

Abstract
Objectives:
To review and analyze the pattern of breast cancer (BC) in the Kingdom of Saudi Arabia (KSA).
Methods:
A retrospective descriptive epidemiological review of BC of all diagnosed Saudi female cases from January 1990 to December 2014 was conducted at the Faculty of Sciences, Department of Biology, University of Tabuk, Tabuk, KSA. This report contains information obtained from the Saudi Cancer Registry and from King Faisal Specialist Hospital and Research Center.
Results:
The number of women with BC increased steadily from 1990-2010. On the basis of the number of cases, the percentage distribution of BC appears to be increasing. There were 1152 female BC cases in 2008 in comparison with 1308 in 2009, and 1473 in 2010. Breast cancer ranked first among females accounting for 27.4% of all newly diagnosed female cancers (5378) in the year 2010. The average age at the diagnosis of BC was 48; weighted average was 49.8, and range 43-52.
Conclusion:
Among Saudi patients, there was a significant increase in the number of cases of BC, which occurs at an earlier age than in Western countries. Continued vigilance, mammographic screening, and patient education are needed to establish early diagnosis and perform optimal treatment.
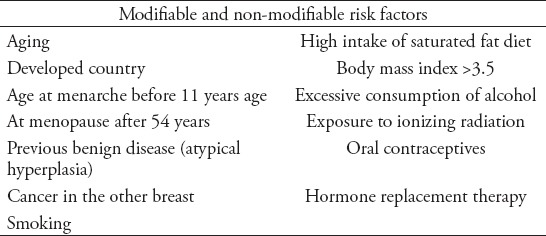
Breast cancer (BC) has a major impact on health of women worldwide and the Kingdom of Saudi Arabia (KSA) is no exception. It is considered the most common malignancy and embodies the second leading cause of cancer deaths after lung cancer. The malignancy carries tremendous socio-economic, emotional, and public health implications. It is estimated that more than one million new cases of BC are diagnosed annually. Breast cancer incidence rates in Arab women have increased during the last 24 years, but women are still being diagnosed with BC at more advanced stages of the disease.1-4 Morbidity and mortality have been shown to be effectively reduced by early detection of BC through screening activities.5-7 Despite this finding, low participation rates in BC screening activities have been reported among Arab women.6,8-10 Breast cancer is reported from developed nations and Western countries, while data on relevant reports from KSA appears either scattered, or not brought to the limelight.11 Regarding risk factors, women with a family history of BC should obtain as much information as possible on those relatives, including age at onset, and type of cancer. The risk of BC development related to family history increases with the number of affected relatives, specific lineage, and age at the time of diagnosis. The younger the age at diagnosis, the more likely that a genetic component may be involved, approximately 5-10% of BC is thought to be linked to changes (mutations) in certain genes. The most common are those of the BRCA 1 and BRCA 2 genes. Women with mutations in BRCA 1 or BRCA 2 have a high risk of developing BC, ovarian cancer, and several other types of cancer during their lifetimes. However, most cases of BC occur “by chance”. The causes are still unknown, but there is probably a combination of factors including lifestyle factors, environmental factors and hormone factors. Several risk factors are involved for BCs are shown in Table 1.12-17 Usually early BC does not cause pain. When the cancer grows, it causes changes in the size or shape of the breast: a lump or thickening may be noticeable. In advanced cases the tumor can show signs of ulceration of the skin, and fixation to the chest wall, and in the worst cases large lymph nodes may be present.18,19 If any of these symptoms appears, a proper investigation should be initiated. The “triple diagnosis” includes clinical examination, mammography, and/or the third component - presumably ultrasound is an additional tool to further define abnormalities detected on mammography. Several studies have reported that mammographic screening reduces BC mortality by 23%.20 Digital mammography employs detection software that can highlight suspicious lesions in the breast not initially seen by a radiologist. Magnetic resonance imaging (MRI) is recommended as a screening tool for women who have a 20-25%, or greater increased lifetime risk of BC. That includes women with a strong family history of BC, and women who are survivors of a previous malignancy that was treated with chest radiation therapy.21 Magnetic resonance imaging is not routinely indicated for women with a personal history of BC, despite a 5-10% increase in risk of a second primary cancer in the first 10 years after diagnosis, as the use of adjuvant chemotherapy and/or hormonal therapy significantly decreases overall risk to less than 5%.22 In our study, an integrative literature scrutiny was undertaken in order to do a retrospective epidemiological study from all BC reports from female patients available up to the present.
