

Supplemental digital content is available in the text.
KEY WORDS: Operational medicine, tactical medicine, telemedicine, damage-control surgery, surgical simulation
BACKGROUND
Hemorrhage is the leading cause of preventable posttraumatic death. Many such deaths may be potentially salvageable with remote damage-control surgical interventions. As recent innovations in information technology enable remote specialist support to point-of-care providers, advanced interventions, such as remote damage-control surgery, may be possible in remote settings.
METHODS
An anatomically realistic perfused surgical training mannequin with intrinsic fluid loss measurements (the “Cut Suit”) was used to study perihepatic packing with massive liver hemorrhage. The primary outcome was loss of simulated blood (water) during six stages, namely, incision, retraction, direction, identification, packing, and postpacking. Six fully credentialed surgeons performed the same task as 12 military medical technicians who were randomized to remotely telementored (RTM) (n = 7) or unmentored (UTM) (n=5) real-time guidance by a trauma surgeon.
RESULTS
There were no significant differences in fluid loss between the surgeons and the UTM group or between the UTM and RTM groups. However, when comparing the RTM group with the surgeons, there was significantly more total fluid loss (p = 0.001) and greater loss during the identification (p = 0.002), retraction (p = 0.035), direction (p = 0.014), and packing(p = 0.022) stages. There were no significant differences in fluid loss after packing between the groups despite differences in the number of sponges used; RTM group used more sponges than the surgeons and significantly more than the UTM group (p = 0.048). However, mentoring significantly increased self-assessed nonsurgeon procedural confidence (p = 0.004).
CONCLUSION
Perihepatic packing of an exsanguinating liver hemorrhage model was readily performed by military medical technicians after a focused briefing. While real-time telementoring did not improve fluid loss, it significantly increased nonsurgeon procedural confidence, which may augment the feasibility of the concept by allowing them to undertake psychologically daunting procedures.
Most battlefield casualties die of their injuries before ever reaching a surgeon.1–3 Before recent conflicts in Iraq and Afghanistan, studies found that traumatic hemorrhage resulted in more than 50% of all battlefield deaths.2 However, these recent conflicts have been characterized by a different type of warfare, asymmetric warfare against nontraditional combatants and small unit engagements instead of the set piece battles of the last century.1 As a result, hemorrhagic deaths have become even more prominent. Eastridge et al.1 reported that during Operation Iraqi Freedom and Operation Enduring Freedom, 87% of all battlefield injury fatalities occurred in the pre–medical treatment facility environment. Most (67%) of these were truncal injuries, with extremity (14%) and junctional (19%) injuries being less common sites.1 Much progress has been made in addressing both extremity and junctional hemorrhage, including improvements in techniques, system design, and pharmacology.4–6 With the aggressive training and dissemination of tourniquet use, an 85% decrease in peripheral extremity hemorrhage mortality has been documented.1 While junctional hemorrhage has been long considered a treatment gap in hemorrhage control, much attention and energy has been directed to addressing this challenge with a number of novel devices being introduced and trialed such as the Combat Ready Clamp (CRoC)7 and the iTClamp.8 However, there has been limited progress in developing techniques to control exsanguinating truncal hemorrhage in the pre–medical treatment facility environment, other than admonitions to decrease the time from point of injury to surgical intervention.1
Damage-control surgery refers to abbreviated techniques used when either the patient’s physiologic reserve or the “local capabilities” of a care setting are inadequate.9,10 Placing packs around bleeding solid organs and leaving the abdomen open are basic elements of damage-control surgery. Recently, remote damage-control resuscitation (RDCR) has been conceived as a method of extending damage-control principles to point of injury.11 Of all the important concepts embraced by RDCR, control of compressible hemorrhage and rapid surgical control of bleeding are the most difficult to achieve in the prehospital setting. However, we believe that these concepts require urgent study. In terms of mechanics, performing a laparotomy by incising the anterior abdominal wall to access the peritoneal cavity is technically practical especially in healthy young subjects with normal to lean body mass and no previous surgery.12 Nonphysicians have been previously reported to perform this successfully,13 although this would be predicted to be very intimidating and stressful to a nonsurgeon. It is possible, however, that recent information technology advances may facilitate this.
