

Abstract
Background
Levels of drinking are unusually elevated among young adults on the U.S.-Mexico border, and this elevation can be largely explained by young border residents’ unusually high frequency of bar attendance. However, this explanation complicates interpretation of high alcohol problem rates that have also been observed in this group. Because bar environments can lower the threshold for many types of problems, the extent to which elevated alcohol problems among young border residents can be attributed to drinking per se – versus this common drinking context – is not clear.
Methods
Data were collected from multi-stage cluster samples of adult Mexican Americans on and off the U.S.-Mexico border (current drinker N=1351). After developing structural models of acute alcohol problems, estimates were subjected to path decompositions to disentangle the common and distinct contributions of drinking and bar attendance to problem disparities on and off the border. Additionally, models were estimated under varying degrees of adjustment to gauge the sensitivity of the results to sociodemographic, social-cognitive, and environmental sources of confounding.
Results
Consistent with previous findings for both drinking and other problem measures, acute alcohol problems were particularly elevated among young adults on the border. This elevation was entirely explained by a single common pathway involving bar attendance frequency and drinking. Bar attendance did not predict acute alcohol problems independently of drinking, and its effect was not moderated by border proximity or age. The common indirect effect and its component effects (of border youth on bar attendance, of bar attendance on drinking, and of drinking on problems) were surprisingly robust to adjustment for confounding in all parts of the model (e.g., fully adjusted indirect effect: b=.11, SE=.04, p<.01).
Conclusions
Bar attendance and associated increases in drinking play a key, unique role in the high levels of acute alcohol problems among the border’s young adult population that cannot be entirely explained by sociodemographic or social-cognitive characteristics of young border residents, by contextual effects of bars on problems, or by broader neighborhood factors. Bar attendance in particular may represent an early modifiable risk factor that can be targeted to reduce alcohol problem disparities in the region.
Keywords: BARS, ALCOHOL PROBLEMS, SOCIAL COGNITIONS, MEXICAN AMERICANS, U.S.-MEXICO BORDER
More than seven million people live near the U.S.-Mexico border, a 2,000 mile region of the southern United States separating two countries with longstanding differences in alcohol policy. Relative to other U.S. regions, levels of drinking and alcohol-related problems are higher on the U.S. side of the border, especially among younger age groups (Caetano et al., 2012, Caetano et al., 2013a, Vaeth et al., 2012; Mills, Caetano, & Vaeth, 2012b; Mills et al., in press). This interactive pattern is consistent with known risk factors in the region. In Mexico, the legal drinking age is 18, alcohol is relatively inexpensive, and bars (many of which are within walking distance of border crossing areas) cater specifically to a younger clientele by promoting an intensely social, party-like atmosphere (Lange et al., 2002, Voas et al., 2002).
Each year, a subset of U.S. border residents capitalize on these incentives and travel to Mexico to drink (Lange & Voas, 2000), which in turn contributes to higher annual levels of drinking and problems on the U.S. side of the border. For example, those who reported physically crossing into Mexico to drink in the past year were younger (over 47% were 18–20 years old) and reported more annual drinking and problems than those who did not cross (Caetano et al., 2012, 2013b). However, these differences do not fully account for observed disparities on the U.S. side. Over 75% of the U.S. border population reported not crossing into Mexico to drink at all in the past year, and levels of drinking remained elevated among those who did not cross and among young adults (ages 18–29) in general (Caetano et al., 2012, 2013b, Mills et al., 2012b; in press).
Mills et al. (2012b; in press) examined whether two types of variables long considered relevant to risky drinking on the Mexico side of the border – bar attendance and social cognitions about drinking (e.g., attitudes, expectancies, norms, motives) – might also explain increased drinking on the U.S. side of the border. Both sets of variables related to drinking in theoretically sensible ways. For example, bar attendance and favorable alcohol-related attitudes were strong positive predictors of drinking. Surprisingly however, only bar attendance could explain the specific elevation in drinking among young border residents. In particular, younger border adults (18–29) attended bars more frequently and drank more alcohol than their non-border counterparts (young or old), despite holding comparable (if not more conservative) alcohol-related cognitions.
In the present study, we extend this line of investigation to the role of bar attendance in the higher rates of alcohol problems that have been observed among younger border age groups (Caetano et al., 2013a, Vaeth et al., 2012). On one hand, this extension follows naturally from previous results: If bar attendance explains increased drinking among border youth, it likely contributes to their higher rates of alcohol problems as a consequence. However, there is also considerable evidence that bar environments affect the likelihood of acute types of alcohol problems independently of drinking. For example, crowding, large groups of young men, low monitoring by staff, sexual competition, and tolerance for rowdy behavior are all environmental characteristics known to lower the threshold for acute alcohol-related problems like accidents and physical/sexual aggression (e.g., Graham et al., 2006a, 2006b, Homel et al., 1992). That is, they affect the likelihood of problems independently of drinking. These characteristics are particularly common in bars on the Mexico side of the border (Lange et al., 2002, Voas et al., 2002, Lange & Voas, 2000).