Table 1.
Possible associated factors increasing risks for breast cancer.
Methods
A retrospective descriptive epidemiological review of BC of all diagnosed Saudi female cases from January 1990 to December 2014 was conducted at the Faculty of Sciences, Department of Biology, University of Tabuk, Tabuk, KSA. This part of the report contains information from the Saudi Cancer Registry (SCR) (www.chs.gov.sa) and from King Faisal Specialist Hospital and Research Center (www.kfshrc.edu.sa) last accessed on August 2015. The data regarding cancer in KSA are publicly available and easily accessible. The latest report of the SCR was published in 2010, and no additional reports were published until the present. From 2010 onwards we tried to go through the literature (PubMed, Google) and reports (cancer registries) available on the pattern of cancer in KSA. Therefore, a retrospective review of all BC reports from female patients from 1990 up to the present in KSA was carried out. The study was conducted using these reports to critically gather all information from reliable sources with the aim of presenting the descriptive epidemiology of female BC in KSA.
Statistical analysis
The descriptive analysis of the epidemiological data was performed by calculating the overall percentages. All statistical analyses were performed using SigmaPlot, Systat Software program version 11 (SPSS Inc., Chicago, IL, USA).
Results
In 1990, the distribution of BC cases was 34.8% at the 30-49 years age group in comparison with 21.5% in the years 1994-2000 (Table 2). A total of 6,922 female BC cases were diagnosed and recorded in the SCR between January 2001 and December 2008. The number of women with BC increased steadily from 2001-2006. On the basis of the number of cases of BC and their percentages, the case appears to be increasing (Figures 1A & 1B). It can be seen that there were 545 cases in 2001 and the number rose to 614 by 2002; representing an increase of 1.2%. By 2007, there were 1,239 cases reported, corresponding to a 6.1% increase; this was the highest figure reported by the SCR. Interestingly, the figure dropped to 1,169 cases in 2008, representing a decline of 1%. The distribution of female BC cases by age groups from 2001-2008 was calculated by the SCR. The overall number of cases and percentages shows the age groups most and least affected by BC in KSA during the years 2001-2008 (Figure 1C & D). The groups reported correspond to ages 15-29, 30-44, 45-59, 60-74, and older than 75 years. There were 1152 female BC cases for year 2008. Breast cancer ranked first among females accounting for 25% of all newly diagnosed female cancers (4,617) in year 2008. The age-standardized incidence rate (ASR) was 19.2/100,000 for female population. The median age at diagnosis was 47 years. In the year 2009 there were 1,308 female BC cases accounting for 25.1% of all newly diagnosed female cancers (5,205) in this year. The median age at diagnosis was 48 years. There were 1,473 female BC cases for year 2010. Breast cancer ranked first among females accounting for 27.4% of all newly diagnosed female cancers (5,378) in year 2010. The ASR was 22.7/100,000 in 2009 compared with 24.9/100,000 in 2010 representing a small increase in 2010. The percentage distributions of BC was 40.2 in 2008, 38.7 in 2009, and 41.2 in 2010, with a small difference of 33.5, 33.9, and 36.1 at the age group 45-59. The average age at the diagnosis of BC was 48; weighted average was 49.8, and range 43-52 (Figures 1C & 1D).
Table 2.
Percentage increase of breast cancer (BC) in Kingdom of Saudi Arabia.
