

Abstract
The present review classifies and describes the multifactorial causes of anterior cruciate ligament (ACL) surgery failure, concentrating on preventing and resolving such situations. The article particularly focuses on those causes that require ACL revision due to recurrent instability, without neglecting those that affect function or produce persistent pain. Although primary ACL reconstruction has satisfactory outcome rates as high as 97%, it is important to identify the causes of failure, because satisfactory outcomes in revision surgery can drop to as much as 76%. It is often possible to identify a primary or secondary cause of ACL surgery failure; even the most meticulous planning can give rise to unexpected findings during the intervention. The adopted protocol should therefore be sufficiently flexible to adapt to the course of surgery. Preoperative patient counseling is essential. The surgeon should limit the patient’s expectations for the outcome by explaining the complexity of this kind of procedure. With adequate preoperative planning, close attention to details and realistic patient expectations, ACL revision surgery may offer beneficial and satisfactory results for the patient.
Keywords: ACL reconstruction, ACL revision, Allografts, Autografts, Failure of ACL reconstruction, Instability, Pain, Review
Introduction
The incidence rate of ACL rupture has recently been reported to be between 36.9 and 60.9 per 100,000 persons/year (1, 2). In the United States, approximately 200,000 ACL ruptures occur annually (3). Historically, ACL reconstruction has been a successful operation, with satisfactory outcomes in 75% to 97% of patients (4, 5). However, with the number of primary procedures being performed increasing each year, the absolute number of graft failures after ACL repair is also rising.
No universally accepted definition for failure of an ACL reconstruction exists. It may be easier to reach a definition of ACL reconstruction failure based on instability, but there are other factors to consider as well. The surgery may be considered to have failed when objective laxity or patient perception of instability develops in a previously ACL-reconstructed knee, or when postoperative pain and/or stiffness occur in a stable ACL-reconstructed knee. Extensor mechanism dysfunction and infection can also result in failure (6,7). A very detailed definition of ACL-reconstruction failure has been published by Noyes and Barber-Westin (8). Their indications for revision surgery are: (1) a complete graft tear with > 6 mm of anterior tibial displacement as compared to healthy knee; (2) a positive pivot shift test graded +2 or +3 compared to the healthy knee, with or without knee pain or inflammation, or subjective sensation of instability or functional limitations for daily life and/or sports activities. Alford and Bach reported that more than 3 mm difference in anteroposterior knee laxity compared to healthy knee or an absolute displacement of >10 mm assessed through the KT-1000 arthrometer (MEDmetric, San Diego, California) represented valid signs of ACL graft rupture with a 99% sensitivity (9).
Failure of ACL reconstruction is of great concern to orthopaedic surgeons. ACL reconstruction is an effective surgery with 75% to 90% of patients reporting good or excellent outcomes (10, 11). Yet, a significant number of patients (10% to 15%) will require a revision. Clasically literature showed that ACL-reconstruction failures are primarily caused by technical mistakes (estimated at around 70%), chronic or acute traumatisms, and biologic causes (10,11). A recent Multicenter ACL Revision Study (MARS) Group developed a multi-surgeon, multicenter prospective longitudinal study to allow multivariable analysis and determine predictors of clinical outcome in revision ACL (12). The MARS cohort (460 patients) showed that mode of failure, as deemed by the revising surgeon, was traumatic (32%), technical (24%), biologic (7%), combination (37%), infection (<1%), and no response (<1%) (12).
The purpose of this article is to review the current knowledge about ACL reconstruction failure, describe in detail its multifactorial etiology, discuss current treatment options and show potential prevention strategies. Special attention will be given to elements that can be controlled by the orthopaedic surgeon, such as graft selection, graft fixation methods and tunnel placement (13).
Preoperative planning
The preoperative planning for the revision of a previous ACL reconstruction is based on a thorough medical history, including information on the primary surgical procedure, the physical exam, the imaging studies, and technical considerations of the surgical technique. Most of the factors that should be considered during the initial approach to a patient with ACL graft failure are shown in [Table 1] (6, 8, 14). Laboratory tests are not included in our table but may be also helpful in some cases to detect infectious or inflammatory processes (15-28).
Table 1.
Relevant history data for the preoperative planning
| PRIMARY PROCEDURE |
| Injury: date, mechanism of injury, symptoms |
| Surgery: date, surgical technique, graft choice, fixation methods, associated injuries, other surgical procedures |
| Postoperative: complications, rehabilitation, return to sports |
| Recurrence: date, mechanism of injury, signs and symptoms (instability/pain/stiffness/knee effusion) |
| PHYSICAL EXAM |
| Inspection: scars, swelling, muscle atrophy, lower limb alignment, gait |
| Palpation: temperature, knee effusion, trigger points, catching, locking, crepitation |
| Function: range of motion, knee strength |
| Special tests: anteroposterior stability (Lachman test, anterior drawer), rotational stability (pivot shift sign test), and mediolateral stability (valgus-varus test), meniscal tests |
| IMAGING STUDIES |
| Plain radiographs (standing anteroposterior view, lateral view at 30º of knee flexion, axial view at 45º of knee flexion [Merchant’s view], standing posteroanterior view at 45º of knee flexion [Fick’s view], functional radiographs): assess lower limb alignment, position of tunnels, tunnel widening, fixation methods, degree of knee osteoarthritis and associated instabilities |
| MRI: assess knee effusion, graft preservation, tunnel preservation, cartilage damage, and meniscal injuries |
| Bone scintigraphy Tc99: degree of knee arthropathy, complex regional pain syndrome, infection |
| CT scan: bone abnormalities, previous tunnels size |
| TECHNICAL CONSIDERATIONS |
| Graft choice: allograft versus autograft, soft tissue tendons versus bone-tendon grafts, ipsilateral versus contralateral graft |
| Surgical technique: all-arthroscopic versus outside-in, single-bundle versus double-bundle, transtibial versus anatomic. |
| Removal of hardware: fluoroscopy, universal set of instruments |
| Other procedures: high tibial osteotomy, treatment of cartilage injuries, meniscectomy vs meniscal repair, meniscal transplant, posterolateral corner injuries, medial collateral ligament |
Etiologic Classification of Failure of ACL Reconstruction
Johnson and Fu identified the three primary clinical signs and symptoms that lead us to consider an ACL reconstruction as a failure: instability, stiffness, and pain [Figure 1] (6). A deficient postoperative rehabilitation program alone can result in an ACL-graft failure despite a correct primary surgery. Additionally, even when there is no identifiable cause, an ACL reconstruction can be considered a relative failure when the outcomes – as indicated by patient-based outcome measures – do not correspond with the patient’s expectations. This generally corresponds with the practice of an athletic activity or sport. The possible causes of ACL reconstruction failures are listed and discussed below in [Table 2].
Figure 1.
Etiologic factors of the failure of ACL reconstruction.
Table 2.
Etiologic classification of failure of ACL reconstruction
| 1. INSTABILITY | |
| Abnormal mechanical loads | Acute traumatic event |
| Chronic repetitive movement | |
| Inappropriate accelerated rehabilitation postoperatively | |
| Non-anatomical tunnel placement | Anterior femoral tunnel |
| Posterior femoral tunnel | |
| Anterior or posterior tibial tunnel | |
| Vertical femoral tunnel | |
| Medial or lateral tibial tunnel | |
| Misdiagnosed associated injuries | Medial collateral ligament |
| Posterolateral corner | |
| Posterior cruciate ligament | |
| Failure of graft fixation | Failure of fixation method |
| Failure of graft tension | |
| Failure of graft isometry | |
| Failure of graft selection | |
| Failure of graft incorporation | |
| Failure of graft due to infection | |
| 2. STIFFNESS | |
| Primary | |
| Secondary | Inappropriate rehabilitation postoperatively |
| Deficient surgical technique | |
| Surgery at acute phase of injury | |
| Infection | |
| Complex regional pain syndrome | |
| Synovitis and hematoma | |
| 3. PAIN | |
| Patello-femoral pain | |
| Donor site pain | Patellar tendon |
| Hamstrings | |
| Femoro-tibial osteoarthritis | |
| Residual meniscal tears | |
| Synovial disease | |
| Neuroma | |
| Complex regional pain syndrome | |
Instability
Recurrent instability is defined as failure of the reconstructed ligament to provide adequate anterior and/or rotatory stability to the knee. Various etiologies of recurrent instability have been identified [Table 2]. Additionally, they can be divided into two main groups regarding the onset: early (<6 months) or late (>6 months) instability (7).
Instability secondary to abnormal mechanical loads
Well positioned or not, abnormal mechanical loads may damage an ACL graft, through either an acute traumatic event (traumatic rupture) or chronic repetitive micro-traumatisms (non-traumatic ruptures). Instability after ACL reconstruction can be precipitated by an acute rupture or loosening of the graft, stresses of daily life, or a sports accident. These can occur in patients with adequate or inadequate graft function.
Traumatic failure of ACL reconstructions has been estimated to occur in between 5% and 10% of cases (28). However, the true incidence is probably higher, as shown above with the MARS cohort (12). Other authors have reported as high as 43% of cases of ACL-reconstruction failure were a consequence of an acute traumatic event (22-29).
Harner et al. included early and aggressive rehabilitation as causes of traumatic failure of ACL reconstruction (30). Clancy observed in animals that the graft is undergoing intense biological bone incorporation and vascularization between 6 and 12 weeks, thus aggressive rehabilitation and/or increased physical activity in this early postoperative phase may increase the risk of injury of the graft (31). Indeed, this has been supported in human patients as well. During the first year after the ACL reconstruction, the strength and resistance of the graft are only 30% and 50% of the original ACL, respectively (31, 32). Excessive loads in this period may induce a plastic deformity and a lengthening of the graft.