This raises a question: If border youth are attending bars more than non-border groups in the U.S., to what extent can their higher rates of alcohol problems be attributed to 1) natural increases in drinking that co-occur with bar attendance, versus 2) more frequent exposure to bar drinking contexts, independently of associated increases in drinking? Following past work and the fact that bar environments should be particularly conducive to problems linked to transient compromises in cognitive-behavioral and motor function that follow heavy ethanol consumption, we focus specifically on acute problems that can occur due to isolated episodes of acute intoxication.
In asking these questions, we presume certain real-world data-generating mechanisms – for example, drinking alcohol causes acute alcohol-related problems, and bar attendance has an independent causal influence on drinking. At issue is whether such a structure can account for the specific pattern of disparities we see across the more distal variables of age and location (border versus non-border). A mediation framework provides a natural way to address these kinds of questions, but it is complicated by the interactive pattern of age and location differences in alcohol outcomes seen to date, as what exactly it is that we seek to explain does not correspond to a standard main effect (e.g., border versus non-border) or even to a simple effect (e.g., border versus non-border among younger age groups). Rather, it corresponds to a shift in the magnitude of the border effect with age, where – due to theoretical factors and empirical considerations reviewed above – alcohol-related risks are selectively increased among the border region’s young adult population. To understand what explains this interaction in the sense of statistical mediation (i.e., a question of mediated moderation), we will therefore need to work with a quantified estimate of the interaction effect when estimating its direct and indirect influences on the outcome, using standard mediation techniques. This will be complemented by post-hoc comparisons of various simple effects within subgroups (e.g., border effects within age subgroups) in models that exclude and include hypothesized mediators. To the extent hypothesized mediators account for the interaction, controlling for them should lead to selective decreases in alcohol-related risks among border young adults.
A modeling framework to disentangle these effects is depicted in Figure 1. We depict the interaction as the unique, synergistic effect of being both young and a border resident (component effects of border residence and age are not shown in Figure 1 but were included in all models). The primary hypothesized indirect pathway – representing elevations in problems among border youth that can be attributed to both bar attendance and drinking – is depicted in bold and includes paths P1, P2, and P3. Conversely, problem elevations among border youth due that can be attributed to bar attendance – but not drinking – are captured by the P1 and P5 paths. Given the findings reviewed above, we expected this pathway to contribute significantly to acute problems as well. Based on previous findings (Mills et al., 2012b, in press), we had no specific expectations about the two other pathways shown in Figure 1.
Figure 1.

Four pathways that could explain an association between border youth and acute alcohol problems. For simplicity, not all exogenous covariates are shown. If border youth attend bars more often than other groups, higher rates of problems might reflect associated increases in drinking (an indirect pathway involving parameters P1, P2, and P3), and/or effects of bar attendance on problems that cannot be attributed to drinking (an indirect pathway involving parameters P1 and P5). Border youth may also exhibit drinking-related increases in problems even after adjusting for differences in rates of bar attendance (an indirect pathway involving parameters P4 and P3). Finally, border youth may report higher levels of acute problems independently of both bar attendance and drinking (a direct effect captured by parameter P6).
We also address two other sets of questions. First, effects depicted in Figure 1 may be obscured by several theoretically plausible moderating effects involving proximity to the border and age. For example, due to their geographic proximity to Mexico, bars in U.S. border regions may have more in common with Mexico bars than with bars deeper within U.S. territory. If these similarities encompass factors thought to underlie the P5 path in Figure 1 (e.g., crowding, rowdy behavior), that effect may very well be stronger in U.S. border regions than in non-border regions. Similarly, bar environments in general may be more conducive to acute alcohol problems for younger age groups due to developmental trends in risk behavior. Consequently, we explicitly test whether border residence or age moderate the bar attendance effect on drinking (P2 in Figure 1) and on problems (P5).
Second, although Figure 1 draws attention to two theoretical mediators we believe are especially relevant to elevated alcohol problems among border youth, other demographic, sociocultural, and environmental characteristics may be confounded with these effects. Moreover, these confounding influences would not necessarily be restricted to any one variable in Figure 1. For example, neighborhood characteristics such as poverty, violence, and perceptions of order/disorder have all been linked to multiple outcome variables shown in Figure 1. Living in an impoverished neighborhood may contribute to observed disparities in alcohol problems via direct effects on rates of bar attendance (due to higher alcohol outlet density in impoverished areas; Berke el at., 2009, Romley et al., 2007), drinking (due to stresses of living in impoverished areas; Mulia et al., 2008, Hill & Angel, 2005), or both. To clarify both the overall impact of confounding on border disparities in acute alcohol problems and exactly where in the model the confounding occurs, we employ a path analytic framework that allows us to simultaneously adjust for confounding in each of the Figure 1 variables.
