

Abstract
Background: Metastatic spread is the most common cause of cancer-related death in colorectal cancer (CRC) patients, with the liver being the mostly affected organ. Circulating tumor cells (CTCs) are a prognostic marker in stage IV CRC. We hypothesized that tumor burden in the liver correlates with CTC quantity. Methods: Blood (7.5 ml) was prospectively collected from 24 patients with novel stage IV CRC diagnosis. Baseline EpCAM+ CTCs were analyzed with the FDA-approved CellSearch® system. Clinicopathological data were collected, and hepatic tumor burden was determined by radiographic liver volumetry with contrast-enhanced CT scans. CRC primary tumors were immunohistochemically stained for EpCAM expression with BerEP4 monoclonal antibody. Statistical analyses were performed using 2-sample T-test, non-parametric Wilcoxon Rank-Sum test, and Fisher's exact test. Results: CTCs were detected n 17 (71%) of 24 patients. The overall mean CTC number as determined by EpCAM-based CellSearch® detection was 6.3 (SEM 2.9). High baseline CTC numbers (≥3) correlated significantly with a high tumor/liver ratio (≥30%), and with high serum CEA levels, as determined by two-sample T-test on log-transformed data and by Fisher's Exact test on categorical data analysis (P < 0.05). The CRC primary tumors were consistently expressing EpCAM by immunostaining. Conclusions: High tumor burden in the liver and high baseline serum CEA levels are associated with high number of baseline CTCs in stage IV CRC patients. Future studies should further investigate the biological role and expression patterns of single CTCs in cancer patients to further improve personalized treatment strategies.
Keywords: Colorectal cancer, circulating tumor cells, liver metastasis, stage IV, tumor burden, liver volumetry
Abbreviations
- CTCsc
circulating tumor cells
- EpCAM
epithelial cell adhesion Molecule
- CRC
colorectal cancer
Introduction
Colorectal cancer (CRC) is the second leading cause of cancer mortality occurring in both genders in the United States.1 90% of CRC-related deaths are caused by metastatic spread, primarily to the liver.1,2 Approximately 50% of CRC patients will be diagnosed with liver metastases, either at the time of initial presentation or as part of recurrent disease.
The initial description of circulating tumor cells (CTCs) goes back to the 19th century, and since then a number of techniques have been developed for the isolation of CTCs in peripheral blood, including reverse transcriptase polymerase chain reaction (rt-PCR), immunocytochemistry, flow cytometry, microchips, and size-based filtration methods.3-8 In 2004, the Food and Drug Administration (FDA) approved the CTC detection in metastatic colorectal, prostate, and breast cancers with CellSearch® system by Veridex that utilizes several molecular parameters to isolate CTCs: immunomagnetic enrichment for epithelial cell adhesion molecule (EpCAM), nuclear staining with 4′,6-diamidino-2-phenylindole (DAPI), and immunofluorescence detection of cytokeratins and CD45.9 In general, CTCs can be considered a non-invasive ‘liquid biopsy’ of the cancer, and detection and characterization of CTCs has potential high-impact implications for prognostication and therapy. However, CTCs are rare (approximately 1 CTC per 105–107 mononuclear cells) and probably only few CTCs have the potential to develop to a solid metastasis.10,11 Several studies have shown that stage IV CRC with ≥3 CTCs have significantly worse survival.12-14 In addition, a strong correlation between detection of CTCs and radiographic disease progression in patients receiving chemotherapy for CRC has been demonstrated.15
We hypothesized that the quantity of baseline CTCs is associated with the tumor burden in the liver in patients with a novel stage IV CRC diagnosis. The study demonstrates that CTC quantity correlates with high tumor burden in the liver and elevated serum CEA levels in stage IV CRC patients.
Results
Patients' clinical characteristics, baseline CTC numbers and liver/tumor volume ratio
In a multidisciplinary CRC clinic at a tertiary care center, 24 CRC patients with newly diagnosed stage IV disease were prospectively analyzed for EpCAM+ CTCs in 7.5 ml of blood with the CellSearch® method. As listed in Table 1, 8 (33%) patients were female and 16 (67%) patients were male. The median age was 64 (range: 42–88) years. The primary factor being investigated was the baseline CTC number. Overall 17 (71%) of 24 patients had CTCs in the peripheral blood (mean 6.3 (SEM 2.9). As previously described to be of prognostic significance for stage IV CRC, CTCs were dichotomized into low/high levels: low: 0–2 CTCs/7.5ml, high: ≥3 CTCs/7.5ml blood. Seven (29%) of 24 patients had high baseline CTC levels. Mean serum CEA level was 370.9 (SEM 221.0). In an attempt to quantify cancer burden in the liver, the tumor and healthy liver volume was determined by standard liver volumetry, as described in the method section. For those patients who had liver metastases (15 (63%) out of 24), 11 patients had adequate imaging with venous phase contrast-enhanced CT images, allowing for liver volumetric analysis. Four patients (#1, #22–24) did not have a baseline contrast-enhanced CT scan, and hence volumetric analysis of the liver was not performed. These patients did have metastatic disease demonstrated on PET or non-contrast enhanced PET/CT scan). Although these patients did have significant liver metastases, liver volumetry was technically not possible due to lack of contrast in the images. The tumor/liver volume ratio was dichotomized to low (<30%) and high (≥30%). Three of 11 patients (27%) had a high liver tumor/volume ratio.
Table 1.