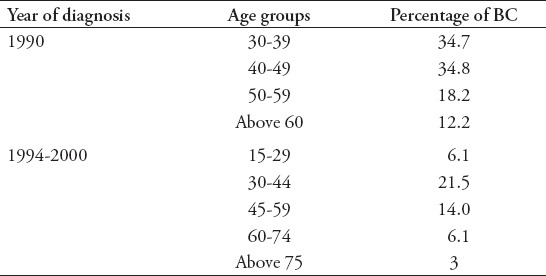
Figure 1.
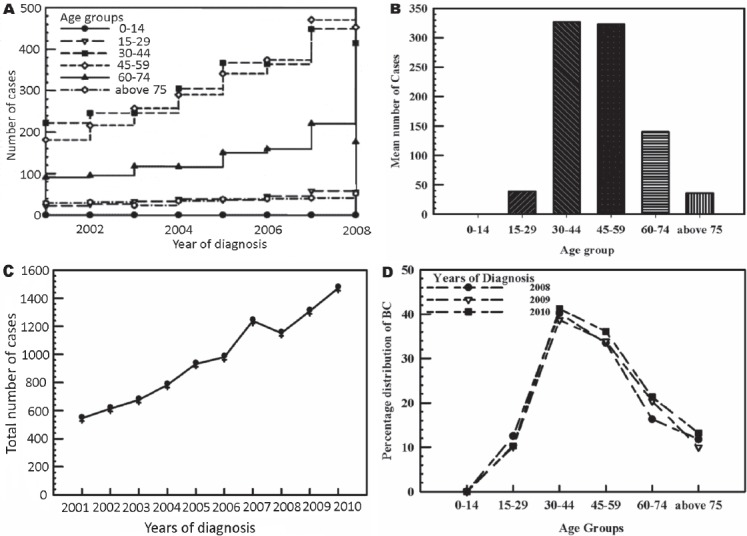
An illustration of the distribution in number of breast cancer (BC) cases in the Kingdom of Saudi Arabia by: A) different age groups from the year 2001-2008; B) the overall mean number; C) total number from 2001-2010; and D) percentage distribution by age group from 2008-2010.
Discussion
The descriptive epidemiology of BC in KSA provides a significant elucidation of the recent trend, confirming the significance of the disease among women. The results of our study were based on the data recorded in the SCR and available in the literature, showing that female BC is one of the most significant causes of disease among women.23,24 The age group most affected by BC in KSA and other developing countries is women younger than 50 years of age.25 However, developed countries have higher BC incidence rates among women aged 50 years and older.
This review on BC in Saudi Arab shows that the percentage increase on BC is highest by the year 2010. It is clear from the epidemiological analysis of the reports registered by the SCR and in the literature that the crude incidence rate and age-standardized incidence rate in female BC incidence are increasing annually. There were 1,152 female BC cases for year 2008, in comparison with 1,308 for year 2009, and 1,473 for year 2010. Breast cancer ranked first among females accounting for 27.4% of all newly diagnosed female cancers (5,378) in year 2010. The ASR was 22.7/100,000 in 2009 compared with 24.9/100,000 in 2010 representing a small increase in 2010. In KSA, the International Agency for Research on Cancer estimated that the age-standardized incidence rate for BC was 22.4 per 100,000 women in 2008, and the age-standardized mortality rate was 10.4 per 100,000 women.24 Furthermore, in 2011, the registry of King Faisal Specialist Hospital and Research Centre reported that the number of BC cases has increased considerably.
In conclusion, it is recommended that intensive health education should be launched immediately. This will involve Saudi Arab females who tend to marry at a young age, according to the traditional conservative values of the society, with childbearing extending practically over the entire reproductive period of life. Due to the conservative nature of the society, most women will refrain from seeking medical advice out of shyness until their disease becomes far-advanced, particularly in breast cancer cases. Therefore, proper education and training should be launched involving, utilization of the different media, social network, as well as person-to-person and house-to-house education. Further analytical epidemiological research is needed to identify the potential risk factors that have contributed to the increase in the occurrence of BC among Saudi women.
Footnotes
Related Articles.
Awan BA, Samargandi OA, Alghamdi HA, Sayegh AA, Hakeem YJ, Merdad L, et al. The desire to utilize postmastectomy breast reconstruction in Saudi Arabian women. Predictors and barriers. Saudi Med J 2015; 36: 304-309.
