

Abstract
There is some evidence to suggest that a benefit might be derived from a program that incorporated both annual physical examination of the breast (BPx) and the teaching of breast self-examination (BSE). Current investigation presents the profile of a multicenter community based intervention for evaluating the effect of BSE+BPx on the reduction of morbidity and mortality due to breast cancer amongst women residing in urban areas of Yazd (Iran) from 2008 to 2018. There were three distinctive phases in this trial with 10 years duration: pilot phase with the duration of 1 year, active intervention phase with 4 rounds of annual screening of BPx+BSE and follow up phase with 5 years duration. Tools of enquiry included a pre-tested questionnaire, repeated annual physical examination of the breast and more importantly mammography, sonography, and fine needle aspiration (FNA). Data were analyzed using descriptive statistics such as frequencies, percent, mean (SD), tests of chi-square and student t-test with 95% confidence level. Comparison of socio-demographic and socio-economic factors such as age, age at marriage, family size, number of live births, occupation, education level, total family income and marital status showed that no significant difference was seen between the groups (P>0.05). A response rate of 84.5% was seen by participants of the experiment group visiting the health centers for the first BPx. Our results showed that except for the education and marital status, the difference in other main demographic and socio-economic factors between the groups were not significant, and the response rate of individuals in the experiment group was at an acceptable level.
Keywords: Breast cancer, Trial, Self-examination, Physical examination, Yazd, Iran
Introduction
Breast cancer is the most common cancer among women globally1 and one of the main concerns of societies, especially for women.2 According to the American Cancer Society report, breast cancer is diagnosed in about 1.3 million women annually worldwide and around 465,000 will die from the disease.3 Present data is showing an increase in the annual incidence rates of the disease and is ranked as the first recorded malignancies among Iranian women since 1999. It is also ranked as the second cause of death in females of all cancer mortalities.4 Results of recent studies in Iran indicated that the age of onset of breast cancer is about 10 years earlier than the developed countries.5-8 Of the available cancer control measures for breast cancer, only screening has the potential for a rapid and major effect, though this will be restricted to a reduction in mortality rather than a reduction in incidence.9
Establishing population-based screening programs, including periodical mammography, breast examination (BPx) by a trained medical staff and monthly breast self-examination (BSE) is useful in detecting breast cancer at an early stage. BSE+BPx as simple non-invasive tests would be a suitable option for countries in economic transition, where incidence rates are on the rise and limited resources do not permit screening by mammography.10 Moreover, some studies have shown that annual mammography does not result in a reduction in breast cancer specific mortality for women aged 40-59 years compared with physical examination alone or the usual care in the community.11 This is the first report of community based trial of Yazd breast cancer project. It attempts to clarify whether BPx combined with BSE would reduce the cumulative incidence of advanced stage (stage 3 or worse) and mortality from breast cancer in a population of Yazd.
Materials and Methods
The present work is the first report of a multicenter community based intervention evaluating the effect of BSE+BPx on the reduction of morbidity and mortality of breast cancer. It is performed among the urban population of Yazd from 2008 to 2018. There are three distinctive phases in this trial with 10 years duration: phase-I included pilot of questionnaire (3 months) along with gathering the baseline data with 9 months duration, phase-II comprised of active intervention phase with 4 rounds of annual screening of BPx+BSE and phase-III involves follow up with 5 years duration.
Following project approval by the Deputy for Research Affairs and the Ethics Committee of Shahid Sadoughi University of Medical Sciences, a pilot study for validating project questionnaire begun in November 2008. Subsequently, three months later, it was finalized and approved by the scientific committee of the project. Data from previous studies were used to calculate the required sample size. Considering 30% reduction in breast cancer mortality at a significance level of 0.05 (one-side) and a power of 0.9, a total of 12,660 women of 35-64 years age group (6,330 in the case group and 6,330 in the control group) were selected from four areas of Yazd. The required sample of each group was selected by the mode of multistage selection. At first, two health centers from middle socio-economic (SE) areas and two health centers from high SE areas of the city were selected in the form of stratified random sampling. Then, from each SE area, one was randomly assigned as the intervention group and other as the control group. Appropriate to the number of women in the age group of 35-64 years living in each area, the allocated size was divided into clusters (urban blocks). Finally, the required number in each cluster was selected by determining the head cluster to complete the sample size (table 1). The exclusion criteria were having a personal history of breast cancer or detection of the disease at the beginning of the study, residing in the city of Yazd for less than five years, suffering from severe illness expecting survival of less than 10 years, and disaccord to attend the designated center for annual evaluation.
