

Abstract
Apigenin is a natural phyto-oestrogen flavonoid, which exerts various biological effects, including anti-oxidative, anti-inflammatory and anticancer activities. In addition, apigenin has recently been reported to target hypoxic markers; however, there are currently no studies regarding the association between apigenin and glucose transporter-1 (GLUT-1) in adenoid cystic carcinoma (ACC). The present study investigated whether apigenin inhibits the proliferation of ACC cells or suppresses the expression of GLUT-1 in ACC cells. The results of the present study demonstrated that apigenin inhibits ACC-2 cell growth in a dose- and time-dependent manner. Treatment with apigenin also induced apoptosis and G2/M-phase arrest in a dose- and time-dependent manner. Corresponding with the above results, the expression levels of GLUT-1 were significantly decreased following treatment in a dose- and time-dependent manner. These results suggest that the inhibition of ACC-2 cell growth by apigenin may be due to the decreased expression of GLUT-1.
Keywords: apigenin, head and neck, adenoid cystic carcinoma, glucose transporter-1, anticancer effect
Introduction
Adenoid cystic carcinoma (ACC) is characterised by a prolonged clinical course, frequent local recurrence and perineural invasion (1–3). The standard primary treatment strategies for local and locoregional disease are surgery and/or irradiation (3); however, the long-term outcomes of these treatments are unfavourable. Various drugs have been used in the field of targeted therapy against ACC; however, the predominant effect of these drugs is disease stabilisation. Therefore, novel strategies are required to improve kill ACC cells with lower systemic toxicity, particularly for use in combination therapy.
Apigenin is a natural phyto-oestrogen flavonoid, which exerts various biological effects, including anti-oxidative, anti-inflammatory and anticancer activities (4). Apigenin has been shown to inhibit prostate (5), thyroid (6), breast (7), pancreatic (8), ovarian (9), and head and neck cancer (10), via the selective inhibition of tumour cell proliferation. Numerous studies have investigated the effects of apigenin; however, the underlying biomolecular mechanism remains to be elucidated.
Apigenin has recently been reported to target the hypoxic markers hypoxia-inducible factor-1α (HIF-1α), glucose transporter-1 (GLUT-1), and vascular endothelial growth factor in human pancreatic (8,11), ovarian (12), and lung carcinoma cell lines (13). Similar to other malignant tumours, ACC cells exhibit increased glucose uptake and utilisation, as compared with their non-malignant counterparts, and GLUT-1 is considered to have a key molecular regulatory role in this process. In addition, GLUT-1 is correlated with the aggressive biological behaviour of other types of human cancer (14,15). Our previous study indicated that the radioresistance of laryngeal carcinoma may be associated with increased expression of GLUT-1 mRNA and protein (16). In addition, GLUT-1 antisense oligodeoxynucleotides were able to enhance the radiosensitivity of laryngeal carcinoma, predominantly via inhibition of GLUT-1 expression (16). Therefore, GLUT-1 is regarded as a potential therapeutic target in certain types of cancer (17,18). To the best of our knowledge, there are currently no studies regarding the association between apigenin and GLUT-1 in ACC.
The present study aimed to investigate whether apigenin inhibits the proliferation of ACC cells, and whether it may suppress the expression of GLUT-1 in ACC cells.
Materials and methods
Cell culture
The ACC-2 human adenoid cystic carcinoma cell line was purchased from the Cell Research Institute of the Chinese Academy of Sciences (Shanghai, China). The ACC-2 cells were cultured in Dulbecco's modified Eagle's medium (DMEM; Gibco Life Technologies, Grand Island, NY, USA) supplemented with 10% heat-inactivated foetal bovine serum (Hyclone, GE Healthcare, Logan, UT, USA), 2 mM L-glutamine, 100 U/ml penicillin, and 100 g/ml streptomycin (100biotech Co., Ltd., Hangzhou, China) at 37°C in an atmosphere containing 5% CO2. The cells were trypsinised and harvested after reaching 80–90% confluence.