To recap, elevations in drinking among young adults living on the northern side of the U.S.-Mexico border seems to be closely linked to their high annual frequency of bar attendance (Mills et al., in press). Elevated levels of alcohol-related problems in this group are likely related to both of these factors, but several distinct mechanisms could explain why. In the present study, we disentangle these explanations.
Method
Sample and Data Collection
The border study (2009–2010) sampled Mexican Americans living along the entire U.S.-Mexico border (N=1,307) and the non-border sample consisted of Mexican Americans living in non-border regions of the U.S. interviewed in the 2006 Hispanic Americans Baseline Alcohol Survey (HABLAS), a study of 5,224 Hispanics (N=1,288 Mexican Americans). Border respondents were interviewed in California (Imperial County: N=365), Arizona (Cochise, Santa Cruz, and Yuma Counties: N=173), New Mexico (Dona Ana County: N=65), and Texas (Cameron, El Paso, Hidalgo and Webb Counties: N=704). Mexican American respondents off the border (HABLAS) were interviewed in Los Angeles (N=609), Houston (N=513), New York (N=86), Philadelphia (N=59), and Miami (N=21).
Each study sampled the adult population aged 18 or over and employed virtually identical multi-stage cluster sampling methodologies and survey instruments (for additional details, see Caetano et al., 2008; Mills et al., in press). Trained bilingual interviewers conducted Computer Assisted Personal Interviews (CAPI) at respondents’ home lasting about 1 hour. All respondents received a $25 incentive for participation and provided written informed consent. Weighted response rates for the border and non-border samples were 67% and 76%, respectively. Current analyses are restricted to current drinkers (one drink in the past 12 months; N=1,351). Both studies were approved by the Committee for the Protection of Human Subjects of the University of Texas Houston Health Science Center.
Measures
Border youth
Location and age were included in all models. Location was coded as border residence (1) versus non-border residence (0). For age, ongoing analyses of this data have shown that age trends in alcohol outcomes are driven largely by younger age groups, whereas older age groups (30–39, 40–49, and 50+) are generally comparable. To capture this nonlinearity, age was modeled as a dichotomy contrasting 18–29 year olds (1) with adults aged 30 or older (0).
In predicting bar attendance, drinking, and acute alcohol problems, the estimate of the interaction between border and age variables quantifies the difference in the magnitude of the border effect on the outcome between young and older adults (or equivalently, the difference in the age effect between border residents and non-border residents). With the specific coding of location and age described above, the product of these two variables takes on a value of one for young border residents and zero for all other groups (young non-border, older border, and older non-border residents). Consequently, the border by age interaction term (“border youth” in the Figures and Tables) corresponds to an adjusted linear contrast of young border residents with an average of the other three groups (i.e., those who are not young border residents)
Frequency of attending (and drinking) at bars
The number of days in the past year on which the respondent went to a bar and drank was computed from items covering the frequency and likelihood of drinking alcohol at “bars, clubs, taverns, or cocktail lounges.” The items were part of a larger subset of questions concerning common contexts of alcohol use (which additionally covered activities such as attending a restaurant, spending a quiet evening home alone, and going to a party at a friend’s house). For each context, respondents indicated how often (in the past year) they engaged in the activity with responses “never,” “sometimes, but less than once a month,” “one or two times a month,” “three or four times a month,” and “once a week or more.” Next, they indicated how often they drank alcohol on those occasions with responses “never,” “less than half the time,” “about half the time,” “more than half the time,” or “almost all of the time.” After assigning numeric values to the responses (using midpoints of referenced ranges) their product was computed (analogous to the graduated frequency method of computing annual volumetric intake – see below) to obtain a measure of how many times the respondent drank alcohol in those contexts over the past year. Due to positive skew, this variable was log-transformed for analyses. Raw means and 95% CIs were: border 18–29 year olds, x̄= 11.6, [8.1 – 15.2]; non-border 18–29 year olds, x̄= 6.5, [4.2 – 8.7]; border 30+ year olds, x̄= 3.9, [1.9 – 5.9]; and non-border 30+ year olds, x̄= 4.1, [2.4 – 5.7].
Drinking
Five variables covering drinking in the past year were used as indicators of a composite latent drinking variable: binge frequency (four/five standard drinks over a two hour period for women/men, respectively); volume consumed (using the “graduated frequencies” method; Clark and Hilton, 1991, Greenfield and Kerr, 2008); heavy drinking frequency (consuming four/five standard drinks in a single day for women/men; this correlated moderately with binge frequency, r = .35); maximum number of drinks consumed on any single day; and whether the respondent “stayed intoxicated for several days at a time” during the past year (dichotomous). Due to substantial positive skew, the first four continuous variables were log-transformed. Previous factor analyses of these items have shown a clear unidimensional structure (dominant first eigenvalue, highly correlated/redundant factors in obliquely rotated multidimensional solutions, and a well fitting unidimensional model: RMSEA=.034, CFI=.99, TLI=.97).