Patients' characteristics of stage IV CRC patients that were analyzed for presence of baseline CTCs
| Total number of patients | 24 | |
|---|---|---|
| Age | • Mean (SEM) | 63.6 (2.5) |
| • Median (range) | 64 (42–88) | |
| Gender | • Females | 8 (33%) |
| • Males | 16 (67%) | |
| Location of primary tumor | • Rectosigmoid | 16 (67%) |
| • Descending colon | 2 (8%) | |
| • Transverse colon | 1 (4%) | |
| • Right colon/cecum/others | 5 (21%) | |
| Tumor invasion depth of primary tumor (data available in 14/24 patients) | • pT1 | 0 |
| • pT2 | 1 (7%) | |
| • pT3 | 5 (36%) | |
| • pT4 | 8 (57%) | |
| Nodal status of primary tumor (data available in 13/24 patients) | • pN0 | 1 (8%) |
| • pN1 | 1 (8%) | |
| • pN2 | 11 (84) | |
| Lymphatic invasion (data available in 12/24 patients) | • Absent | 3 (25%) |
| • Present | 9 (75%) | |
| Venous invasion (data available in 11/24 patients) | • Absent | 4 (36%) |
| • Present | 7 (64%) | |
| Perineural invasion (data available in 11/24 patients) | • Absent | 6 (55%) |
| • Present | 5 (45%) | |
| Histological differentiation (data available in 21/24 patients) | • Moderate | 15 (72%) |
| • Poor | 3 (14%) | |
| • Undifferentiated | 3 (14%) | |
| Histology of adenocarcinomas (AC) | • AC | 19 (79%) |
| • AC with signet cell features | 2 (8%) | |
| • AC with mucinous features | 3 (13%) | |
| Serum CEA level (ng/ml; normal <5) | • Mean (SEM) | 370.9 (221.0) |
| • Median (range) | 8.0 (1.4–4967.7) | |
| KRAS mutation (codon 12 or 13) | 1/20 (5%) | |
| BRAF mutation (codon 600) | 3/19 (16%) | |
| High EGFR expression | 12/15 (80%) | |
| High ERCC1 expression | 1/14 (7%) | |
| High TS expression | 6/14 (43%) | |
| Circulating tumor cells (CTCs) | • Detectable | 17/24 (71%) |
| • Mean (SEM) | 6.3 (2.9) | |
| • Median (Range) | 1 (0–56.3) | |
| • Low baseline: | ||
| • 0 | 7/24 (29%) | |
| • 1–2 | 10 (42%) | |
| • High baseline: | ||
| • ≥3 | 7 (29%) | |
| Liver metastases present | 15/24 (63%) | |
| Tumor/liver volume ratio (data available in 11/15 patients) | • Low (<30%) | 8/11 (73%) |
| • High (≥30%) | 3/11 (27%) |
Table 1 provides other clinical and pathological parameters, such as features of the primary CRC (location, tumor invasion depth (pT), nodal status (pN), presence of lymphatic/venous/perineural invasion, histological differentiation), KRAS and BRAF mutational status, and EGFR, ERCC1 and TS expression. Table 2 lists further study details of the 24 stage IV CRC on an individual basis, including sites of metastases, mean CTC numbers and categories (low/high), total liver volumes and tumor volumes in including the tumor/liver volume ratio and categories (low/high).
Table 2.
List of the individual patients with CTC counts and tumor/liver volume ratio
| Patient # | Sites of Metastases | CEA serum level (normal range: 0–5ng/ml) | Mean CTC (±SEM) per 7.5cc blood | CTCs low (0–2) or high (≥3) | Tumor/liver volume ratio: low (<30%) or high (≥30%) | Tumor/liver volume ratio (%) | Total liver volume (cc) | Tumor volume (cc) |
|---|---|---|---|---|---|---|---|---|
| 1 | Lymph nodes (retroperitoneal, abdominal, supraclavicular) | 3.7 | 3 (±0.6) | high | — | — | — | — |
| 2 | Lymph nodes (abdominal) | 1.6 | 0.67 (±0.3) | low | — | — | — | — |
| 3 | Liver, lymph nodes, omentum, bone | 4.3 | 0.5 (±0.5) | low | low | 0.3 | 1704 | 5 |
| 4 | Liver, lymph nodes (retroperitoneal) | 31.9 | 2.3 (±0.3) | low | low | 0.2 | 1704 | 4 |
| 5 | Bone | 18.3 | 1 (±0.6) | low | ||||
| 6 | Liver | 4.7 | 0 | low | low | 0.8 | 1381 | 11 |
| 7 | Liver, lung | 4967.7 | 56.3 (±7.1) | high | high | 54.3 | 3182 | 1729 |
| 8 | Liver, lung, lymph nodes (mesenteric, mediastinal) | 1.6 | 1 (±1) | low | low | 5.1 | 2856 | 145 |
| 9 | Liver | 2246 | 42.7 (±3.0) | high | high | 43.7 | 2831 | 1238 |
| 10 | Liver | 275.5 | 11.5 (±1.5) | high | low | 2.8 | 1386 | 39 |
| 11 | Liver, adrenal gland | 7.9 | 0.5 (±0.5) | low | low | 0.7 | 1682 | 12 |
| 12 | Lung, lymph nodes (mediastinal, mesenteric, periaortic) | 2.3 | 1 (0) | low | — | — | — | — |
| 13 | Lung | 61.5 | 0 | low | — | — | — | — |
| 14 | Lymph nodes (mediastinal) | 3.4 | 0.3 (±0.3) | low | — | — | — | — |
| 15 | Lymph nodes (mediastinal) | 93.6 | 0 | low | — | — | — | — |
| 16 | Liver, lung, brain | 7.2 | 4.5 (±0.5) | high | high | 72.1 | 2808 | 2024 |
| 17 | Liver | 1.4 | 0 | low | — | — | — | — |
| 18 | Liver, lung | 2.7 | 1 (±1.0) | low | low | 4.5 | 1346 | 61 |
| 19 | Lung, lymph nodes | 3.5 | 0 | low | — | — | — | — |
| 20 | Liver, lymph nodes, adrenal glands | 137.9 | 0 | low | low | 1.5 | 1123 | 17 |
| 21 | Lymph nodes (retroperitoneal, abdominal, supraclavicular) | 8.0 | 0 | low | — | — | — | — |
| 22 | Liver, lymph nodes (abdominal) | 86.2 | 2 | low | — | — | — | — |
| 23 | Liver, lymph nodes, omentum, bone | 492.4 | 7 (±2.0) | high | — | — | — | — |
| 24 | Liver, lymph nodes (retroperitoneal) | 438.2 | 16 | high | — | — | — | — |
Baseline CTC numbers levels correlate with the tumor burden in the liver
To statistically analyze the association between CTC numbers and tumor burden in the liver, a log-transformed tumor/liver volume ratio was calculated to assure the validity of statistical assumptions (Fig. 1). The relationships between categorized low (0–2) and high (≥3) baseline CTC values and the log-transformed tumor/liver volume ratio were examined (Fig. 1). Statistical analysis revealed a significant association between the log-transformed tumor/liver volume ratio and CTC baseline levels by both parametric (P = 0.0036 (2-sample T-test)) and non-parametric (P = 0.0298 (Wilcoxon Rank-Sum test) analysis).
