

Abstract
Background and purpose
We report the radiographic response rate of SBRT compared to conventional fractionated radiotherapy (CF-EBRT) for thoracic, abdominal, skin and soft tissue RCC lesions treated at our institution.
Material and methods
Fifty three lesions where included in the study (36 SBRT, 17 CF-EBRT), treated from 2004 to 2014 at our institution. We included patients that had thoracic, skin & soft tissue (SST), and abdominal metastases of histologically confirmed RCC. The most common SBRT fractionation was 50 Gy in 5 fractions.
Results
The median time of follow-up was 16 months (range 3–97 months). Median BED was 216.67 (range 66.67–460.0) for SBRT, and 60 (range 46.67–100.83) for CF-EBRT. Median radiographic local control rates at 12, 24, and 36 months were 100, 93.41, and 93.41 % for lesions treated with SBRT versus 62.02, 35.27 and 35.27 % for those treated with CF-EBRT (p < 0.001). Predictive factors for radiographic local control under univariate analysis included BED ≥ 100 Gy (HR, 0.048; 95 % CI, 0.006–0.382; p = 0.005), dose per fraction ≥ 9 Gy (HR, 0.631; 95 % CI, 0.429–0.931; p = 0.021), and gender (HR, 0.254; 95 % CI, 0.066–0.978; p = 0.048). Under multivariate analysis, there were no significant predictors for local control. Toxicity rates were low and equivalent in both groups, with no grade 4 or 5 side effects reported.
Conclusions
SBRT is safe and effective for the treatment of RCC metastases to thoracic, abdominal and integumentary soft tissues. Radiographic response rates were greater and more durable using SBRT compared to CF-EBRT. Further prospective trials are needed to evaluate efficacy and safety of SBRT for RCC metastases.
Keywords: Renal cell carcinoma, Local control, SBRT, Conventional fractionation
Background
The global annual incidence of renal cell carcinoma (RCC) is nearly 209,000 cases, killing over 100,000 people each year [5]. The majority of these patients present with isolated disease, however, about 30 % of these patients recur after treatment either locally or, more frequently, distantly and about the same percentage present with metastatic spread at the time of diagnosis [18]. In the setting of metastatic disease, RCC most commonly spreads to the lung, accounting for approximately 60 % of metastatic cases. Hepatic involvement occurs in about 20 % of cases. Prognosis is generally favorable for patients with non-metastatic disease however the two-year survival in patients with widespread disease is much worse (10–20 %) [18].
As patients with RCC continue to live longer given the rapid advances seen in systemic treatment for RCC with targeted agents (eg, tyrosine kinase inhibitors (TKIs), vascular endothelial growth factor (VEGF) inhibitors, and mTOR inhibitors), localized treatment of enlarging or anatomically problematic masses is becoming increasingly utilized to further lengthen and improve quality of life [4, 6, 11]. In patients with oligo-metastatic disease, surgical resection has been employed with promising results. For instance, Loizzi et al. demonstrated improved overall survival, four-year survival of 50 %, after surgically resecting easily accessible RCC lung lesions [9].
In addition to surgical therapy, traditionally fractionated radiotherapy has been used to treat metastatic disease despite the traditional thinking of RCC being “radioresistant”. However, over the past decade, increased use of hypofractionation with stereotactic body radiotherapy (SBRT) has allowed clinicians to accurately target lesions and deliver more ablative doses. Efficacy of SBRT has been demonstrated in multiple metastatic sites, with local control rates above 90 % [13, 17, 18]. Bextracranial stereotactic radiotherapyextracranial stereotactic radiotherapysingle-institution studies demonstrating high local control rates using SBRT, we sought to directly compare the radiographic outcomes of RCC lesions between traditional or conventional fractionation (CF-EBRT) and SBRT in our institution to enhance the dataset analyzing the radiosensitivity of RCC. Additionally, the goal of this study was to further define the most effective radiation delivery by estimating a minimum dose, either fraction size or biologic effective dose (BED) cutoff, needed to achieve long term local control.