Acute problems of intoxication
We focused specifically on problems that can (and often do) correspond to a specific episode of acute ethanol intoxication, as these are the types of problems directly affected by bar environments (Graham et al., 2006a, 2006b, Homel et al., 1992). The guiding criterion was that a single, acute state of ethanol intoxication be sufficient to cause a corresponding instance of the problem (in contrast to most problems related to dependence, where a specific episode of intoxication is neither a necessary nor sufficient precondition of problem occurrence). Respondents were asked whether they experienced ten such problems in the past year (including alcohol-related belligerence, job problems, problems involving the police, accidents, problems with spouse or with others, recurrent drinking under hazardous circumstances, despite legal or social/interpersonal consequences, or despite interference with major roles and obligations). These 10 binary items were used as indicators of a latent acute alcohol problem variable. As with the latent drinking variable, factor analyses strongly suggested a unidimensional structure (dominant first eigenvalue, highly correlated factors in multidimensional solutions, and a well fitting unidimensional model: RMSEA=.024, CFI=.98, TLI=.98; factor loadings ranged from .34 to .91, with 8 of 10 exceeding .70).
Other variables
Sociodemographics
In addition to age and border residence status, these included gender, employment and marital status, education, and income.
Social cognitions
These previously validated one-dimensional measures (Mills et al., 2012a, Mills and Caetano, 2010, 2012) include drinking norms (nine items covering levels of drinking considered acceptable in various circumstances; e.g., “with friends at home”; Cronbach’s α = .85), alcohol-expectancies of emotional fluidity (four items; e.g., the extent to which alcohol makes you “become more friendly”; α = .80) and emotional/behavioral impairment (e.g., “become more aggressive” or “lose coordination”; five items; α = .90), positive alcohol attitudes (eight items; e.g., “Having a drink is one of the pleasures of life,”; α = .76), negative alcohol attitudes (four items; e.g., “Drinking brings out the worst in people”; α = .59), and motives for drinking (nine items; e.g., “helps forget about my worries” and “a good way to celebrate”; α = .84).
Neighborhood characteristics
Also used previously (Mills et al., 2012b, in press), three five-item measures assessed perceived aspects of respondents’ neighborhoods: social cohesion and control (α = .72 and .78, respectively), and perceived neighborhood violence (α = .81), all adapted from Sampson et al. (1997).
Data Analyses
All analyses accounted for the complex sampling design of the studies and were conducted on weighted data that adjusts the sample to known Hispanic population distributions. Loadings on dichotomous latent variable indicators were modeled using probit link functions. Paths of interest shown in Figure 1 were estimated with Mplus 7.11 (Muthén & Muthén, 2013) as a structural equation model. Indirect effects from the border youth term to the acute problem variable were estimated using resampling (bootstrapping) methods and bias-corrected 95% confidence intervals within Fairchild & MacKinnon’s (2009) general framework for testing mediated-moderation hypotheses (see also MacKinnon et al., 2004).
Following preliminary interaction tests, non-significant interactions were dropped and the model was refitted to arrive at a baseline mediation model. Estimates from this model – which adjusted for both bar attendance and drinking – were compared with a) estimates adjusted only for bar attendance and b) estimates adjusted for neither. Next, path decomposition was performed on estimates from the baseline mediation model to quantify four possible indirect effects on acute problems (Figure 1). Finally, we re-estimated this model adjusting for sociodemographic (block 1) and social-cognitive/neighborhood effects (block 2) on endogenous variables, repeated the path decomposition, and compared the impact on indirect effects with previous models.
Results
Preliminary Models
We first tested several moderating influences on paths shown in Figure 1 to ensure that effects of bar attendance on drinking and problems did not vary across age or border residence. These interactions did not reach significance. Specifically, border residence did not moderate the bar attendance effect on drinking (b = −.07, SE = .06, p = .25) or problems (b = .07, SE = .08, p = .41). Likewise young age did not moderate the bar attendance effect on drinking (b = −.07, SE = .06, p = .29) or problems (b = −.02, SE = .09, p = .82). Consequently, these terms were dropped and the model was refitted to arrive at the baseline mediation model discussed next.
Impact of Bar Attendance and Drinking
Figure 2 illustrates three key points: 1) Age and location differences in acute problem severity reflect an interactive pattern, 2) adjustment for bar attendance and drinking eliminate this pattern, and 3) the interaction’s disappearance is due entirely to change in the estimate for border youth. Adjustment for the more distal bar attendance variable alone had a notable impact on the interactive pattern, which completely disappeared following additional adjustment for drinking. Change across the three graphs was driven by shifts in the estimate for young border residents, whose estimated severity decreased by roughly one-half of a standard deviation. In contrast, the basic configuration and magnitude of effects across the other three groups remained largely unchanged.
Figure 2.
