

Abstract
Background
Dislocation is a common complication after total hip arthroplasty (THA). Although the etiology of dislocation is multifactorial, longer-term changes in muscle such as atrophy may influence the risk of prosthetic dislocation. Biological differences in wear products generated by different bearing surfaces may influence differences in the appearance of periarticular muscle after THA; however, such bearing-associated differences to our knowledge have not been studied in vivo, and few studies have evaluated bearing-associated differences in dislocation risk.
Questions/purposes
(1) Is there a correlation between the postoperative risk of dislocation at revision and the bearing surfaces of the primary arthroplasty? (2) Is there a higher extent of fatty muscle atrophy on CT scan in hips with osteolysis (polyethylene hips) as compared with hips without osteolysis (ceramic-on-ceramic hips)? (3) Are these two abnormalities (bone osteolysis and fatty atrophy) associated with a decrease of mesenchymal stem cells (MSCs) in bone and in muscle?
Methods
We retrospectively evaluated 240 patients (240 hips) who had a THA revision (98% of which, 235 of the 240, were isolated acetabular revisions) and a normal contralateral hip. All patients had received the same implants for the primary arthroplasty (32-mm head) except for bearing surfaces (80 hips with ceramic-on-ceramic, 160 with polyethylene). No differences were noted between the groups in terms of age, sex, body mass index, proportion of patients who had a dislocation after the index arthroplasty but before the revision, and proportion of the patients with stem loosening in addition to acetabular loosening. Indications for revision generally were cup loosening. The revisions in the hips with polyethylene bearings generally had more acetabular bone loss, but the position of the center of the cup and the orientation of the cup were similar after reconstruction in the two groups. Before revision, osteolysis, muscle atrophy, and fatty degeneration were evaluated on CT scan and compared with the contralateral side. Bone muscle progenitors were evaluated by bone marrow MSCs and satellite cells for muscle. At revision, all the hips received the same implants with the same head diameter (32 mm) and a standard liner. Revisions were performed between 1995 and 2005. The followup after revision was at a mean of 14 years (range, 10–20 years) for ceramic revision and 12 years (range, 10–20 years) for polyethylene hips, and there was no differential loss to followup between the groups.
Results
More hips with polyethylene liners at the time of index arthroplasty dislocated after revision than did hips with ceramic liners (18% [29 of 160] compared with 1% [one of 80]; odds ratio, 17.5; 95% confidence interval, 2.3363–130.9100; p = 0.005). For the 80 hips with ceramic-on-ceramic, no osteolysis was detected before revision; there was no muscle fatty degeneration of the gluteus muscles on CT scan or histology. For the 160 hips with polyethylene liners, osteolytic lesions on the acetabulum and femur were observed in 100% of the hips. The increased atrophy of the gluteus muscles observed on CT scan correlated with the increase of osteolysis (r = 0.62; p = 0.012). The surgical limbs in the patients with polyethylene hips as compared with ceramic-on-ceramic hips demonstrated a greater reduction in cross-sectional area (respectively, 11.6% compared with 3%; odds ratio, 3.82; p < 0.001) and radiological density (41% [14.1/34.1] compared with 9%; odds ratio, 6.8; p = 0.006) of gluteus muscles when compared with the contralateral normal side. (41% compared with 9%; odds ratio, 6.8; p = 0.006).
Conclusions
Ceramic bearing surfaces were associated with fewer dislocations after revision than polyethylene bearing surfaces. The reasons of the lower rate of dislocation with ceramic-on-ceramic bearings may be related to observed differences in the periarticular muscles (fat atrophy or not) with the two bearing surfaces.
Level of Evidence
Level III, therapeutic study.
Introduction
Ceramic-on-ceramic (CoC) primary THA has demonstrated decreased osteolysis [8, 18, 31] and decreased capsule atrophy [21] with a decreased risk of late dislocation in an earlier study from our group [16] as compared with polyethylene (PE) hips. We also remarked [16, 17] that at the time of revision, muscles of CoC hips had less structural changes than muscles of PE hips. However, little is known about muscular changes after THA and it is not known whether these changes are related to the bearing surfaces and to the nature of the debris particles. We also noted that the risk of dislocation was decreased after revision of CoC when compared with the risk after revision of hips with osteolysis related to PE wear.
Although atrophy of the muscles has been described in patients with osteoarthritis of the hip [1, 27] and after THA [24], to our knowledge, no studies have evaluated longer-term changes to the radiographic appearance and histological qualities of the periarticular musculature after THA. Muscle atrophy is indicated as a loss of volume and conventionally measured by a reduced cross-sectional area [27] on CT scan. However, an additional loss of contractile muscle is fatty muscle atrophy (or infiltration) described first in shoulder muscles [14] and indicated by a reduced radiological density [12, 13] assessed in Hounsfield units. Although the etiology of dislocation is multifactorial, longer-term changes in muscle such as atrophy may influence the risk of prosthetic dislocation. Biological differences in wear products generated by different bearing surfaces may influence differences in the appearance of periarticular muscle after THA; however, such bearing-associated differences in hip musculature to our knowledge have not been studied in vivo, and few studies have evaluated bearing-associated differences in dislocation risk [16].