Materials and methods
Patients were retrospectively identified by searching an institutional database of patients treated with radiation for RCC at the University of Colorado Cancer Center between December 2005 and May 2014. This study was approved by the University of Colorado Institutional Review Board. We included patients that had pathological confirmation of primary RCC and radiographic evidence of metastatic lesions. All patients included had a minimum follow up of 3 months post radiation therapy. Sites of metastasis were grouped into thorax, skin & soft tissue (SST), and abdomen.
Patients were treated with SBRT using intensity modulated radiotherapy (IMRT) planning. All patients treated with SBRT underwent treatment simulation prior. Simulation scans were CT based, with 3 mm slice thickness. In the more recent years, lesions with tumor motion underwent 4D imaging with abdominal compression. Patients were supine and immobilized with a vac-loc or alphacrade. IV contrast use was at the discretion of the treating physician. For treatment planning, the gross tumor volume (GTV) was considered equal to the clinical target volume (CTV). An internal target volume (ITV) was generated for lesions with motion who underwent 4D imaging, which was then expanded to the planned tumor volume (PTV). The PTV expansion depended on the treatment site and physician discretion. CF-EBRT were treated with simple 2D planning, 3D, and at times intensity modulated radiotherapy (IMRT) if there were nearby critical organs at risk nearing maximum dose tolerance. All SBRT cases underwent daily image guidance (IGRT) during treatment.
Patients were evaluated for radiographic response after treatment. Radiographic complete response was defined as: no evidence of disease in the treatment volume by interpretation of available Fludeoxyglucose-Positron emission tomography/computed tomography (FDG-PET/CT), Magnetic Resonance Imaging (MRI), or computed tomography (CT) scans 3 months after SBRT. Stable disease was defined as absence of marked change or increase in the treated lesion. Partial response was defined as not meeting the criteria for complete response or stable disease. Patients were labeled as radiographic responders if they had a complete response, partial response and/or stable disease after radiation. Treated metastasis control was defined as the time from the last day of radiation treatment to failure at the treated site or last follow-up in living patients without evidence of recurrence or progression. Use of the Response Evaluation Criteria in Solid Tumors (RECIST) was not used due to difficulty assessing parenchymal changes common after SBRT, especially to sites treated to 20 Gy or higher. Instead failure at the treated site was scored as lesions that experienced a complete, partial or stable response after therapy; all other lesions that had an increase in standardized uptake value (SUV) on PET or expansion of a solid mass compared to prior CT-based imaging. All scans were verified by a certified radiologist.
Univariate survival analysis was performed with the log-rank test, with Cox proportional hazards regression used to estimate hazard ratios (HR). Multivariate Cox regression analysis was performed to evaluate the association between clinical factors and LRC with a significance level of p < 0.05. The independent variables considered were total dose, number of fractions, dose per fraction, biologic effective dose (BED), site (thorax vs other), histology (clear cell vs other), GTV, PTV, gender, age, time from initial diagnoses to end of radiation therapy, smoking status, extensive disease (as defined by greater than five metastatic lesions), and systemic therapy pre- and post-radiation. CTCAE version 4.0 was used for scoring toxicity. Patients were censored at the time of death and lost to follow up.
Results
Patient and treatment characteristics
In total, 34 patients were selected, with 53 treated lesions; 36 (68 %) lesions were treated with SBRT and 17 (32 %) with conventional fractionation (CF-EBRT). The study cohort was followed for a median time of 16 months (range 3–97 months) and the median time for first follow-up was similar in both groups. The majority of patients were male (59 %) with clear cell histology (91 %). The most common SBRT fractionation was 50 Gy given in 5 fractions (10 Gy per fraction); the most common CF-EBRT treatment was 40 Gy in 10 fractions (4 Gy per fraction); 47 % (N = 8) of CF-EBRT were treated with palliative intent (20 Gy in 5 fractions/30 Gy in 10 fractions) (Table 1). The majority of lesions treated were located in the thorax [lung parenchyma (N = 23), hilar and mediastinal lymph nodes (N = 12), and pericardium (N = 1)]. Eight lesions were located in skin/soft tissue [skin/soft tissue extremity (N = 5), parotid (N = 1), gingiva (N = 1), and tongue (N = 1)], and nine lesions treated were within the abdomen [abdominal lymph nodes (N = 3), kidney (N = 3), pancreas (N = 2), and liver (N = 1)]. Median number of lesions treated per patient was 1 (range 1–3). There was no difference between median tumor size between the two groups (SBRT - 21 mm (4–87) and CF-EBRT - 23 mm (15–57)) after t-test comparison (p = 0.357). Median BED was 216.67 (range 66.67–460.0) and 60 (range 46.67–100.83) for SBRT and CF-EBRT respectively. The majority of patients were on systemic therapy before (72 %) and after radiation (57 %) (Table 2).