Telemedicine is defined as providing medicine at a distance.14 Remote telementoring is a specific telemedical technique wherein a remote expert is able to guide a novice in performing medical procedures outside his or her normal scope of practice in an urgent medical situation, using information technology.15 Remote telementoring has global applications, essentially enabling providers to deliver advanced medical care via remote guidance anywhere on (or above the) earth, which has internet connectivity or satellite coverage.16–19 Much work in this area has already been done by NASA investigators, who have successfully demonstrated the ability to remotely telementor emergency ultrasound examinations.20,21 Furthermore, reports of the telementoring of surgical procedures have described there being no obvious differences in skill acquisition among telementored versus locally mentored surgeons.22,23 Thus, we sought to explore the practicalities of mentoring surgically naive but motivated first responders to perform damage-control laparotomies and packing of exsanguinating liver injuries as a means of obtaining surgical control of truncal injuries in austere circumstances.
PATIENTS AND METHODS
Ethical approval for this study was obtained from the University of Calgary (REB14-0634) and the National Research Council of Canada. This was a randomized nonblinded trial where medical technicians (MedTechs) in the Canadian Armed Forces were randomized to perform a trauma laparotomy with or without telementoring on a human patient simulator.
Study Participants
All participants were volunteers who were free to withdraw from the study at any time without consequence. Military MedTechs were recruited from the 1 Canadian Field Hospital, a national-level element that reports directly to the Canadian Forces Health Services and provides deployable tertiary-level medical and surgical assets in support of the Canadian Armed Forces. A separate control group of fully credentialed surgeons performed the same task as military MedTechs to establish a benchmark for the primary outcomes of the study. None of these surgeons were telementored.
Independent Variable
MedTechs were randomized to an unmentored (n = 5) (UTM) or remotely telementored (n = 7) (RTM) group, which included real-time guidance by a trauma surgeon. Those allocated to the RTM group received continuous instructions and feedback from an experienced trauma surgeon with previous telementoring experience.
Equipment and Methods
Mentored MedTechs wore a USB audio headset with built-in microphone (Logitech, Romanel-sur-Morges, Switzerland) and wore a head-mounted 1.3-Megapixel video camera (Logitech Webcam 2 Megapixel Autofocus, Karl-Zeiss lens 2.0/3.7, Lausanne, Switzerland), which captured their point of view of the operative procedures required. This video capture was thereafter displayed on the mentor’s laptop computer (HP Probook 4520s, Hewlett Packard, Palo Alto, CA) through the use of Skype (Luxembourg City, Luxembourg), which provided for one-way visual and two-way audio communication over an encrypted Internet connection (Fig. 1). All study procedures were conducted in a ground floor room of a research building for all mentored procedures, with the remote mentor residing within a separate room on a separate floor of the same building using the internal wireless network.
Figure 1.

Remote mentor’s screen illustrating the surgical simulator as viewed through the MedTechs head-mounted camera.
Outcome
The primary outcome was “simulated blood loss” during a staged laparotomy on a surgical simulator with fluid loss measurement capabilities.
Surgical Task
All participants were asked to perform a laparotomy with midline incision into the peritoneal cavity followed by sponge packing of an exsanguinating liver hemorrhage (see Video, Supplemental Digital Content 1, http://links.lww.com/TA/A630). These surgical tasks were performed on the torso and viscera of a customized “Cut Suit” Human Worn Partial Task Surgical Simulator (Strategic Operations, San Diego, CA), without a human actor. The standardized laparotomy was compartmentalized into six different phases, each with a 60-second time limit, with specific objective goals to be accomplished within each task (Table 1). This compartmentalization was intended to allow study of the various subtasks required within the overall laparotomy and to facilitate comparisons with future studies in the weightless windows of parabolic flight. The primary outcome was the amount of fluid loss for 60 seconds after the hemostasis phase.
TABLE 1.
Compartmentalized Stages of the Standardized Laparotomy and Hepatic Packing

The specially modified Cut Suit torso was equipped with a sensitive fluid flow meter that recorded both total fluid loss and fluid loss velocities and was equipped with a remote control fob for accurate measurement of simulated hemorrhage (Fig. 2). The pressure setting of the Cut Suit pump was consistently set to the maximum flow rate of 12 psi (82.74 kPa). A senior surgeon (university professor and former command military surgeon) acted as a dual surgical assistant and safety surgeon for all participants. He was instructed to assist only as requested by the UTM MedTechs and surgeons and responded only to remote direction from the mentor for the RTM cohort of MedTechs. He did not handle any instruments or packs and only retracted as directed. He had, however, the authority to terminate all procedures by any participant he felt potentially unsafe.
Figure 2.