Proliferation assay of ACC-2 cells using the Cell Counting kit-8 (CCK-8) system
Cultured ACC-2 cells were trypsinised with 0.25% trypsin (100biotech Co., Ltd). Cell proliferation was measured using the CCK-8 system (Beyotime Institute of Biotechnology, Nanjing, China), according to the manufacturer's instructions. Briefly, 3×103 ACC-2 cells were seeded into 96-well culture plates and treated with either DMEM, or 10, 40 or 160 µM apigenin (Selleckchem, Houston, TX, USA) The cells were cultured in serum-free medium (100biotech Co., Ltd.) at 37°C for 1, 2, 3, 4 or 5 days. A total of 10 µl CCK-8 reagent was added to each well, and incubated at 37°C for 3 h, and the absorbance was measured at 450 nm. Optical density (OD) was calculated as follows: OD = ODcell − ODblank.
Cell cycle analysis using flow cytometry
A total of 3×103 ACC-2 cells were seeded into 96-well culture plates and treated with either DMEM, or 10, 40 or 160 µM apigenin for 24, 48 or 72 h. The cells from each group were trypsinised with 0.25% trypsin and rinsed in phosphate-buffered saline (PBS). The cells were centrifuged at 800 × g for 5 min and resuspended in up to 500 µl PBS. The cells were centrifuged at 2,000 × g for 5 min, collected and fixed in ice-cold 70% ethanol for 24 h, prior to re-centrifugation. The cells were then incubated with RNase (0.5 mg/ml) and stained with 1 ml of 50 µg/ml propidium iodide (PI; Sigma-Aldrich, St. Louis, MO, USA) in the dark for 30 min at room temperature. The cells were subsequently added to 5 µl Annexin V-fluorescein isothiocyanate (FITC) and 5 µl PI, and incubated for a further 15 min at 25°C. The cells were then added to 400 µl binding buffer in the dark for 1 h. The FACScan analysis system (BD Biosciences, Franklin Lakes, NJ, USA) was then used to collect flow cytometry (FCM) data to determine changes in cell cycle distribution. Each experiment was performed three times in triplicate.
Cell apoptosis analysis using flow cytometry
A total of 3×103 ACC-2 cells were seeded into 96-well culture plates and treated with either DMEM or 10, 40, or 160 µM apigenin for 24, 48 or 72 h. The cells from each group were trypsinised using 0.25% trypsin and rinsed in PBS. The cells were centrifuged at 800 × g for 5 min and resuspended in up to 500 µl PBS. The cells was centrifuged at 2,000 × g for 5 min, collected and fixed in ice-cold 70% ethanol for 24 h and re-centrifuged. The cells were then incubated with 500 µl binding buffer in the dark for 30 min at room temperature. The cells were added to 5 µl Annexin V-FITC and 5 µl PI, followed by incubation for 15 min at 25°C. The FACScan analysis system was then used to collect FCM data on changes in cell apoptosis. Each experiment was performed three times in triplicate.