Our aim therefore was to evaluate the quality of the muscle mass in the long term after THA with different bearing surfaces. We specifically asked the following questions: (1) Is there a correlation between the postoperative risk of dislocation at revision and the bearing surfaces of the primary arthroplasty? (2) Is there a higher extent of fatty muscle atrophy on CT scan in hips with osteolysis (PE hips) as compared with hips without osteolysis (CoC hips)? (3) Are these two abnormalities (bone osteolysis and fatty atrophy) associated with a decrease of mesenchymal stem cells (MSCs) in bone and in muscle?
Patients and Methods
We retrospectively evaluated 240 patients (240 hips) who had a THA revision (98% of which [235 of the 240] were isolated acetabular revisions) and a normal contralateral hip. Revisions were performed between 1995 and 2005. All patients had received the same implants (Ceraver Osteal, Roissy, France) for the primary arthroplasty (32-mm head) except for bearing surfaces (80 hips with CoC, 160 with conventional PE). The indications for each bearing surface were at the discretion of the surgeon. No differences (Table 1) were noted between the groups in terms of age, sex, body mass index, proportion of patients who had a dislocation after the index arthroplasty but before the revision, and proportion of the patients with stem loosening in addition to acetabular loosening. The mean age at surgery was 65 years (range, 54–84 years). The indication for revision was cup loosening.
Table 1.
Demographic data of the two groups of patients
| Demographic | Ceramic-on-ceramic (80 hips) | Polyethylene (160 hips) | p value |
|---|---|---|---|
| Age at primary hip (mean years; range) | 44 (28–55) | 48 (26–57) | 0.43 |
| Age at revision (mean years; range) | 66 (56–80) | 64 (54–84) | 0.36 |
| Sex (men; number) | 59 men (74%) | 114 men (71%) | 0.24 |
| BMI (mean kg/m2; range) | 23 (16–28) | 21 (17–27) | 0.16 |
| Previous hip procedure | None (exclusion criteria) | None (exclusion criteria) | NA |
| Hip dislocation before (number) | 2 (2.5%) | 8 (5%) | 0.42 |
| Time (years) between primary and revision arthroplasty | 12 (4–25) | 15 (9–20) | 0.74 |
| Injection | None (exclusion criteria) | None (exclusion criteria) | NA |
| Activity level | Not exactly know but not high (rather normal) | Not exactly known but not high (rather normal) | NA |
BMI = body mass index; NA = not available.
Acetabular defects were more severe in PE hips: most of them were Paprosky III; the acetabular defects in ceramic hips were typically Paprosky II. As a consequence, Kerboull cross plate devices and allograft were used more frequently in revision of PE hips than in ceramic hips. The position of the center of the cup and the orientation of the cup were similar after reconstruction in the two groups. After revision the position of the center of rotation and the abduction acetabular angle were similar in the two groups (mean angle 48° ± 10° in the PE group versus 50° ± 13° in the alumina group; p = 0.24); the acetabular anteversion measured on CT scan was also similar (mean angle 22° ± 8° in the PE group versus 27° ± 11° in the CoC group; p = 0.16); and the leg length discrepancy acquired with cup loosening was reestablished to the original value by reestablishing the center of rotation in a similar manner in both groups. The femoral anteversion was not measured but did not change after revision because the number of stem revisions was very low. We performed stem revision when stem loosening was present; in this series there was one hip with stem loosening and revision in the CoC group and four with stem loosening and revisions in the PE group (p = 0.55). Surgery was performed with a posterolateral approach under general anesthesia. At revision, all the hips received the same implants with the same head diameter (32 mm) and a standard liner. The cup diameter sizes were similar (p = 0.04) in both groups: mean 52.4 mm (range, 48–56 mm) for the PE groups and mean 52.8 mm (range, 48–58 mm) for the CoC groups. The 32-mm alumina head was always anchored through the same Morse taper (14–16 mm; 5°–42°). Therefore, all patients had the same head-neck ratio. The acetabular component was a PE cup or an alumina cup and was always cemented. Both components were fixed with cement (Palacos G; Heraeus Medical Gmbh, Hanau, Germany) containing antibiotics (gentamicin). No bracing or casting was performed in any patient.
