

Abstract
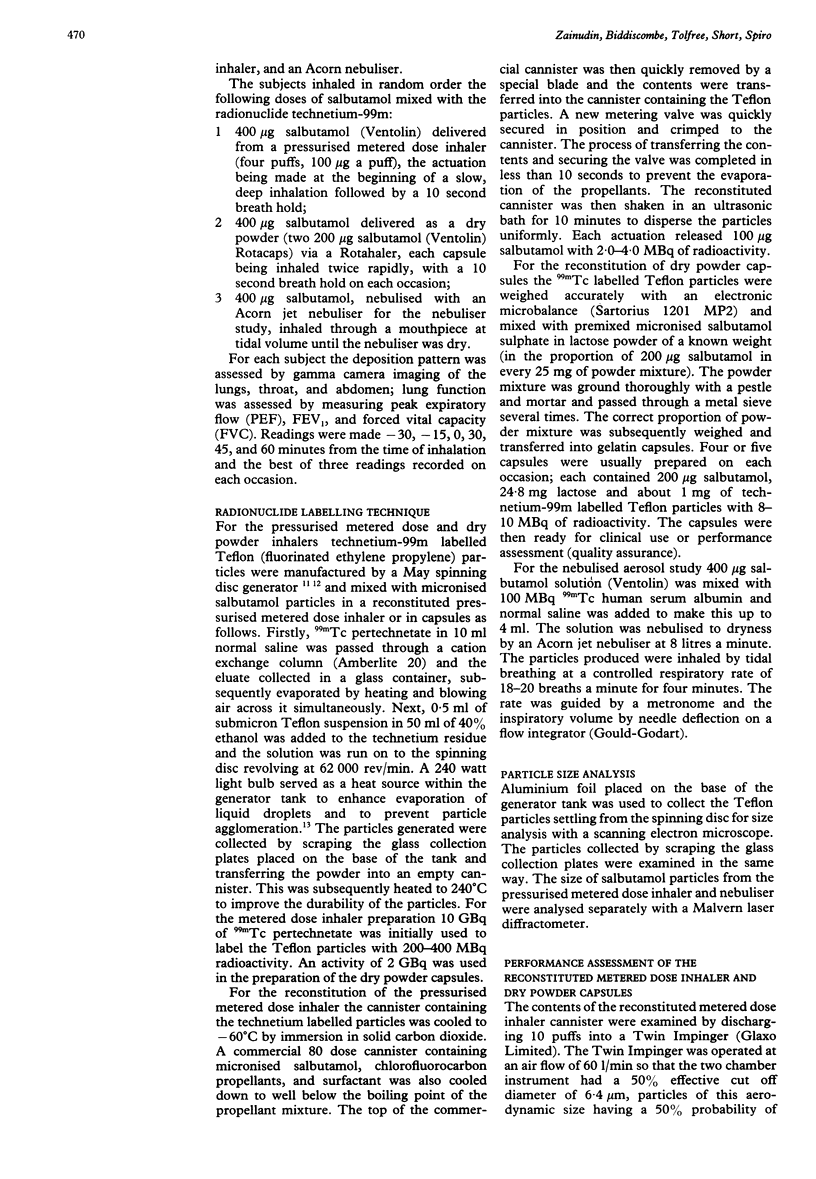
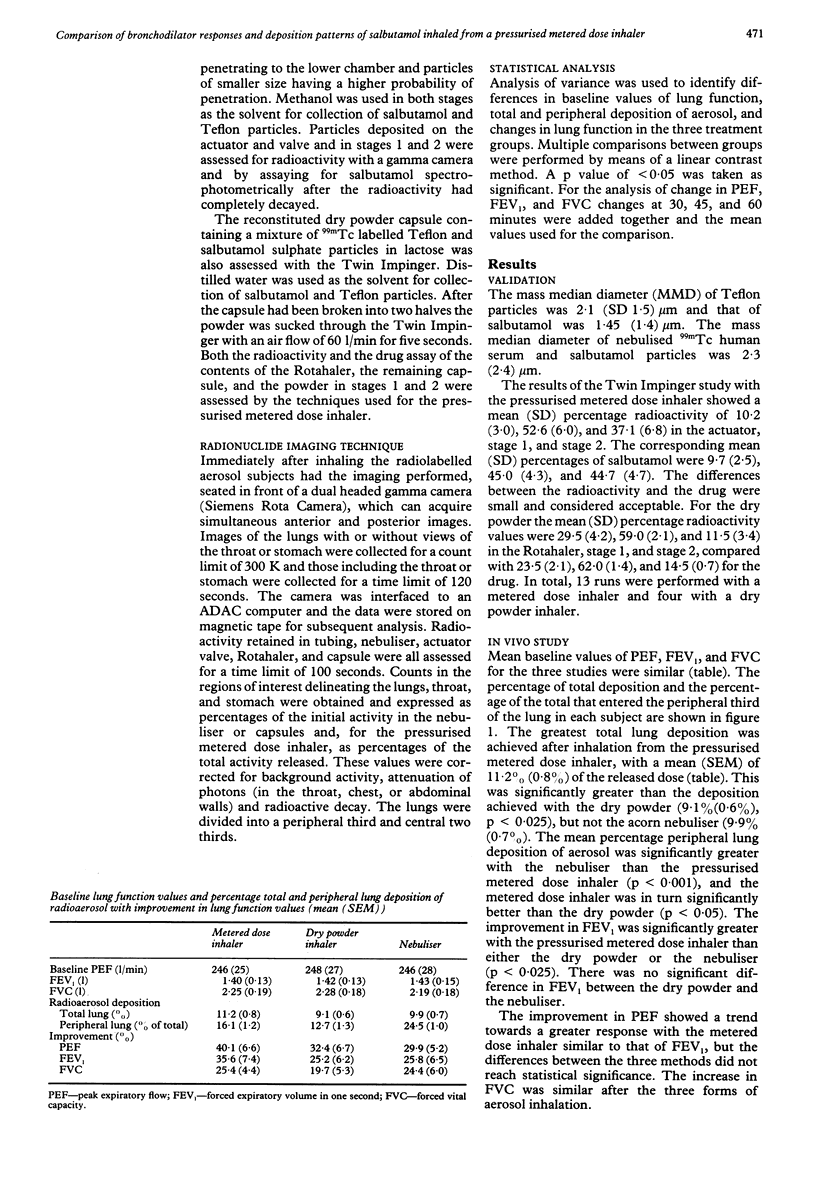
The lung dose and deposition patterns of drug delivered by dry powder inhaler are not known. The effects of inhaling 400 micrograms salbutamol delivered by dry powder inhaler (two 200 micrograms salbutamol Rotacaps), by pressurised metered dose inhaler, and by Acorn nebuliser were studied in nine subjects with chronic stable asthma. Technetium-99m labelled Teflon particles were mixed with micronised salbutamol in the pressurised metered dose inhaler and in the capsules; technetium-99m labelled human serum albumin was mixed with the salbutamol solution for the nebuliser study. The pressurised metered dose inhaler deposited 11.2% (SEM 0.8%) of the dose within the lungs; this was significantly more than the dose deposited by the dry powder inhaler (9.1% (0.6%], but did not differ significantly from the dose delivered by the nebuliser (9.9% (0.7%]. Distribution within the peripheral third of the lung was significantly greater with the nebuliser than with the other two systems; FEV1 improved to a significantly greater extent after inhalation of 400 micrograms salbutamol from the pressurised metered dose inhaler (35.6% from baseline) than from the nebuliser (25.8%) or dry powder inhaler (25.2%). Thus after inhalation of similar doses of salbutamol a larger proportion of drug was deposited within the lungs when it was inhaled from a metered dose inhaler than from a dry powder system; the nebuliser achieved the greatest peripheral deposition. The bronchodilator response seems to depend on the amount of drug within the lungs rather than its pattern of distribution.
Full text
PDF

Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Camner P., Philipson K., Svedberg J. Production of 7 mu monodisperse fluorocarbon resin particles tagged with 18F. Int J Appl Radiat Isot. 1971 Jun;22(6):349–353. doi: 10.1016/0020-708x(71)90061-5. [DOI] [PubMed] [Google Scholar]
- Chambers S., Dunbar J., Taylor B. Inhaled powder compared with aerosol administration of fenoterol in asthmatic children. Arch Dis Child. 1980 Jan;55(1):73–74. doi: 10.1136/adc.55.1.73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crompton G. K. Problems patients have using pressurized aerosol inhalers. Eur J Respir Dis Suppl. 1982;119:101–104. [PubMed] [Google Scholar]