Determination of GLUT-1 mRNA expression in ACC-2 cells by reverse transcription-quantitative polymerase chain reaction (RT-qPCR)
Briefly, 3×103 ACC-2 cells were seeded into 96-well culture plates and treated with either DMEM, or 10, 40 or 160 µM apigenin for 24, 48, or 72 h. The ACC-2 cells were homogenised in TRIzol® reagent (Invitrogen Life Technologies, Carlsbad, CA, USA) and total RNA was extracted, according to the manufacturer's instructions. A total of l µg RNA was added to M-MLV reverse transcriptase (100biotech Co., Ltd.) in a 20 µl reaction volume, and the reaction mix was pre-denatured at 65°C for 10 min. After the addition of 200 U M-MLV, the samples were incubated at 42°C for 1 h and annealed at 70°C for 10 min. The newly synthesised cDNA was used as a template for RT-qPCR. The 20 µl PCR reaction mix consisted of 10 µl 2X SYBR Green (Toboyo Co., Ltd., Tokyo, Japan), 1 µl cDNA template, 1 µl upstream and downstream specific primers, and 8 µl deionised water. The PCR cycling conditions were as follows: Pre-denaturation at 95°C for 2 min, followed by 40 cycles at 95°C for 15 sec, 59°C for 20 sec and 72°C for 20 sec and a final extension step at 72°C for 10 min. Experiments were performed in triplicate and were repeated at least twice independently. The primers used were as follows: Forward: 5′-CCGCAACGAGGAGAACCG-3′ and reverse: 5′-GTGACCTTCTTCTCCCGCATC-3′ for GLUT-1; and forward: 5′-TGTTGCCATCAATGACCCCTT-3′, and reverse: 5′-CTCCACGACGTACTCAGCG-3′ fir GAPDH. GAPDH was used as an internal standard for data calibration. The lengths of the PCR products were 123 bp (GLUT-1) and 202 bp (GAPDH). Dissociation curve analysis was conducted, and the 2−ΔΔCt quantification method was used to calculate differential gene expression.
Determination of GLUT-1 protein levels in ACC-2 cells by western blotting
The GLUT-1 and β-actin (control) protein expression levels were detected in each group of ACC-2 cells by western blotting. Following extraction of the GLUT-1 and β-actin proteins, the protein concentration was determined using a bicinchoninic acid protein quantitative kit (Wuhan Boster Biological Technology Co. Ltd., Wuhan, China). Briefly, 80 µg protein was separated by 10% SDS-PAGE and transferred onto a nitrocellulose membrane (EMD Millipore, Billerica, MA, USA). Skimmed milk (2%) was used to block the membrane at room temperature for 1 h. The membrane was then incubated with the following primary antibodies: Rabbit anti-human polyclonal GLUT-1 (1:1,000; cat. no. ab14683; Abcam, Cambridge, UK) and mouse anti-human monoclonal β-actin (1:5,000; Abcam) at room temperature for 3 h, followed by an incubation with donkey anti-rabbit (1:5,000) and donkey anti-mouse (1:2,000) secondary antibodies at room temperature for 1 h. The blots were visualized using an enhanced chemiluminescence system (Santa Cruz Biotechnology, Inc., Dallas, TX, USA) and were exposed to X-ray film. Protein expression was semi-quantitatively analysed using the Kodak Gel Logic Analysis system (Kodak, Rochester, NY, USA).
Statistical analysis
Statistical analyses were performed using SPSS for Windows, version 19.0 (IBM SPSS, Armonk, NY, USA). An independent t-test was used for analysis. P<0.05 was deemed to indicate a statistically significant difference.
Results
Apigenin inhibits the growth of ACC-2 cells
The CCK-8 assay demonstrated that various concentrations (10–160 µM) and durations (1–5 days) of apigenin treatment resulted in a dose- and time-dependent inhibition of ACC-2 cell growth, as compared with the control (P<0.05; Fig. 1).
Figure 1.

Various concentrations (10–160 µM) and durations (1–5 days) of apigenin treatment resulted in a dose- and time-dependent inhibition of ACC-2 human adenoid cystic carcinoma cell growth, as determined by Cell Counting kit-8. *P<0.05 vs. control on days 2–5.
Apigenin induces apoptosis and cell cycle arrest in ACC-2 cells
The ACC-2 cells were treated with various concentrations (10–160 µM) of apigenin for 24, 48, and 72 h and apoptotic cell death and cell cycle alterations were detected using FCM (Fig. 2A). Treatment with apigenin induced apoptosis in a dose- and time-dependent manner, as compared with the control (Fig. 2B). The percentage of apoptotic cells increased to 64.8% following treatment with 160 µM apigenin. In addition, the results of the FCM demonstrated that the cell cycle progressed from G1 to G2 phase, and was arrested at G2/M phase in a dose- and time-dependent manner (Fig. 3A). The G2/M-phase population of the control cells was 14.65%, and was markedly increased after 24, 48 and 72 h of treatment with various concentrations of apigenin (Table I, Fig. 3B).