Albasri A, Hussainy AS, Sundkji I, Alhujaily A. Histopathological features of breast cancer in Al-Madinah region of Saudi Arabia. Saudi Med J 2014; 35: 1489-1493.
Al-Shaikh GK, Almussaed EM, Fayed AA, Khan FH, Syed SB, Al-Tamimi TN, et al. Knowledge of Saudi female university students regarding cervical cancer and acceptance of the human papilloma virus vaccine. Saudi Med J 2014; 35: 1223-1230.
Baghlaf SS, Abulaban AA, Abrar MB, Al-Shehri AS. Chemotherapy-induced febrile neutropenia in patients with breast cancer. A multivariate risk assessment model for first cycle chemotherapy. Saudi Med J 2014; 35: 612-616.
References
- 1.Brown R, Kerr K, Haoudi A, Darzi A. Tackling cancer burden in the Middle East: Qatar as an example. Lancet Oncol. 2012;13:e501–e508. doi: 10.1016/S1470-2045(12)70461-8. [DOI] [PubMed] [Google Scholar]
- 2.Othman A, Ahram M, Al-Tarawneh MR, Shahrouri M. Knowledge, attitudes and practices of breast cancer screening among women in Jordan. Health Care Women Int. 2015;36:578–592. doi: 10.1080/07399332.2014.926900. [DOI] [PubMed] [Google Scholar]
- 3.Al-Saad S, Al-Shinnawi H, Mahmood Shamsi N. Risk Factors of Breast Cancer in Bahrain. Bahrain Medical Bulletin. 2009;31:1–11. [Google Scholar]
- 4.Miller AB. Screening for breast cancer in the Eastern Mediterranean Region. East Mediterr Health J. 2010;16:1022–1024. [PubMed] [Google Scholar]
- 5.Baron-Epel O, Friedman N, Lernau O. Reducing disparities in mammography-use in a multicultural population in Israel. Int J Equity Health. 2009;8:19. doi: 10.1186/1475-9276-8-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bener A, El Ayoubi HR, Moore MA, Basha B, Joseph S, Chouchane L. Do we need to maximise the breast cancer screening awareness? Experience with an endogamous society with high fertility. Asian Pac J Cancer Prev. 2009;10:599–604. [PubMed] [Google Scholar]
- 7.Cohen M, Azaiza F. Increasing breast examinations among arab women using a tailored culture-based intervention. Behav Med. 2010;36:92–99. doi: 10.1080/08964280903521313. [DOI] [PubMed] [Google Scholar]
- 8.Keten HS, Yıldırım F, Ölmez S, Üçer H, Çelik M. Knowledge, attitudes and behavior about breast cancer in women presenting to Early Cancer Diagnosis, Screening and Education Centre in Kahramanmaraş, Turkey. Gaziantep Medical Journal. 2014;20:212–216. [Google Scholar]
- 9.Kawar LN. Jordanian and Palestinian immigrant women’s knowledge, affect, cultural attitudes, health habits, and participation in breast cancer screening. Health Care Women Int. 2009;30:768–782. doi: 10.1080/07399330903066111. [DOI] [PubMed] [Google Scholar]
- 10.Azaiza F, Cohen M, Awad M, Daoud F. Factors associated with low screening for breast cancer in the Palestinian Authority: relations of availability, environmental barriers, and cancer-related fatalism. Cancer. 2010;116:4646–4655. doi: 10.1002/cncr.25378. [DOI] [PubMed] [Google Scholar]
- 11.Yousuf SA. Breast Cancer Awareness among Saudi Nursing Students. Journal of King Abdulaziz University Medical Sciences. 2010;17:67–78. [Google Scholar]
- 12.Brandt J, Garne JP, Tengrup I, Manjer J. Age at diagnosis in relation to survival following breast cancer: a cohort study. World J Surg Oncol. 2015;13:33. doi: 10.1186/s12957-014-0429-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Arce-Salinas C, Aguilar-Ponce JL, Villarreal-Garza C, Lara-Medina FU, Olvera-Caraza D, Alvarado Miranda A, et al. Overweight and obesity as poor prognostic factors in locally advanced breast cancer patients. Breast Cancer Res Treat. 2014;146:183–188. doi: 10.1007/s10549-014-2977-8. [DOI] [PubMed] [Google Scholar]
- 14.Papageorgiou EI, Jayashree Subramanian, Karmegam A, Papandrianos N. A risk management model for familial breast cancer: A new application using Fuzzy Cognitive Map method. Comput Methods Programs Biomed. 2015 doi: 10.1016/j.cmpb.2015.07.003. pii: S0169-2607(15)00180-7. [DOI] [PubMed] [Google Scholar]
- 15.Alvarez K. Oral Contraceptive Androgenicity and Cognitive Performance Among Women (Doctoral dissertation, Drexel University) Available from: https://idea.library.drexel.edu/islandora/object/idea%3A4454/datastream/OBJ/download/Oral_Contraceptive_Androgenicity_and_Cognitive_Performance_Among_Women.pdf .