Figure 1.
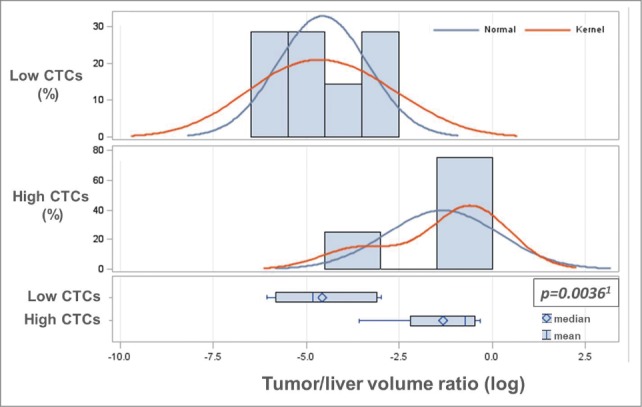
Baseline CTC levels correlate with tumor burden in the liver. To statistically analyze the association between CTC numbers and tumor burden in the liver, baseline CTCs were categorized into low (0–2) and high (≥3), and the tumor/liver volume ratio was log-transformed to assure the validity of statistical assumptions. A significant association between the log-transformed tumor/liver volume ratio and baseline low/high CTC levels by both parametric (1two-sample T-test (P = 0.0036)) and non-parametric (Wilcoxon Rank-Sum test) (P = 0.0298) analysis was determined. As shown in Table 3, the tumor/liver volume ratio was dichotomized into low (<30%) and high (≥30%) tumor/liver volume ratio, which was also found to be significantly associated with baseline CTC levels (high/low).
In addition, the tumor/liver volume ratio was dichotomized into low tumor/liver volume (<30%), and high (≥30%) tumor/liver volume ratio. There were 3 stage IV CRC patients categorized to have high tumor/liver volume ratio. The relationship between baseline CTC level categories (low/high) and tumor/liver volume ratio (low/high) was statistically significant as well (P = 0.0242 (Fisher's exact test)) (Table 3)
Table 3.
Correlation of categorized tumor/liver volume ratio and CEA serum level with baseline CTC numbers in stage IV CRC
| Total | Low CTC baseline (0–2) | High CTC baseline (≥3) | P value | |
|---|---|---|---|---|
| Tumor/liver volume ratio | ||||
| • Low (<30%) | 8/11 (73%) | 7 (100%) | 1 (25%) | 0.0242 |
| • High (≥30%) | 3/11 (27%) | 0 | 3 (75%) | |
| Serum CEA level (ng/ml) | ||||
| • <2.5 | 4 (17%) | 4 (24%) | 0 | 0.0019 |
| • 2.5–5 | 6 (25%) | 5 (28%) | 1 (14%) | |
| • 5–50 | 5 (21%) | 4 (24%) | 1 (14%) | |
| • 50–200 | 4 (17%) | 4 (24%) | 0 | |
| • >200 | 5 (21%) | 0 | 5 (72%) |
P values were calculated by Fisher's Exact test
Baseline CTC levels correlate with serum CEA levels
Similar to the tumor/liver volumetry analysis, the baseline serum CEA levels were log-transformed to stabilize the variance and make the associated statistical calculations more valid. A significant correlation between log-transformed serum CEA levels and CTC baseline counts (low/high) was determined by parametric (P = 0.0016 (2-sample T-test)) and non-parametric analysis (P = 0.0092 (Wilcoxon Rank-Sum test)) (Fig. 2). Baseline serum CEA levels were also categorized (<2 .5; 2.5–5; 5–50; 50–200; >200 ng/ml), and the correlation analysis with low/high baseline CTC levels was also statistically significant (P = 0.0019; Fisher's exact test) (Table 3).
Figure 2.