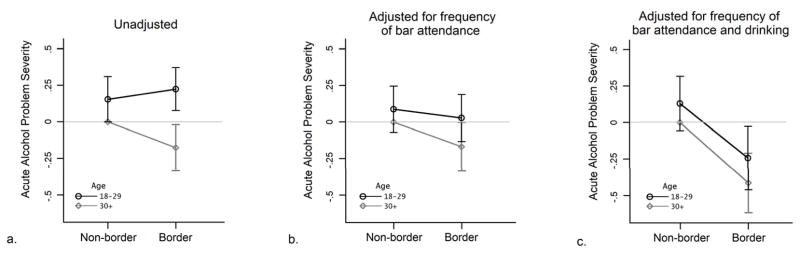
Unadjusted and adjusted differences in mean acute problem severity by location and age. Error bars show standard errors. Unadjusted estimates (a) were derived from the simple regression of acute alcohol problem severity on location, age, and their interaction. Means in the middle graph (b) were derived from models that additionally adjusted for the effect of bar attendance on acute alcohol problem severity. The final graph (c) shows means implied by the baseline mediation model, which adjusted for effects of both bar attendance and drinking on acute alcohol problem severity. In the unadjusted model, border young adults reported significantly higher acute alcohol problem severity than older border residents (b = .41, SE=.18, p<.05); other comparisons were nonsignificant. Acute alcohol problems is a latent variable scaled in a standard deviation metric, where the reference group (non-border residents aged 30+) intercept/mean is defined as zero.
Parameter estimates from the baseline mediation model are shown in Table 1. As expected, border youth predicted higher frequency of bar attendance, which in turn predicted higher levels of drinking. Not unexpectedly, drinking was a positive predictor of acute alcohol problems. Border youth did not predict drinking independently of bar attendance, and a higher frequency of bar attendance also did not predict acute problems independently of drinking. Additionally, border youth did not predict problems independently of both drinking and bar attendance. The path decomposition of these estimates (bottom of Table 1) showed that of four ways that being young and living on the border might be linked to higher levels of acute alcohol problems, only the common pathway involving bar attendance and drinking was significant.
Table 1.
Structural parameter estimates and path decompositions of mediation models.
| Baseline Mediation Model
|
+ Sociodemographic Adjustment
|
|||
|---|---|---|---|---|
| Outcome and Predictors | Estimate (SE) | p | Estimate (SE) | p |
|
|
|
|||
| Frequency of Bar Attendance | ||||
| Border Residence | −.04 (.12) | .729 | .03 (.09) | .749 |
| Young Age (18–29) | .35 (.11) | .002 | .15 (.09) | .110 |
| Border Youth (Border Residence X Young Age) | .55 (.20) | .006 | .56 (.15) | < .001 |
| R2 | .08 | .16 | ||
| Severity of Drinking | ||||
| Frequency of Bar Attendance | .40 (.04) | < .001 | .43 (.03) | < .001 |
| Border Residence | .14 (.10) | .171 | .25 (.11) | .024 |
| Young Age (18–29) | −.01 (.11) | .948 | −.01 (.10) | .930 |
| Border Youth (Border Residence X Young Age) | .14 (.17) | .410 | .15 (.16) | .362 |
| R2 | .22 | .37 | ||
| Severity of Acute Problems | ||||
| Severity of Drinking | 1.09 (.10) | < .001 | .96 (.08) | < .001 |
| Frequency of Bar Attendance | −.07 (.06) | .214 | −.06 (.05) | .242 |
| Border Residence | −.40 (.22) | .073 | −.43(.19) | .023 |
| Young Age (18–29) | .14 (.19) | .437 | .03 (.16) | .859 |
| Border Youth (Border Residence X Young Age) | .03 (.33) | .932 | .02 (.27) | .933 |
| R2 | .59 | .61 | ||
| Path Decomposition | Estimate p | 95% CI | Estimate p | 95% CI |
|---|---|---|---|---|
| Border Youth → Bar Freq. → Drinking → Acute Problems | .24 (.10) | .011 [.06–.42] | 23 (.07) | .001 [.09–.42] |
| Border Youth → Bar Freq. → Acute Problems | −.04 (.04) | .268 [−.13–.01] | −.04 (.03) | .254 [−.13–.02] |
| Border Youth → Drinking → |
Sensitivity of Results to Adjustment for Confounding Influences
Estimates from models that additionally adjusted for confounding influences of five sociodemographic and nine neighborhood/social-cognitive variables on endogenous model variables are shown in the second and third (super) columns of Table 1. Beginning with the path decomposition, the common indirect pathway was surprisingly robust to adjustment for these 14 other influences, remaining significant across both blocks of adjustment. Comparing their impact, control for the nine social-cognitive/neighborhood variables seemed to have a larger influence on the common indirect effect than control for sociodemographics. Among the components of the effect (i.e., of border youth on bar attendance, of bar attendance on drinking, and of drinking on problems; upper part of Table 1), the largest change was seen for the effect of bar attendance on drinking (−28%, from .40 to .29), while the border youth effect on bar attendance was affected the least. Importantly, note that across the two blocks of adjustment, all three components of this pathway remained significant, and moreover, there were no differences in effect directions or significance patterns in the path decomposition. Consequently, inferences concerning the key mediation pathways of interest were not affected by confounder adjustment. Note also that although the magnitude of the significant indirect path does change (from .24 to .11), this does not seem surprising considering the number of possible confounders being controlled (output from the models, including all covariate effects, is available on request from the first author). Given that the adjustments had no impact on the mediation pathways of interest, and because our inferential objectives did not concern testing a broader structural model of relations between these other variables, we do not report an exploratory respecification of the model (we have estimated one however: after dropping covariate effects that were nonsignificant, there were no substantive changes in the pattern of results discussed presently; the direction and pattern of significance for all component paths in the path decomposition remained identical). A final point of interest is that the R2 increases in the adjusted models provide reassurance that the adjustments were not trivial and did in fact capture additional, unique variation in the three outcomes.
