

Abstract
Tracheomegaly has not been reported in amyotrophic lateral sclerosis (ALS). Herein, the authors report a case of tracheomegaly secondary to tracheotomy tube cuff in a patient with ALS. To our knowledge, this is the first report of an ALS patient with tracheomegaly and of tracheomegaly being associated with tracheotomy tube cuff and home tracheotomy mechanical ventilator.
The clinician should consider the possibility of tracheomegaly in the differential diagnosis, if a patient with ALS develops repeat air leakage around the tracheotomy tube or rupture of tracheotomy tube cuff.
INTRODUCTION
Tracheomegaly is an extremely rare condition characterized by marked dilatation of the trachea.1–3 Tracheomegaly has been reported in cases of congenital disease, connective tissue disease, and acquired conditions.1–3 The pathogenesis of tracheomegaly in amyotrophic lateral sclerosis (ALS), however, is unclear. Herein, we report a case of tracheomegaly secondary to tracheotomy tube cuff in a patient with ALS.
CASE REPORT
A 51-year-old man was referred to our hospital for dyspnea and recurrent air leakage around the tracheotomy tube of recent origin. Fourteen years ago, he was diagnosed with ALS. The patient was a nonsmoker with no history of alcohol consumption. The patient had a tracheotomy 4 years ago for respiratory failure, which required prolonged all-day mechanical ventilation. There were instances of respiratory distress that occurred after either air leakage around the tracheotomy tube or rupture of tracheotomy tube cuff. The cause of these episodes was attributed to a dilated trachea, which led to air leakage around the tracheotomy tube, an increased need for air volume to ensure an adequate cuff seal, and trouble in maintaining mechanical ventilation. After tracheotomy, we performed chest computed tomography (CT) scan annually. Before this event, the diameter of the trachea was unremarkable.
A chest radiograph and CT scan revealed tracheomegaly, mainly at the level of the tracheotomy tube cuff (Figs. 1 and 2). The maximum transverse diameter of the trachea was measured to be 43 mm and 42 mm in the axial and sagittal sections, respectively (Fig. 1). On three-dimensional CT scans (Fig. 2), the shape and diameter of tracheal dilatation matched those of tracheotomy tube cuff.
FIGURE 1.
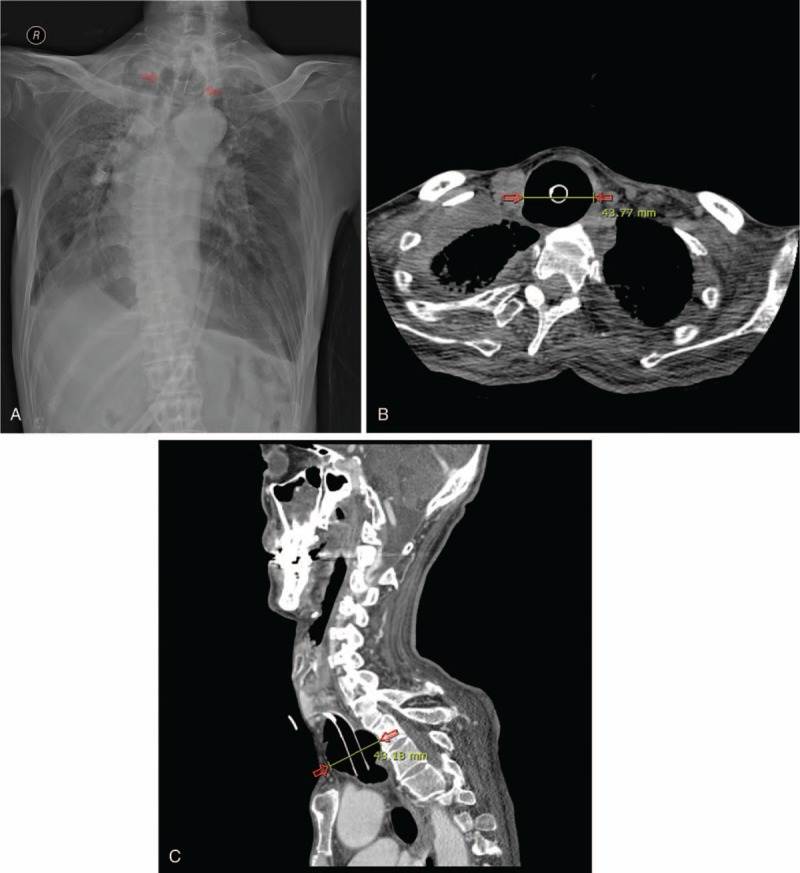
(A) Anteroposterior radiograph of the chest shows marked tracheomegaly (arrows). Computed tomography scans in axial (B) and sagittal (C) planes show marked tracheomegaly at the level of the tracheotomy tube cuff (arrows).
FIGURE 2.