Figure 2.

(A) Flow cytometry was used to determine the rate of apoptosis of ACC-2 human adenoid cystic carcinoma cells following treatment with apigenin. (B) Treatment with apigenin induced apoptosis in a dose- and time-dependent manner, as compared with the control. *P<0.05 vs. control. FITC, fluorescein isothiocyanate; PI, propidium iodide.
Figure 3.
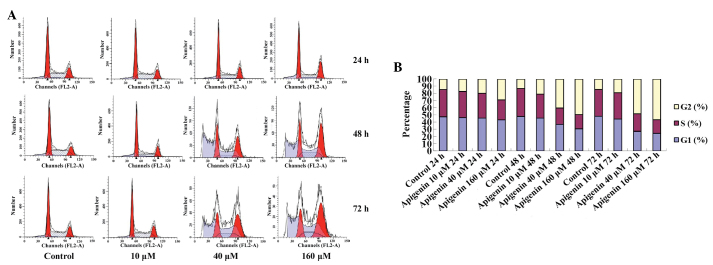
(A) Flow cytometry was used to determine cell cycle distribution of ACC-2 human adenoid cystic carcinoma cells following treatment with apigenin. (B) The G2/M-phase population of the control cells was 14.65%, which was markedly increased after 24, 48 and 72 h of treatment with various doses of apigenin.
Table I.
Distribution of ACC-2 cells in the cell cycle exposed to different concentration of apigenin over time.
| Group | G1 (%) | S (%) | G2 (%) |
|---|---|---|---|
| 24 h | |||
| Control | 47.42 | 37.93 | 14.65 |
| 10 µM apigenin | 46.13 | 36.49 | 17.38 |
| 40 µM apigenin | 45.42 | 34.54 | 20.04 |
| 160 µM apigenin | 43.26 | 27.89 | 28.85 |
| 48 h | |||
| Control | 47.89 | 38.74 | 13.37 |
| 10 µM apigenin | 45.51 | 33.4 | 21.09 |
| 40 µM apigenin | 36.81 | 22.91 | 40.28 |
| 160 µM apigenin | 30.46 | 20.08 | 49.46 |
| 72 h | |||
| Control | 48.05 | 37.46 | 14.49 |
| 10 µM apigenin | 44.41 | 36.43 | 19.16 |
| 40 µM apigenin | 27.32 | 24.41 | 48.27 |
| 160 µM apigenin | 24.64 | 18.75 | 56.61 |
Apigenin downregulates the mRNA and protein expression levels of GLUT-1 in ACC-2 cells
To determine the GLUT-1 mRNA and protein expression levels in ACC-2 cells, RT-qPCR and western blotting were conducted, respectively. GLUT-1 mRNA expression levels were significantly reduced following treatment with increasing doses of apigenin (P<0.05; Table II, Fig. 4). Following treatment with 10 µM apigenin, the mRNA expression levels of GLUT-1 did not vary significantly with increasing treatment duration (P>0.05). Conversely, following treatment with 40 and 160 µM apigenin, the expression levels of GLUT-1 mRNA were significantly reduced with increasing treatment duration (P<0.05; Table II, Fig. 4). Western blotting demonstrated that the GLUT-1 protein expression levels were reduced following apigenin treatment in a dose- and time-dependent manner (Fig. 5A and B).
Table II.
mRNA expression levels of GLUT-1 in ACC-2 cells treated with different concentrations of apigenin over time.
| Group | GLUT-1 mRNA
|
||
|---|---|---|---|
| 24 h | 48 h | 72 h | |
| Control | 1.00±0.11 | 1.00±0.20 | 1.00±0.07 |
| Apigenin | |||
| 10 µM | 0.72±0.08 | 0.69±0.09 | 0.60±0.06 |
| 40 µM | 0.48±0.09 | 0.40±0.04 | 0.25±0.02 |
| 160 µM | 0.28±0.05 | 0.22±0.02 | 0.13±0.01 |
Expression values are expressed relative to GAPDH.