Table 1.
Stages of sample selection of eligible women age 35-64 years allocated to study groups
| Health center | Allocated group | Eligible women (N) | Proportionate sample size | Allocated cluster N (size) | |
|---|---|---|---|---|---|
| Imam shahr | Intervention (middle SE) | 5,340 | 3,750 | Total=6,300 | 5 (750) |
| Saffaeye | Intervention (high SE) | 3,856 | 2,550 | 3 (850) | |
| Azada share | Control (middle SE) | 4,386 | 3,750 | Total=6,300 | 5 (750) |
| Maskan | Control (high SE) | 3,184 | 2,550 | 3 (850) | |
| Total | 4 | 16,766 | 12,600 | 12,600 | 12 |
Tools of enquiry were a pre-tested pre-coded questionnaire, physical examination and paraclinical procedures such as mammography and fine needle aspiration. Personal identifying information was collected for both the case and control groups. Firstly, all individuals were visited at their homes and debriefed on the importance of breast cancer and the goal of the project. After obtaining written informed consent, personal information was collected.
Secondly, the participants in the case group were requested to attend a designated center to fill-in specific questionnaire followed by breast physical examination combined with training on self-examination of breast by skilled female general physicians. The flow diagram in figure 1 represents the follow up steps of the participants in the case group.
Figure 1.
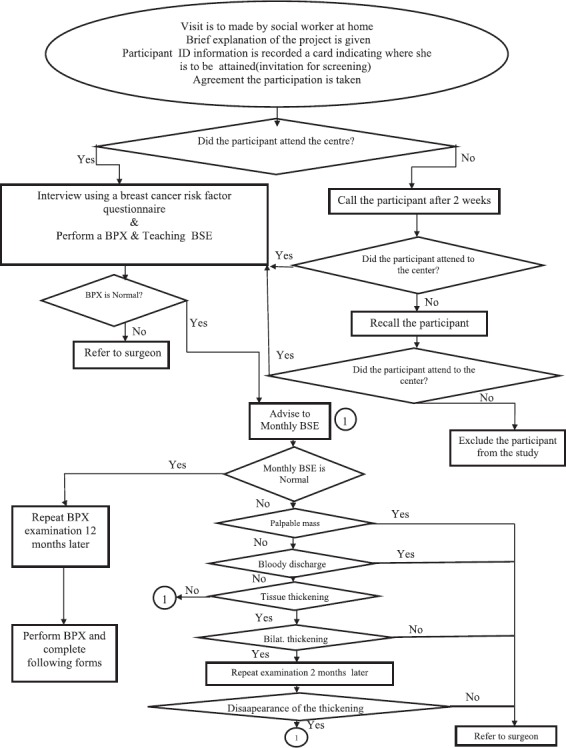
Shows the follow up flow diagram of intervention group attending health centers.
Morbidity and mortality data of the individuals in the control group were enquired yearly by phone and adjusted with the active registry systems of “cancer and death events” available at the deputy for health affairs of the university.
Main outcome measures of the study are a comparison of cumulative incidence of advanced (stage 3 or worse) breast cancer, the survival rate of breast cancer and mortality rate from breast cancer among the study groups. Evaluation and monitoring of the project were done weekly and monthly by the selected supervisors of the provincial deputy for health affairs, quarterly by the national supervisor of the program and by random control telephony of 5% of the filled questionnaire by the executive team of the program. Using the SPSS software, descriptive statistics such as frequencies, percent, mean (SD), tests of chi-square and student t-test with 95% confidence level were analyzed.
Results
Personal identifying information of a total 12,602 individuals in both groups (6,302 in experiment and 6,300 in control groups) was analyzed. Comparison of socio-demographic and socio-economic factors such as age, age at marriage, family size, number of live births, occupation, education level, total family income and marital status of the participants showed no significant difference between the groups (P<0.05). The majority of those were householders (90% experiments, 91% controls), lower education level (62.9% experiments, 67.4% of controls) and married (94.3% experiment, 94.1% control). The response rate of individuals from both groups, during the phase of primary data collection at their homes, was 100% and the response rate of 84.5% was noted for the intervention group visiting the assigned health centers to undertake breast physical examination.