Discussion
The U.S.-Mexico border has been of interest to alcohol researchers because of the distinct alcohol policies on the two sides of the border, the presence of multiple risk factors for poor health (such as low income), and known elevations in alcohol use and associated problems among the region’s population. The present findings demonstrate that elevations in acute alcohol-related problems among Mexican American youth in the region are tightly connected to this group’s higher frequency of bar attendance and associated increases in drinking. With respect to previous findings showing travel to Mexico confers increased risk for alcohol use and associated problems (Caetano et al., 2013b; Lange et al., 2002, Voas et al., 2002; Lange& Voas, 2000), a crucial point here is that these elevations in risk do not seem to simply reflect a south-of-the-border phenomenon. Young adults north of the border are also attending bars, drinking, and exhibiting alcohol problems at unusually high levels, regardless of whether they traveled to Mexico to drink1. This is an important point in light of previous findings linking high rates of problems to drinking in Mexico bars. While risky drinking in Mexico is a clear problem, U.S. policymakers need to be aware that 1) there are also elevations in alcohol-related problems among young adults in the general U.S. border population and 2) this disparity can be explained by factors within U.S. borders and under their direct control.
Another interesting aspect of the present findings was how robust the common indirect pathway and its component effects were to adjustment for other possible explanations. We remained deliberately agnostic regarding how 14 different confounding effects influence the three variables of theoretical interest (bar attendance, drinking, and problems). That is, rather than placing theoretical constraints on these influences (e.g., assuming some paths were zero), reported models controlled for all 14 influences on endogenous variables simultaneously. This is a particularly stringent adjustment for confounding. For example, in the bold pathway in Figure 1 in the fully adjusted model, P1 estimates the impact of border youth on bar attendance, partialling out 14 potentially confounded sociodemographic, social-cognitive, and neighborhood sources of variation in bar attendance. P2 estimates the impact of bar attendance on drinking partialling out the same 14 sources of variation in drinking, and P3 estimates drinking’s effect on acute problems, again controlling for these 14 distinct possible effects on acute problems. Consequently, this indirect effect quantifies variation in acute problem severity that a) is specifically attributable to variance these three antecedents (border youth, bar attendance, and drinking) have in common, and b) is independent of 42 different confounded explanations (not counting other pathways in figure 1 or border/age “main effect” terms). Some caution is of course warranted here given the cross-sectional nature of the data, yet its independence from such a broad range of alternative explanations strongly warrants further attention. Bar attendance may represent an early modifiable risk factor that plays a key and perhaps critical role in the high levels of alcohol problems among the border’s young adult Mexican American population.
Contrary to one of our hypotheses, bar attendance did not affect acute problem severity independently of drinking. In evaluating this finding, it is important to keep our original objectives in mind. Those objectives concerned testing hypotheses about what explains disparities in drinking among Mexican Americans on and off the border, not about how (or whether) bar environments uniquely influence alcohol problems. Support for the latter type of hypothesis has been found in studies employing a multilevel approach that accommodates variation in environmental characteristics and drinking levels across both bars and patrons (e.g., Graham et al., 2006a, 2006b). The present findings do not speak to these types of questions, and instead simply indicate that on average, there is no evidence that attending bars more frequently increases risk for acute alcohol problems independently of drinking.
Another unanticipated aspect of the present findings emerged in the specific configuration problem severity estimates take following adjustment for hypothesized mediators. As can be seen in Figure 2c, once bar attendance and drinking are taken into account, the lines not only become parallel: Both data points for the border wind up notably lower than the two non-border data points. Although a “main” effect of border residence is not parameterized in the models of Table 1 (all were interaction models), the “border” term closely approximates one, (given that the interaction’s direct influence on problems was effectively zero across all adjustment blocks). That effect was large across all models and significant when adjusting for other covariates. Taken together, these considerations lead to two tentative inferences about the specific elevation in alcohol-related risks seen among younger border residents: 1) it can be largely accounted for by this group’s high frequency of bar attendance and amount of drinking, but also 2) the resulting elevation may be masking a more general protective influence of border residence applicable to all ages. Generally speaking, a factor as distal as geographic residence likely affects specific individual health outcomes via the cumulative impact of many underlying mechanisms, some acting in concert, and others as opponent-processes that counter-act one another’s influence.