Figure 4.
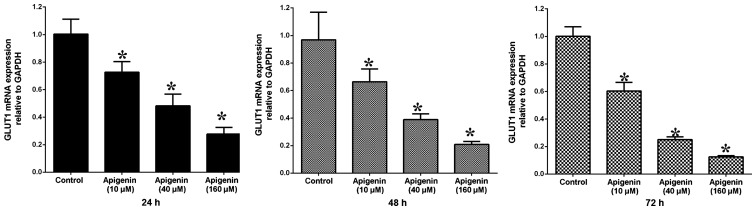
GLUT-1 mRNA expression levels were significantly reduced in the ACC-2 human adenoid cystic carcinoma cells following treatment with increasing doses of apigenin (P<0.05), as determined by reverse transcription-quantitative polymerase chain reaction. Following treatment with 10 µM apigenin, the expression levels of GLUT-1 mRNA did not vary significantly with increasing treatment duration (P>0.05). Following treatment with 40 and 160 µM apigenin, the expression levels of GLUT-1 mRNA were significantly reduced with increasing treatment duration. *P<0.05 vs. control. GLUT-1, glucose transporter-1.
Figure 5.

(A) Western blotting detected GLUT-1 protein levels in ACC-2 human adenoid cystic carcinoma cells following treatment with increasing doses of apigenin. (B) Relative protein expression levels of GLUT-1 were reduced in a dose- and time-dependent manner. *P<0.05 vs. control. GLUT-1, glucose transporter-1.
Discussion
At present, patients with ACC receive comprehensive treatment, including extensive local resection; medical neck dissection when cervical lymph node metastases are present; and treatment combined with postoperative radiotherapy and/or chemotherapy in cases of advanced ACC; however, the results are usually unfavourable. In addition, patients with ACC are usually insensitive to chemo-radiotherapy, which results in high recurrence rates and distant metastasis at an early stage (3). Therefore, identification of novel molecular targets is of great importance.
Apigenin has previously been reported to exert its anticancer effect via various mechanisms (5–11). It has been reported that apigenin may suppress human cancer by inhibiting the expression of GLUT-1 (8,11). To the best of our knowledge, there are currently no studies regarding the interaction between apigenin and GLUT-1 in ACC. The results of the present study demonstrated that apigenin inhibits the proliferation of ACC-2 cells in a dose-and time-dependent manner, this finding is concordant with the results of previous studies regarding other types of cancer (13,19,20). In other cell lines, apigenin has also been shown to induce apoptosis and cell cycle arrest (13,19,20). In T24 bladder cancer cells, Zhu et al (21) demonstrated that treatment with apigenin resulted in increases in apoptosis and G2/M-phase arrest, with an almost 2.6-fold increase, in a dose-dependent manner. In a lung adenocarcinoma cell line, Bruno et al (19) demonstrated that apigenin significantly decreased cell proliferation and augmented cell death and apoptosis. In addition, apigenin has been shown to inhibit growth, induce apoptosis, and promote G2/M phase cell cycle arrest in head and neck squamous cell carcinoma cells (10). In the present study, apigenin induced ACC-2 cell apoptosis, and G2/M-phase arrest. The percentage of apoptotic cells increased to 64.8% following treatment with 160 µM apigenin, and the percentage of cells in G2/M phase dose-dependently increased from 17.38 to 28.85% after 24 h, from 21.09 to 49.46% after 48 h, and from 19.16 to 56.61%, an almost 2.7-fold increase, after 72 h. In addition, the percentage of cells in the G2/M phase increased in a time-dependent manner from 17.38 to 56.61%, an almost 3.3-fold increase. The results of the present study, as well as those of previous studies, suggested that apigenin-induced cell growth inhibition may be due to cell cycle arrest (21). In addition, apigenin has been shown to cause G0/G1-phase arrest, resulting in death and apoptosis of human prostate cancer cells (20) and cervical carcinoma cells (22). These results suggested that apigenin-induced cell cycle arrest may be caused by various molecular regulatory mechanisms, and the distinct characteristics of cancer cell lines.