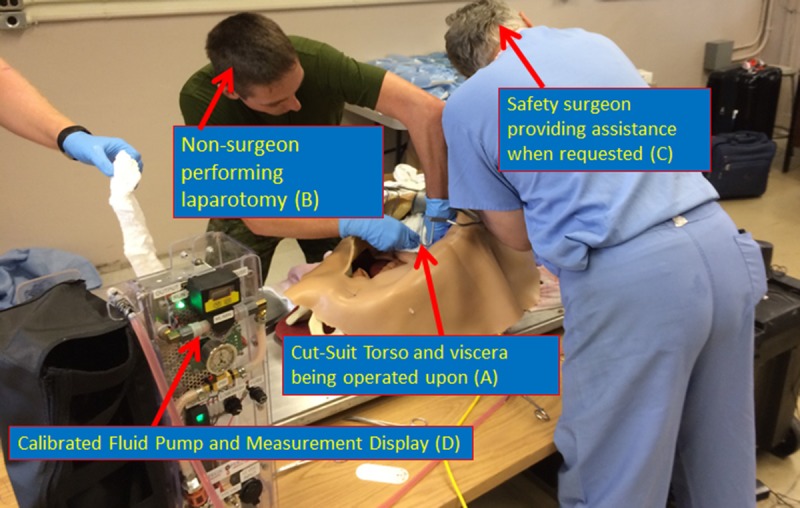
Simulated surgical suite for damage-control laparotomy and perihepatic packing. The torso and viscera of a customized Cut Suit (A) is being operated on by a nonsurgeon (B). Assistance is being provided only after a direct request from the experienced “safety surgeon” (C). Fluid loss representing the degree of massive hemorrhage is being measured by the calibrated fluid pump (D).
Randomization
After enrollment but before group allocation, all participants (including surgeons) were given a standardized introduction to the study, which included an introduction to damage-control surgery, the Cut Suit surgical trainer, and a tutorial on the basics of visceral packing for hemorrhage control (see Supplemental Digital Content 2, http://links.lww.com/TA/A631). After responding to questions and reinforcing the teaching, MedTechs were then randomized through random number generation to either laparotomy without telementoring (UTM) or laparotomy with remote telementoring (RTM).
The detailed study protocol is available online (see Supplemental Digital Content 3, http://links.lww.com/TA/A632). Prestudy questionnaires concerning demographics and previous surgical experience was administered to all participants (see Supplemental Digital Content 4, http://links.lww.com/TA/A633), as were posttest questionnaires (see Supplemental Digital Content 5, http://links.lww.com/TA/A634).
RESULTS
Six credentialed surgeons and 12 MedTechs were recruited. The MedTechs were randomized to unmentored (n = 5) (UTM) or remotely telementored (n = 7) (RTM) real-time guidance by a trauma surgeon. When comparing age and sex among the three groups, there was no significant difference. RTMs were mostly male, 5 (71.4%) of 7, and had a mean (SD) age of 32 (7) years. The UTM also consisted mainly of males, with 80% (4 of 5) being men. The mean (SD) age for the UTM was 31 (11) years. The surgeon group was mostly men (5 of 6, 83.3%), with a mean (SD) age of 37 (7) years. None of the MedTechs had a valid license to practice surgery or had training on intra-abdominal surgery, although the majority (12 of 13) had advanced trauma training such as Advanced Trauma Life Support. All of the surgeons in the study possessed a valid specialty certification from the Royal College of Physicians and Surgeons of Canada and held an independent license to practice surgery in a province of Canada. Moreover, all of the surgeons had been trained on intra-abdominal surgery, had taken advanced trauma training, and had been trained in and performed trauma laparotomies. Detailed specific procedure-related training that was captured is presented in Supplemental Digital Content 6 (http://links.lww.com/TA/A635).
All participants, notably all the MedTechs, were able to perform all steps of the trauma laparotomy and to place hemostatic packs around the liver. There were no instances that were considered unsafe by the safety surgeon, and no procedures required termination. However, no participant was able to complete the skin closure within 1 minute. The overall fluid lost by the surgeons was a mean of 1,819 mL, versus 2,144 mL for the UTM and 2,721 mL for the RTM MedTechs (Tables 2 and 3). This was significantly different between surgeons and RTM MedTechs (p = 0.005), but not between surgeons and UTM MedTechs (p = 1.000) or between the two groups of MedTechs (p = 0.432). When comparing surgeons with the RTM group, there was significantly greater loss during the identification (p = 0.002), retraction (p = 0.035), direction (p = 0.014), and packing (p = 0.022) stages. There were no significant differences in fluid loss after packing between the groups despite differences in the number of sponges used. The RTM MedTechs used more sponges under direction than surgeons and significantly more than UTM MedTechs (p = 0.048).
TABLE 2.