Number of Dislocations After Revision
The followup routine time was at 3, 6, and 12 months and then annually thereafter. At each visit, patients had clinical and radiological evaluation. From the charts, we determined whether there were any dislocations (posterior or anterior) or revisions for recurrent dislocation or loosening. We routinely evaluated patients, in person or by means of a standardized letter or telephone questionnaire, at 2 to 3 months postoperatively and then at each subsequent 1-year interval until rerevision or death. In the ceramic group (80 hips), six hips (7.5%) were lost to followup before 10 years (between 6 and 10 years) and three (3.8%) patients had died (between 3 and 10 years). In the PE group (160 hips), 15 (9.3%) hips were lost to followup before 10 years (between 7 and 10 years) and eight (5%) patients had died (between 5 and 10 years) indicating no differential loss to followup (p = 0. 40) between the groups. The followup after revision was 14 years (range, 10–20 years) for ceramic revision and 12 years (range, 10–20 years) for PE hips.
At each time point, we asked patients about whether they had dislocation of the hip. We did not consider a sensation of subluxation of the hip to be sufficiently specific to represent an episode of hip instability. We considered only those events that required either a closed or open reduction. Electrodiagnostic testing (muscles) and study of sensory and motor conduction velocities were only performed for patients with postoperative dislocation.
Evaluation of Osteolysis and Muscle Atrophy
CT was performed for every patient with the patient in a supine position. CT scan was performed preoperatively and at the most recent followup. Hips were scanned from 8 cm proximal to the acetabular component to a point distal to the end of the femoral implant. The maximum thickness of the cuts ranged from 1 to 3 mm. To calculate the volume of the osteolysis, lesions were identified and traced on each axial cut with use of a semiautomated edge-detection module (Adobe Photoshop; Adobe Systems Software Ireland Ltd, Dublin, Ireland). The areas of the lytic lesions were then calculated from each tracing by determining the number of pixels per square millimeter. The volume between adjacent cuts was calculated by averaging the areas between adjacent cuts multiplied by the thickness of the cuts. Summation of the volumes on each of these cuts was used to determine the total volume of bone loss resulting from lysis as previously described [18]. Muscle cross-sectional area and radiological density (Fig. 1) were assessed bilaterally in the gluteus maximus, medius, and minimus. For the area, the surface was measured in millimeters squared. Radiological density was identified and quantified by use of standard Hounsfield unit (HU) thresholds [12, 13], which represent the physical properties of tissues expressed in numerical form (skeletal muscle −29 to 150 HU; intramuscular fat −190 to −30 HU). These methods are highly reliable with reported intra- and interclass coefficients of variation between 0.2% and 4.8% [12, 13]. To guarantee the same transverse evaluation level at each time point, the anatomically correct height was adjusted on the coronal planes in the scout at the CT scan workstation. Muscle cross-sectional area and radiological density were compared with the contralateral side without arthroplasty. On histology objective quantification of skeletal muscle, lipid staining was performed by using the oil red O soluble dye, which stains neutral lipid with an orange-red tint. Muscle lipid content was measured as the area occupied by lipid staining, and lipid accumulation (LA) was calculated as follows: LA = total area occupied by lipid droplets of muscle fiber /total cross-sectional area of a muscle fiber.
Fig. 1.
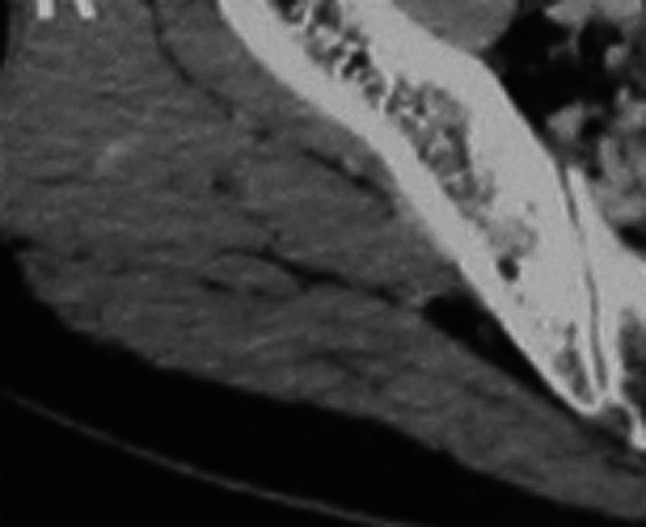
The CT scan demonstrates the variability of the density of the muscle.
Evaluation of the Number Stem Cells in Bone and in Muscle
For bone, bone marrow was collected at the beginning of surgery from the ilium corresponding to the hip under revision under general anesthesia just before hip skin incision. The needle was rinsed with a heparin solution introduced by hand in the iliac crest at a distance from the osteolysis and three aliquots were aspirated. The number of total nucleated cells was determined by counting marrow smears on a hemocytometer and then normalizing the counts to the volume of marrow aspirated. The number of colony-forming unit fibroblasts was determined as an indication of the number of MSCs present in the bone marrow aspirate before processing and in the bone marrow-derived cell concentrate. The assay has been described previously [15, 16]. For muscle, four biopsies were obtained from the gluteus medius and gluteus maximus at surgery; one muscle biopsy was for evaluation of fatty infiltration; and one biopsy muscle sample was examined by light microscopy after staining with hematoxylin-eosin, periodic acid Schiff, and Masson’s trichrome to check fatty degeneration. The second biopsy was for evaluation of satellite cells. Approximately 50 mg of the biopsy sample was mounted in optimum cutting temperature and frozen in isopentane cooled in liquid nitrogen; mononuclear cells isolated from muscle biopsies were then stained with an antibody against desmin, a muscle-specific marker. Slides were incubated at 4 °C. Mononuclear cells were then cytostained with Pax7 [26–30].