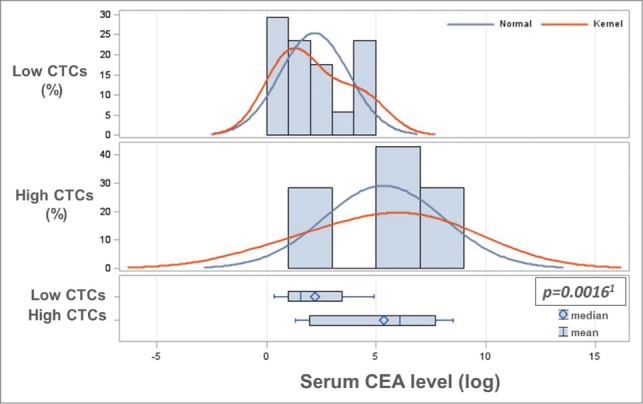
Baseline CTC levels correlate with serum CEA levels. Baseline serum CEA levels were log-transformed to stabilize the variance and make the associated statistical assumption more valid. A significant association between log-transformed serum CEA levels and categorized baseline CTC counts (low: 0–2, high: ≥3) was determined by parametric (1two-sample T-test (P = 0.0016)) and non-parametric analysis (Wilcoxon Rank-Sum test (P = 0.0092)). As shown in Table 3, baseline serum CEA levels were also categorized and the correlation analysis with low/high baseline CTC levels was also statistically significant.
Baseline serum CEA levels did not correlate with the tumor burden in the liver
The log-transformed value of tumor liver volume ratio and its relationship with serum CEA level was investigated. In general, patients with high baseline CEA level had a higher liver tumor burden. However, the relationship did not reach level of significance (p-value = 0.3571 (2-sample T-test)). The categorized liver tumor burden (high/low) was also correlated with serum CEA level. Patients with low liver tumor burden (4/8; 50%) had high baseline serum CEA level, and those 3 patients with high liver tumor burden had all high baseline serum CEA level. However, also this relationship was not statistically significant (P = 0.2364 (Fisher's exact test)).
Baseline CTC numbers did not correlate with other clinical and pathological parameters
We explored the bivariate relationship between baseline CTC numbers (low/high) versus various other clinical and pathological parameters that are listed in Table 1. Except the described significant correlation of baseline CTC levels with liver/tumor volume ratio and serum CEA level, no other of the relationships was statistically significant. No association was noted between CTC numbers (low/high) and gender distribution, presence of liver or lung metastases, primary CRC differentiation, tumor location, histology, tumor invasion depth (pT), nodal status (N), lymphatic/venous invasion/perineural invasion, mutational status (KRAS, BRAF), EGFR, ERCC1, or TS expression (P = N.S.).
EpCAM immunohistochemistry of primary CRC tumors
As the CellSearch® detection system is based on immunomagnetic bead selection of exclusively EpCAM+ CTCs, EpCAM immunostaining of the respective primary CRC tumors with a monoclonal antibody (BerEP4) was performed to confirm positivity. The primary CRC tumors were chosen for immunostaining because actual metastatic tissue was not available in most patients. CRC primary tumors of the stage IV patients analyzed for CTC by CellSearch® were shown to express EpCAM, demonstrating that its expression was not silenced. Figure 3 illustrates different examples of stage IV CRC patients with liver metastases with high or zero baseline CTCs that all had consistent and homogenous EpCAM expression in the primary tumor.
Figure 3.
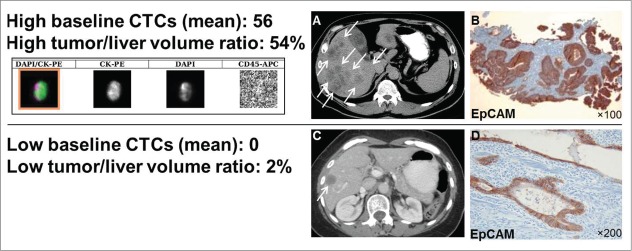
Computer tomography (CT), CTC images and EpCAM immunostaining of CRC tumors. EpCAM is consistently expressed in CRC primary tumors, also in patients that have no CTCs detectable by EpCAM-based CellSearch® system. Shown are: mean CTC numbers (±SEM), the actual liver/tumor volume ratio, a CTC (CellSearch® system qualifies a cell as a CTC if it has an evident nucleus by DAPI and if it is EpCAM+, cytokeratin 8/18/19+, and CD45-), (A) CT scan of a patient with a high tumor/liver ratio (≥30%) and high baseline CTCs (≥3), (B) EpCAM immunostaining with a monoclonal antibody (BerEP4) and peroxidase method of the respective CRC primary tumor, (C) CT scan of a patient with a low high tumor/liver ratio (<30%) zero baseline CTCs, and (D) EpCAM immunostaining of the respective CRC primary tumor.
Discussion
Nearly half of all CRC patients will be diagnosed with liver metastases, either at the time of initial presentation or as part of recurrent disease.1,2 The liver is by far the most frequent site of CRC spread, and can harbor significant amounts of cancer quantities as it is the largest internal organ. Complete surgical resection of oligometastatic disease that is limited to the liver can significantly improve survival and potentially cure patients.2,16 Recent advances in chemotherapy regimens with innovative agents, tumor ablation techniques and regional (intraarterial) chemotherapy administration provide for a variety of treatment options to improve outcome for patients diagnosed with stage IV CRC metastatic to the liver.17
CTCs are a strong prognostic marker in metastatic breast, prostate and CRC patients.18 In general, detection of CTCs provides a unique opportunity to achieve a ‘liquid biopsy’ for cancer testing, monitoring, and prognostication. In general stage IV CRC patients with diffuse spread that usually involves the liver have the highest number of CTCs, in contrast to patients with metastases limited to the liver or lungs.19 We hypothesized that CTCs could also correlate with the patient's actual tumor burden in the liver as the largest internal organ. Several studies have shown that stage IV CRC patients with ≥3 CTCs, as measured by CellSearch®, have a significantly worse survival, so that 3 CTCs are the accepted cutoff.12,13 Consequently, we chose the same cutoff for analysis for our stage IV CRC patient group.