Table 1.
Patient and clinical characteristics
| Variable | Value |
|---|---|
| Total Number of Patients | 34 |
| Age | |
| Median (range) | 68 (27–84) |
| Sex | |
| Male | 20 (59 %) |
| Female | 14 (41 %) |
| KPS | |
| Median (range) | 90 (60–100) |
| Histology | |
| Clear Cell | 48 (91 %) |
| Papillary | 4 (7 %) |
| Not Otherwise Specified | 1 (2 %) |
| Treatment Patterns | |
| Treated with SBRT | 36 (68 %) |
| 25 Gy/1 fx | 2 |
| 30 Gy/2 fx | 1 |
| 54 Gy/4 fx | 1 |
| 24–60 Gy/3 fx | 15 |
| 25–50 Gy/5 fx | 14 |
| 40 Gy/8 fx | 1 |
| 50 Gy/10 fx | 2 |
| Treated with CF-EBRT | 17 (32 %) |
| 20 Gy/5 fx | 5 |
| 32 Gy/8 fx | 1 |
| 30–40 Gy/10 fx | 8 |
| 45 Gy/13 fx | 1 |
| 45 Gy/15 fx | 1 |
| 55 Gy/22 fx | 1 |
KPS karnofsky performance status, SBRT stereotactic body radiotherapy, CF-EBRT conventional fractionated external beam radiotherapy
Table 2.
Treatment characteristics between SBRT and CF-EBRT
| Variable | SBRT (n = 36) | CF-EBRT (n = 17) |
|---|---|---|
| Location, n (%) | ||
| Thorax | 27 (75 %) | 9 (53 %) |
| Skin & Soft Tissue | 3 (8.3 %) | 5 (29 %) |
| Abdomen | 6 (16.7 %) | 3 (18 %) |
| Median Dose Per Fraction (range, Gy) | 10 (5–25) | 4 (2.5–4) |
| Median Tumor Size (range, mm)* | 21 (4–87) | 23 (15–57) |
| Gross Tumor Volume (GTV) (range, cm3) | 5.14 (0.93–184.07) | - |
| Planned Tumor Volume (PTV) (range, cm3) | 20.01 (6.00–295.51) | - |
| Biological Effective Dose (BED) (range) | 216.67 (66.67–460) | 60.00 (46.67–100.83) |
| Systemic Therapy Prior to Radiation, n (%) | ||
| Yes | 26 (72 %) | 12 (71 %) |
| No | 10 (28 %) | 5 (29 %) |
| Systemic Therapy After Radiation, n (%) | ||
| Yes | 20 (55 %) | 10 (59 %) |
| No | 16 (45 %) | 7 (41 %) |
GTV gross tumor volume, PTV planned tumor volume, BED biologic effective dose
*As determined from the greatest tumor dimension by pre-treatment radiographic imaging. No difference was found between the two groups via t-test comparison (p = 0.357)
Response rates
For all patients combined, radiation therapy provided a median 12 and 24 months treated metastasis control rate of 87.45 and 72.16 %, respectively. The median 12 and 24 months treated metastasis control rate in SBRT treated lesions were 100 and 93.41 % versus 62.02 and 35.27 % in the CF-EBRT (Fig. 1). Radiographic local control rates were significantly different (p < 0.001). There was no difference in overall survival between the two groups (p = 0.831) (Fig. 2).