Study Group Performance During Simulated Laparotomy and Hepatic Packing
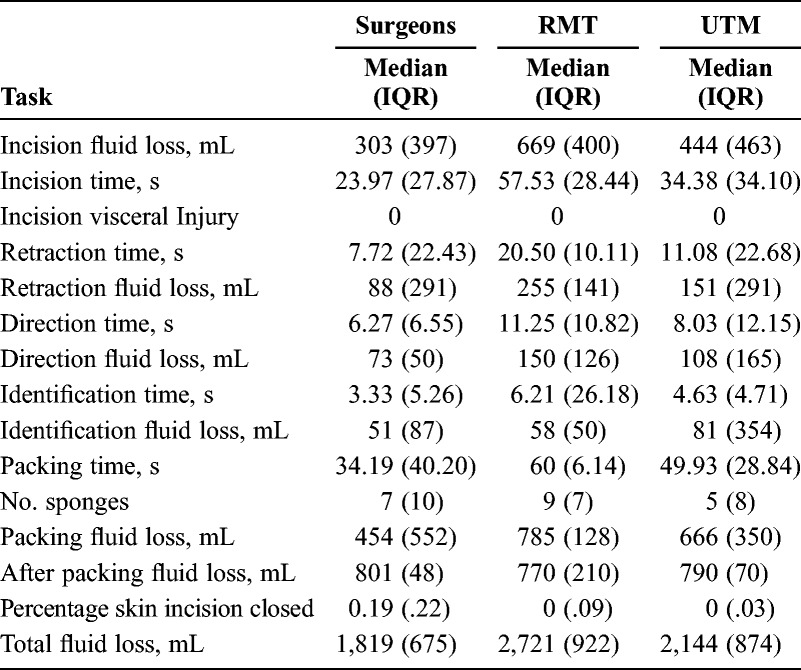
TABLE 3.
Table of p Value (Mann-Whitney U-Test) for the Study Group Performance During Simulated Laparotomy and Hepatic Packing

Mentoring significantly increased nonsurgeon procedural confidence when asked if damage-control laparotomy was a realistic task for them to perform (p = 0.030), if they felt confident in their current abilities to perform a damage-control laparotomy (p = 0.004), and if damage-control laparotomy would be less dangerous for the patient than beneficial in their hands (p = 0.004) for the RTM MedTechs compared with the UTM MedTechs. Surgeons were significantly more confident in their current ability to perform a damage-control laparotomy when compared with either RMT (p = 0.002) or UTM (p = 0.004) groups. The telementored group also felt strongly that telementoring was beneficial. When asked if they would want to be telementored again if they were asked to perform another laparotomy or if telementoring would increase their confidence when performing another laparotomy, subjects strongly agreed, answering a median of 5 of 5 on a Likert scale. When asked if telementoring would decrease their stress when performing another laparotomy, mentored subjects felt it would help, answering a median of 4 of 5 on the same scale (Table 2).
DISCUSSION
The Cut Suit is an anatomically accurate simulator that can be safely worn by humans and allows for the performance of a variety of complex, realistic surgeries and procedures as encountered in real casualties.24 After a relatively brief period of instruction, all nonsurgically trained military MedTechs were able to understand the basic principles and steps of a damage-control laparotomy and were able to perform one using a Cut Suit with simulated massive hemorrhage. Furthermore, after the completion of a surgical packing task, there was no significant difference in postpacking fluid loss between any group, implying that if a novice responder can access the site of hemorrhage, then an effective but radical prehospital intervention might be provided.
Thus, theoretically otherwise unsurvivable casualties with no other treatment options might be offered such as a lifesaving intervention (LSI), considering that the most recent review of Canadian Forces deaths in Afghanistan automatically deemed all cases of torso exsanguination “nonpreventable.”25 The Trauma Hemostasis and Oxygenation Research (THOR) Network has defined an LSI as a medical procedure that if not performed conveys a high probability of morbidity or death,11,26 with the terms far-forward and austere denoting environments in which professional health care providers do not normally operate.11 Delayed evacuations refer to situations in which evacuation times exceed 60 minutes and prolonged for more than 6 hours from point of wounding until arrival at a medical treatment facility capable of providing damage-control surgery.11 The current reality is that the wounded warriors of the future will increasingly be seriously injured in far-forward locations, facing prolonged or nonevacuations, being cared for by motivated but nonsurgically trained providers, yet requiring LSIs (most commonly for hemorrhage control) if they have a hope of survival.