The study showed that baseline CTC quantity correlates with tumor/liver volume ratio and serum CEA levels in stage IV CRC patients. Analysis revealed that CTC numbers and serum CEA levels might be a potential indicator for macroscopic cancer quantity that a patient carries. Data demonstrated that patients with high liver tumor burden do consistently have high CTC counts, although the overall sample size is low. Consequently, the statistical analysis of our study needs to be interpreted with caution. In contrast, few patients with a high baseline CTCs had low tumor burden in the liver. The authors assume that these patients have poor clinical outcome, which needs to be further investigated with a longitudinal follow-up study. We chose liver volumetry as a tool for measurement of tumor burden quantity as this is a standardized and clinically applied method to measure healthy and diseased liver. Liver volumetry has been developed for preoperative planning of hepatic resections.20 The liver often carries the highest burden in terms of tumor quantity in an individual patient. We chose a threshold of 30% tumor burden to be a potential predictor of presence of CTCs, however the significant liver tumor volume quantity leading to increased CTC shedding needs to be determined in future trials.
In our patient group, serum CEA levels correlated significantly with CTC numbers, although other investigators have found contradictory results.21,22 All our patients had a novel diagnosis of stage IV disease, and none of them had any treatments for metastatic CRC. We chose to include patients with true baseline CTC and serum CEA levels only, as it has been shown that any local or systemic treatment can impact CTCs and serum CEA levels. Moreover, persisting CTC numbers predict poor response and outcome in patients receiving systemic treatment.12 Another study provided evidence of a strong correlation between CTC detection and radiographic disease progression in patients receiving chemotherapy for CRC.15 In agreement with these findings, a recent meta-analysis demonstrated that the detection of CTCs in patients with resectable CRC liver metastases is associated with poor survival.23 Finally, serum CEA levels did not correlate with high tumor burden in the liver, however the statistical power to verify this relationship may not have enough strength. A larger sample size for definitive conclusions will be needed.
CTC isolation has potential relevance for future CRC staging and chemosensitivity testing. Findings on CTCs in patients with multiple and unresectable liver metastases could initiate clinical trials based on CTCs to improve local treatments, such as intraarterial drug application to the liver. Due to the CellSearch® system's limited capture efficiency to detect rare CTCs, future studies will need to evaluate innovative technologies, such as novel filtration-based CTC isolation techniques.5 These may have a higher CTC capture efficiency and allow isolation of viable cells for further chemosensitivity testing. By analyzing biomarker expression in CTCs and metastases, molecular changes required for metastases reformation and therapeutic molecular targets will be identified.
One limitation with CTC detection is that CTC numbers are low in the peripheral blood.10,11 CellSearch® is a technology that reliably captures CTCs and provides a semi-automated platform for enumerating CTCs based on multiple markers to yield high accuracy, recovery, and reproducibility. But the FDA-approved CellSearch® technology does not detect CTCs in many patients with widely metastatic disease, while few have exceedingly high CTC numbers in the peripheral blood.18 Intraoperative CTC isolation during surgery could be an exceptional opportunity to isolate higher numbers of CTCs in patients undergoing liver metastasectomy, due to surgical manipulation and direct access to tumor outflow blood. Pilot trials on few patients demonstrated that CTCs can be isolated more frequently in tumor outflow than in the peripheral blood during surgery of primary CRC.24,25 To further address this we initiated a clinical trial on intraoperative CTC isolation during CRC lung and liver metastasectomy, comparing the CellSearch® system with a size-based CTC isolation technique (ClinicalTrials.gov Identifier: NCT01722903) that demonstrated higher CTC capture efficiency intraoperatively with an innovative filter.31
Several studies have demonstrated the clinical significance of CTC numbers as a prognostic marker when enumerated by the CellSearch® system in metastatic tumors of breast, colon and prostate.12,26,27 However, CellSearch® is limited by the selection of EpCAM+ CTCs only. EpCAM downregulation has been described in the process of epithelial-mesenchymal transformation (EMT) of metastasizing cancer cells.28 A recent study has also shown that EpCAM- CTCs may have a crucial role in development of distant metastasis.29,30 In our study, CRC primary tumors of the stage IV CRC patients were consistently expressing EpCAM by immunohistochemistry. CRC patients with high volume liver metastasis had the highest number of CTCs detected by CellSearch®, but patients with low CTCs expressed EpCAM homogeneously in their respective CRC primary tumors. In the present patient group, the actual metastasis tissue was not available, and future studies should analyze EpCAM expression in metastases specimens for definitive clarification.
This prospective single institution study on 24 stage IV CRC patients has several limitations. The analysis has a low sample size, and consequently statistical power is very limited. There were 3 patients that had high tumor/liver volume ratio and CTC data available only. However, this is a unique and fundamental analysis on liver tumor burden with a novel character that provides very interesting data. Patients with metastatic CRC can be very heterogeneous and sometimes have previously received various systemic and surgical treatments. In our series, we included patients with a novel stage IV CRC diagnosis only. True baseline CTC and serum CEA levels were determined, as any local or systemic treatment can influence CTC quantity and serum CEA level, and would lead to treatment response in the liver.13 Another limitation was the fact that some patients did not undergo a contrast-enhanced CT scan, and had alternative imaging for staging. Liver volumetry data could not be gathered in these patients. Other reliable methods of liver or even whole-body tumor quantification, possibly by PET/CT analysis, should be further explored. Finally, our study does not include CTC number kinetics after initiation of treatment, and no follow-up outcome data were gathered.