Fig. 1.
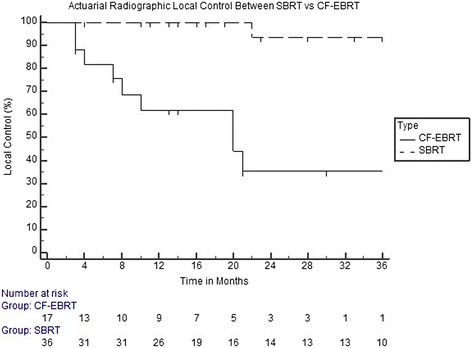
Kaplan-Meier curve demonstrating actuarial radiographic control rates between SBRT and CF-EBRT
Fig. 2.
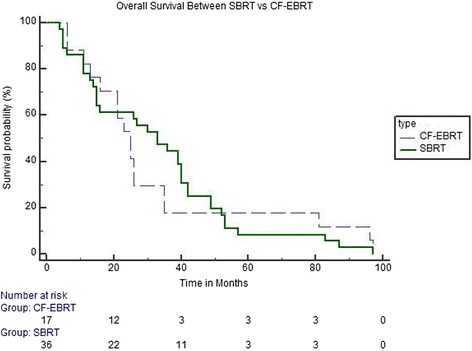
Kaplan-Meier curve demonstrating Overall Survival Rates between SBRT and CF-EBRT
Predictors for local control
When combining all patients included in the study (SBRT and CF-EBRT), predictive factors for radiographic local control under univariate analysis included BED ≥ 100 Gy (HR, 0.048; 95 % CI, 0.006–0.382; p = 0.005) and a dose per fraction ≥ 9 Gy (HR, 0.631; 95 % CI, 0.429–0.931; p = 0.021). Another predictor included gender (HR, 0.254; 95 % CI, 0.066–0.978; p = 0.048). Non-significant predictive factors for radiographic local control included age, lesion location, total dose, smoking, and systemic therapy before or after treatment. GTV and PTV size were non-significant for SBRT patients (p = 0.429). All significant predictors under univariate analysis did not maintain significance under multivariate analysis (Tables 3, 4 and 5). Toxicity rates were low and equivalent in both groups, with no grade 4 or 5 side effects reported (Table 6).
Table 3.
Univariate and multivariate analysis for radiographic predictors of Local Control (LC) for all patients
| Univariate | Multivariate | ||
|---|---|---|---|
| Variable | P-value | HR (95 % CI) | P-value |
| Total Dose (Gy) | 0.001* | 0.999 (0.998 to 1.001) | 0.209 |
| Number of Fractions | 0.189 | 1.004 (0.849 to 1.185) | 0.966 |
| Dose per Fractions (≥9 Gy) | 0.021 | 0.726 (0.469 to 1.124) | 0.153 |
| BED (100 Gy) | 0.005* | 0.264 (0.022 to 3.119) | 0.293 |
| Site (Thorax vs Other) | 0.185 | 1.941 (0.515 to 7.323) | 0.329 |
| Time from Primary Diagnosis | 0.318 | 0.996 (0.980 to 1.012) | 0.663 |
| Male Gender | 0.048 | 0.481 (0.120 to 1.915) | 0.301 |
| Age | 0.610 | 0.990 (0.916 to 1.071) | 0.816 |
| Smoker | 0.123 | 0.276 (0.058 to 1.311) | 0.107 |
| Greater than 5 Metastatic Lesions | 0.808 | 0.674 (0.170 to 2.673) | 0.577 |
| Pre-Radiation Systemic Therapy | 0.517 | 2.299 (0.605 to 8.724) | 0.223 |
| Post-Radiation Systemic Therapy | 0.332 | 0.201 (0.038 to 1.037) | 0.056 |
BED biologic effective dose, HR hazard ratio, CI confidence interval
*-Statistically significant values
Table 4.
