

Abstract
Uterine perforation is one of the serious complications associated with use of the intrauterine contraceptive device (IUD). Uterine perforation by IUD can involve several neighboring organs. A case of acute appendicitis was caused by a Multiload Cu 375 IUD inserted previously. This is a rare complication and only fourteen previous cases were recorded in the literature.
Keywords: Appendicitis, Intrauterine contraceptive device, Uterine perforation
INTRODUCTION
Intrauterine contraceptive device (IUD) has been widely used since 1965[1]. Perforation of the uterus by an IUD is a rare and serious complication, occurring in 1/350 to 1/2 500 insertions[2]. Perforation by IUD can involve several neighboring organs such as the bladder, and particularly the intestinal tract[3] resulting frequently in serious complications which require intensive treatment including intestinal surgery. Perforation can occur during insertion or later[4]. Perforation occurring at the time of insertion correlates directly with the skill of the clinician. Delayed onset of symptoms is mostly due to chronic inflammatory reaction of copper-containing IUD. We report a case of acute appendicitis in a 50-year-old woman caused by a Multiload Cu 375 IUD inserted 18 years previously.
CASE REPORT
The patient was a 50-year-old gravida 3 para 3 woman, admitted because of severe lower abdominal pain associated with fever, nausea and vomiting. A Multiload Cu 375 IUD had been inserted, 18 years prior to the present admission and she did not receive regular physical examination after insertion.
On physical examination, the abdomen had decreased bowel sounds and rebounding tenderness mostly in the right lower quadrant. Laboratory data revealed leukocytosis and plain abdominal film showed the IUD to be overlying the right iliac crest (Figure 1). The abdomen was opened through a McBurney incision under the impression of acute appendicitis. The operative finding was the IUD located in the abdominal cavity behind the ileocecal junction and its tip had penetrated the tip of appendix (Figure 2). The whole area was edematous and covered with omentum. No fecalith impaction in appendix was found. Appendectomy was performed and the IUD was retrieved. The patient recovered uneventfully.
Figure 1.
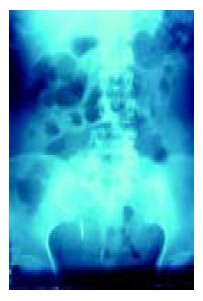
KUB showed IUD migration.
Figure 2.

Intraoperative photograph showing IUD penetrated the tip of appendix.
DISCUSSION
IUD is generally a safe modality for long-term contraception. Associated complications are bleeding, infection, ectopic pregnancy and uterine perforation. Uterine perforation is one of the most serious but uncommon complications associated with an IUD[3]. The mechanism of perforation is thought to be the insertion procedure or chronic inflammatory reaction with gradual erosion through the uterine wall[1]. The incidence is influenced by several factors including the timing of insertion, parity, previous abortions, type of IUD inserted, experience of the operator and position of the uterus[4]. Most of the perforations take place at the time of insertion. Delayed onset of symptoms supports secondary migration[1]. The timing of IUD insertion is flexible. Previous studies showed IUD insertion 0-3 mo postpartum increased the risk of uterine perforation as did insertions at 3-6 mo postpartum[4].
In this case, we considered the mechanism of IUD perforation was secondary by gradual erosion through uterine wall due to inserted 18 years prior to the present admission. No fecalith impaction in the appendix was found during operation and we considered that the acute appendicitis was induced by chronic inflammatory reaction of the copper-containing IUD.
Patients with IUD should be alerted about the possibility of its migration. Regular self examination for “missing threads” is useful in the early detection of migration of the IUD. A plain radiograph of the abdomen is usually the initial examination of choice to verify the presence of the IUD in the pelvis. Once found, an ultrasound examination has to be done to determine the location of the IUD relative to the uterus. The treatment of a migrated IUD is surgical, either laparoscopy or laparotomy. Withdrawal of the migrated IUD is advisable even if its migration has not given rise to any clinical symptoms[5] and can avoid further complications like bowel perforation, bladder perforation, or fistula formation[6]. To our knowledge, this is the 15th case of a perforated IUD causing acute appendicitis[7-18].