Discussion
The efforts for controlling breast cancer at the level of primary prevention are limited to a few risk factors with marginal effectiveness. Consequently, the main attention and activity for the control of breast cancer have to be concentrated on secondary prevention level applying screening tests. Developing countries are showing an increase in the incidence of breast cancer, but they face inadequate resources to implement screening with high-cost equipment such as mammography.12 Since mammography is the only known effective screening test in reducing mortality from breast cancer, it requires expensive technology, highly trained radiologist, and radiographers, which is scarce in most developing countries.9 Breast physical examination (BPx) has been recommended as an alternative to mammography in these settings. In an unscreened population in Indonesia, BPx is known to be almost as effective as mammography in detecting prevalent breast cancers.12 Furthermore, in women under the age of 50, there is little evidence of a benefit at least in the first 10 years after screening is initiated,13 or if a benefit exists it is less in older women.9 Miller et al. also showed that annual mammography does not result in a reduction in breast cancer specific mortality for women aged 40-59 years compared with physical examination alone or with the usual care in the community.11 In this context, some commentators in the developed countries have strongly emphasized on the rationale in which screening by mammography should be urgently reassessed by policy makers.14 A greater benefit of early detection could be obtained in communities where most cancers that present clinically are larger and a higher proportion are node positive.15 In a study in Boston (USA), 80% first abnormally sign or symptom of cancer was reported by self-detected breast and only 6% abnormalities detected by clinical breast examination.1
In a study done in India, only 23.2% of women reported practicing BPx.16
A similar study was carried out in Yazd in which 92% of women heard about breast self-examination, but only 17.4% performed it monthly and only 4.7% with good performance.17
Data from the first year of our study showed that the response rate from participants in both groups with respect to data collection at their homes was 100% and for the participants in the intervention group visiting the assigned centers for the first breast physical examination was an acceptable level of 84.5%. These indicate that our study settings, design, and methodological manner were at a favorable level.
On the one hand it is known that Iran has a high number of mortality with an increasing incidence rate of breast cancer.18,19 Additionally, marginal practice by Iranian women results in late attendance by health centers. On the other hand, availing some evidence suggests that a benefit might be derived from a program that incorporated both annual BPx and BSE. Consequently, Yazd province was selected as a national site for the community based trial of breast cancer. It is anticipated that the obtained results and experiences from this trial would generalize to other parts of the country.
Our study limitations were migration of few participants and loss of contact due to change in phone numbers that resulted in limited serial follow up and unavailability of national identification number. Further details of the results obtained from annual follow-ups and related outcomes will be presented in the next reports.
Conclusion
Our data show that difference of socio-demographic and socio-economic factors between the groups were not statistically significant. In addition, with response rates of 100% in collecting the primary information at the homes of the participants as well as 84.5% for the experimental group in visiting the assigned centers for the first breast physical examination, it is fair to claim that our study settings, design, and methodological manner were at a favorable level.
Acknowledgment
This work was partly sponsored by a research grant from the Deputy of Research Affairs, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
Conflicts of Interest: None declared.
References
- 1.Norlaili AA, Fatihah MA, Daliana NF, Maznah D. Breast cancer awareness of rural women in Malaysia: is it the same as in the cities? Asian Pac J Cancer Prev. 2013;14:7161–4. doi: 10.7314/APJCP.2013.14.12.7161. [DOI] [PubMed] [Google Scholar]
- 2.Hirai A, Abe T, Taya K, Kurihara M, Chiu WC, Ochiai T, et al. Validity of estimating left ventricular relaxation and filling dynamics by Doppler trans-mitral flow. J Cardiol. 1989;19:1137–45. [PubMed] [Google Scholar]
- 3.The Women’s Health Resource. Breast cancer: statistics on incidence, survival, and screening. [cited 2008 Jan 23]. Available from: http://www.imaginis.com/breast-health/breast-cancer-statistics-on-incidence-survival-andscreening-1 .