Chronic repetitive micro-traumas may cause graft loosening that leads to failure. According to a review by Karmath et al., the cause of failure in 24% to 100% of cases was repetitive trauma (7). The failures are due to chronic repetitive micro-traumatisms, often related to inadequate surgical technique and non-anatomical tunnel placement (29, 33-35).
Instability secondary to non-anatomical tunnel placement
The influence of non-anatomical tunnel placement on knee stability has been clearly identified (36-43). Karmath et al. reviewed the literature regarding results after revision ACL reconstruction and reported that technical errors accounted for 22% to 79% of failure cases and 70 to 80% of these may involve non-anatomical tunnel placement (3, 7).
Inadequate reproduction of the native ACL anatomical footprints of either the femoral, tibial or both tunnels may increase graft stress and produce modifications in graft length and tension. From the MARS cohort, femoral tunnel malposition was reported to be the most common technical failure (80%), followed by tibial tunnel malposition (37%)(12). Note the denominator is > 100% because surgeons were instructed to ‘‘check all that apply’’ (43).
Errors in sagittal plane
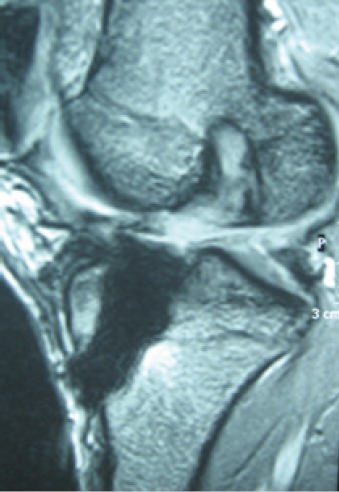
The placement of the femoral tunnel too anterior in the sagittal plane is the most common technical mistake related to bone drilling that may cause a failure of ACL reconstruction [Figure 2] (44).
Figure 2.
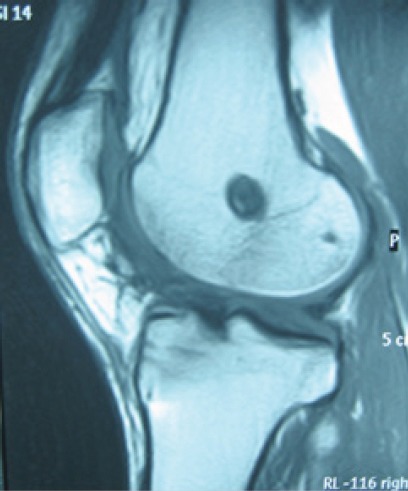
Excessive anterior femoral tunnel location (MRI sagittal view).
Some authors have postulated that the transtibial drilling technique may lead to non-anatomic femoral tunnel placement because the tibial tunnel drives the surgeon to a more anterior aspect of the femoral ACL footprint (6, 28, 29, 45). The drilling of a poorly placed anterior femoral tunnel may also result from an insufficient visualization of the posterior wall, or its confusion with the “resident’s ridge”, which separates both fascicles of the native ACL. Even small changes in the placement of the femoral tunnel towards the tibial center of rotation may impact the kinematics of the knee (42, 46-48). A graft fixed at knee extension in a femoral tunnel drilled too anteriorly may: (1) lead to a very tightened graft when the knees flexes, reducing the range of knee flexion, or (2) lead to graft stretching and resultant laxity of the graft (36, 49, 50). If the graft is fixed and tightened at knee flexion, then the graft will be loose at knee extension. Furthermore, if the tibial tunnel is excessively anterior, additional impingement of the graft into the superior aspect of the inter-condylar groove may occur. Nonetheless, a recent study found that failure due to excessively anterior tunnel placement is a predictor of a better result in the subsequent ACL-revision reconstruction, as avoiding tunnel overlap becomes easier to achieve during surgery (44) [Figure 3].
Figure 3.
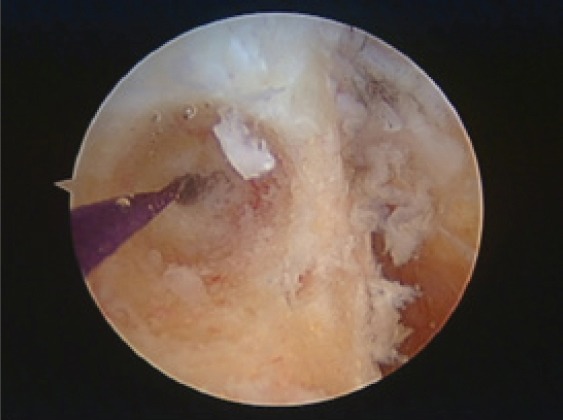
Suitable femoral tunnel positioning leaving 2 mm of posterior wall (arthroscopic intraoperative view).
When the femoral tunnel is too posterior, the graft may tighten in knee extension and have laxity on flexion; this may cause eventual weakness. If the graft does not break, then the knee may adapt to this circumstance by creating a knee flexion contracture with a deficit of complete extension. The biomechanical effect of this could impair the gait and cause anterior knee pain due to overload of the patello-femoral joint. In this case, graft fixation can be done in extension to compensate for the tunnel malposition, but the deficit of knee flexion may still develop (47).
Originally, less importance was given to the position of the tibial tunnel with respect to its contribution to postoperative outcomes because of a wide area of isometry in the sagittal plane (37-40). The orientation of the tibial tunnel in the sagittal plane should allow the fibers of the ACL graft to be parallel to Blumensaat’s line when the knee is in extension [Figure 4].
Figure 4.
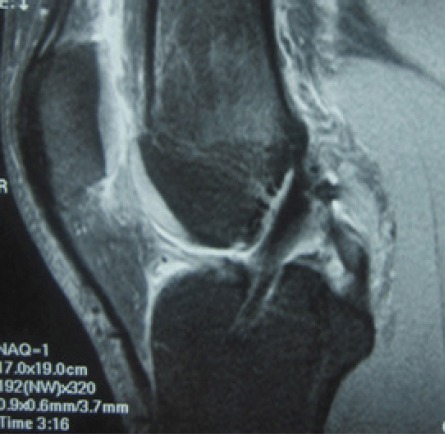
Posterior location of the tibial tunnel showing ACL reconstructed fibers non-parallel to the Blumensaat line.
To achieve this orientation, it has been suggested that the tibial tunnel should be placed in the anteromedial fibers of the native ACL footprint (30, 37-39, 51, 52). However, other authors defend the placement of the tibial tunnel in the posterolateral fibers of native ACL footprint to prevent the risk of impingement on extension and/or contracture on knee flexion (30, 38, 39, 41, 51, 53) [Figure 5].
Figure 5.

Intraarticular guide pin exiting at the anteromedial aspect of the ACL tibial footprint (arthroscopic intraoperative view from AL portal).
As stated before, a tibial tunnel too anteriorly placed may produce an impingement between the graft and the superior aspect of the inter-condylar notch when the knee is in extension. Consequently, the increased tension may interfere with the biological incorporation of the graft, may cause a cyclops syndrome or may cause a loss of knee extension (26, 37, 39, 51, 54-59). A tibial tunnel overly posterior may result in impingement against the posterior cruciate ligament and cause an excessive knee laxity in flexion and knee stiffness in extension. However, in patients with “genu recurvatum,” the placement of a more posterior tibial tunnel than usual may be indicated. This may also necessitate additional reaming of the superior aspect of the inter-condylar notch to achieve a complete range of motion and prevent the impingement of the graft in extension (37, 55, 60).
Errors in the coronal plane
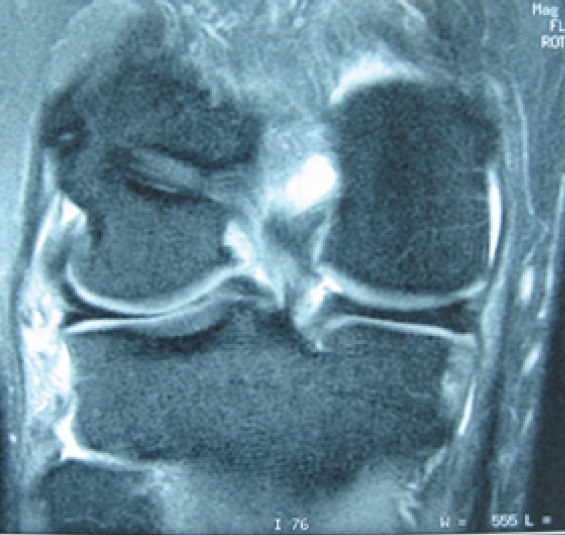
With regards to the coronal plane, a centered and vertical femoral tunnel (near 12 o’clock instead of 10 or 1 o’clock position) may restore anteroposterior stability but produce a rotational instability with a positive pivot shift test (61,62) [Figure 6]. A tibial tunnel placed too medially may produce an impingement of the graft with the medial femoral condyle and the posterior cruciate ligament. On the other hand, an excessively lateral position of the tibial tunnel may generate an impingement of the graft with the internal aspect of the lateral femoral condyle and create a rotational instability. Both of these occurrences may produce injuries to the tibial plateau cartilage when the drilling is performed (13, 34, 38, 51, 63, 64). Table 3 summarizes the most common mistakes in the placement of both femoral and tibial tunnel and the consequences on the graft.