The present findings indicate that pathways involving bar attendance and drinking may be salient enough to substantively attenuate marginal estimates of alcohol-related disparities between border and non-border groups, particularly for samples varying widely in age. The present findings should also be considered in light of several strengths and limitations. Strengths included use of representative samples of Mexican Americans on and off the border and sampling from the entire U.S.-Mexico border (previous studies have typically sampled from isolated regions of the border). By comparing homogeneous, representative samples of Mexican Americans on and off the border, possible influences of national culture on estimates of drinking, problems, and associated variables are controlled. This constrains the present findings’ generalization to other ethnic/national border groups. The cross-sectional nature of the data also limits causal inference, and it is possible that use of different measures (particularly related to social-cognition), may result in different findings. Finally, latent representations of drinking and acute problems are less sensitive to noise inherent in individual items, and consequently, associations with other variables are less likely to be artificially attenuated by measurement error (for a similar approach, see Mulia et al., 2008). However, this applies only to what these measures’ items have in common; the findings would not necessarily generalize to any specific problem or drinking index.
In conclusion, more frequent bar attendance explains higher rates of drinking and associated acute alcohol problems among border young adults, and these relationships cannot be entirely attributed to border residence, respondents’ sociodemographic characteristics, neighborhood characteristics, or social-cognitive predictors of alcohol use. These heightened levels of bar attendance, drinking, and problems among border youth may reflect a protracted consequence of the longstanding differences in alcohol policy on the two sides of the border. Within this general environmental context of alcohol use, a sharp geographic policy gradient creates transient incentives that one targeted age group (those under 21) exploits over a period that, although brief, may be long enough to have a broader impact on the U.S. side. Risky drinking in Mexico of course does not occur in a vacuum, and U.S. residents who cross into Mexico to drink return (usually within 24 hours) to a broader social, behavioral, and temporal context on the U.S. side (Lange et al., 2002). Upon returning and interacting with their broader peer network, crossers’ previous experience with drinking in Mexico likely has some impact on where drinking happens on subsequent occasions in the U.S. Similarly, patterns of behavior – such as where one drinks – molded during formative drinking years (travelling to Mexico to drink is most likely prior to 21; Caetano et al., 2013b) are unlikely to suddenly disappear at an arbitrary age threshold of 21. Instead, they are likely to manifest in other ways throughout young adulthood, such as drinking in bars on the U.S. side.
Acknowledgments
Preparation of this article was supported by grants (RO1-AA013642 and RO1-AA016827) from the National Institute on Alcohol Abuse and Alcoholism to the University of Texas School of Public Health.
Contributor Information
Britain A. Mills, University of Texas School of Public Health – Dallas, TX.
Raul Caetano, Prevention Research Center, Pacific Institute for Research and Evaluation, Oakland, CA.
Patrice A.C. Vaeth, Prevention Research Center, Pacific Institute for Research and Evaluation, Oakland, CA.
Jennifer M. Reingle Gonzalez, University of Texas School of Public Health – Dallas, TX.
References
- Berke EK, Tanski SE, Demidenko E, Alford-Teaster J, Shi X, Sargent JD. Alcohol retail density and demographic predictors of health disparities: a geographic analysis. American Journal of Public Health. 2009;100:1967–1971. doi: 10.2105/AJPH.2009.170464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caetano RC, Mills BA, Vaeth PAC. Alcohol consumption and binge drinking among U.S.–Mexico border and non-border Mexican Americans. Alcoholism: Clinical and Experimental Research. 2012;36:677–685. doi: 10.1111/j.1530-0277.2011.01652.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caetano R, Ramisetty-Mikler S, Rodriguez LA. The Hispanic Americans Baseline Alcohol Survey (HABLAS): Rates and predictors of alcohol abuse and dependence across Hispanic national groups. Journal of Studies on Alcohol and Drugs. 2008;69(3):441–448. doi: 10.15288/jsad.2008.69.441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caetano R, Vaeth PAC, Mills BA, Rodriguez LA. Alcohol abuse and dependence among U.S.-Mexico border and non-border Mexican Americans. Alcohol Clin Exp Res. 2013a;37:847–853. doi: 10.1111/acer.12061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caetano RC, Mills BA, Vaeth PAC. Alcohol use among Mexican American U.S.–Mexico border residents: Differences between those who drink and who do not drink in Mexico. Addict Behav. 2013b;38:2026–2031. doi: 10.1016/j.addbeh.2013.01.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clark WB, Hilton M. Alcohol in America: Drinking practices and problems. Albany, NY: State University of New York Press; 1991. [Google Scholar]