Gerhardt et al.26 recently reviewed data from a forward operating base supporting urban combat. They found that while LSIs were required in most casualties requiring evacuation, the scope of practice required for performing these LSIs before medical treatment facility arrival were beyond that of conventional forces combat medics, and thus, few LSIs were performed by them near the point of injury. They thus speculated that emergency telemedical direction might enable the potential deployment of advanced LSIs, thus providing a more efficient RDCR to those most in need.26 Telemedicine is simply the provision of medical care at a distance using communication technologies. Remote telementoring is a form of telemedicine that involves a more experienced mentor providing guidance at a distance to a less experienced mentee who may be performing any number of required tasks.15,23,27,28 Mentoring may be best achieved in a “just in time” fashion where an appropriate mentor is available to facilitate problem solving in response to immediate needs.27 With ongoing improvements in technology and especially connectivity, it is likely that austere medical situations in the future will have access to remote medical direction. We used a conceptually (but not necessarily technically) simple model of hepatic packing. It is likely that other remote damage-control surgical techniques may also be telementorable, and further efforts will continue to evaluate these requirements. Any amount of prepreformance briefing would be highly desirable and augmentative to the flexibility in the scope telementoring provides.
Great strides have been made through the introduction of RDCR techniques and philosophies in recent years,11 with major advances in resuscitative techniques that a far-forward damage-control laparotomy might not be unthinkable. Chaudery et al.29 recently reviewed the current technologies potentially available in the prehospital setting to enable abdominal hemorrhage control in catastrophic hemorrhage, noting that most studies were preclinical in vivo trials. Of the potential techniques, specifically intra-abdominal foam injection30–32 and resuscitative endovascular aortic balloon occlusion,33,34 were considered as attractive candidates.29 Chaudery et al. notably did not consider prehospital open surgical interventions as a potential option despite noting that “manual force is one of the most effective means of controlling bleeding.” However, as early as 1983, NASA think-tanks identified the ability to perform laparotomy as the minimum desirable surgical capability to save lives before transfer to earth, arguably one of the most dramatic prehospital settings.35,36
In the present study, there was no difference in fluid loss between nonmentored MedTechs and surgeons; however, there was greater fluid loss in those being mentored. This was likely related to the technical settings of the Cut Suit, which has a versatile fluid loss capability. Thus, the selection of a 12 psi (82.74 kPa) hemorrhage rate, while accurately replicating conditions of exsanguination, was conducted at supraphysiologic pressures, greatly exaggerating any effect of delay, even appropriate delay, on fluid loss parameters in any group. We thus speculate that the mentored group had greater fluid loss because of the brief but inherent nature of a two-way communication between the mentor and the mentee. So while this delay likely explains increased fluid loss, the increased confidence that the mentored MedTechs reported was notable. Preliminary data still being fully analyzed noted that the while the RTM MedTechs demonstrated stress levels similar to those of the surgeons, the UTM MedTechs had significantly higher stress levels as indexed by the low frequency–to–high frequency ratio of heart rate variability (Jocelyn Keillor, personal communication, February 1, 2014). Therefore, one of the greatest benefits of the telepresence of an experienced and presumably emotionally distanced expert may be to bring reassurance and confidence to a far-forward responder, who will often unfortunately be extremely emotionally close to the victim.
The information technologies used were simple “off-the-shelf” software with two-way audio and one-way video display as this was a proof-of-concept study. The Skype proprietary “closed source” software is protected by multiple systems to address security and privacy.37 All information is sent over secured socket layer that uses 256-bit Advanced Encryption Standard (AES) for all the information, leaving a transmitting computer that can only be decrypted by the Skype server. Nonetheless, greater encryption will typically be required for special operations. It is only logical that ever greater information and encryption capabilities will continue to expand in the future. The same can be expected of the degree of communication richness between the mentor and the mentee. The mentored MedTechs could only hear the remote mentor. There are rapidly evolving technologies in which the mentor may in the future by able to telestrate38 on displayed images such as anatomy demonstration on a heads-up video display39 worn by the MedTech for instance.
Limitations of the Study
There are limitations to this study. We were not able to measure iatrogenic injuries as a result of improper laparotomy techniques. Therefore, this may have biased the study against telementored medics. More “simulated blood loss” was observed in the telementored group, as these medics took longer to open the abdomen and pack the solid organs. While the Cut Suit currently will demonstrate gross inadvertent bowel injuries and advances in the materials and construction of the model is constantly progressing, mammalian tissues are still perceived to be more susceptible to inadvertent injury. Thus, future complementary studies may be considered in animal models, where the outcome of interest is not only time to task completion and successful solid organ packing but also iatrogenic injuries to the bowel or other visceral structures.
In conclusion, perihepatic packing of an exsanguinating liver hemorrhage simulation was readily performed by military MedTechs after a focused briefing without obvious performance differences compared with trained surgeons. While real-time RTM did not improve study outcomes, it significantly increased nonsurgeon procedural confidence, which may increase the feasibility of the concept in actual operational application.