Figure 6.

Verticalized femoral tunnel using transtibial technique for ACL reconstruction (coronal sequence on MRI).
Special consideration: Double-bundle ACL reconstruction technique.
Table 3.
Summary of common mistakes in femoral and tibial tunnel placement and its consequences on the graft
| Tunnel | Position | Consequences on the graft |
|---|---|---|
| Femoral | Anterior | Excessive tension in flexion or stiffness in extension |
| Posterior | Excessive tension in extension or laxity in flexion | |
| Central/Vertical | Rotational instability | |
| Tibial | Anterior | Excessive tension in flexion or impingement against intercondylar notch in extension |
| Posterior | Excessive tension in extension or impingement against the posterior cruciate ligament | |
| Medial | Impingement against the medial femoral condyle or against the posterior cruciate ligament | |
| Lateral | Impingement against the lateral femoral condyle |
An anatomic reconstruction that restores normal knee function may deliver better results and decreased rates of instability. Some surgeons argue that a double-bundle reconstruction of the ACL restores native knee biomechanics more effectively, although there is still no consensus over the technique of choice. Both cadaveric and in vivo studies have demonstrated greater rotational knee stability with the double-bundle technique compared to the single-bundle ACL reconstruction (65-67). However, these results have not been consistently reproduced in all studies and the overall additionally, overall functional differences between the techniques have not been clearly identified (66). A recent meta-analysis found a potential benefit in adding a posterolateral bundle to ACL reconstructions (68). This is suggested by statistically significant differences between single- and double-bundle reconstruction for anterior-posterior laxity, as measured by KT arthrometer and Lachman test, and for rotational laxity, as measured by manual pivot-shift test (65). However, no significant differences in outcome measures were found among techniques when validated patient-reported outcome measures were used (68). Potential pitfalls of the double-bundle ACL reconstruction are the greater complexity of the surgical technique, the greater likelihood of mistakes in the tunnel placement, the lack of consensus on the tension of both fascicles, or the rupture of the bone bridge between tunnels. When a patient has a tibial or femoral ACL insertion site of less than 14 mm in diameter, a double-bundle reconstruction can present a challenge, and thus a single-bundle reconstruction may be indicated. The size of the harvested tendon dictates the tunnel size, and could potentially limit the option for double-bundle reconstruction. Other indications for single-bundle reconstruction are open physes, severe bone bruising, a narrow notch, arthritic changes, and multiple ligamentous injuries (69). The use of double-bundle ACL reconstruction makes the revision surgery of failed reconstructions difficult because of the greater number of tunnels and because of the widening of the tibial ACL footprint. Also, it is questionable whether double-bundle ACL reconstruction protects the menisci and reduces the development of knee osteoarthritis more than the anatomic single-bundle reconstruction. All these issues argue against the systematic use of the double-bundle ACL reconstruction.
Instability secondary to misdiagnosed associated injuries
When the ACL ruptures, an assessment of the rest of the ligaments of the knee cannot be omitted. Associated lesions can compromise the future of the graft due to residual instability. Lesions in structures such as the medial collateral ligament (MCL), lateral collateral ligament (LCL), posterolateral corner (PLC), posterior cruciate ligament (PCL) or the posterior capsule must be ruled out. In addition, procedures such as meniscectomies (especially involving the posterior horn of the medial meniscus) can alter knee biokinetics, which can increase the total load over the ACL.
Percentages reported in the literature vary, but it is estimated that more than 15% of ACL reconstruction failures may be a result of missing a diagnosis of an associated ligament, meniscus or cartilage lesion at the time of surgery. In 1995, Getelman et al. published a study of 26 cases of failed ACL revisions and reported that 15% (4/26) were due to accompanying posterolateral and anteromedial instabilities (33).
Medial collateral ligament
The association of ACL and MCL injuries (anteromedial instability) calls for a simultaneous action on both structures, as a failure of the MCL implies an increase in the tension on or loads of the ACL. The reported incidence of ACL failure after a missed collateral instability or malalignment is between 3% and 31% (43). Possible treatment options for MCL reconstruction are multiple and include the use of auto or allograft. The preferred technique for the senior author at our insitution is to reproduce the MCL anatomy through a medial knee approach centered over the medial femoral epicondyle with tendon allograft. The tunnels for the ACL reconstruction should be drilled first; the graft should then be fixed in the femur. The MCL is then addressed before tensioning and tibial fixation of the ACL reconstruction. MCL fixation to the medial epicondyle is executed, then the isometric point of the MCL is placed at the anteromedial surface of the tibia. A tunnel is drilled in the tibia for the graft to pass through and be anchored [Figure 7].
Figure 7.

A. Guide pins showing anatomic insertion points during MCL reconstruction with Achilles tendon allograft. B. Tibial tunnel drilling during MCL reconstruction with Achilles tendon allograft. C. Final fixation and tensioning at 30ª angle for MCL reconstruction with Achilles tendon allograft. The flexible guide is used for interference screw insertion. Anteriorly, the other half of the Achilles tendon allograft is shown exiting from the tibial tunnel created during the ACL concomitant reconstruction.
The MCL technique can also be varied, such as using a double-stranded semitendinosus autograft reconstruction technique for the MCL. The semitendinosus distal insertion is left attached to the tibia, and dissection is carried directly down to bone in the femoral footprint to allow for placement of a fully threaded cancellous screw and spiked washer or an interference screw fixation system. If severe anteromedial instability is present and the patient has previously undergone a medial menisectomy, an internal meniscal transplant may be considered (52).
Posterolateral corner
Posterolateral instability is probably the associated injury that is overlooked the most often. Gersoff and Clancy estimated that the incidence of posterolateral instability in patients with chronic ACL deficit is 10-15% (70). When the ACL and the posterolateral corner both fail, a simultaneous reconstruction is advised. The surgical treatment could include a primary repair of acute lesions or a delayed reconstruction of the LCL and popliteal tendon [Figure 8].
Figure 8.

Posterolateral corner reconstruction using Achilles tendon allograft. The distal graft is seen exiting through the anterolateral aspect of the proximal tibia.
Occasionally, when an extreme varus deviation and a lateral thrust are present, a valgus tibial osteotomy could be indicated to avoid a failure of the ACL graft from chronic repeated elongation (52, 71).
Posterior cruciate ligament
ACL and PCL injuries seldom present together and require careful decision-making when they do. Generally, it is best to reconstruct the PCL first and return the tibia to its anterior position; reconstruction of the ACL may be achieved in a subsequent surgery [Figure 9]. If by mistake, the ACL was fixed first in a posteriorly displaced tibia, it would predictably lead to ACL failure. The main reason to adopt this staged surgery is that the rehabilitation for ACL and PCL reconstructions differ. The PCL requires a slow rehabilitation concerning motion; the predominant work is on the quadriceps muscle. The ACL reconstruction benefits from early rehabilitation with specific work on the ischiotibial muscles, which are ACL agonists. However, some authors have reported satisfactory results with simultaneous ACL and PCL reconstructions (72-74).
Figure 9.

Arthroscopic intraoperative view of a monofascicular reconstructed PCL using Achilles tendon allograft.
Instability secondary to failure of graft fixation
Failure of the fixation method [Figure 10]
Figure 10.

AP view Xray showing different fixation methods in a patient with a previous history of multiple ACL reconstructions. In the femur, a metallic interference screw and a variation of suspensory cortical device is demonstrated. Fixation devices visualized on the tibia are a metal staple and a screw-post system with a spiked head.
Kurosaka et al. established that the weakest point of a fixation is the weakest link during the immediate postoperative period (75). For this reason, a solid fixation is essential to prevent changes in the position of the graft inside the tunnel, keeping in mind that bone-bone integration happens faster than soft tissue-bone integration (52).
The resistance of the fixation depends on the type of graft and fixation used and on the quality of the bone. The fixation of bone-patellar tendon-bone (BTB) is more secure and presents fewer problems than hamstrings fixation; however, the ideal placement of the bone plugs can present a technical challenge. For the BTB fixation, the interference screws have proven to be more effective than staples, posts or other devices (75,76). Yet, screws can pose problems at the time of fixation, such as being driven into the tunnel, divergence caused by the screw, rupture of the bone plug or screw, damage of tendinous fibers, among others. Usually, extra-cortical suspensory systems are employed for the fixation of the quadruple reconstruction of hamstrings, although interference screws and staples could also be used.
Failure of graft tension and isometry
An inadequate tension on the reconstruction at the time of fixation, either too much or too little, could be a reason for its failure. The ideal tension of the reconstruction at the moment of fixation depends on various factors including length, flexibility and elasticity of the graft, as well as on the preconditioning of the graft and the position of the leg during fixation (29). Along these lines, knee flexion angles that are not between 0° and 30° have a greater influence over the final strength of the graft than the applied tension from the surgeon (49, 77).