Taken together, our study on a limited number of stage IV CRC patients suggests that high tumor burden in the liver and baseline serum CEA levels correlate with baseline CTC counts in stage IV CRC patients. Future studies should increase patient numbers, focus on the biologic significance of CTCs, and further investigate options for single CTC analysis to improve personalized treatment strategies.
Materials and Methods
Patient selection
Institutional Review Board (IRB) approval was obtained at Penn State Hershey Medical Center. Between January 2011 and March 2013, venous blood (7.5 ml) was prospectively drawn from 24 stage IV CRC patients that were evaluated for treatment at the multidisciplinary CRC clinics at the Penn State Hershey Cancer Institute. Inclusion criteria were patients with a novel diagnosis of stage IV CRC with active disease proven by biopsy or imaging criteria that have not received any treatments, so that CTC numbers and serum CEA levels were truly baseline.
CTC detection
CTC detection was performed with FDA-approved CellSearch® (Veridex, Raritan, NJ) system. 7.5 ml of venous blood were obtained after the first 5 ml of blood was discarded to avoid contamination with normal epithelial cells. Samples were collected in CellSave® tubes (Veridex), and all samples were analyzed within 3 d using the standard CellSearch® protocol and the CTC Epithelial Cell Kit (Veridex). The CellSearch® system qualifies a cell as a CTC if it is EPCAM+, and has an associated nucleus by DAPI, cytokeratin 8,18/19+, and CD45-. Analysis and enumeration of CTCs was conducted by a certified assay operator (D.D.) in a blinded fashion.
Clinical and pathological data
Clinical and pathological data were collected by reviewing electronic records, including primary tumor characteristics (TNM) and baseline serum CEA levels. Imaging (CT, MRI, PET and PET/CT scans) were discussed in a multidisciplinary cancer conference to determine metastatic organ involvement. Mutational status (KRAS, BRAF, PI3K, NRAS), microsatellite instability (MSI) and epidermal growth factor receptor (EGFR), excision repair cross-complementing group 1 (ERCC1), thymidylate synthetase (TS) expression were determined within the Department of Pathology, or by sending out specimens to Response DX Colon® (Los Angeles, CA), or Quest Diagnostics® (Lyndhurst, NJ).
Liver volumetry and calculations of liver/tumor volume ratio
Three-dimensional (3D) liver volume analysis (volumetry) was performed by technologists in a clinical 3D Lab, using an independent commercially available workstation (Aquarius Intuition, TeraRecon, Inc., Foster City, CA). All volumetric analysis was performed on the venous phase of the initial CT examination, to allow accurate differentiation of normal healthy liver from liver metastasis, as well as the identification and exclusion of the major vessels from volume analysis. Initially, the entire liver volume was calculated using a semi-automated technique, requiring contouring of the liver on selected CT slices with computer interpolation to complete the liver volume. Major vessels were excluded from the total liver volume calculation. Subsequently, each metastatic focus in the liver was manually contoured, and in case of multiple liver lesions, tumor volumes were added together. The ratio of liver tumor volume to liver volume was calculated using the following formula:
Liver and tumor volume analysis was not performed if non-contrast imaging studies were available only (i.e., PET-CT), as liver lesions would be more difficult to contour, and inaccuracies in identifying major vessels would occur.
EpCAM immunostaining of CRC tumors
The respective CRC primary tumors were chosen for EpCAM protein expression analysis by immunhistochemistry. All tissue specimens were fixed in buffered formalin, routinely processed and embedded in paraffin. Sections from representative tumor blocks of all cases were cut at 4-μm thickness, and hematoxylin and eosin (H&E) staining was performed per routine histology protocol. Antigen retrieval was done with EDTA (pH 8.0), and immunohistochemical staining for EpCAM with a monoclonal mouse antihuman antibody (clone BerEP4) (Dako, Carpinteria, CA) diluted 1:100 was performed on Dako Autostainer Plus® using the streptavidin-biotin-peroxidase system, and the signal was visualized with 3,3′-Diaminobenzidine (DAB) detection kit, applied according to the manufacturer's manual. The staining was visualized with Olympus® microscope and the images were captured with Olympus® DP26 digital camera (Tokyo, Japan). All slides were examined by a pathologist (Z. Y.).
Statistical analysis
Summary statistics, such as mean (±SEM) for quantitative measures and (relative) frequency numbers for the categorical measures were generated. The primary relationship of interest, the correlation between baseline CTC numbers (or number category) and various clinical parameters was studied using 2-sample Student's T-test, non-parametric Wilcoxon Rank-Sum test, or Fisher's Exact test when appropriate. Data transformation (for example, log-transformation) was done when necessary for the validity of statistical assumptions. All analyses were performed using statistical software SAS® version 9.3 (SAS Institute, Cary, NC, USA). Significance statements refer to a p-value of <0.05.
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
Acknowledgments
We thank all participating patients for their involvement in this study.
Funding
This work was supported by an Award of the Commonwealth Universal Research Enhancement Program (CURE/Tobacco Funds of the State of Pennsylvania) (J.T.K.). W.S.E-D. is an American Cancer Society Research Professor.