The anticancer mechanism of apigenin remains unclear (23). Apigenin has recently been reported to target hypoxic markers, and GLUT-1 is an intrinsic marker of malignant tumour hypoxia (24). GLUT-1 overexpression enables the transport of increased levels of glucose to fulfil the high metabolic rate and rapid growth requirements of malignant cells. In our previous study, it was demonstrated that overexpression of GLUT-1 may have a role in the development of recurrence of ACC-2 cells (2). In addition, GLUT-1 has been suggested as a potential therapeutic target in other types of cancer (14,15). In certain human cancer cell lines, apigenin has been shown to decrease the expression of GLUT-1, and exert an anticancer effect (5–12). The present study demonstrated that apigenin-induced cell apoptosis may be due to decreased expression of GLUT-1 in ACC-2 cells. Corresponding with the inhibition of proliferation of ACC-2 cells and increased cell apoptosis, the expression levels of GLUT-1 were significantly decreased following treatment with apigenin in a dose- and time-dependent manner. The relative mRNA expression levels of GLUT-1 were decreased by ~5.5-fold from 0.72 to 0.13, and the relative protein expression levels of GLUT-1 decreased by ~14.6-fold from 0.73 to 0.05. The mechanism underlying these changes may involve inhibition of glucose absorption by ACC-2 cells. In human pancreatic cancer cells, Melstrom et al (8) demonstrated that 100 µM apigenin inhibited cell growth and lowered GLUT-1 mRNA expression. The same study also reported that apigenin was able to inhibit GLUT-1 expression at the transcriptional and translational levels in a dose- and time-dependent manner in human pancreatic cancer. However, the mechanism by which apigenin inhibits GLUT-1 expression is currently unknown. Melstrom et al (8) reported that apigenin may inhibit the phosphoinositide 3-kinase (PI3K)/Akt pathway in order to reduce GLUT-1 expression, thus inhibiting the absorption of glucose by pancreatic cancer cells, resulting in apoptosis. However, it was also detected that overexpression of phosphorylated-Akt did not completely attenuate the effects of apigenin on GLUT-1, indicating that the PI3K/Akt pathway is not solely responsible for the downregulation of GLUT-1 in pancreatic cancer cells treated with apigenin (8). Therefore, the mechanism by which apigenin inhibits GLUT-1 expression requires further investigation. Our future studies aim to investigate whether apigenin inhibits GLUT-1 expression via the PI3K/Akt-HIF axis in ACC.
In conclusion, the present study demonstrated that apigenin inhibits proliferation and induces cell apoptosis, and G2/M-phase arrest in ACC-2 cells, possibly due to decreased GLUT-1 expression.
Acknowledgments
The present study was supported by the Health Department of Zhejiang Province, China (grant no. 2012KYB206), and the National Natural Science Foundation of China (grants nos. 81172562 and 81372903).