Yoshiya et al. in their experimental study on dogs, observed that, when increased tension diminished vascularization and incorporation of the graft was delayed, myxoil degeneration resulted (78). Another study measured the tension of ACL reconstructions after several cycles of knee flexion and found a significant early loss of graft tension despite a thorough preconditioning protocol (79). A lack of tension can result in a residual instability (52). Conversely, excessive tension on the reconstruction, especially with BTB technique, can increase articular pressure. The patient may interpret this as stiffness and pain; increased articular pressure may even lead to the development of arthritis
An ideal intra-operatory tension has yet to be defined (17). However, a recent meta-analysis found adequate evidence to suggest the ideal amount of tension for an ACL reconstruction, using hamstring–polyester graft, is 80 N. For reconstructions using semitendinosus-gracillis tendon (ST-G) or patellar tendon grafts, no consensus exists for the ideal graft tensioning (80). Jaureguito and Paulos recommend a tension of 2.3 - 4.5 kg (5-10 lbs.) for the BTB technique, at a knee flexion of 10°-15°(25). Hamstrings are fixed with a greater tension 4.5 - 6.8 kg (10-15 lbs.) with the knee at 20°-30° of flexion. With an even more practical approach, Howe et al. established that the tension applied to the graft at the moment of fixation should be enough to eliminate the anterior displacement of the tibia while allowing complete knee motion (17).
Once the graft is fixed to the femur, repeated flexing-extending cycles of the knee must be done in order to preinstall the graft before the fixation (81). This reduces the elongation of the graft after fixation and allows the surgeon to verify that the graft does not have any movement at the tibial exit, proving that it is at an isometric position. Before tibial fixation, the tension of the graft is tested with the probe under arthroscopic control and the surgeon’s perception must be that the tension is the same or very close to the one felt with a normal ACL.
Regarding the double-bundle techniques, the dynamic role of the anteromedial and posterolateral bundles in stability at different angles of flexion is not clear. The anteromedial bundle has a constant tension from complete extension to 90° of flexion, whereas the tension of the posterolateral bundle decreases at greater angles of flexion (82).
Instability secondary to failure of graft selection
Recently, systematic reviews on randomized prospective studies that compare the hamstrings with BTB grafts have suggested that the type of graft is not the main determining factor for success in ACL reconstructions. These studies confirm that the use of hamstrings prevents anterior knee pain, while patellar tendon grafts offer more stability (83).
Since most of the failures are a result of technical errors and not of graft choice, the surgeon’s technical experience is of most importance. The autograft BTB technique has been the gold standard for many years; nevertheless, the use of the quadruple ST-G graft has gained popularity [Figure 11; Table 4]. shows the pros and cons of each type of autograft. Other possibilities, though used less often, are the quadriceps tendon and iliotibial band.
Figure 11.
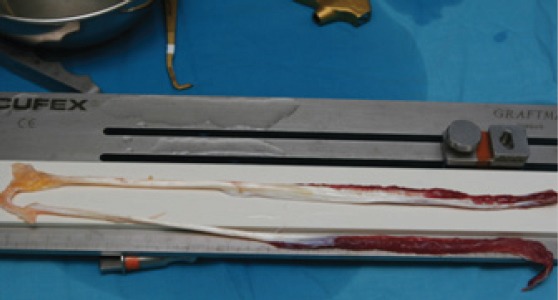
Autologous hamstrings tendons prior to preparation and inmediately after extraction.
Table 4.
Fundamental differences classically associated to the use of BTB or ST-G autografts
| Pros | Cons | |
|---|---|---|
| BTB | - Fixation with osseous plug - Greater revascularization capacity - Less failure - Greater tensional strength - Better flexion - Faster and more vigorous return to sports - Better Tegner Score |
- Anterior knee pain - Late arthritis, specially patellofemoral - Kneeling difficulty - Knee flexion and extension difficulty - Less strength at extension (first 6 months) - Patellar tendon shortening - Sensation reduction in medial region - More demanding technique - Skeletal immature patients |
| ST-G | - Extension ease - Less anterior knee pain - Less kneeling pain |
- Reduction in flexion strength (first 6 months) - Posterior knee pain - LCA agonist muscles weakening - Bone-soft tissue fixation - Tunnels widening - Internal saphenous neuromas - Hematomas |
Among the advantages of the autograft are faster integration to bone and no risks of disease transmission or immune reactions. Nonetheless, the morbidity at the site of extraction as well as the potential limitations of the size of the graft are worth discussing. Additionally, the use of autografts imposes a limitation in the chance that revision surgery is required. In these cases, ipsilateral BTB grafts are often the choice if it has not been previously used in the primary surgery; if it has, the contralateral BTB can be used (84,85). The repeat use of BTB or of quadruple ST-G have also succeeded, although there are doubts about the mechanical properties of the re-extracted autograft. For this reason, reuse is not advised (52, 84, 86-90). Yet Rubinstein et al. have used re-extracted auto-graft without encountering greater complications (91). A history of patello-femoral problems in the patient should cause the surgeon to consider options other than the BTB autograft for ACL revision (45, 87, 92).
Incrasingly, allografts are being used in revision and primary surgeries. Among the potential graft choices are Achilles tendon [Figure 12], tibialis anterior, tibialis posterior, patellar tendon, quadriceps tendon, iliotibial band and hamstrings. They offer advantages such as decreased morbidity, absence of complications at the graft extraction site, shorter surgical time and more options for sizing and shaping of the graft. Among the worries are the biologic integration, the risk of transmitting diseases, the adjustment of the size to the receptor, and the availability and cost (93-99). Possible transmission of diseases is one factor that discourages the extended use of allografts, as the risk involved in fresh frozen allografts has not been completely extinguished. It is estimated that the infection risk is 1/1,000,000 cases, as long as the guidelines of the American Association of Tissue Banks are strictly followed. To eliminate this risk, a secondary sterilization with gamma ray radiation at 3 mrads may be of benefit; however, this dose may also weaken the mechanical properties of the graft, the integration rate and immunogenesis (93-97). For this reason, after sterile extraction, the allograft is quickly frozen at -80°C (-112°F); this eliminates the cellular viability but maintains mechanical properties of the tissue (100,101). Several studies have failed to identify significant differences between autografts and allografts at one-year follow-up (33, 34, 102-104).
Figure 12.

Achilles tendon allograft exiting through the tibial tunnel during ACL reconstruction. Tibial fixation was achieved using two 8-mm metal staples.
Therefore, because no graft has been shown to be ideal in all situations, each case must be individually evaluated. Factors such as the previous use of the graft, the condition and width of tunnels, the presence of patello-femoral symptoms, the presence of scars on the skin, and the patient’s preference, among others, should be taken into account. Rehabilitation should be individualized keeping differences in biologic behavior and integration times of the autografts and allografts in mind (52).
While popular in the 80s, artificial ligaments like Dacron and Gore-Tex have been discarded due to the great number of complications they developed, such as loosening and mechanical failure, synovitis, osteolysis, persistent pain and infections (92, 102, 103, 105-107). If one of these artificial ligaments must be removed, it should be done in whole. Remaining artificial ligaments could produce an inflammatory response resulting in widening of the tunnels and cartilage degeneration, possible necessitating a synovectomy. A staged procedure is frequently necessary, especially when there is an accentuated osteolysis and widening of the femoral tunnel (52).
Instability secondary to failure of graft incorporation
In the absence of surgical technical errors or subsequent trauma, when a knee with either an autograft or allograft ACL reconstruction becomes unstable, it is considered have a biologic failure of graft integration (45). It is well known that, once implanted, any auto or allograft undergoes biologic processes such as graft necrosis, revascularization, cellular repopulation, deposition of collagen fibers and remodeling, a process that is known as ligamentization (30, 54, 108). A delay in revascularization of the graft, due to excessive tension, inadequate postoperative immobilization, infection or immune reactions, postpones graft integration (76,108,109).
During the ligamentization phase the graft is particularly sensitive, requiring very careful rehabilitation; this is especially true when allografts are used (93, 110). In animal models, the ligamentous graft integration is slower than the BTB ones, although this has not been proven clinically (111).
Instability secondary to failure of graft due to infection
Infections should be classified under the category of biologic failure, though technical factors during the surgery or postoperative period could have an influence. Infection is rare in this surgery, with a 0.5% rate of occurrence, but it can be devastating when it occurs. The persistence of clinical signs such as fever higher than 38°-39°C (100°-102° F), elevated laboratory results (leukocytosis, high C-reactive protein (RCP) and erythrocyte sedimentation rate (ESR)), pain at the subquadricipital pouch and/or a knee effusion of infectious or inflammatory characteristics, should signal the immediate need for abdundant joint irrigation. Arthroscopic lavage and debridement with associated wide-spectrum empiric antibiotic therapy should be started while waiting for culture results. The decision to remove the graft should be made on an individual basis, although early lavage is often sufficient to resolve the issue. Factors for consideration include the extension of the infection, causal organism, type of graft (especially artificial) and the type of fixation. In cases of an irreversible deterioration of the graft, the revision surgery should not be considered until 6 weeks have passed, the laboratory values have returned to normal, and the signs and symptoms of infection have subsided (82, 112-114).
Stiffness
The most common complication after an ACL surgery is stiffness, with an incidence between 5.5% and 24%. Stiffness can result in deficits of knee motion (loss of flexion, extension or both), which could range from a few degrees to complete stiffness (24, 115,116).
Generally, the loss of extension produces functional problems, mainly because of secondary overload of the patello-femoral joint due to a flexed gait. Also, loss of extension makes it difficult to gain quadriceps strength, which worsens patello-femoral problems (24, 115). Depending on the patient’s lifestyle, a side-to-side extension deficit of more than 5° may lead to complications (117). A lack of flexion would only become significant during certain activities such as climbing stairs, crouching, sitting or kneeling.
There are two accepted causes of motion deficit and the subetiologies that originate from them. These two main groups, primary arthrofibrosis (adhesive capsulitis) and secondary arthrofibrosis, are discussed below (20, 24, 114).