Univariate and multivariate analysis for radiographic predictors of Local Control (LC) for SBRT patients
| Univariate | Multivariate | ||
|---|---|---|---|
| Variable | P-value | HR (95 % CI) | P-value |
| Total Dose (Gy) | 0.772 | 0.999 (0.997 to 1.001) | 0.608 |
| Number of Fractions | 0.789 | 1.086 (0.528 to 2.233) | 0.822 |
| Dose per Fractions (≥9 Gy) | 0.474 | 0.835 (0.528 to 1.319) | 0.442 |
| BED (100 Gy) | 0.534 | 0.988 (0.957 to 1.019) | 0.461 |
| Site (Thorax vs Other) | 0.961 | 0.948 (0.915 to 1.012) | 0.957 |
| GTV | 0.429 | 0.958 (0.921 to 1.091) | 0.967 |
| PTV | 0.429 | - | - |
| Time from Primary Diagnosis | 0.491 | 1.224 (0.645 to 2.320) | 0.537 |
| Age | 0.701 | 1.063 (0.885 to 1.277) | 0.513 |
| Smoker | 0.965 | - | - |
| Greater than 5 Metastatic Lesions | 0.963 | - | - |
| Pre-Radiation Systemic Therapy | 0.959 | - | - |
| Post-Radiation Systemic Therapy | 0.961 | - | - |
BED biologic effective dose, GTV gross tumor volume, HR hazard ration, CI confidence interval
Table 5.
Univariate and multivariate analysis for radiographic predictors of Local Control (LC) for CF-EBRT patients
| Univariate | Multivariate | ||
|---|---|---|---|
| Variable | P-value | HR (95 % CI) | P-value |
| Total Dose (Gy) | 0.025* | 0.994 (0.986 to 1.003) | 0.216 |
| Number of Fractions | 0.114 | 0.872 (0.698 to 1.090) | 0.232 |
| Dose per Fractions (≥9 Gy) | 0.950 | 0.729 (0.195 to 2.725) | 0.640 |
| BED (100 Gy) | 0.017* | 3.94 (0.028 to 2.345) | 0.325 |
| Site (Thorax vs Other) | 0.867 | 1.579 (0.404 to 6.173) | 0.513 |
| Time from Primary Diagnosis | 0.714 | 0.987 (0.961 to 1.015) | 0.386 |
| Male Gender | 0.653 | 1.003 (0.244 to 4.128) | 0.995 |
| Age | 0.560 | 0.953 (0.860 to 1.056) | 0.366 |
| Smoker | 0.172 | - | - |
| Greater than 5 Metastatic Lesions | 0.933 | 0.886 (0.216 to 3.623) | 0.867 |
| Pre-Radiation Systemic Therapy | 0.536 | 2.340 (0.586 to 9.345) | 0.231 |
| Post-Radiation Systemic Therapy | 0.417 | 0.206 (0.035 to 1.242) | 0.086 |
BED biologic effective dose, HR hazard ration, CI confidence interval
*-Statistically significant values
Table 6.