Statistics
Continuous descriptive statistics used means ± SD or range, percentages within groups, median values, ranges, and 95% confidence intervals where appropriate. Qualitative data between the two groups were compared with use of the chi-square test or Fisher’s exact test and quantitative data with the Mann-Whitney test. The level of significance was set at p < 0.05 in all analyses.
Results
More hips with PE liners at the time of index arthroplasty dislocated after revision than did hips with ceramic liners (18% [29 of 160] compared with 1% [one of 80]; odds ratio [OR], 17.5; 95% confidence interval [CI], 2.3363–130.9100; p = 0.005). For the 80 hips with CoC as the primary bearing surface, one dislocation (1%) was observed during followup. For the 160 hips with PE liners as the primary bearing surface, the risk of dislocation after revision was 5% at 1 month, 10% (16 hips) at 1 year, and 18% (29 hips) at 10 years. No neurologic lesions were observed on the electromyelogram. Revision for recurrent dislocation was performed in 13 hips (8%).
No osteolysis was observed in the CoC hips, whereas all of the PE hips demonstrated some osteolysis; increasing amounts of osteolysis were associated with increasing amounts of muscle atrophy observed on CT scan. The increase in the fatty atrophy of the gluteus muscles correlated with the increase of osteolysis (r = 0.62; p = 0.012). For hips with PE, osteolytic lesions on acetabulum and femur were observed in 100% of the hips with a volume of osteolysis ranging from 5 to 90 cm3 (mean, 35 cc); the surgical limbs in the patients with PE hips demonstrated reduced cross-sectional area compared with the contralateral normal side (Table 2); this reduction was more severe than in the gluteus maximus of patients with CoC hips compared with the contralateral normal side (respectively, 11.6% [449 of 3854] compared with 3% [124 of 3756]; OR, 3.82; 95% CI, 3.1214–4.6962; p < 0.001). There also was a reduced radiological density (Table 2) in the gluteus maximus of PE hips with the contralateral normal side as compared with CoC hips (41% [14.1/34.1] compared with 9% [2.9/32.4]; OR, 6.8; 95% CI, 1.7178–26.6543; p = 0.006). Muscle fatty infiltration determined in vivo with CT scan was associated with muscle LA determined in muscle biopsy specimens. Increased LA assessed microscopically was observed both in the gluteus medius (containing some PE debris), but also in the gluteus maximus without PE debris of patients with PE hips (Figs. 2, 3). Lipid contained within muscle fibers as determined with staining of lipid was negatively associated with muscle density (r = −0.43, p = 0.001). Roughly each HU reduced density was equivalent to a 1% increase in LA when assessed microscopically. There was an increased LA in the gluteus maximus of PE hips as compared with CoC hips (15.4%; range, 4.2%–36% compared with 3.1%; range, 0.8%–6.2%; OR, 5.7; 95% CI, 1.5970–20.3861; p = 0.007). Dislocations (Table 3) were observed in hips with severe osteolysis and with severe reduced radiological muscular density. Values stratified by osteolysis amount revealed that fat infiltration was greater in those with advanced osteolysis (p = 0.01).
Table 2.
Mean values (SD) of preoperative cross-sectional area (CSA) in millimeters squared and of radiological density in Hounsfield units (HU) in the healthy hip (without arthroplasty) and in the CoC and PE hips with arthroplasty before revision*
| Parameters | Healthy side | CoC hip | Difference | p value |
|---|---|---|---|---|
| CSA (mm2) | ||||
| Gluteus maxiumus | 3756 (648) | 3632 (637) | 3% | 0.64 |
| Gluteus medius + minimus | 4832 (542) | 4785 (534) | 1% | 0.82 |
| Density (HU) | ||||
| Gluteus maxiumus | 32.4 (10.3) | 29.5 (9.8) | 9% | 0.07 |
| Gluteus medius + minimus | 36.8 (11.3) | 32.6 (10.2) | 11% | 0.06 |
| Parameters | Healthy side | PE hip | Difference | p value |
|---|---|---|---|---|
| CSA (mm2) | ||||
| Gluteus maxiumus | 3854 (732) | 3435 (681) | 11% | 0.02 |
| Gluteus medius + minimus | 4952 (793) | 4438 (702) | 10% | 0.02 |
| Density (HU) | ||||
| Gluteus maxiumus | 34.2 (11.5) | 20.1 (9.3) | 41% | 0.001 |
| Gluteus medius + minimus | 38.5 (12.3) | 25.9 (10.4) | 33% | 0.001 |
* Gluteus medius and gluteus minimus were not individualized for measurements; CoC = ceramic-on-ceramic; PE = polyethylene.