Primary arthrofibrosis
Adhesive capsulitis or arthrofibrosis has been defined as a scarring process that occurs with the formation of adherences and fibrous tissue secondary to an inflammatory process or an intra-articular effusion of any etiology. Knees with adhesive capsulitis are very painful and have persistent inflammation, flexion or extension motion deficits (losses range between 10° in extension and 25° in flexion), patellar motion alterations, and low patella and infra-patellar contracture syndrome (20, 23, 26, 117).
Primary arthrofibrosis, by definition, does not have an identifiable cause. Histologically, primary arthrofibrosis is seen as an exaggerated endothelial proliferation and a disorganized disposition of the protein matrix caused by an activation and proliferation of fibroblasts. Additionally, a dense collagen deposition is common.
Secondary arthrofibrosis
Unlike primary arthrofibrosis, secondary arthrofibrosis has a specific cause that limits the motion of the knee and triggers an exaggerated scarring response.
Inappropriate rehabilitation postoperatively
Either excessive postsurgical immobilization or post-operative pain with repeated effusions could play an important role in the origin of arthrofibrosis. A soft, painless rehabilitation with avoidance of a large inflammatory reaction is advised. Ideal goals for short-term rehabilitation have not been defined, but postoperative knees should achieve complete extension and flexion of at least 90° by the fourth week, considering that the graft fixation allows a rapid complete extension. Otherwise, extension exercises should be increased over time.
Deficient surgical technique
As it was described in detail above, tunnel malposition can lead to extension and/or flexion deficits, or worse, lead towards progressive loosening of the graft (6, 28, 29, 45). Common causes for impingement are cyclops lesion, anterior tibial tunnel, inadequate trochleoplasty and large grafts (24, 53, 54, 115).
The Cyclops lesion consists of the anterolateral interposition of fibrous tissue in front of the tibial insertion of the new ligament, which will work as an end point during extension, thus limiting the last degrees of motion. Its formation can be minimized by carefully cleaning the rest of the cruciate ligament or by debridement during surgery. Adequate positioning of the tunnels will prevent the anterior impingement that could damage some fibers of the graft and form a Cyclops lesion (55).
MRI is indicated to evaluate a possible impingement on the graft (29, 47, 51). The grafts that remain friction free will appear with a homogenous low-intensity signal similar to tendons, whereas impinged grafts demonstrate an irregular increase of the signal and a narrowing of their inner substance (51). To avoid friction in the trochlea, milling of the notch must be adequate, so that complete flexion-extension can be achieved without contact with the graft.
Surgery at acute phase of injury
ACL surgery performed too soon after the injury (less than 4 weeks) is thought to increase the rate of arthrofibrosis. However, a study by Mayr et al. implicated a pre-existing inflammatory reaction of the knee or the previous articular balance of the knee as predictive factors for arthrofibrosis (118). Ideal preoperative knee status is pain free, has a complete articular balance and no inflammatory signs. If the surgery is performed in an acute phase, the immediate recovery period should be closely monitored; it is sometimes necessary to begin rehabilitation earlier. Particular attention is required for patients with an associated lesion of the MCL proximal site. This can be an extremely painful area and limit the rehabilitation process.
Infection
Postsurgical septic arthritis can provoke fibrous adhesions that would trigger arthrofibrosis. Treatment recommendations are stated above.
Complex regional pain syndrome (CRPS)
Complex regional pain syndrome (CRPS) when it occurs in the knee provokes articular stiffness at its latest stages and should be considered within the diferential diagnosis.
Synovitis and hematoma
Despite the unpredictable character some complications, some of them could be potentially minimized by paying careful attention to details such as patient selection, timing of the surgery, preoperative medication, and the application of a refined, precise, careful and sterile surgical technique. Immediate postoperative and rehabilitation care are also crucial; special emphasis is given to achievement of complete extension, patellar mobilization, quadriceps and ischiotibial strength gain and progressive weight bearing. Mechanical limitations of the graft should not be exceeded at any time.
No matter the cause of stiffness, its resolution in early phases must be oriented towards an intense, thorough, graft-preserving recovery. Tools at our disposal are continuous passive movement devices, casts or braces in extension, quadriceps and/or hamstring strengthening, passive mobilization and physiotherapy. Proper medical treatment can also minimize the pain and inflammatory process. The management of hemarthrosis and/or synovitis is also important in these cases, since important effusions could inhibit muscular activation of the quadriceps, producing an altered gait dynamic with loss of movement, especially at extension. In refractory cases, an arthroscopic arthrolysis must be performed, removing the abundant fibrous tissue recently formed and resecting possible cyclops lesions. If impingement is present, a trochleoplasty could be necessary. Action over the graft is rarely necessary. If the deficit is mainly in extension, a cast with the knee in extension for 24-48 hours must be placed following surgery. Once the mechanical factor is corrected a residual tension tends to develop in the posterior capsule (20, 24, 55, 115, 119).
On rare occasions, stiffness is great enough to render a reconstruction unnecessary. ACL graft resection could be advised to minimize the pressures on the articular cartilage and increase range of motion (20, 26, 117, 120).
Pain
Failure of ACL reconstruction surgery is not exclusively associated with stability. Other circumstances, such as persistent pain, may lead the patient to feel that a bad result was reached. Pain alone is rarely a cause for revision of the reconstruction. However, in refractory cases, reintervention might be needed.
Patello-femoral pain
Anterior knee pain is one of the most frequent complications after ACL reconstruction surgery, with an incidence that varies between 3 and 47% (19, 60). The existence of previous anterior pain, patello-femoral pre-existing lesions, flexion contracture, quadricep muscle weakness and aggressive rehabilitation with patellar tendon overload, will increase the risk of anterior knee pain (19, 121-123).
A specific case is the contracture of the patellar tendon accompanied with a low patella. This can be seen as part of the infra-patellar contracture syndrome, resulting in increased contact forces of the patello-femoral joint. Noyes and Barber recommended avoidance of use of patellar tendon grafts [Figure 13] in certain situations: cases of previous extraction, patients with severe patello-femoral chondropathy, patellar malalignment cases, professions requiring frequent kneeling position, narrow patellar tendon and in patients with previous patellar tendinopathy (93). Shelbourne and Trumper studied a group of 602 patients who had anterior cruciate ligament reconstructions with autologous patellar tendon graft and did not find any differences compared to a control non-operative group with regards to anterior knee pain (122). They suggested that the increased incidence of anterior knee pain with an autologous patellar tendon graft can be prevented by obtaining full knee hyperextension postoperatively.
Figure 13.
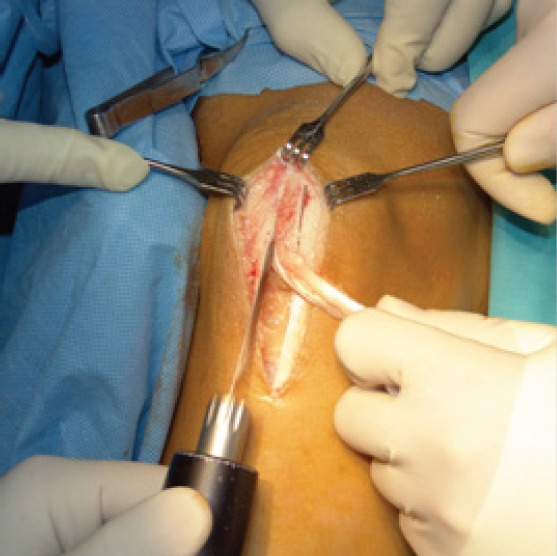
Intraoperative view during excision of bone-tendon-bone patellar tendon.
Tibio-Femoral Osteoarthritis
One of the main objectives of ACL surgery is stabilization of the knee to prevent premature knee wear down. Previous lesions or any initial trauma that could have caused cartilage, ligamentous or meniscal lesions or bone bruises may predispose the patient to develop arthritis. In a study using MRIs to examine 54 acute ACL lesions, the incidence of bone bruises was found to be as high as 80%, with 68% having a bone bruise in the internal region of the lateral femoral condyle and 54% in the posterolateral tibial plateau (124). Both scenarios are concerning for the potential to lead to arthritis in the future (124, 125).
Residual meniscal tears
Meniscal lesions are also frequent in patients with acute ACL tears (45% to 81% of cases) and slightly more frequent in the lateral meniscus. When meniscal lesions cannot be repaired it can predisposes the knee to develop arthritis (126-132).
Additionally, recurrent instability before or after the ACL reconstruction can compromise meniscal and cartilage tissue. The incidence of meniscal lesions in patients with chronic ACL instability is about 73% to 91%, with medial meniscus lesions occurring more frequently (128, 130). This is because the menisci function as secondary knee stabilizers, especially at the posterior horn of the medial meniscus (133, 134). Trojani et al. reported that patients who sustained a total meniscectomy before, during or after the primary or the revision reconstruction, had significantly poorer function and knee stability than the patients with conserved menisci (44). Moreover, a recent update from the MARS cohort reported that a previous partial menisectomy is associated with a higher rate of chondral changes at the time of revision, and that the incidence of chondrosis is lower after meniscal repair compared with menisectomy (135). This supports conserving or repairing the menisci, whenever possible, at the time of primary ACL reconstruction. These preexisting lesions are not always repaired in ACL surgeries and can be a source of patient dissatisfaction. The surgeon must be aware that, in such cases, revision surgery is unlikely to achieve a completely satisfactory result.