- 16.Kiely D, Schwartz S. Assessing breast cancer risk in a primary care setting. The Nurse Practitioner. 2014;39:49–53. doi: 10.1097/01.NPR.0000453643.59404.ad. [DOI] [PubMed] [Google Scholar]
- 17.Uday CK, Devarayalu BVSK, Mahmood S. Overall survival rate in breast cancer patients treated with 5-fluorouracil: a review of randomized clinical trials. Int J Pharmaceut Biomed Res. 2010;1:132–135. [Google Scholar]
- 18.Waters EA, McNeel TS, Stevens WM, Freedman AN. Use of tamoxifen and raloxifene for breast cancer chemoprevention in 2010. Breast Cancer Res Treat. 2012;134:875–880. doi: 10.1007/s10549-012-2089-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Schroyen S, Adam S, Jerusalem G, Missotten P. Ageism and its clinical impact in oncogeriatry: state of knowledge and therapeutic leads. Clin Interv Aging. 2014;10:117–125. doi: 10.2147/CIA.S70942. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Wang AT, Vachon CM, Brandt KR, Ghosh K. Breast Density and Breast Cancer Risk: A Practical Review. Mayo Clinic Proceedings. 2014;89:548–557. doi: 10.1016/j.mayocp.2013.12.014. [DOI] [PubMed] [Google Scholar]
- 21.Postma EL, van Hillegersberg R, Daniel BL, Merckel LG, Verkooijen HM, van den Bosch MA. MRI-guided ablation of breast cancer: where do we stand today? J Magn Reson Imaging. 2011;34:254–261. doi: 10.1002/jmri.22599. [DOI] [PubMed] [Google Scholar]
- 22.Geijer M, Domanski HA. Image-Guided Fine-Needle Aspiration Cytology. In: Domanski HA, editor. Atlas of Fine Needle Aspiration Cytology. 2014 ed. London (UK): Springer; 2014. pp. 35–46. [Google Scholar]
- 23.Sung H, Rosenberg PS, Chen WQ, Hartman M, Lim WY, Chia KS, et al. Female breast cancer incidence among Asian and Western populations: more similar than expected. J Natl Cancer Inst. 2015;107 doi: 10.1093/jnci/djv107. pii: djv107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Alghamdi IG, Hussain II, Alghamdi MS, El-Sheemy MA. The incidence rate of female breast cancer in Saudi Arabia: an observational descriptive epidemiological analysis of data from Saudi Cancer Registry 2001-2008. Breast Cancer (Dove Med Press) 2013;5:103–109. doi: 10.2147/BCTT.S50750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Molah Karim SA, Ali Ghalib HH, Mohammed SA, Fattah FH. The incidence, age at diagnosis of breast cancer in the Iraqi Kurdish population and comparison to some other countries of Middle-East and West. Int J Surg. 2015;13:71–75. doi: 10.1016/j.ijsu.2014.11.029. [DOI] [PubMed] [Google Scholar]