Fig. 2.
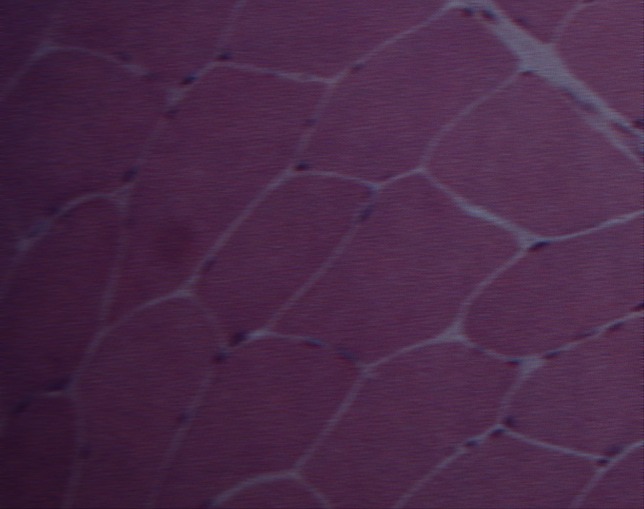
This biopsy demonstrates the normal aspect of the muscle (gluteus maximus) (Stain, hematoxylin-eosin; original magnification, ×100).
Fig. 3.
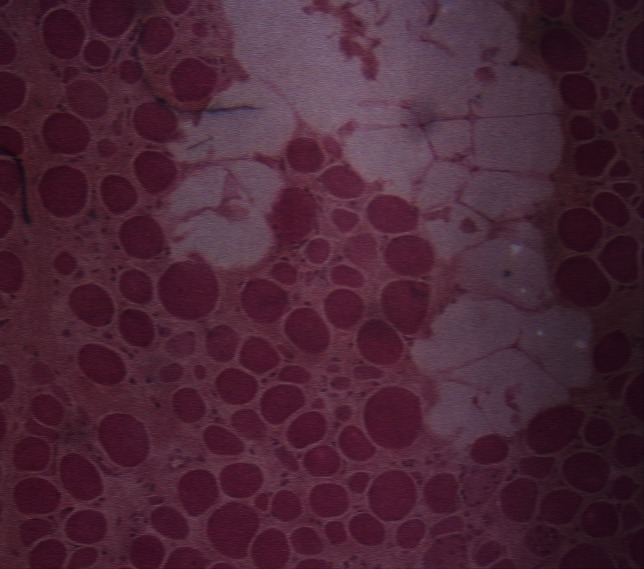
This biopsy of the gluteus maximus muscle demonstrates fatty infiltration of the muscle (30% of fat degeneration) (Stain, hematoxylin-eosin; original magnification, ×50).
Table 3.
Osteolysis (mean volume in cc; range), muscle density in Hounsfield units (mean; range), and cross-sectional area (CSA) of the gluteus maximus muscle in millimeters squared (mean surface; range)
| Parameter | No dislocation (131 hips) | Dislocation (29 hips) | p value |
|---|---|---|---|
| Osteolysis (cc) | 15 (5–45) | 70 (50–90) | 0.001 |
| Muscle density (HU) | 26 (22–32) | 10 (9–18) | 0.001 |
| CSA (mm2) | 3640 (3200–4900) | 3124 (2834–3642) | 0.07 |
HU = Hounsfield units.
In patients with PE hips, a decrease of bone marrow MSCs and muscle satellite cells was observed compared with CoC hips. The mean difference in the concentration of bone marrow MSCs per 1.0 mL of bone marrow aspirates of the iliac crest was 788 (range, 280–1200; 95% CI, 234–1245; p < 0.001); the mean values in the CoC group were 1002 ± 324 MSCs/mL (range, 1430–732 MSCs/mL) and in the PE group 214 ± 128 MSCs/mL (range, 18–310 MSCs/mL). The mean difference in the number of satellite cells/g was 49,910 (range, 21,000–82,000; 95% CI, 26,000–82,000; p < 0.001). The mean number of satellite cells/g in the CoC group was 62,540 (range, 41,500–102,490) and in the PE group 12,630 (range, 8760–24,300). These decreases of MSCs (mean, 788; range, 80–1200; 65%) and satellite cells (mean, 49,910; range, 21,000–82,000; 79%) in the PE group (as compared with the CoC group) correlated with the increase of osteolysis (respectively, r = −0.34; p = 0.021 and r = −0.56; p = 0.028), the decrease of muscle density (respectively, r = 0.48; p < 0.001 and r = 0.62; p < 0.001), and the increase of fat infiltration on histology (respectively, r = −0.51; p < 0.001 and r = −0.67; p < 0.001).