Relative Failure
Patient-Reported Outcome
Despite normal findings on physical examination, some patients may be unsatisfied with the outcome of the surgery, especially when unable to return to previous level of activity and/or competitiveness. In these cases, patient-reported outcome scales may reflect suboptimal results and help pinpoint the problem area (27, 28). Many subjective patient-reported outcome measures for knee disorders exist (136). Some surgeons believe these patient-based outcome scales have greater validity than clinical evaluation. Clinicians and researchers must assess an instrument’s utility based on its applicability to their patient population of interest (137). The recommended instruments for ACL assessment are the Cincinnati, KOOS and Lysholm scales (137).
Poor muscle control, relative stiffness, joint laxity and generalized soreness are problems seen in the postoperative setting, which may be independent of the reconstructed ligament and may not improve after revision surgery. ACL revision surgery is a demanding technique and often results are poorer than those of primary surgery (4, 34, 35, 52, 85, 104, 138-141), especially when assessed by various patient-reported outcome measures (142).
Difficulties such as cartilage and meniscal problems are reported in up to 90% of cases; varus alignment or ligament lesions can also affect results (4, 34, 35, 85, 104, 138, 143). Many experts consider ACL revision surgery as a rescue surgery, with its primary objective being to restore stability and function for every-day activities. The patient should be advised that return to sports is not always possible, but the completion of an intense rehabilitation will maximize outcomes (21, 144). Unrealistic expectations could turn a technically successful procedure into a subjective failure from the patient’s viewpoint (52, 113). For this reason, sedentary patients or those who are willing to modify their level of activity should be considered for more conservative treatment (145).
Rehabilitation Impact on ACL Failure
As stated above, a deficient postoperative rehabilitation program may explain many of the clinical signs and symptoms causative of failure. A poorly planned and executed rehabilitation program may lead to an ACL reconstruction failure by itself, even after a correct primary surgery.
With current rehabilitation techniques, the graft undergoes more cycles of flexion in the early postoperative stage than before, which increases the probability of failure. The process is often progressive and smooth until the failure is produced. Individual fibers start to fail; the volume of the ligamentous remnant decreases and could reduce the resistance of the graft. This contributes to elongation and failure of tenser fibers, leaving the knee with an abnormal anterior laxity.
Rehabilitation after ACL revision surgery must be different and more conservative than the aggressive protocols used for primary surgery. Patients must remember that results are less predictable and that they should not exceed the limits indicated for them. Each rehabilitation protocol must be individualized and based on the type of reconstruction performed, the strength of the fixation and the type of graft used. Using crutches when walking for 6 weeks is advised, is delayed return to intense activities (52).
Diverse studies have detailed key factors during functional recovery after ACL reconstructive surgery [Table 5] and certain protocols set standards to allow a patient to return to restricted activities or sports when specific criteria are met [Table 6] (146).
Table 5.
Key factors for functional recovery after ACL reconstruction surgery
| Active extension produces an important stress on the ACL graft. It must be performed with assistance during the first weeks limited from 30° to 0°. |
| Open chain exercises produce maximal shearing forces. |
| Close chain exercises do not produce stress on the ACL graft. |
Table 6.
Standard criteria for allowing patients to return to restricted activities or sports (160)
| Complete range of motion. |
| Quadriceps strength over 85% of contralateral side. |
| Hamstrings strength of 100% of contralateral side. |
| Good ischio/quad muscle balance over 70%. |
| One-legged jump of 85% of length of contralateral side. |
| KT-1000 measured difference of less than 3mm between knees. |
Revision ACL Surgical Tips
Establishing realistic goals and expectations is important, especially when the only evidence of a primary ACL reconstruction failure is patient dissatisfaction. In a study using the MOON cohort (Multicenter Orthopaedic Outcomes Network), researchers found that patients who underwent a revision ACL surgery usually scored poorer on patient-based subjective measures of outcomes and functionality compared with primary ACL reconstruction (147).
When ACL reconstruction has failed due to non-anatomical tunnel placement, one of the most important aspects of the revision surgery is to ensure adequate visualization of the previous tunnels and the integrity of the postero-medial wall of the lateral femoral condyle. Occasionally, trochleoplasty can be needed, especially with narrowing or osteophytes in the intercondylar notch. Once these previous steps have been conducted, drilling of the new tunnels may be performed as close as possible to their anatomical location. If possible, both tunnels should be placed far enough and divergent enough from previous tunnels to ensure adequate knee stability and prevent tunnel overlapping (4).
In order to avoid a previous non-anatomical femoral tunnel, an anteromedial parapatellar portal can be created in front of the medial femoral condyle and as low as possible; special care has to be taken to avoid damaging the medial femoral condyle and the anterior horn of the medial meniscus respectively. The drilling of the femoral tunnel should be performed with at least 90º of knee flexion in order to decrease the risk of damage to lateral neurovascular structures and to ensure proper tunnel length [Figure 14; 15].
Figure 14.
Anatomic positioning of the femoral tunnel (MRI coronal view).
Figure 15.

External intraoperative view showing a guide pin through the accessory anteromedial portal used for femoral drilling. An expanding tunnel device is shown inferiorly positioned and exiting from the tibial tunnel.
If the posteromedial wall of the lateral femoral condyle is insufficient, several surgical options still can be performed to create a new anatomic femoral socket: a) extra-cortical fixation with suspensory devices; b) over-the-top fixation through a lateral post; c) changing the orientation of the femoral tunnel through the use of an accessory anteromedial portal; d) using the classical open outside-in drilling technique 4; and e) new options such as retro-drilling arthroscopic outside-in technique.
Hardware removal is another factor to consider and should be planned in advance as it may involve intraoperative difficulties, longer surgery and a loss of bone stock;, thus hardware should only be removed when it is in the way of the new tunnels. Sometimes previous hardware can be useful in avoiding old tunnels when the new ones are drilled. New screws should be placed with caution, taking care that they do not enter into the old tunnels. If both communicate, the graft should be positioned in contact with the “healthy” wall instead of the old tunnel. When removal of previous interference screws is necessary, it is imperative to have an adequate screwdriver and to reproduce the degree of portal and knee flexion used during insertion. If previous screws are not removable, it is possible to drill over them if they are reabsorbable. If staples were used, it is strongly recommended to have the appropriate extractors and to consider the potential bone loss after removal, which could affect tibial fixation (52).
Two-stage revision surgery is necessary in cases of tunnel widening [Figure 16], synovial fluid fistulas through the tunnel or artificial grafts with severe synovitis. In such cases, an initial surgery may be performed to remove remnants of the previously reconstructed ACL and place the bone graft into the old tunnel [Figure 17]. Tunnel widening occurs more commonly when using soft tissue or synthetic grafts (4). This situation usually arises when the graft does not exactly match the tunnel width and may have been diminished by using interferential screws that locked the graft as close as possible to its entrance into the joint in both femur and tibia.
Figure 16.
Widened tibial and femoral tunnel (MRI sagittal view).
Figure 17.

Tibial tunnel filled with allograft cancellous bone chips
Two-stage revision surgery may also be needed with a ROM deficit of more than 5º in extension or 20º in flexion, as well as in cases of active infection. Two-stage revision usually requires a 4 to 6-month gap between procedures. Surgeon and patient have to be aware that this prolonged period of instability can produce secondary chondral and/or meniscal injuries (148). In general, what seems to provide the most influence on the lack of success of an ACL revision surgery is the association of factors like a complete or partial menisectomy, articular cartilage damage, or additional operative procedures (149).
Results
Revision anterior cruciate ligament (ACL) reconstruction is believed to have an inferior outcome compared with primary ACL reconstruction. The available literature on the outcome of revision ACL reconstruction is sparse compared with that for primary reconstruction. A recent systematic review from Wright et al. included twenty-one studies where 863 of the 1004 patients had a minimum of two years of follow-up and concluded that Revision ACL reconstruction resulted in a worse outcome compared with primary ACL reconstruction (150). Patient-reported outcome scores were inferior to previously published results of primary ACL reconstruction. A dramatically elevated failure rate was noted after revision ACL reconstruction, nearly three to four times higher compared with prospective series of primary ACL reconstruction.
Some of the collected data from this study showed that objective failure occurred in 13.7% ± 2.7% of the patients (95% confidence interval, 8.0% to 19.4%). The mean Lysholm score was obtained in 491 patients and was 82.1 ± 3.3 (95% confidence interval, 74.6 to 89.5) according to a mixed-model meta-analysis. The mean IKDC subjective score in 202 patients was 74.8 ± 4.4 (95% confidence interval, 62.5 to 87.0). The pooled demographic data were compared with data for the first 460 patients in the Multi-center ACL Revision Study (MARS) cohort (12). Demographics in the two studies were similar, with only minor differences.
This study also compared the pooled results of revision ACL reconstruction with those of large prospective studies and systematic reviews of primary ACL reconstruction that used the same outcome measures; both the mean Cincinnati and the mean Lysholm score were lower after revision ACL reconstruction than after primary reconstruction. A systematic review by Spindler et al. included nine studies of primary ACL reconstruction (151). The mean Cincinnati scores in the studies included in the Spindler meta-analysis ranged from 86 to 94 compared with 81 in the systematic review from Wright et al (150). The Lysholm mean score was 85 in one study and >90 in other four compared with 82.1 for the revision ACL systematic review. Furthermore, the mean IKDC subjective score in the MOON (Multicenter Orthopaedic Outcomes Network) primary ACL reconstruction cohort 149 was 84 compared with 74.8 in the mixed-model meta-analysis in the aforementioned systematic review study (150).
