] [Google Scholar]
- 16.Parkes IL, Schenker JG, Shufaro Y. Thyroid disorders during pregnancy. Gynecol Endocrinol 2012;28:993-8. [DOI] [PubMed] [Google Scholar]
- 17.Stagnaro-Green A, Pearce E. Thyroid disorders in pregnancy. Nat Rev Endocrinol 2012;8:650-8. [DOI] [PubMed] [Google Scholar]
- 18.Casey BM. Subclinical thyroid dysfunction during pregnancy. Clin Obstet Gynecol 2011;54:493-8. [DOI] [PubMed] [Google Scholar]
- 19.Williams GR. Neurodevelopmental and neurophysiological actions of thyroid hormone. J Neuroendocrinol 2008;20:784-94. [DOI] [PubMed] [Google Scholar]
- 20.Ellis L, Hellberg J. Fetal exposure to prescription drugs and adult sexual orientation. Pers Individ Dif 2005;38:225-36. [Google Scholar]
- 21.Frisch M, Nielsen NM, Pedersen BV. Same-sex marriage, autoimmune thyroid gland dysfunction and other autoimmune diseases in Denmark 1989-2008. Eur J Epidemiol 2014;29:63-71. [DOI] [PubMed] [Google Scholar]
- 22.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC: American Psychiatric Association; 1994. [Google Scholar]
- 23.Zucker KJ, Seto MC. Gender identity and sexual disorders. Rutter M, Bishop DWM, Pine DS, et al., eds. Rutter’s child and adolescent psychiatry. 5th ed. Oxford: Blackwell Publishing Ltd; 2008. pp. 864-881. [Google Scholar]
- 24.Moser C, Kleinplatz PJ, Zuccarini D, Reiner WG. Situating unusual child and adolescent sexual behavior in context. Child Adolesc Psychiatr Clin N Am 2004;13:569-89. [DOI] [PubMed] [Google Scholar]
- 25.Fowden AL, Giussani DA, Forhead AJ. Intrauterine programming of physiological systems: causes and consequences. Physiology (Bethesda) 2006;21:29-37. [DOI] [PubMed] [Google Scholar]
- 26.Okosieme OE. Thyroid hormone replacement: current status and challenges. Expert Opin Pharmacother 2011;12:2315-28. [DOI] [PubMed] [Google Scholar]
- 27.Blanchard R. Fraternal birth order and the maternal immune hypothesis of male homosexuality. Horm Behav 2011;40:105-14. [DOI] [PubMed] [Google Scholar]