Supplementary Material
ACKNOWLEDGMENT
We thank Major Barbaraanne Besenyodi, Major Douglas Kromrey, Master Warrant Officer Danyal Beale, Warrant Officer Paul Trudel, Warrant Officer (Retired) Patrick Papineau, Dr. Brett Mador, Dr. Michael Kim, Dr. Jacinthe Lampron, and Dr. Paul Cantle for supporting the study.
DISCLOSURE
This research was primarily funded by the Canadian Forces Health Services with support from the Royal College of Physicians and Surgeons on Canada. A.W.K. was the principal investigator of a randomized trial on open abdomen management funded by the Kinetic Concepts Corporation. A.W.K. has received travel reimbursement to attend laboratories from the Innovative Trauma Care, Synthes, and Life Cell Corporations and the donation of a NannoMax portable ultrasound machine for unrestricted research purposes from the Sonosite Corporation. J.L.M. is the research director of Innovative Trauma Care, Edmonton, Alberta, Canada. K.L. is the executive vice-president of Strategic Operations, San Diego, California.
Footnotes
Trial Registration: ID ISRCTN/77929274.
This study was presented at the annual meeting of the Trauma Association of Canada, April 9–10, 2015, in Calgary, Alberta, Canada.
The opinions expressed herein represent those of the authors alone and do not reflect any official policies or opinions representative of the Canadian Forces or any other official departments of the Governments of Canada or the United States.
Supplemental digital content is available for this article. Direct URL citations appear in the printed text, and links to the digital files are provided in the HTML text of this article on the journal’s Web site (www.jtrauma.com).
REFERENCES
- 1. Eastridge BJ, Mabry RL, Seguin P, Cantrell J, Tops T, Uribe P, Mallett O, Zubko T, Oetjen-Gerdes L, Rasmussen TE, et al. Death on the battlefield (2001–2011): implications for the future of combat casualty care. J Trauma Acute Care Surg. 2012; 73: S431– S437. [DOI] [PubMed] [Google Scholar]
- 2. Bellamy RF. The causes of death in conventional land warfare: implications for combat casualty care research. Mil Med. 1984; 149: 55– 62. [PubMed] [Google Scholar]
- 3. Bellamy RF, Maningas PA, Vayer JS. Epidemiology of trauma: military experience. Ann Emerg Med. 1986; 15: 1384– 1388. [DOI] [PubMed] [Google Scholar]
- 4.CRASH-2 Collaborators IBS. Effect of tranexamic acid in traumatuc brain injury: a nested randomized, placebo, controlled trial (CRASH-2 Intracranial Bleeding Study). Br Med J. 2011; 343: d3795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Beekley AC, Sebesta JA, Blackbourne LH, Herbert GS, Kauvar DS, Baer DG, Walters TJ, Mullenix PS, Holcomb JB. Prehospital tourniquet use in Operation Iraqi Freedom: effect on hemorrhage control and outcomes. The Journal of trauma. 2008; 64: S28– S37; discussion S. [DOI] [PubMed] [Google Scholar]
- 6. Kotwal RS, Montgomery HR, Kotwal BM, Champion HR, Butler FK, Jr, Mabry RL, Cain JS, Blackbourne LH, Mechler KK, Holcomb JB. Eliminating preventable death on the battlefield. Arch Surg. 2011; 146: 1350– 1358. [DOI] [PubMed] [Google Scholar]
- 7. Kheirabadi BS, Terrazas IB, Hanson MA, Kragh JF, Jr, Dubick MA, Blackbourne LH. In vivo assessment of the Combat Ready Clamp to control junctional hemorrhage in swine. J Trauma Acute Care Surg. 2013; 74: 1260– 1265. [DOI] [PubMed] [Google Scholar]
- 8. Filips D, Logsetty S, Tan J, Atkinson I, Mottet K. The iTClamp controls junctional bleeding in a lethal swine exsanguination model. Prehosp Emerg Care. 2013; 17: 526– 532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Burch JM, Ortiz VB, Richardson RJ, Martin RR, Mattox KL, Jordan GL., Jr Abbreviated laparotomy and planned reoperation for critically injured patients. Ann Surg. 1992; 215: 476– 483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Mattox KL. Introduction, background, and future projections of damage control surgery. Surg Clin North Am. 1997; 77: 753– 759. [DOI] [PubMed] [Google Scholar]