Finally, the objective failure rate after revision ACL reconstruction in the present study was 13.7% compared with 3.67% after primary ACL reconstruction in the prospective studies analyzed by Spindler et al. (151); this is compared with the 2.9% at two years of follow-up in the MOON cohort and the 5.8% at a minimum of five years of follow-up in another recent systematic review (152).
In another recent study, Gifstad et al. directly compared results after revision ACL reconstructions with primary ACL reconstructions (153). The revision group had significantly inferior KOOS and Lysholm scores compared with the primary group. Patients in the revision group also showed greater laxity measured with the pivot shift test, a larger reduction in the Tegner activity score, reduced muscle strength in the injured knee, and more severe radiological osteoarthritis; however, no difference in anterior-posterior translation was found.
Revision ACL surgery is a challenging procedure that necessitates consideration of many factors; satisfactory outcomes in revision surgery can be 3-4 times lower than that of primary ACL reconstruction. Correct identification of the cause of failure, anatomic positioning of tunnels and careful, individualized rehabilitation protocol are the keys for success in a patient with realistic expectations.
Acknowledgements
The authors would like to thank Alex Lazarides BSc for his contributions.
References
- 1.Gianotti SM, Marshall SW, Hume PA, Bunt L. Incidence of anterior cruciate ligament injury and other knee ligament injuries: a national population-based study. J Sci Med Sport. 2009;12(6):622–7. doi: 10.1016/j.jsams.2008.07.005. [DOI] [PubMed] [Google Scholar]
- 2.Parkkari J, Pasanen K, Mattila VM, Kannus P, Rimpela A. The risk for a cruciate ligament injury of the knee in adolescents and young adults: a population-based cohort study of 46 500 people with a 9-year follow-up. Br J Sports Med. 2008;42(6):422–6. doi: 10.1136/bjsm.2008.046185. [DOI] [PubMed] [Google Scholar]
- 3.Griffin LY, Albohm MJ, Arendt EA, Bahr R, Beynnon BD, Demaio M, et al. Understanding and preventing noncontact anterior cruciate ligament injuries: a review of the Hunt Valley II meeting, January 2005. Am J Sports Med. 2006;34(9):1512–32. doi: 10.1177/0363546506286866. [DOI] [PubMed] [Google Scholar]
- 4.Bach BR., Jr Revision anterior cruciate ligament surgery. Arthroscopy. 2003;19(Suppl 1):14–29. doi: 10.1016/j.arthro.2003.09.044. [DOI] [PubMed] [Google Scholar]
- 5.Baer GS, Harner CD. Clinical outcomes of allograft versus autograft in anterior cruciate ligament reconstruction. Clin Sports Med. 2007;26(4):661–81. doi: 10.1016/j.csm.2007.06.010. [DOI] [PubMed] [Google Scholar]
- 6.Johnson DL, Fu FH. Anterior cruciate ligament reconstruction: why do failures occur? Instr Course Lect. 1995;44(11):391–406. [PubMed] [Google Scholar]
- 7.Kamath GV, Redfern JC, Greis PE, Burks RT. Revision anterior cruciate ligament reconstruction. Am J Sports Med. 2011;39(1):199–217. doi: 10.1177/0363546510370929. [DOI] [PubMed] [Google Scholar]
- 8.Noyes FR, Barber-Westin SD. Revision anterior cruciate surgery with use of bone-patellar tendon-bone autogenous grafts. J Bone Joint Surg Am. 2001;83(8):1131–43. doi: 10.2106/00004623-200108000-00001. [DOI] [PubMed] [Google Scholar]
- 9.Alford JW, Bach BR., Jr Arthrometric aspects of anterior cruciate ligament surgery before and after reconstruction with patellar tendon grafts. Tech Orthop. 2005;20(4):421–38. [Google Scholar]
- 10.Bach BR., Jr . Revision ACL reconstruction: indications and technique. In: Miller MD, Cole BJ, editors. Textbook of Arthroscopy. Philadelphia: Elsevier; 2004. p. 896. [Google Scholar]
- 11.George MS, Dunn WR, Spindler KP. Current concepts review: revision anterior cruciate ligament reconstruction. Am J Sports Med. 2006;34(12):2026–37. doi: 10.1177/0363546506295026. [DOI] [PubMed] [Google Scholar]
- 12.Wright RW, Huston LJ, Spindler KP, Dunn WR, Haas AK, Allen CR, et al. Descriptive epidemiology of the multicenter ACL revision study (MARS) cohort. Am J Sports Med. 2010;38(10):1979–86. doi: 10.1177/0363546510378645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Muneta T, Yamamoto H, Ishibashi T, Asahina S, Murakami S, Furuya K. The effects of tibial tunnel placement and roofplasty on reconstructed anterior cruciate ligament knees. Arthroscopy. 1995;11(1):57–62. doi: 10.1016/0749-8063(95)90089-6. [DOI] [PubMed] [Google Scholar]
- 14.Cugat BR, Samitier SG, Alvarez DP, Steinbacher G. Fracaso de la cirugia del LCA. Trauma. 2008;19(Suppl 1):55–75. [Google Scholar]
- 15.Harter RA, Osternig LR, Singer KM, James SL, Larson RL, Jones DC. Long-term evaluation of knee stability and function following surgical reconstruction for anterior cruciate ligament insufficiency. Am J Sports Med. 1988;16(5):434–43. doi: 10.1177/036354658801600502. [DOI] [PubMed] [Google Scholar]
- 16.Holmes PF, James SL, Larson RL, Singer KM, Jones DC. Retrospective direct comparison of three intraarticular anterior cruciate ligament reconstructions. Am J Sports Med. 1991;19(6):596–9. doi: 10.1177/036354659101900607. [DOI] [PubMed] [Google Scholar]
- 17.Howe JG, Johnson RJ, Kaplan MJ, Fleming B, Jarvinen M. Anterior cruciate ligament reconstruction using quadriceps patellar tendon graft. Part I. Long-term followup. Am J Sports Med. 1991;19(5):447–57. doi: 10.1177/036354659101900505. [DOI] [PubMed] [Google Scholar]
- 18.Kaplan MJ, Howe JG, Fleming B, Johnson RJ, Jarvinen M. Anterior cruciate ligament reconstruction using quadriceps patellar tendon graft. Part II. A specific sport review. Am J Sports Med. 1991;19(5):458–62. doi: 10.1177/036354659101900506. [DOI] [PubMed] [Google Scholar]
- 19.Aglietti P, Buzzi R, D’Andria S, Zaccherotti G. Patellofemoral problems after intraarticular anterior cruciate ligament reconstruction. Clin Orthop Relat Res. 1993;288(3):195–204. [PubMed] [Google Scholar]
- 20.Bach BR, Jr, Wojtys EM, Lindenfeld TN. Reflex sympathetic dystrophy, patella infera contracture syndrome, and loss of motion following anterior cruciate ligament surgery. Instr Course Lect. 1997;46(1):251–60. [PubMed] [Google Scholar]
- 21.Daniel DM, Stone ML, Dobson BE, Fithian DC, Rossman DJ, Kaufman KR. Fate of the ACL-injured patient. A prospective outcome study. Am J Sports Med. 1994;22(5):632–44. doi: 10.1177/036354659402200511. [DOI] [PubMed] [Google Scholar]
- 22.Dye SF, Chew MH. Restoration of osseous homeostasis after anterior cruciate ligament reconstruction. Am J Sports Med. 1993;21(5):748–50. doi: 10.1177/036354659302100521. [DOI] [PubMed] [Google Scholar]
- 23.Graf B, Uhr F. Complications of intra-articular anterior cruciate reconstruction. Clin Sports Med. 1988;7(4):835–48. [PubMed] [Google Scholar]
- 24.Harner CD, Irrgang JJ, Paul J, Dearwater S, Fu FH. Loss of motion after anterior cruciate ligament reconstruction. Am J Sports Med. 1992;20(5):499–506. doi: 10.1177/036354659202000503. [DOI] [PubMed] [Google Scholar]
- 25.Jaureguito JW, Paulos LE. Why grafts fail. Clin Orthop Relat Res. 1996;325(1):25–41. doi: 10.1097/00003086-199604000-00005. [DOI] [PubMed] [Google Scholar]
- 26.Paulos LE, Rosenberg TD, Drawbert J, Manning J, Abbott P. Infrapatellar contracture syndrome. An unrecognized cause of knee stiffness with patella entrapment and patella infera. Am J Sports Med. 1987;15(4):331–41. doi: 10.1177/036354658701500407. [DOI] [PubMed] [Google Scholar]
- 27.Shelbourne KD, Wilckens JH, Mollabashy A, DeCarlo M. Arthrofibrosis in acute anterior cruciate ligament reconstruction. The effect of timing of reconstruction and rehabilitation. Am J Sports Med. 1991;19(4):332–6. doi: 10.1177/036354659101900402. [DOI] [PubMed] [Google Scholar]
- 28.Johnson DL, Harner CD, Maday MG, Fu FH. Revision anterior cruciate ligament surgery. In: Fu FH, Harner CD, Vince KG, editors. Knee Surgery. Baltimore: Williams & Wilkins; 1994. pp. 877–95. [Google Scholar]