- Davies D. S. Pharmacokinetics of inhaled substances. Postgrad Med J. 1975;51(7 Suppl):69–75. [PubMed] [Google Scholar]
- Epstein S. W., Manning C. P., Ashley M. J., Corey P. N. Survey of the clinical use of pressurized aerosol inhalers. Can Med Assoc J. 1979 Apr 7;120(7):813–816. [PMC free article] [PubMed] [Google Scholar]
- Hartley J. P., Nogrady S. G., Seaton A. Long-term comparison of salbutamol powder with salbutamol aerosol in asthmatic out-patients. Br J Dis Chest. 1979 Jul;73(3):271–276. [PubMed] [Google Scholar]
- Hetzel M. R., Clark T. J. Comparison of salbutamol Rotahaler with conventional pressurized aerosol. Clin Allergy. 1977 Nov;7(6):563–568. doi: 10.1111/j.1365-2222.1977.tb01486.x. [DOI] [PubMed] [Google Scholar]
- Newman S. P., Pavia D., Garland N., Clarke S. W. Effects of various inhalation modes on the deposition of radioactive pressurized aerosols. Eur J Respir Dis Suppl. 1982;119:57–65. [PubMed] [Google Scholar]
- Newman S. P., Pavia D., Morén F., Sheahan N. F., Clarke S. W. Deposition of pressurised aerosols in the human respiratory tract. Thorax. 1981 Jan;36(1):52–55. doi: 10.1136/thx.36.1.52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paterson I. C., Crompton G. K. Use of pressurised aerosols by asthmatic patients. Br Med J. 1976 Jan 10;1(6001):76–77. doi: 10.1136/bmj.1.6001.76-a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rodenstein D., Stănescu D. C. Mouth spraying versus inhalation of fenoterol aerosol in healthy subjects and asthmatic patients. Br J Dis Chest. 1982 Oct;76(4):365–373. doi: 10.1016/0007-0971(82)90072-9. [DOI] [PubMed] [Google Scholar]
- Shore S. C., Weinberg E. G., Dürr M. H. Buccal administration of fenoterol aerosol in young children with asthma. S Afr Med J. 1976 Aug 14;50(35):1362–1364. [PubMed] [Google Scholar]
- Spiro S. G., Singh C. A., Tolfree S. E., Partridge M. R., Short M. D. Direct labelling of ipratropium bromide aerosol and its deposition pattern in normal subjects and patients with chronic bronchitis. Thorax. 1984 Jun;39(6):432–435. doi: 10.1136/thx.39.6.432. [DOI] [PMC free article] [PubMed] [Google Scholar]