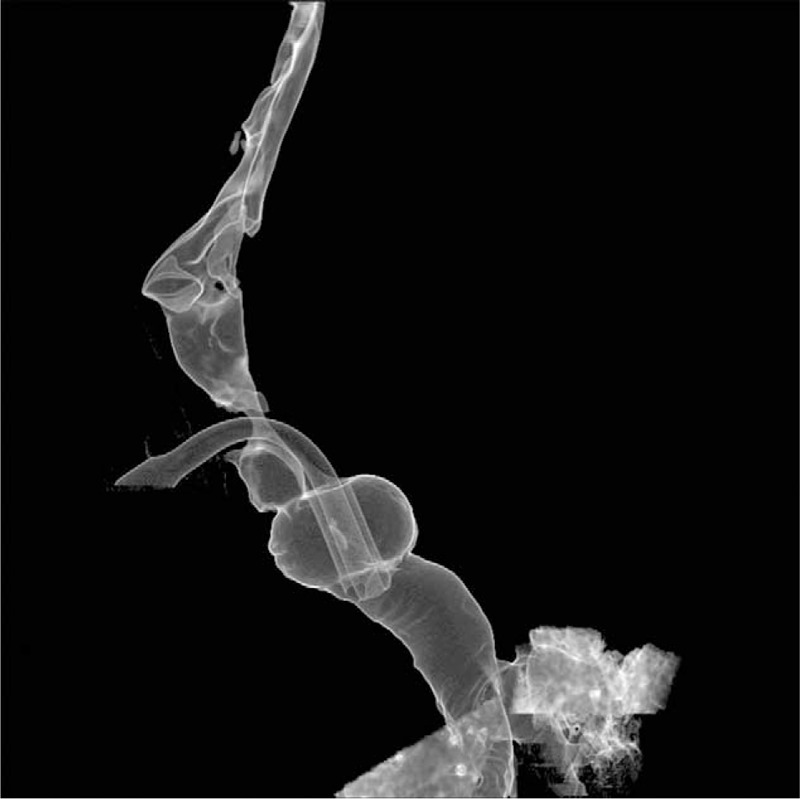
Three-dimensional computed tomography scan demonstrates that the shape and diameter of tracheal dilatation are exactly similar to those of tracheotomy tube cuff.
After the CT scan, tracheomegaly was considered to be secondary to the tracheotomy tube cuff. Considering the patient's clinical status, we performed conservative treatment instead of surgical correction. We used the adjustable tracheotomy tube, which can pass above the level of tracheomegaly. After using the adjustable tracheotomy tube, air leakage around the tracheotomy tube or rupture of tracheotomy tube cuff did not occur. In addition, serial chest radiograph revealed gradual reduction of the initial tracheomegaly (Fig. 3).
FIGURE 3.

Anteroposterior radiograph of the chest shows decrease in tracheomegaly after using the adjustable tracheotomy tube (arrows).
This study was approved by the Institutional Review Board of the Chonnam National University Hwasun Hospital. Informed consent was given by the patient.
DISCUSSION
Amyotrophic lateral sclerosis, also known as Lou Gehrig disease, is a specific disorder that is characterized by stiff muscles, muscle twitching, and gradual loss of muscle power. Besides a general lack of mobility, the affected individuals have difficulty in speaking, swallowing, and breathing. Recently, home tracheotomy mechanical ventilators have become the device of choice for patients with advanced ALS as their use can prolong survival, reduce hospitalization, and improve quality of life.4 In this case, the patient had used the home tracheotomy mechanical ventilator.
The pathogenesis of tracheomegaly in ALS remains speculative. Tracheomegaly in ALS may result from pressure necrosis, impairment of blood supply, infection, and injury to tracheal mucosa because of mechanical ventilation and prolonged intubation.1,3 The unique finding of this report is that the diameter of trachea progressively increased on serial CT scans after tracheotomy. This result suggested that tracheomegaly might have occurred because of mechanical ventilation or pressure from the tracheotomy tube. Our three-dimensional CT scans demonstrated a size and shape match between the dimensions of tracheomegaly and the tracheotomy tube cuff. Therefore, in this case, the primary cause of tracheomegaly was believed to be the tracheotomy tube cuff.
Tracheomegaly is diagnosed when the transverse diameter of the trachea exceeds 25 mm and 21 mm in men and women, respectively.2,3 In this report, the maximum transverse diameter was measured to be 43 mm on CT scan.
The management of tracheomegaly is difficult and still debated.5 A variety of surgical treatments have been suggested, but these are multistaged surgical procedures and each procedure carries serious risks. Because this patient had advanced ALS, we performed conservative treatment instead of opting for surgery. We tried to use the adjustable tracheotomy tube accommodating the enlarged trachea and thus maintaining the use of the home tracheotomy mechanical ventilator in addition to protecting the trachea.5
In conclusion, tracheomegaly has not been reported in an ALS case and this is the first report of tracheomegaly associated with tracheotomy tube cuff and a home tracheotomy mechanical ventilator. When a patient with ALS develops repeat air leakage around the tracheotomy tube or rupture of tracheotomy tube cuff, the clinician should consider the possibility of tracheomegaly in the differential diagnosis.
Footnotes
Abbreviations: ALS = amyotrophic lateral sclerosis, CT = computed tomography.
Tracheomegaly has not been reported in amyotrophic lateral sclerosis.
This is the first report of tracheomegaly associated with tracheotomy tube cuff and a home tracheotomy mechanical ventilator.
The authors declare no conflict of interest.
REFERENCES
- 1.Woodring JH, Barrett PA, Rehm SR, et al. Acquired tracheomegaly in adults as a complication of diffuse pulmonary fibrosis. AJR Am J Roentgenol 1989; 152:743–747. [DOI] [PubMed] [Google Scholar]
- 2.Celenk C, Celenk P, Selcuk MB, et al. Tracheomegaly in association with rheumatoid arthritis. Eur Radiol 2000; 10:1792–1794. [DOI] [PubMed] [Google Scholar]
- 3.Kim MY, Kim EJ, Min BW, et al. Anesthetic experience of a patient with tracheomegaly: a case report. Korean J Anesthesiol 2010; 58:197–201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sancho J, Servera E, Diaz JL, et al. Home tracheotomy mechanical ventilation in patients with amyotrophic lateral sclerosis: causes, complications and 1-year survival. Thorax 2011; 66:948–952. [DOI] [PubMed] [Google Scholar]
- 5.Giudice M, Gallo S, Maffioli MP, et al. Acquired tracheal dilatation after prolonged ventilation: an unusual treatment option. Laryngoscope 2014; 124:2309–2312. [DOI] [PubMed] [Google Scholar]