- 11. Jenkins DH, Rappold JF, Badloe JF, Berséus O, Blackbourne L, Brohi KH, Butler FK, Cap AP, Cohen MJ, Davenport R, et al. Trauma hemostasis and oxygenation research position paper on remote damage control resuscitation: definitions, current practice, and knowledge gaps. Shock. 2014; 41(Suppl 1): 3– 12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Kirkpatrick AW, Campbell MR, Jones JA, Broderick TJ, Ball CG, McBeth PB, McSwain NE, Hamilton DR, Holcomb JB. Extraterrestrial hemorrhage control: terrestrial developments in technique, technology, and philosophy with applicability to traumatic hemorrhage control in long-duration spaceflight. J Am Coll Surg. 2005; 200: 64– 76. [DOI] [PubMed] [Google Scholar]
- 13. Tisherman SA, Vandevelde K, Safar P, Morioka T, Obrist W, Corne L, Buckman RF, Rubertsson S, Stephenson HE, Grenvik A, et al. Future directions for resuscitation research. V. Ultra-advanced life support. Resuscitation. 1997; 34: 281– 293. [DOI] [PubMed] [Google Scholar]
- 14. Zachariah R, Bienvenue B, Ayada L, Manzi M, Maalim A, Engy E, Jemmy JP, Ibrahim Said A, Hassan A, Abdulrahaman F, et al. Practicing medicine without borders: tele-consultations and tele-mentoring for improving paediatric care in a conflict setting in Somalia? Trop Med Int Health. 2012; 17: 1156– 1162. [DOI] [PubMed] [Google Scholar]
- 15. Pian L, Gillman LM, McBeth PB, Xiao Z, Ball CG, Blaivas M, Hamilton DR, Kirkpatrick AW. Potential Use of Remote Telesonography as a Transformational Technology in Underresourced and/or Remote Settings. Emerg Med Int. 2013; 2013: 986160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Kirkpatrick AW, Blaivas M, Sargsyan AE, McBeth PB, Patel C, Xiao Z, Pian L, Panebianco N, Hamilton DR, Ball CG, et al. Enabling the mission through trans-Atlantic remote mentored musculoskeletal ultrasound: case report of a portable hand-carried tele-ultrasound system for medical relief missions. Telemed J E Health. 2013; 19: 530– 534. [DOI] [PubMed] [Google Scholar]
- 17. Crawford I, McBeth PB, Mitchelson M, Tiruta C, Ferguson J, Kirkpatrick AW. Telementorable “just-in-time” lung ultrasound on an iPhone. J Emerg Trauma Shock. 2011; 4: 526– 527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. McBeth P, Crawford I, Tiruta C, Xiao Z, Zhu GQ, Shuster M, Sewell L, Panebianco N, Lautner D, Nicolaou S, et al. Help is in your pocket: the potential accuracy of smartphone- and laptop-based remotely guided resuscitative telesonography. Telemed J E Health. 2013; 19: 924– 930. [DOI] [PubMed] [Google Scholar]
- 19. McBeth PB, Crawford I, Blaivas M, Hamilton T, Musselwhite K, Panebianco N, Melniker L, Ball CG, Gargani L, Gherdovich C, et al. Simple, almost anywhere, with almost anyone: remote low-cost telementored resuscitative lung ultrasound. J Trauma. 2011; 71: 1528– 1535. [DOI] [PubMed] [Google Scholar]
- 20. Fincke EM, Padalka G, Lee D, van Holsbeeck M, Sargsyan AE, Hamilton DR, Martin D, Melton SL, McFarlin K, Dulchavsky SA. Evaluation of shoulder integrity in space: first report of musculoskeletal US on the International Space Station. Radiology. 2005; 234: 319– 322. [DOI] [PubMed] [Google Scholar]
- 21. Sargsyan AE, Hamilton DR, Jones JA, Melton S, Whitson PA, Kirkpatrick AW, Martin D, Dulchavsky SA. FAST at MACH 20: clinical ultrasound aboard the International Space Station. J Trauma. 2005; 58: 35– 39. [DOI] [PubMed] [Google Scholar]
- 22. Ponsky TA, Bobanga ID, Schwachter M, Stathos TH, Rosen M, Parry R, Nalugo M, Rothenberg SS. Transcontinental telementoring with pediatric surgeons: proof of concept and technical considerations. J Laparoendosc Adv Surg Tech A. 2014; 24: 892– 896. [DOI] [PubMed] [Google Scholar]
- 23. Rosser JC, Wood M, Payne JH, Fullum TM, Lisehora GB, Rosser LE, Barcia PJ, Savalgi RS. Telementoring. A practical option in surgical training. Surg Endosc. 1997; 11: 852– 855. [DOI] [PubMed] [Google Scholar]