Toxicities (N = 31)
| Toxicity | Grade 1 | Grade 2 | Grade 3 |
|---|---|---|---|
| Esophagitis | 2 | 0 | 0 |
| Edema | 2 | 0 | 0 |
| Mucositis | 3 | 2 | 1 |
| Pneumonitis | 1 | 2 | 0 |
| Fatigue | 15 | 1 | 0 |
| Dermatitis | 2 | 0 | 0 |
| Emesis | 1 | 1 | 0 |
| Nausea | 3 | 1 | 0 |
| Hiccups | 0 | 1 | 0 |
| SOB | 1 | 0 | 0 |
| Pain | 0 | 1 | 0 |
No Grade 4 or 5 toxicities to report
Discussion
As assessment of radiation therapy’s effectiveness in RCC is dependent on the BED administered and this work provides an important comparison between SBRT and EBRT in this regard. Presently, the majority of SBRT data for RCC tumors focuses on osseous metastatic sites, with less data on non-bony locations. In the era of SBRT, our findings in addition to other single institutional studies, have demonstrated long-term radiographic local control rates for RCC lesions with the use of SBRT instead of CF-EBRT. The data presented here is an update of prior data published at our institution, which had included 25 lesions (in 13 RCC patients) treated with SBRT; the results here, which includes more lesions with longer follow up, confirms our prior findings that aggressive SBRT can result in good local control rates. Additional institutions have also demonstrated similar results [12, 18]. Wersall and colleagues published their results and demonstrated local control rates above 90 % in their series of RCC treated sites including lung, renal bed, lymph nodes, and adrenal gland; 30 % of patients had complete regression of lesions within 3–36 months, 60 % with partial volume reduction or no change after a median follow-up of 37 months, 2 % had progression, and 8 % were non-evaluable due to early death or atelectasis 18]. Svedman et al. demonstrated very similar findings with a 98 % local control rate. Complete response in their cohort was observed in 21 % of the patients and 58 % of the patients had a partial volume reduction or local stable disease after a median follow-up of 52 months [16]. These findings are similar to our results, with local control rates of 90 % or higher. Taken together, these single institutional studies suggest that SBRT may be more effective at controlling RCC lesions, which were once thought to be radioresistant with the use of lower dose, conventional therapy.
The results presented here also illustrate predictors for local response included BED ≥ 100 and fraction size ≥ 9 Gy. These findings are again supported by earlier results published at our institution evaluating the use of SBRT and doses needed to establish effective control rates for metastatic melanoma and RCC [1, 15]. Stinauer and colleagues included 25 RCC lesions treated with 40–50 Gy in 5 fractions or 42–60 Gy in 3 fractions and had a local control rate of 88 % at 18 months [15]. Predictors of in-field local control included BED > 100 Gy and fraction size > 11 Gy, comparable to our findings. BED has been confirmed to be a strong predictive factor in many other studies, including several Radiation Therapy Oncology Group (RTOG) clinical trials evaluating local control rates with SBRT [10, 13, 17]. Radiobiologically, the higher dose per fraction with SBRT-based treatments has been shown to provide improved local control over standard fractionation. As the survival and proliferation of tumor cells are directly dependent on the blood supply, SBRT has been shown to have a direct effect on tumor vasculature. Hypoxia can increase the expression of vascular endothelial growth factors, which is associated with higher grade tumors and metastatic disease [3]. High-dose single fractionation at 10 Gy or higher has been shown to cause severe vascular damage in human tumor xenografts or animal tumors [2, 8]. SBRT, coupled with targeted agents including vascular endothelial growth factor (VEGF) inhibitors and TKIs, may have both a synergistic local effect in addition to systemic effect and is currently being studied. Additionally, the vascular injury and ensuing chaotic intratumor environment such as hypoxic, acidic and nutritionally-deprived environment caused by high-dose fraction SBRT, may significantly hinder the repair of radiation damage [14]. RCC has several hypothesized mechanisms for radiation resistance with EBRT. One may be a mutation or silencing of the von Hippel-Lindau (VHL) gene which is present in over 50 % of cases and is thought to lead in the accumulation of hypoxic-inducible factor 1-alpha (HIF1A), which then creates angiogenesis leading to further tumor growth and potential disease spread [7]. As described, the mechanism in which SBRT can cause endothelial apoptosis with single high dose treatments may help overcome this pathway.
Currently, the role of systemic therapy in RCC continues to improve with more targeted therapies, providing patients with improved survival and quality of life. Because of this, SBRT is positioned to play a valuable role in providing not only high local control rates but prolonged duration of symptomatic control from months to years. This in turn could translate into both symptomatic relief for the patients and improved survival, especially in those with oligo-progressive disease. In addition, new agents are constantly being developed that may have a synergistic effect with SBRT and will need to be evaluated in clinical trials.