Discussion
Dislocation is a common complication after THA. Although the etiology of dislocation is multifactorial, longer-term changes in muscle such as atrophy may influence the risk of prosthetic dislocation. Biological differences in wear products generated by different bearing surfaces may influence differences in the appearance of periarticular muscle after THA. However, no one has looked at muscle changes and bone changes related to different bearing surfaces to see whether the bearing used at the index arthroplasty was associated with a difference in likelihood of dislocation after revision. We have investigated CT-based measures of skeletal muscle adiposity in patients undergoing THA presenting different bearing surfaces (CoC or PE), evaluated the risk of dislocation after revision in these patients according to their bearing surfaces and muscular status before revision, and analyzed bone and muscle progenitors around the hip of these patients. We found that ceramic surfaces used in THAs at the index arthroplasty were associated with fewer dislocations after revision THA as compared with PE bearing surfaces. This difference may be related to the reduced amount of fatty atrophy observed in the periarticular musculature in patients whose index THA included a CoC bearing compared with those with ceramic-on-PE bearings.
We note several limitations to our study. First, ours was a retrospective study of a nonrandomized patient population. Thus, our study is a study of association, not causation, and not all important variables have been controlled for; the difference in dislocation risk could be a function of bone loss, for example, which differed substantially between the groups. Likewise, activity level was not controlled for or even measured. These factors, and others, could well have influenced the findings. Second, the small patient cohort may limit the generalizability of the study, although we had adequate power to identify the findings of interest. Third, measurement of skeletal muscle adiposity based on a standard CT image after surgical approach may be difficult. However, we were at a distance (several years) from the initial primary arthroplasty, and studies using CT have reported coefficients of variation between 1.5% and 2.5% for tissue cross-sectional area and 1% for muscle attenuation [13]. This study was also limited in that the femoral stem anteversion was not assessed systematically on preoperative CT scan, but the positioning of the stem was analyzed on the postoperative CT scan of patients with dislocation and we did not found abnormalities. The femoral head sizes (32 mm) and the acetabular components were similar in the two groups. There was a risk that some patients had rupture of the gluteus medius tendon, which affects elderly women and often has a sudden onset [11, 20]. These ruptures are clearly seen at revision and we excluded these patients (six patients). Another bias could be the inclusion of patients with nerve injury or spinal disease. We excluded these patients but did not perform electromyelography preoperatively for each patient. Electrodiagnostic tests were performed only in patients with postoperative dislocations and although they were difficult to interpret because the patients had difficulty in performing hip abduction by adequately contracting the gluteus medius muscles, these tests excluded neurogenic distress.
The major findings of this study are the extent of knowledge regarding the risk of dislocation after revision. Although the dislocation risk has been previously reported to vary depending on the component revised [2, 6, 7, 22, 23], our results support the idea that the risk is also related to the bearing surface of the primary arthroplasty. We tested only two bearing surfaces (CoC and PE), but another study [25] has also demonstrated high risk (28% [nine of 32]) of dislocation after revision of metal-on-metal.
We found that CT scans were able to demonstrate reduced density corresponding to fatty muscle degeneration associated with increased osteolysis and also to predict the risk of postoperative dislocation in the case of revision. To our knowledge, this question of the relationship between muscle quality and dislocation after revision has not been evaluated before.
It is well known that skeletal muscle has a close relationship with bone mass, starting in the embryonic period. Developmentally, osteoblasts and muscle cells derive from a common mesenchymal precursor [3–5, 9, 19]. There is a positive correlation between muscle strength and bone mass. It appears that in case of osteolysis, there is osteolysis-associated reduced bone regenerative capacity with a decrease of MSCs and that this is accompanied by a reduced muscle mass and increased fatty degeneration. The cause of the reduced regenerative capacity of bone and muscle in PE hips is unknown. The possible mechanism was evaluated by an experimental study [10] demonstrating that contact PE particles inhibit the osteogenic activity of osteoprogenitor cells in a murine model, which may result in reduced periprosthetic bone regeneration. Future studies should evaluate the effect of PE particles on satellite cells of humans.
In conclusion, the use of alumina-on-alumina bearing surfaces at the index arthroplasty was on murine associated with a lower frequency of dislocation after revision THA as compared with alumina-on-PE bearing surfaces. The reasons for the lower rate of dislocation with CoC bearings may be related to observed differences in the periarticular muscles (fat atrophy or not) with the two bearing surfaces. Our research suggests that there could be a new focus in ceramic component research, beyond wear and tribology to better understand the role of bearing surface debris on muscular atrophy. Experimental studies could evaluate first whether contact PE particles and ceramic particles have different effects on the activity of satellite muscle cells of humans.