- Fairchild AJ, MacKinnon DP. A general model for testing mediation and moderation effects. Prevention Science. 2009;10:87–99. doi: 10.1007/s11121-008-0109-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fairchild AJ, MacKinnon DP. A general model for testing mediation and moderation effects. Prevention Science. 2009;10:87–99. doi: 10.1007/s11121-008-0109-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Graham K, Bernards S, Osgood DW, Wells S. Bad nights or bad bars? Multilevel analysis of environmental predictors of aggression in late-night large-capacity bars and clubs. Addiction. 2006a;101:1569–1580. doi: 10.1111/j.1360-0443.2006.01608.x. [DOI] [PubMed] [Google Scholar]
- Graham K, Osgood DW, Wells S, Stockwell T. To what extent is intoxication associated with aggression in bars? A multilevel analysis. Journal of Studies on Alcohol and Drugs. 2006b;67:382–390. doi: 10.15288/jsa.2006.67.382. [DOI] [PubMed] [Google Scholar]
- Greenfield TK, Kerr WC. Alcohol measurement methodology in Epidemiology: Recent advances and opportunities. Addiction. 2008;103:1082–1100. doi: 10.1111/j.1360-0443.2008.02197.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hill TD, Angel RJ. Neighborhood disorder, psychological distress, and heavy drinking. Social Science & Medicine. 2005;61:965–975. doi: 10.1016/j.socscimed.2004.12.027. [DOI] [PubMed] [Google Scholar]
- Homel R, Tomsen S, Thommeny J. Public drinking and violence: not just an alcohol problem. Journal of Drug Issues. 1992;22:679–97. [Google Scholar]
- Lange JE, Voas RB. Youth escaping limits on drinking: Bingeing in Mexico. Addiction. 2000;95:521–528. doi: 10.1046/j.1360-0443.2000.9545214.x. [DOI] [PubMed] [Google Scholar]
- Lange JE, Voas RB, Johnson MB. South of the border: A legal haven for underage drinking. Addiction. 2002;97:1195–1203. doi: 10.1046/j.1360-0443.2002.00182.x. [DOI] [PubMed] [Google Scholar]
- MacKinnon DP, Lockwood CM, Williams J. Confidence Limits for the Indirect Effect: Distribution of the Product and Resampling Methods. Multivariate Behavioral Research. 2004;39:99–128. doi: 10.1207/s15327906mbr3901_4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mills BA, Caetano RC. The Hispanic Americans Baseline Alcohol Survey (HABLAS): Predictors of alcohol attitudes and expectancies in Hispanic national groups. Alcohol Clin Exp Res. 2010;34:1–10. doi: 10.1111/j.1530-0277.2010.01151.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mills BA, Caetano RC. Decomposing associations between acculturation and drinking in Mexican Americans. Alcohol Clin Exp Res. 2012;36:1205–1211. doi: 10.1111/j.1530-0277.2011.01712.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mills BA, Caetano RC, Ramisetty-Mikler S, Bernstein IH. The dimensionality and measurement properties of alcohol outcome expectancies across Hispanic national groups. Addict Behav. 2012a;37:327–330. doi: 10.1016/j.addbeh.2011.10.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mills BA, Caetano RC, Vaeth PAC. What explains higher levels of drinking among Mexican Americans on the U.S-Mexico border? Alcohol Clin Exp Res. 2012b;36:258. [Google Scholar]
- Mills BA, Caetano R, Vaeth PAC. Cross-border policy effects on alcohol outcomes: drinking without thinking on the U.S.-Mexico border? Alcohol Clin Exp Res. doi: 10.1111/acer.12548. (in press) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mulia N, Schmidt L, Bond J, Jacobs L, Korcha R. Stress, social support, and problem drinking among women in poverty. Addiction. 2008;103:1283–1293. doi: 10.1111/j.1360-0443.2008.02234.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus User's Guide. 7. Los Angeles, CA: Muthén & Muthén; 1998–2013. [Google Scholar]
- Romley JA, Cohen D, Ringel J, Strum R. Alcohol and environmental justice: the density of liquor stores and bars in urban neighborhoods in the United States. Journal of Studies on Alcohol and Drugs. 2007;68:48–55. doi: 10.15288/jsad.2007.68.48. [DOI] [PubMed] [Google Scholar]
- Sampson RJ, Raudenbush SW, Earls F. Neighborhoods and violent crime: A multilevel study of collective efficacy. Science. 1997;277:918–924. doi: 10.1126/science.277.5328.918. [DOI] [PubMed] [Google Scholar]
- Vaeth PAC, Caetano RC, Mills BA. Alcohol-related social problems among Mexican Americans living in U.S.–Mexico border and non-border areas. Addictive Behaviors. 2012;37:998–1001. doi: 10.1016/j.addbeh.2012.04.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Voas RB, Lange JE, Johnson MB. Reducing high-risk drinking by young Americans south of the border: The impact of a partial sales ban on sales of alcohol. Journal of Studies on Alcohol. 2002;63:286–292. doi: 10.15288/jsa.2002.63.286. [DOI] [PubMed] [Google Scholar]