References
- 1.Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin 2010; 60:277–300; PMID:20610543; http://dx.doi.org/ 10.3322/caac.20073 [DOI] [PubMed] [Google Scholar]
- 2.Winawer S, Fletcher R, Rex D, Bond J, Burt R, Ferrucci J, Ganiats T, Levin T, Woolf S, Johnson D, et al.. Colorectal cancer screening and surveillance: clinical guidelines and rationale-Update based on new evidence. Gastroenterology 2003; 124:544–60; PMID:12557158; http://dx.doi.org/ 10.1053/gast.2003.50044 [DOI] [PubMed] [Google Scholar]
- 3.Liu MC, Shields PG, Warren RD, Cohen P, Wilkinson M, Ottaviano YL, Rao SB, Eng-Wong J, Seillier-Moiseiwitsch F, Noone AM, et al.. Circulating tumor cells: a useful predictor of treatment efficacy in metastatic breast cancer. J Clin Oncol 2009; 27:5153–9; PMID:19752342; http://dx.doi.org/ 10.1200/JCO.2008.20.6664 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wicha MS, Hayes DF. Circulating tumor cells: not all detected cells are bad and not all bad cells are detected. J Clin Oncol 2011; 29:1508–11; PMID:21422428; http://dx.doi.org/ 10.1200/JCO.2010.34.0026 [DOI] [PubMed] [Google Scholar]
- 5.Williams A, Balic M, Datar R, Cote R. Size-based enrichment technologies for CTC detection and characterization. Recent Results Cancer Res 2012; 195:87–95; PMID:22527497; http://dx.doi.org/ 10.1007/978-3-642-28160-0_8 [DOI] [PubMed] [Google Scholar]
- 6.Nagrath S, Sequist LV, Maheswaran S, Bell DW, Irimia D, Ulkus L, Smith MR, Kwak EL, Digumarthy S, Muzikansky A, et al.. Isolation of rare circulating tumour cells in cancer patients by microchip technology. Nature 2007; 450:1235–9; PMID:18097410; http://dx.doi.org/ 10.1038/nature06385 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lin HK, Zheng S, Williams AJ, Balic M, Groshen S, Scher HI, Fleisher M, Stadler W, Datar RH, Tai YC, et al.. Portable filter-based microdevice for detection and characterization of circulating tumor cells. Clin Cancer Res 2010; 16:5011–8; PMID:20876796; http://dx.doi.org/ 10.1158/1078-0432.CCR-10-1105 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Diehl F, Schmidt K, Choti MA, Romans K, Goodman S, Li M, Thornton K, Agrawal N, Sokoll L, Szabo SA, et al.. Circulating mutant DNA to assess tumor dynamics. Nat Med 2008; 14:985–90; PMID:18670422; http://dx.doi.org/ 10.1038/nm.1789 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hayes DF, Smerage JB. Circulating tumor cells. Prog Mol Biol Transl Sci 2010; 95:95–112; PMID:21075330; http://dx.doi.org/ 10.1016/B978-0-12-385071-3.00005-8 [DOI] [PubMed] [Google Scholar]
- 10.Lianidou ES, Mavroudis D, Sotiropoulou G, Agelaki S, Pantel K. What's new on circulating tumor cells? A meeting report. Breast Cancer Res 2010; 12:307; PMID:20727231; http://dx.doi.org/ 10.1186/bcr2601 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Yu M, Stott S, Toner M, Maheswaran S, Haber DA. Circulating tumor cells: approaches to isolation and characterization. J Cell Biol 2011; 192:373–82; PMID:21300848; http://dx.doi.org/ 10.1083/jcb.201010021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cohen SJ, Punt CJ, Iannotti N, Saidman BH, Sabbath KD, Gabrail NY, Picus J, Morse M, Mitchell E, Miller MC, et al.. Relationship of circulating tumor cells to tumor response, progression-free survival, and overall survival in patients with metastatic colorectal cancer. J Clin Oncol 2008; 26:3213–21; PMID:18591556; http://dx.doi.org/ 10.1200/JCO.2007.15.8923 [DOI] [PubMed] [Google Scholar]
- 13.Cohen SJ, Punt CJ, Iannotti N, Saidman BH, Sabbath KD, Gabrail NY, Picus J, Morse MA, Mitchell E, Miller MC, et al.. Prognostic significance of circulating tumor cells in patients with metastatic colorectal cancer. Ann Oncol 2009; 20:1223–9; PMID:19282466; http://dx.doi.org/ 10.1093/annonc/mdn786 [DOI] [PubMed] [Google Scholar]
- 14.Allen JE, El-Deiry WS. Circulating Tumor Cells and Colorectal Cancer. Curr Colorectal Cancer Rep 2010; 6:212–20; PMID:20890370; http://dx.doi.org/ 10.1007/s11888-010-0069-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.de Albuquerque A, Kubisch I, Stolzel U, Ernst D, Boese-Landgraf J, Breier G, Stamminger G, Fersis N, Kaul S. Prognostic and predictive value of circulating tumor cell analysis in colorectal cancer patients. J Transl Med 2012; 10:222; PMID:23146106; http://dx.doi.org/ 10.1186/1479-5876-10-222 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Headrick JR, Miller DL, Nagorney DM, Allen MS, Deschamps C, Trastek VF, Pairolero PC. Surgical treatment of hepatic and pulmonary metastases from colon cancer. Ann Thorac Surg 2001; 71:975–9; discussion 9-80; PMID:11216816; http://dx.doi.org/ 10.1016/S0003-4975(00)02522-4 [DOI] [PubMed] [Google Scholar]