References
- 1.Kim B. Palliative radiotherapy in a patient with pulmonary adenoid cystic carcinoma. Cancer Res Treat. 2007;39:185–188. doi: 10.4143/crt.2007.39.4.185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Fang J, Bao YY, Zhou SH, Luo XM, Yao HT, He JF, Wang QY. Recurrent prognostic factors and expression of GLUT-1, PI3K and p-Akt in adenoid cystic carcinomas of the head and neck: Clinicopathological features and biomarkers of adenoid cystic carcinoma. Oncol Lett. 2012;4:1234–1240. doi: 10.3892/ol.2012.895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Papaspyrou G, Hoch S, Rinaldo A, Rodrigo JP, Takes RP, van Herpen C, Werner JA, Ferlito A. Chemotherapy and targeted therapy in adenoid cystic carcinoma of the head and neck: A review. Head Neck. 2011;33:905–911. doi: 10.1002/hed.21458. [DOI] [PubMed] [Google Scholar]
- 4.Patel D, Shukla S, Gupta S. Apigenin and cancer chemo-prevention: Progress potential and promise (review) Int J Oncol. 2007;30:233–245. [PubMed] [Google Scholar]
- 5.Oishi M, Iizumi Y, Taniguchi T, Goi W, Miki T, Sakai T. Apigenin sensitizes prostate cancer cells to Apo2L/TRAIL by targeting adenine nucleotide translocase-2. PLoS One. 2013;8:e55922. doi: 10.1371/journal.pone.0055922. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kim SH, Kang JG, Kim CS, Ihm SH, Choi MG, Yoo HJ, Lee SJ. Apigenin induces c-Myc-mediated apoptosis in FRO anaplastic thyroid carcinoma cells. Mol Cell Endocrinol. 2013;369:130–139. doi: 10.1016/j.mce.2013.01.012. [DOI] [PubMed] [Google Scholar]
- 7.Cao X, Liu B, Cao W, Zhang W, Zhang F, Zhao H, Meng R, Zhang L, Niu R, Hao X, Zhang B. Autophagy inhibition enhances apigenin-induced apoptosis in human breast cancer cells. Chin J Cancer Res. 2013;25:212–222. doi: 10.3978/j.issn.1000-9604.2013.04.01. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Melstrom LG, Salabat MR, Ding XZ, Milam BM, Strouch M, Pelling JC, Bentrem DJ. Apigenin inhibits the GLUT-1 glucose transporter and the phosphoinositide 3-kinase/Akt pathway in human pancreatic cancer cells. Pancreas. 2008;37:426–431. doi: 10.1097/MPA.0b013e3181735ccb. [DOI] [PubMed] [Google Scholar]
- 9.He J, Xu Q, Wang M, Li C, Qian X, Shi Z, Liu LZ, Jiang BH. Oral administration of apigenin inhibits metastasis through AKT/P70S6K1/MMP-9 pathway in orthotopic ovarian tumor model. Int J Mol Sci. 2012;13:7271–7282. doi: 10.3390/ijms13067271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Chan LP, Chou TH, Ding HY, Chen PR, Chiang FY, Kuo PL, Liang CH. Apigenin induces apoptosis via tumor necrosis factor receptor- and Bcl-2-mediated pathway and enhances susceptibility of head and neck squamous cell carcinoma to 5-fluorouracil and cisplatin. Biochim Biophys Acta. 2012;1820:1081–1091. doi: 10.1016/j.bbagen.2012.04.013. [DOI] [PubMed] [Google Scholar]
- 11.Melstrom LG, Salabat MR, Ding XZ, Strouch MJ, Grippo PJ, Mirzoeva S, Pelling JC, Bentrem DJ. Apigenin down-regulates the hypoxia response genes: HIF-1α, GLUT-1, and VEGF in human pancreatic cancer cells. J Surg Res. 2011;167:173–181. doi: 10.1016/j.jss.2010.10.041. [DOI] [PubMed] [Google Scholar]
- 12.Fang J, Zhou Q, Liu LZ, Xia C, Hu X, Shi X, Jiang BH. Apigenin inhibits tumor angiogenesis through decreasing HIF-1alpha and VEGF expression. Carcinogenesis. 2007;28:858–864. doi: 10.1093/carcin/bgl205. [DOI] [PubMed] [Google Scholar]