- 4.Lotfi MH, Charkhatti S, Shobairi S. Breast cancer risk factors in an urban area of Yazd city- Iran, 2006. Acta Med Iran. 2008;46:253–7. [Google Scholar]
- 5.Kolahdoozan S, Sadjadi A, Radmard AR, Khademi H. Five common cancers in Iran. Arch Iran Med. 2010;13:143–6. [PubMed] [Google Scholar]
- 6.FarshbafKhalili A, Shahnazi M, Ghahvechi A, Torabi Sh. Performance conditions of breast cancer screening methods and its efficient factors among women referring to health centers of Tabriz. Iran J Nurs Res. 2009;4:27–38. Persian. [Google Scholar]
- 7.Mousavi SM, Montazeri A, Mohagheghi MA, Jarrahi AM, Harirchi I, Najafi M, et al. Breast cancer in Iran: an epidemiological review. Breast J. 2007;13:383–91. doi: 10.1111/j.1524-4741.2007.00446.x. [DOI] [PubMed] [Google Scholar]
- 8.Harirchi I, Ghaemmaghami F, Karbakhsh M, Moghimi R, Mazaherie H. Patient delay in women presenting with advanced breast cancer: an Iranian study. Public Health. 2005;119:885–91. doi: 10.1016/j.puhe.2004.11.005. [DOI] [PubMed] [Google Scholar]
- 9.IARC Handbooks of Cancer prevention. Breast cancer screening. Lyon: IARCPress; 2002. [Google Scholar]
- 10.Yadollahie M, Simi A, Habibzadeh F, Ghashghaiee RT, Karimi S, Behzadi P, et al. Knowledge of and attitudes toward breast self-examination in Iranian women: a multi-center study. Asian Pac J Cancer Prev. 2011;12:1917–24. [PubMed] [Google Scholar]
- 11.Miller AB, Wall C, Baines CJ, Sun P, To T, Narod SA. Twenty five year follow-up for breast cancer incidence and mortality of the Canadian National Breast Screening Study: randomised screening trial. BMJ. 2014;348:g366. doi: 10.1136/bmj.g366. [ PMC Free Article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kardinah D, Anderson BO, Duggan C, Ali IA, Thomas DB. Short report: Limited effectiveness of screening mammography in addition to clinical breast examination by trained nurse midwives in rural Jakarta, Indonesia. Int J Cancer. 2014;134:1250–5. doi: 10.1002/ijc.28442. [DOI] [PubMed] [Google Scholar]
- 13.Miller AB, To T, Baines CJ, Wall C. The Canadian National Breast Screening Study-1: breast cancer mortality after 11 to 16 years of follow-up. A randomized screening trial of mammography in women age 40 to 49 years. Ann Intern Med. 2002;137:305–12. doi: 10.7326/0003-4819-137-5_Part_1-200209030-00005. [DOI] [PubMed] [Google Scholar]
- 14.Stark A, Kleer CG, Martin I, Awuah B, Nsiah-Asare A, Takyi V, et al. African ancestry and higher prevalence of triple-negative breast cancer: findings from an international study. Cancer. 2010;116:4926–32. doi: 10.1002/cncr.25276. [ PMC Free Article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Vona-Davis L, Rose DP. The influence of socioeconomic disparities on breast cancer tumor biology and prognosis: a review. J Womens Health (Larchmt) 2009;18:883–93. doi: 10.1089/jwh.2008.1127. [DOI] [PubMed] [Google Scholar]
- 16.Grosse Frie K, Ramadas K, Anju GA, Mathew BS, Muwonge R, Sauvaget CS, et al. Determinants of participation in a breast cancer screening trial in trivandrum district, India. Asian Pac J Cancer Prev. 2013;14:7301–7. doi: 10.7314/apjcp.2013.14.12.7301. [DOI] [PubMed] [Google Scholar]
- 17.Bokaie M, Lotfi MH. Performed a Qualitative and Quantitative of Breast Self-Examination: a Checklist Approach. JCHR. 2013;2:107–16. [Google Scholar]
- 18.Naghavi M, Abolhassani F, Pourmalek F, Lakeh M, Jafari N, Vaseghi S, et al. The burden of disease and injury in Iran 2003. Popul Health Metr. 2009;7:9. doi: 10.1186/1478-7954-7-9. [ PMC Free Article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Harirchi I, Kolahdoozan S, Karbakhsh M, Chegini N, Mohseni SM, Montazeri A, et al. Twenty years of breast cancer in Iran: downstaging without a formal screening program. Ann Oncol. 2011;22:93–7. doi: 10.1093/annonc/mdq303. [DOI] [PubMed] [Google Scholar]