- 17.Heinemann V, Douillard JY, Ducreux M, Peeters M. Targeted therapy in metastatic colorectal cancer – an example of personalised medicine in action. Cancer Treat Rev 2013; 39:592–601; PMID:23375249; http://dx.doi.org/ 10.1016/j.ctrv.2012.12.011 [DOI] [PubMed] [Google Scholar]
- 18.Joosse SA, Pantel K. Biologic challenges in the detection of circulating tumor cells. Cancer Res 2013; 73:8–11; PMID:23271724; http://dx.doi.org/ 10.1158/0008-5472.CAN-12-3422 [DOI] [PubMed] [Google Scholar]
- 19.Kaifi JT, Kunkel M, Zhu J, Dicker DT, Gusani NJ, Yang Z, Sarwani NE, Li G, Kimchi ET, Staveley-O'Carroll KF, et al.. Circulating tumor cells are associated with diffuse spread in stage IV colorectal cancer patients. Cancer biology & therapy 2013; 14; PMID:24153154 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Chun YS, Vauthey JN. Extending the frontiers of resectability in advanced colorectal cancer. Eur J Surg Oncol 2007; 33 Suppl 2:S52–8; PMID:18006265; http://dx.doi.org/ 10.1016/j.ejso.2007.09.026 [DOI] [PubMed] [Google Scholar]
- 21.Aggarwal C, Meropol NJ, Punt CJ, Iannotti N, Saidman BH, Sabbath KD, Gabrail NY, Picus J, Morse MA, Mitchell E, et al.. Relationship among circulating tumor cells, CEA and overall survival in patients with metastatic colorectal cancer. Ann Oncol 2013; 24:420–8; PMID:23028040; http://dx.doi.org/ 10.1093/annonc/mds336 [DOI] [PubMed] [Google Scholar]
- 22.Lu CY, Uen YH, Tsai HL, Chuang SC, Hou MF, Wu DC, Juo SH, Lin SR, Wang JY. Molecular detection of persistent postoperative circulating tumour cells in stages II and III colon cancer patients via multiple blood sampling: prognostic significance of detection for early relapse. Br J Cancer 2011; 104:1178–84; PMID:21343933; http://dx.doi.org/ 10.1038/bjc.2011.40 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Groot Koerkamp B, Rahbari NN, Buchler MW, Koch M, Weitz J. Circulating tumor cells and prognosis of patients with resectable colorectal liver metastases or widespread metastatic colorectal cancer: a meta-analysis. Ann Surg Oncol 2013. 20:2156–65; PMID:23456317; http://dx.doi.org/ 10.1245/s10434-013-2907-8 [DOI] [PubMed] [Google Scholar]
- 24.Rahbari NN, Bork U, Kircher A, Nimitz T, Scholch S, Kahlert C, Schmidt T, Steinert G, Ulrich AB, Reissfelder C, et al.. Compartmental Differences of Circulating Tumor Cells in Colorectal Cancer. Ann Surg Oncol 2012; 19:2195–202; PMID:22230943; http://dx.doi.org/ 10.1245/s10434-011-2178-1 [DOI] [PubMed] [Google Scholar]
- 25.Jiao LR, Apostolopoulos C, Jacob J, Szydlo R, Johnson N, Tsim N, Habib NA, Coombes RC, Stebbing J. Unique localization of circulating tumor cells in patients with hepatic metastases. J Clin Oncol 2009; 27:6160–5; PMID:19884529; http://dx.doi.org/ 10.1200/JCO.2009.24.5837 [DOI] [PubMed] [Google Scholar]
- 26.Cristofanilli M, Budd GT, Ellis MJ, Stopeck A, Matera J, Miller MC, Reuben JM, Doyle GV, Allard WJ, Terstappen LW, et al.. Circulating tumor cells, disease progression, and survival in metastatic breast cancer. N Engl J Med 2004; 351:781–91; PMID:15317891; http://dx.doi.org/ 10.1056/NEJMoa040766 [DOI] [PubMed] [Google Scholar]
- 27.de Bono JS, Scher HI, Montgomery RB, Parker C, Miller MC, Tissing H, Doyle GV, Terstappen LW, Pienta KJ, Raghavan D. Circulating tumor cells predict survival benefit from treatment in metastatic castration-resistant prostate cancer. Clin Cancer Res 2008; 14:6302–9; PMID:18829513; http://dx.doi.org/ 10.1158/1078-0432.CCR-08-0872 [DOI] [PubMed] [Google Scholar]
- 28.Gorges TM, Tinhofer I, Drosch M, Rose L, Zollner TM, Krahn T, von Ahsen O. Circulating tumour cells escape from EpCAM-based detection due to epithelial-to-mesenchymal transition. BMC Cancer 2012; 12:178; PMID:22591372; http://dx.doi.org/ 10.1186/1471-2407-12-178 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Zhang L, Ridgway LD, Wetzel MD, Ngo J, Yin W, Kumar D, Goodman JC, Groves MD, Marchetti D. The Identification and Characterization of Breast Cancer CTCs Competent for Brain Metastasis. Sci Transl Med 2013; 5:180ra48; PMID:23576814; http://dx.doi.org/ 10.1126/scitranslmed.3005109 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Mego M, De Giorgi U, Dawood S, Wang X, Valero V, Andreopoulou E, Handy B, Ueno NT, Reuben JM, Cristofanilli M. Characterization of metastatic breast cancer patients with nondetectable circulating tumor cells. Int J Cancer 2011; 129:417–23; PMID:20857493; http://dx.doi.org/ 10.1002/ijc.25690 [DOI] [PubMed] [Google Scholar]
- 31.Kaifi JT, Kunkel M, Das A, Harouaka RA, Dicker DT, Li G, Zhu J, Clawson GA, Yang Z, Reed MF, Gusani NJ, Kimchi ET, Staveley-O'Carroll KF, Zheng SY, El-Deiry WS . Circulating tumor cell isolation during resection of colorectal cancer lung and liver metastases: a prospective trial with different detection techniques. Cancer Biol Ther. 2015 Mar; 25:0. [Epub ahead of print] PMID:25807199 [DOI] [PMC free article] [PubMed] [Google Scholar]