- 24. Hoang TN, Kang J, Laporta AJ, Makler VI, Chalut C. Filling in the gaps of predeployment fleet surgical team training using a team-centered approach. J Spec Oper Med. 2013; 13: 22– 33. [DOI] [PubMed] [Google Scholar]
- 25. Pannell D, Brisebois R, Talbot M, Trottier V, Clement J, Garraway N, McAlister V, Tien HC. Causes of death in Canadian Forces members deployed to Afghanistan and implications on tactical combat casualty care provision. J Trauma. 2011; 71: S401– S407. [DOI] [PubMed] [Google Scholar]
- 26. Gerhardt RT, Berry JA, Blackbourne LH. Analysis of life-saving interventions performed by out-of-hospital combat medical personnel. J Trauma. 2011; 71: S109– S113. [DOI] [PubMed] [Google Scholar]
- 27. Jaffer U, Vaughan-Huxley E, Standfield N, John NW. Medical mentoring via the evolving world wide web. J Surg Educ. 2013; 70: 121– 128. [DOI] [PubMed] [Google Scholar]
- 28. Miller JA, Kwon DS, Dkeidek A, Yew M, Hisham Abdullah A, Walz MK, Perrier ND. Safe introduction of a new surgical technique: remote telementoring for posterior retroperitoneoscopic adrenalectomy. ANZ J Surg. 2012; 82: 813– 816. [DOI] [PubMed] [Google Scholar]
- 29. Chaudery M, Clark J, Wilson MH, Bew D, Yang GZ, Darzi A. Traumatic intra-abdominal hemorrhage control: has current technology tipped the balance toward a role for prehospital intervention? J Trauma Acute Care Surg. 2015; 78: 153– 163. [DOI] [PubMed] [Google Scholar]
- 30. Rago A, Duggan MJ, Marini J, Beagle J, Velmahos G, De Moya MA, Sharma U, Hwabejire J, King DR. Self-expanding foam improves survival following a lethal, exsanguinating iliac artery injury. J Trauma Acute Care Surg. 2014; 77: 73– 77. [DOI] [PubMed] [Google Scholar]
- 31. Peev MP, Rago A, Hwabejire JO, Duggan MJ, Beagle J, Marini J, Zugates G, Busold R, Freyman T, Velmahos GS, et al. Self-expanding foam for prehospital treatment of severe intra-abdominal hemorrhage: dose finding study. J Trauma Acute Care Surg. 2014; 76: 619– 623. [DOI] [PubMed] [Google Scholar]
- 32. Duggan MJ, Rago A, Marini J, Beagle J, Peev M, Velmahos G, Sharma U, King DR. Development of a lethal, closed-abdomen, arterial hemorrhage model in noncoagulopathic swine. J Surg Res. 2014; 187: 536– 541. [DOI] [PubMed] [Google Scholar]
- 33. Morrison JJ, Percival TJ, Markov NP, Villamaria C, Scott DJ, Saches KA, Spencer JR, Rasmussen TE. Aortic balloon occlusion is effective in controlling pelvic hemorrhage. J Surg Res. 2012; 177: 341– 347. [DOI] [PubMed] [Google Scholar]
- 34. Morrison JJ, Ross JD, Rasmussen TE, Midwinter MJ, Jansen JO. Resuscitative endovascular balloon occlusion of the aorta: a gap analysis of severely injured UK combat casualties. Shock. 2014; 41: 388– 393. [DOI] [PubMed] [Google Scholar]
- 35. Houtchens B. System for the management of trauma and emergency surgery in space: final report. Houston, Texas; 1983. 1983. [DOI] [PubMed] [Google Scholar]
- 36. Kirkpatrick AW, Ball CG, Campbell M, Williams DR, Parazynski SE, Mattox KL, Broderick TJ. Severe traumatic injury during long duration spaceflight: light years beyond ATLS. J Trauma Manag Outcomes. 2009; 3: 4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Crawford I, McBeth PB, Mitchelson M, Fergusen J, Tiruta C, Kirkpatrick AW. How to set up a low cost tele-ultrasound capable videoconferencing system with wide applicability. Crit Ultrasound J. 2012; 4: 13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Budrionis A, Augestad KM, Patel HR, Bellika JG. An evaluation framework for defining the contributions of telestration in surgical telementoring. Interact J Med Res. 2013; 2: e14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Carenzo L, Barra FL, Ingrassia PL, Colombo D, Costa A, Della Corte F. Disaster medicine through Google Glass. Eur J Emerg Med. 2015; 22: 222– 225. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.