Our study is limited by its retrospective nature, short-term follow up which may have underestimated disease recurrence rates and long term toxicity, and variability in treatment (specifically, fractionation size and total dosage). A common weakness in these studies is the inherent selection bias that may exist as patients who are treated with SBRT may have had less systemic burden, lower comorbidities, and better overall performance status. However, as our endpoints focuses on local radiographic control, it is unlikely these factors contribute significantly to our findings. Further, this study includes data over a long period of time, where technical and systemic treatment approaches have vastly changed. Additionally, due to the relative small numbers of lesions included in this study, subset analysis of each group was difficult. The majority of our patients who underwent SBRT were asked to hold their systemic therapies such as TKIs the day prior to starting SBRT and resumed the day after completion; future studies would need to evaluate toxicity of combining TKIs and other targeted agents with SBRT. Lastly, long term follow up of how these treatments influence the overall survival of patients with RCC is unknown and worthy of prospective follow up.
To conclude, based on our results and emerging data from other investigators, a difference in efficacy between SBRT and CF-EBRT is emerging in the treatment of RCC. Future prospective studies are needed to evaluate efficacy and toxicity of SBRT in the setting of oligometastatic disease for RCC, especially in the setting of newer immune-modulating therapies. With the current published single institutional studies available, SBRT appears to significantly improve local control rates and symptom relief for metastatic RCC to the bone and should be considered for these patients.
Acknowledgements
This work was supported by the Paul Calabresi Career Development Award for Clinical Oncology (K12). We would also like to acknowledge Fundación Aramont for their support in Dr. Bourlon’s research activities.
Footnotes
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
BA was responsible for data collection, data analysis, the writing and review of the manuscript. AA was responsible for data collection, data analysis, study design, and the writing and review of the manuscript. MY was responsible for data analysis and review of the manuscript. MTB was responsible for the study design, data gathering and review of the manuscript. EEK was responsible for the study design, writing and review of the manuscript. TWF was responsible for the study design, writing and review of the manuscript. CMF was responsible for the study design, writing and review of the manuscript. BDK responsible for the study design, writing and review of the manuscript. SDK was responsible for data analysis, study design, and the writing and review of the manuscript. All authors read and approved the final manuscript.
References
- 1.Amini A, Altoos B, Bourlon MT, Bedrick E, Bhatia S, Kessler ER, et al. Local control rates of metastatic renal cell carcinoma (rcc) to the bone using stereotactic body radiation therapy: Is rcc truly radioresistant? Practical radiation oncology 2015. doi:10.1016/j.prro.2015.05.004 [DOI] [PMC free article] [PubMed]
- 2.Chen FH, Chiang CS, Wang CC, Tsai CS, Jung SM, Lee CC, et al. Radiotherapy decreases vascular density and causes hypoxia with macrophage aggregation in tramp-c1 prostate tumors. Clin Cancer Res. 2009;15:1721–9. [DOI] [PMC free article] [PubMed]
- 3.De Meerleer G, Khoo V, Escudier B, Joniau S, Bossi A, Ost P, et al. Radiotherapy for renal-cell carcinoma. Lancet Oncol. 2014;15:e170–7. doi: 10.1016/S1470-2045(13)70569-2. [DOI] [PubMed] [Google Scholar]