Footnotes
Science Editor Guo SY Language Editor Elsevier HK
References
- 1.Zakin D, Stern WZ, Rosenblatt R. Complete and partial uterine perforation and embedding following insertion of intrauterine devices. I. Classification, complications, mechanism, incidence, and missing string. Obstet Gynecol Surv. 1981;36:335–353. doi: 10.1097/00006254-198107000-00001. [DOI] [PubMed] [Google Scholar]
- 2.Ohana E, Sheiner E, Leron E, Mazor M. Appendix perforation by an intrauterine contraceptive device. Eur J Obstet Gynecol Reprod Biol. 2000;88:129–131. doi: 10.1016/s0301-2115(99)00142-6. [DOI] [PubMed] [Google Scholar]
- 3.Key TC, Kreutner AK. Gastrointestinal complications of modern intrauterine devices. Obstet Gynecol. 1980;55:239–244. [PubMed] [Google Scholar]
- 4.Heartwell SF, Schlesselman S. Risk of uterine perforation among users of intrauterine devices. Obstet Gynecol. 1983;61:31–36. [PubMed] [Google Scholar]
- 5.Treisser A, Colau JC. Causes, diagnosis and treatment of uterine perforations by intrauterine devices. J Gynecol Obstet Biol Reprod (Paris) 1978;7:837–847. [PubMed] [Google Scholar]
- 6.Berman MC, Cohen HL. Diagnostic Medical Sonography. Lippincott; 1997. Obstetrics and gynecology: A guide to clinical practice; pp. 569–571. [Google Scholar]
- 7.Carson SA, Gatlin A, Mazur M. Appendiceal perforation by Copper-7 intrauterine contraceptive device. Am J Obstet Gynecol. 1981;141:586–587. doi: 10.1016/s0002-9378(15)33284-1. [DOI] [PubMed] [Google Scholar]
- 8.Gruchy MV. Perforated appendix caused by an IUD. Med J Aust. 1982;2:116–117. doi: 10.5694/j.1326-5377.1982.tb124284a.x. [DOI] [PubMed] [Google Scholar]
- 9.Goldman JA, Peleg D, Feldberg D, Dicker D, Samuel N. IUD appendicitis. Eur J Obstet Gynecol Reprod Biol. 1983;15:181–183. doi: 10.1016/0028-2243(83)90135-1. [DOI] [PubMed] [Google Scholar]
- 10.McWhinney NA, Jarrett R. Uterine perforation by a Copper 7 intrauterine contraceptive device with subsequent penetration of the appendix. Case report. Br J Obstet Gynaecol. 1983;90:774–776. doi: 10.1111/j.1471-0528.1983.tb09310.x. [DOI] [PubMed] [Google Scholar]
- 11.Serra I. Appendicitis caused by an intrauterine contraceptive device. Br J Surg. 1986;73:927–928. doi: 10.1002/bjs.1800731130. [DOI] [PubMed] [Google Scholar]
- 12.McLaughlin DI, Bevins W, Karas BK, Sonnenberg L. IUD appendicitis during pregnancy. West J Med. 1988;149:601–602. [PMC free article] [PubMed] [Google Scholar]
- 13.Abbey RK, Gupta R, Sharma RK, Sood PC. Acute appendicitis--an unusual cause. Indian J Med Sci. 1999;53:108–110. [PubMed] [Google Scholar]
- 14.Rubinoff ML. IUD appendicitis. JAMA. 1975;231:67–68. [PubMed] [Google Scholar]
- 15.Chang TC, Eden JA. Intra-uterine device appendicitis. J Obstet Gynaecol (Lahore) 1989;9:257–258. doi: 10.3109/01443618909151058. [DOI] [PubMed] [Google Scholar]
- 16.Cuillier F, Ben Ghalem S, Haffaf Y. Intrauterine device appendicitis: an exceptional complication. J Gynecol Obstet Biol Reprod (Paris) 2003;32:55–57. [PubMed] [Google Scholar]
- 17.Khanna AK, Khanna A. Perforation of the appendix caused by an IUD. Med J Aust. 1986;144:109. doi: 10.5694/j.1326-5377.1986.tb113678.x. [DOI] [PubMed] [Google Scholar]
- 18.Katara AN, Chandiramani VA, Pandya SM, Nair NS. Migra-tion of intrauterine contraceptive device into the appendix. Indian J Surg. Indian J Surg. 2004;66:179–180. [Google Scholar]