Footnotes
Each author certifies that he or she, or a member of his or her immediate family, has no funding or commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Clinical Orthopaedics and Related Research ® neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA-approval status, of any drug or device prior to clinical use.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
This work was performed at Hospital Henri Mondor, University Paris East, Paris, France.
References
- 1.Adolphson P, von Sivers K, Dalen N, Jonsson U, Dahlborn M. Bone and muscle mass after hip arthroplasty: a quantitative computed tomography study in 20 arthrosis cases. Acta Orthop Scand. 1993;64:181–184. doi: 10.3109/17453679308994566. [DOI] [PubMed] [Google Scholar]
- 2.Alberton GM, High WA, Morrey BF. Dislocation after revision total hip arthroplasty: an analysis of risk factors and treatment options. J Bone Joint Surg Am. 2002;84:1788–1792. [PubMed] [Google Scholar]
- 3.Alessandri G, Pagano S, Bez A, Benetti A, Pozzi S, Iannolo G, Baronio M, Invernici G, Caruso A, Muneretto C, Bisleri G, Parati E. Isolation and culture of human muscle-derived stem cells able to differentiate into myogenic and neurogenic cell lineages. Lancet. 2004;364:1872–1883. doi: 10.1016/S0140-6736(04)17443-6. [DOI] [PubMed] [Google Scholar]
- 4.Armand O, Boutineau AM, Mauger A, Pautou MP, Kieny M. Origin of satellite cells in avian skeletal muscles. Arch Anat Microsc Morphol Exp. 1983;72:163–181. [PubMed] [Google Scholar]
- 5.Asakura A, Komaki M, Rudnicki M. Muscle satellite cells are multipotential stem cells that exhibit myogenic, osteogenic, and adipogenic differentiation. Differentiation. 2001;68:245–253. doi: 10.1046/j.1432-0436.2001.680412.x. [DOI] [PubMed] [Google Scholar]
- 6.Berry DJ, Von Knoch M, Schleck CD, Harmsen WS. The cumulative long-term risk of dislocation after primary Charnley total hip arthroplasty. J Bone Joint Surg Am. 2004;86:9–14. doi: 10.2106/00004623-200401000-00003. [DOI] [PubMed] [Google Scholar]
- 7.Berry DJ, von Knoch M, Schleck CD, Harmsen WS. Effect of femoral head diameter and operative approach on risk of dislocation after primary total hip arthroplasty. J Bone Joint Surg Am. 2005;87:2456–2463. doi: 10.2106/JBJS.D.02860. [DOI] [PubMed] [Google Scholar]
- 8.Bizot P, Banallec L, Sedel L, Nizard R. Alumina-on-alumina total hip prostheses in patients 40 years of age or younger. Clin Orthop Relat Res. 2000;379:68–76. doi: 10.1097/00003086-200010000-00010. [DOI] [PubMed] [Google Scholar]
- 9.Charge SB, Rudnicki MA. Cellular and molecular regulation of muscle regeneration. Physiol Rev. 2004;84:209–238. doi: 10.1152/physrev.00019.2003. [DOI] [PubMed] [Google Scholar]
- 10.Chiu R, Ma T, Smith RL, Goodman SB. Ultrahigh molecular weight polyethylene wear debris inhibits osteoprogenitor proliferation and differentiation in vitro. J Biomed Mater Res A. 2009;89:242–247. doi: 10.1002/jbm.a.32001. [DOI] [PubMed] [Google Scholar]
- 11.Chung CB, Robertson JE, Cho GJ, Vaughan LM, Copp SN, Resnick D. Gluteus medius tendon tears and avulsive injuries in elderly women: imaging findings in six patients. AJR Am J Roentgenol. 1999;173:351–353. doi: 10.2214/ajr.173.2.10430134. [DOI] [PubMed] [Google Scholar]
- 12.Daguet E, Jolivet E, Bousson V, Boutron C, Dahmen N, Bergot C, Vicaut E, Laredo J-D. Fat content of hip muscles: an anteroposterior gradient. J Bone Joint Surg Am. 2011;93:1897–1905. doi: 10.2106/JBJS.J.00509. [DOI] [PubMed] [Google Scholar]
- 13.Goodpaster BH, Kelley DE, Thaete FL, He J, Ross R. Skeletal muscle attenuation determined by computed tomography is associated with skeletal muscle lipid content. J Appl Physiol. 2000;89:104–110. doi: 10.1152/jappl.2000.89.1.104. [DOI] [PubMed] [Google Scholar]
- 14.Goutallier D, Postel JM, Bernageau J, Lavau L, Voisin MC. Fatty muscle degeneration in cuff ruptures. Pre- and postoperative evaluation by CT scan. Clin Orthop Relat Res. 1994;304:78–83. [PubMed] [Google Scholar]