- 4.Escudier B, Pluzanska A, Koralewski P, Ravaud A, Bracarda S, Szcylik C, et al. Bevacizumab plus interferon alfa-2a for treatment of metastatic renal cell carcinoma: A randomised, double-blind phase III trial. Lancet. 2007;370:2103–11. doi: 10.1016/S0140-6736(07)61904-7. [DOI] [PubMed] [Google Scholar]
- 5.Escudier B, Porta C, Schmidinger M, Algaba F, Patard JJ, Khoo V, et al. Renal cell carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2014;25(Suppl 3):iii49–56. doi: 10.1093/annonc/mdu259. [DOI] [PubMed] [Google Scholar]
- 6.Escudier B, Szcylik C, Hutson TE, Demkow T, Staehler M, Rolland F, et al. Randomized phase II trial of first-line treatment with sorafenib versus interferon alfa-2a in patients with metastatic renal cell carcinoma. J Clin Oncol. 2009;27:1280–9. doi: 10.1200/JCO.2008.19.3342. [DOI] [PubMed] [Google Scholar]
- 7.Jonasch E, Futreal PA, Davis IJ, Bailey ST, Kim WY, Brugarolas J, et al. State of the science: An update on renal cell carcinoma. Mol Cancer Res. 2012;10:859–80. doi: 10.1158/1541-7786.MCR-12-0117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kioi M, Vogel H, Schultz G, Hoffman RM, Harsh GR, Brown JM. Inhibition of vasculogenesis, but not angiogenesis, prevents the recurrence of glioblastoma after irradiation in mice. J Clin Invest. 2010;120:694–705. [DOI] [PMC free article] [PubMed]
- 9.Loizzi M, Sollitto F, Sardelli P, De Palma A, Lopez C, Lacitignola A, et al. Endothoracic nodules in patients who under-went nephrectomy for renal cell carcinoma. Results of surgical resection. Minerva Med. 2003;94:103–10. [PubMed] [Google Scholar]
- 10.Onishi H, Shirato H, Nagata Y, Hiraoka M, Fujino M, Gomi K, et al. Hypofractionated stereotactic radiotherapy (hypofxsrt) for stage i non-small cell lung cancer: Updated results of 257 patients in a japanese multi-institutional study. J Thorac Oncol. 2007;2:S94–100. doi: 10.1097/JTO.0b013e318074de34. [DOI] [PubMed] [Google Scholar]
- 11.Pantuck AJ, Seligson DB, Klatte T, Yu H, Leppert JT, Moore L, et al. Prognostic relevance of the mtor pathway in renal cell carcinoma: Implications for molecular patient selection for targeted therapy. Cancer. 2007;109:2257–67. doi: 10.1002/cncr.22677. [DOI] [PubMed] [Google Scholar]
- 12.Ranck MC, Golden DW, Corbin KS, Hasselle MD, Liauw SL, Stadler WM, et al. Stereotactic body radiotherapy for the treatment of oligometastatic renal cell carcinoma. Am J Clin Oncol. 2013;36:589–95. [DOI] [PubMed]
- 13.Rusthoven KE, Kavanagh BD, Cardenes H, Stieber VW, Burri SH, Feigenberg SJ, et al. Multi-institutional phase I/II trial of stereotactic body radiation therapy for liver metastases. J Clin Oncol. 2009;27:1572–8. [DOI] [PubMed]
- 14.Song CW, Cho LC, Yuan J, Dusenbery KE, Griffin RJ, Levitt SH. Radiobiology of stereotactic body radiation therapy/stereotactic radiosurgery and the linear-quadratic model. Int J Radiat Oncol Biol Phys. 2013;87:18–9. doi: 10.1016/j.ijrobp.2013.03.013. [DOI] [PubMed] [Google Scholar]
- 15.Stinauer MA, Kavanagh BD, Schefter TE, Gonzalez R, Flaig T, Lewis K, et al. Stereotactic body radiation therapy for melanoma and renal cell carcinoma: Impact of single fraction equivalent dose on local control. Radiat Oncol. 2011;6:34. doi: 10.1186/1748-717X-6-34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Svedman C, Sandstrom P, Pisa P, Blomgren H, Lax I, Kalkner KM, et al. A prospective phase ii trial of using extracranial stereotactic radiotherapy in primary and metastatic renal cell carcinoma. Acta Oncol. 2006;45:870–5. doi: 10.1080/02841860600954875. [DOI] [PubMed] [Google Scholar]
- 17.Timmerman R, Paulus R, Galvin J, Michalski J, Straube W, Bradley J, et al. Stereotactic body radiation therapy for inoperable early stage lung cancer. JAMA. 2010;303:1070–6. [DOI] [PMC free article] [PubMed]
- 18.Wersall PJ, Blomgren H, Lax I, Kalkner KM, Linder C, Lundell G, et al. Extracranial stereotactic radiotherapy for primary and metastatic renal cell carcinoma. Radiother Oncol. 2005;77:88–95. doi: 10.1016/j.radonc.2005.03.022. [DOI] [PubMed] [Google Scholar]