- 13.Liu LZ, Fang J, Zhou Q, Hu X, Shi X, Jiang BH. Apigenin inhibits expression of vascular endothelial growth factor and angiogenesis in human lung cancer cells: Implication of chemoprevention of lung cancer. Mol Pharmacol. 2005;68:635–643. doi: 10.1124/mol.105.011254. [DOI] [PubMed] [Google Scholar]
- 14.Li LF, Zhou SH, Zhao K, Wang SQ, Wu QL, Fan J, Cheng KJ, Ling L. Clinical significance of FDG single-photon emission computed tomography: Computed tomography in the diagnosis of head and neck cancers and study of its mechanism. Cancer Biother Radiopharm. 2008;23:701–714. doi: 10.1089/cbr.2008.0510. [DOI] [PubMed] [Google Scholar]
- 15.Wu XH, Chen SP, Mao JY, Ji XX, Yao HT, Zhou SH. Expression and significance of hypoxia-inducible factor-1α and glucose transporter-1 in laryngeal carcinoma. Oncol Lett. 2013;5:261–266. doi: 10.3892/ol.2012.941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Yan SX, Luo XM, Zhou SH, Bao YY, Fan J, Lu ZJ, Liao XB, Huang YP, Wu TT, Wang QY. Effect of antisense oligodeoxynucleotides glucose transporter-1 on enhancement of radiosensitivity of laryngeal carcinoma. Int J Med Sci. 2013;10:1375–1386. doi: 10.7150/ijms.6855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Xu YY, Bao YY, Zhou SH, Fan J. Effect on the expression of MMP-2, MT-MMP in laryngeal carcinoma Hep-2 cell line by antisense glucose transporter-1. Arch Med Res. 2012;43:395–401. doi: 10.1016/j.arcmed.2012.07.003. [DOI] [PubMed] [Google Scholar]
- 18.Liu TQ, Fan J, Zhou L, Zheng SS. Effects of suppressing glucose transporter-1 by an antisense oligodeoxynucleotide on the growth of human hepatocellular carcinoma cells. Hepatobiliary Pancreat Dis Int. 2011;10:72–77. doi: 10.1016/S1499-3872(11)60010-6. [DOI] [PubMed] [Google Scholar]
- 19.Bruno A, Siena L, Gerbino S, Ferraro M, Chanez P, Giammanco M, Gjomarkaj M, Pace E. Apigenin affects leptin/leptin receptor pathway and induces cell apoptosis in lung adenocarcinoma cell line. Eur J Cancer. 2011;47:2042–2051. doi: 10.1016/j.ejca.2011.03.034. [DOI] [PubMed] [Google Scholar]
- 20.Shukla S, Gupta S. Apigenin-induced cell cycle arrest is mediated by modulation of MAPK, PI3K-Akt, and loss of cyclin D1 associated retinoblastoma dephosphorylation in human prostate cancer cells. Cell Cycle. 2007;6:1102–1114. doi: 10.4161/cc.6.9.4146. [DOI] [PubMed] [Google Scholar]
- 21.Zhu Y, Mao Y, Chen H, Lin Y, Hu Z, Wu J, Xu X, Xu X, Qin J, Xie L. Apigenin promotes apoptosis, inhibits invasion and induces cell cycle arrest of T24 human bladder cancer cells. Cancer Cell Int. 2013;13:54. doi: 10.1186/1475-2867-13-54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Zheng PW, Chiang LC, Lin CC. Apigenin induced apoptosis through p53-dependent pathway in human cervical carcinoma cells. Life Sci. 2005;76:1367–1379. doi: 10.1016/j.lfs.2004.08.023. [DOI] [PubMed] [Google Scholar]
- 23.Bao YY, Zhou SH, Fan J, Wang QY. Anticancer mechanism of apigenin and the implications of GLUT-1 expression in head and neck cancers. Future Oncol. 2013;9:1353–1364. doi: 10.2217/fon.13.84. [DOI] [PubMed] [Google Scholar]
- 24.Kim JI, Choi KU, Lee IS, Choi YJ, Kim WT, Shin DH, Kim K, Lee JH, Kim JY, Sol MY. Expression of hypoxic markers and their prognostic significance in soft tissue sarcoma. Oncol Lett. 2015;9:1699–1706. doi: 10.3892/ol.2015.2914. [DOI] [PMC free article] [PubMed] [Google Scholar]