- 15.Hernigou P, Homma Y, Flouzat Lachaniette CH, Poignard A, Allain J, Chevallier N, Rouard H. Benefits of small volume and small syringe for bone marrow aspirations of mesenchymal stem cells. Int Orthop. 2013;37:2279–2287. doi: 10.1007/s00264-013-2017-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hernigou P, Homma Y, Pidet O, Guissou I, Hernigou J. Ceramic-on-ceramic bearing decreases the cumulative long-term risk of dislocation. Clin Orthop Relat Res. 2013;471:3875–3882. doi: 10.1007/s11999-013-2857-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hernigou P, Pariat J, Queinnec S, Homma Y, Flouzat Lachaniette CH, Chevallier N, Rouard H. Supercharging irradiated allografts with mesenchymal stem cells improves acetabular bone grafting in revision arthroplasty. Int Orthop. 2014;38:1913–1921. doi: 10.1007/s00264-014-2285-2. [DOI] [PubMed] [Google Scholar]
- 18.Hernigou P, Zilber S, Filippini P, Poignard A. Ceramic-ceramic bearing decreases osteolysis: a 20-year study versus ceramic-polyethylene on the contralateral hip. Clin Orthop Relat Res. 2009;467:2274–2280. doi: 10.1007/s11999-009-0773-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Hill M, Wernig A, Goldspink G. Muscle satellite (stem) cell activation during local tissue injury and repair. J Anat. 2003;203:89–99. doi: 10.1046/j.1469-7580.2003.00195.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Jarvinen TA, Jarvinen TL, Kaariainen M, Kalimo H, Jarvinen M. Muscle injuries: biology and treatment. Am J Sports Med. 2005;33:745–764. doi: 10.1177/0363546505274714. [DOI] [PubMed] [Google Scholar]
- 21.Lerouge S, Huk O, Yahia L. Ceramic-ceramic or metal-PE. A comparison of periprosthetic tissues from loosened total hip arthroplasty. J Bone Joint Surg Br. 1997;79:135–139. doi: 10.1302/0301-620X.79B1.6621. [DOI] [PubMed] [Google Scholar]
- 22.Lindberg HO, Carlsson AS, Gentz CF, Pettersson H. Recurrent and non-recurrent dislocation following total hip arthroplasty. Acta Orthop Scand. 1982;53:947–952. doi: 10.3109/17453678208992853. [DOI] [PubMed] [Google Scholar]
- 23.Meek RMD, Allan DB, McPhillips G, Kerr L, Howie CR. Epidemiology of dislocation after total hip arthroplasty. Clin Orthop Relat Res. 2006;447:9–18. doi: 10.1097/01.blo.0000218754.12311.4a. [DOI] [PubMed] [Google Scholar]
- 24.Muller M, Tohtz S, Dewey M, Springer I, Perka C. Evidence of reduced muscle trauma through a minimally invasive anterolateral approach by means of MRI. Clin Orthop Relat Res. 2010;468:3192–3200. doi: 10.1007/s11999-010-1378-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Munro JT1, Masri BA, Duncan CP, Garbuz DS. High complication rate after revision of large-head metal-on-metal total hip arthroplasty. Clin Orthop Relat Res. 2014;472:523–528. doi: 10.1007/s11999-013-2979-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Rantanen J, Hurme T, Lukka R, Heino J, Kalimo H. Satellite cell proliferation and the expression of myogenin and desmin in regenerating skeletal muscle: evidence for two different populations of satellite cells. Lab Invest. 1995;72:341–347. [PubMed] [Google Scholar]
- 27.Rasch A, Bystrom AH, Dalen N, Berg HE. Reduced muscle radiological density, cross-sectional area, and strength of major hip and knee muscles in 22 patients with hip osteoarthritis. Acta Orthop. 2007;78:505–510. doi: 10.1080/17453670710014158. [DOI] [PubMed] [Google Scholar]
- 28.Relaix F, Montarras D, Zaffran S, Gayraud-Morel B, Rocancourt D, Tajbakhsh S, Mansouri A, Cumano A, Buckingham M. Pax3 and Pax7 have distinct and overlapping functions in adult muscle progenitor cells. J Cell Biol. 2006;172:91–102. doi: 10.1083/jcb.200508044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Relaix F, Rocancourt D, Mansouri A, Buckingham M. A Pax3/ Pax7-dependent population of skeletal muscle progenitor cells. Nature. 2005;435:948–953. doi: 10.1038/nature03594. [DOI] [PubMed] [Google Scholar]
- 30.Seale P, Ishibashi J, Scime A, Rudnicki MA. Pax7 is necessary and sufficient for the myogenic specification of CD451:Sca11 stem cells from injured muscle. PLoS Biol. 2004;2:E130. doi: 10.1371/journal.pbio.0020130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Sedel L, Nizard R, Kerboull L, Witwoet J. Alumina-alumina hip replacement in patients younger than 50 years old. Clin Orthop Relat Res. 1994;298:175–183. [PubMed] [Google Scholar]