- 29.Wetzler MJ, Bartolozzi AR, Gillespie MJ, Rubenstein DL, Ciccotti MG, Miller LS. Revision anterior cruciate ligament reconstruction. Oper Tech Orthop. 1996;6(3):181–9. [Google Scholar]
- 30.Harner CD, Giffin JR, Dunteman RC, Annunziata CC, Friedman MJ. Evaluation and treatment of recurrent instability after anterior cruciate ligament reconstruction. Instr Course Lect. 2001;50(1):463–74. [PubMed] [Google Scholar]
- 31.Clancy WG, Jr, Narechania RG, Rosenberg TD, Gmeiner JG, Wisnefske DD, Lange TA. Anterior and posterior cruciate ligament reconstruction in rhesus monkeys. J Bone Joint Surg Am. 1981;63(8):1270–84. [PubMed] [Google Scholar]
- 32.Drez DJ, Jr, DeLee J, Holden JP, Arnoczky S, Noyes FR, Roberts TS. Anterior cruciate ligament reconstruction using bone-patellar tendon-bone allografts. A biological and biomechanical evaluation in goats. Am J Sports Med. 1991;19(3):256–63. doi: 10.1177/036354659101900308. [DOI] [PubMed] [Google Scholar]
- 33.Getelman MH, Schepsis AA, Zimmer J. Revision ACL reconstruction: Autograft versus allograft. Arthroscopy. 1995;11(1):378. [Google Scholar]
- 34.Uribe JW, Hechtman KS, Zvijac JE, Tjin-A-T EW. Revision anterior cruciate ligament surgery: experience from Miami. Clin Orthop Relat Res. 1996;325(3):91–9. doi: 10.1097/00003086-199604000-00010. [DOI] [PubMed] [Google Scholar]
- 35.Johnson DL, Swenson TM, Irrgang JJ, Fu FH, Harner CD. Revision anterior cruciate ligament surgery: experience from Pittsburgh. Clin Orthop Relat Res. 1996;325(11):100–9. doi: 10.1097/00003086-199604000-00011. [DOI] [PubMed] [Google Scholar]
- 36.Hoogland T, Hillen B. Intra-articular reconstruction of the anterior cruciate ligament. An experimental study of length changes in different ligament reconstructions. Clin Orthop Relat Res. 1984;185(1):197–202. [PubMed] [Google Scholar]
- 37.Howell SM, Barad SJ. Knee extension and its relationship to the slope of the intercondylar roof. Implications for positioning the tibial tunnel in anterior cruciate ligament reconstructions. Am J Sports Med. 1995;23(3):288–94. doi: 10.1177/036354659502300306. [DOI] [PubMed] [Google Scholar]
- 38.Howell SM, Clark JA. Tibial tunnel placement in anterior cruciate ligament reconstructions and graft impingement. Clin Orthop Relat Res. 1992;283(2):187–95. [PubMed] [Google Scholar]
- 39.Howell SM, Taylor MA. Failure of reconstruction of the anterior cruciate ligament due to impingement by the intercondylar roof. J Bone Joint Surg Am. 1993;75(7):1044–55. doi: 10.2106/00004623-199307000-00011. [DOI] [PubMed] [Google Scholar]
- 40.Jackson DW, Gasser SI. Tibial tunnel placement in ACL reconstruction. Arthroscopy. 1994;10(2):124–31. doi: 10.1016/s0749-8063(05)80079-9. [DOI] [PubMed] [Google Scholar]
- 41.Romano VM, Graf BK, Keene JS, Lange RH. Anterior cruciate ligament reconstruction. The effect of tibial tunnel placement on range of motion. Am J Sports Med. 1993;21(3):415–8. doi: 10.1177/036354659302100315. [DOI] [PubMed] [Google Scholar]
- 42.Vergis A, Gillquist J. Graft failure in intra-articular anterior cruciate ligament reconstructions: a review of the literature. Arthroscopy. 1995;11(3):312–21. doi: 10.1016/0749-8063(95)90009-8. [DOI] [PubMed] [Google Scholar]
- 43.Wright RW, Huston LJ, Spindler KP, Dunn WR, Haas AK, Allen CR, et al. Descriptive epidemiology of the multicenter ACL revision study (MARS) cohort. Am J Sports Med. 2010;38(10):1979–86. doi: 10.1177/0363546510378645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Trojani C, Sbihi A, Djian P, Potel JF, Hulet C, Jouve F, et al. Causes for failure of ACL reconstruction and influence of meniscectomies after revision. Knee Surg Sports Traumatol Arthrosc. 2011;19(2):196–201. doi: 10.1007/s00167-010-1201-6. [DOI] [PubMed] [Google Scholar]
- 45.Maday MG, Harner CD, Fu FH. Revision ACL surgery: evaluation and treatment. The crucial ligaments. In: Feagin JA, editor. Diagnosis and treatment of ligamentous injuries about the knee. 2nd ed. New York: Churchill-Livingstone; 1994. pp. 711–723. [Google Scholar]
- 46.Hosseini A, Lodhia P, Van de Velde SK, Asnis PD, Zarins B, Gill TJ, et al. Tunnel position and graft orientation in failed anterior cruciate ligament reconstruction: a clinical and imaging analysis. Int Orthop. 2012;36(4):845–52. doi: 10.1007/s00264-011-1333-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Carson EW, Simonian PT, Wickiewicz TL, Warren RF. Revision anterior cruciate ligament reconstruction. Instr Course Lect. 1998;47(7):361–8. [PubMed] [Google Scholar]
- 48.Girgis FG, Marshall JL, Monajem A. The cruciate ligaments of the knee joint. Anatomical, functional and experimental analysis. Clin Orthop Relat Res. 1975;106(2):216–31. doi: 10.1097/00003086-197501000-00033. [DOI] [PubMed] [Google Scholar]
- 49.Bylski-Austrow DI, Grood ES, Hefzy MS, Holden JP, Butler DL. Anterior cruciate ligament replacements: a mechanical study of femoral attachment location, flexion angle at tensioning, and initial tension. J Orthop Res. 1990;8(4):522–31. doi: 10.1002/jor.1100080408. [DOI] [PubMed] [Google Scholar]
- 50.Good L, Odensten M, Gillquist J. Sagittal knee stability after anterior cruciate ligament reconstruction with a patellar tendon strip. A two-year follow-up study. Am J Sports Med. 1994;22(4):518–23. doi: 10.1177/036354659402200414. [DOI] [PubMed] [Google Scholar]
- 51.Howell SM, Clark JA, Farley TE. Serial magnetic resonance study assessing the effects of impingement on the MR image of the patellar tendon graft. Arthroscopy. 1992;8(3):350–8. doi: 10.1016/0749-8063(92)90067-l. [DOI] [PubMed] [Google Scholar]
- 52.Getelman MH, Friedman MJ. Revision anterior cruciate ligament reconstruction surgery. J Am Acad Orthop Surg. 1999;7(3):189–98. doi: 10.5435/00124635-199905000-00005. [DOI] [PubMed] [Google Scholar]
- 53.Tanzer M, Lenczner E. The relationship of intercondylar notch size and content to notchplasty requirement in anterior cruciate ligament surgery. Arthroscopy. 1990;6(2):89–93. doi: 10.1016/0749-8063(90)90004-w. [DOI] [PubMed] [Google Scholar]
- 54.Corsetti JR, Jackson DW. Failure of anterior cruciate ligament reconstruction: the biologic basis. Clin Orthop Relat Res. 1996;325(4):42–9. doi: 10.1097/00003086-199604000-00006. [DOI] [PubMed] [Google Scholar]
- 55.Jackson DW, Schaefer RK. Cyclops syndrome: loss of extension following intra-articular anterior cruciate ligament reconstruction. Arthroscopy. 1990;6(3):171–8. doi: 10.1016/0749-8063(90)90072-l. [DOI] [PubMed] [Google Scholar]
- 56.Delcogliano A, Franzese S, Branca A, Magi M, Fabbriciani C. Light and scan electron microscopic analysis of cyclops syndrome: etiopathogenic hypothesis and technical solutions. Knee Surg Sports Traumatol Arthrosc. 1996;4(4):194–9. doi: 10.1007/BF01567962. [DOI] [PubMed] [Google Scholar]
- 57.Lindenfeld TN, Wojtys EM, Husain A. Surgical treatment of arthrofibrosis of the knee. Instr Course Lect. 2000;49(3):211–21. [PubMed] [Google Scholar]
- 58.Richmond JC, al Assal M. Arthroscopic management of arthrofibrosis of the knee, including infrapatellar contraction syndrome. Arthroscopy. 1991;7(2):144–7. doi: 10.1016/0749-8063(91)90099-j. [DOI] [PubMed] [Google Scholar]
- 59.Sprague NF., 3rd Motion-limiting arthrofibrosis of the knee: the role of arthroscopic management. Clin Sports Med. 1987;6(3):537–49. [PubMed] [Google Scholar]
- 60.Brown CH, Jr, Carson EW. Revision anterior cruciate ligament surgery. Clin Sports Med. 1999;18(1):109–71. doi: 10.1016/s0278-5919(05)70133-2. [DOI] [PubMed] [Google Scholar]
- 61.Ristanis S, Giakas G, Papageorgiou CD, Moraiti T, Stergiou N, Georgoulis AD. The effects of anterior cruciate ligament reconstruction on tibial rotation during pivoting after descending stairs. Knee Surg Sports Traumatol Arthrosc. 2003;11(6):360–5. doi: 10.1007/s00167-003-0428-x. [DOI] [PubMed] [Google Scholar]
- 62.Woo SL, Kanamori A, Zeminski J, Yagi M, Papageorgiou C, Fu FH. The effectiveness of reconstruction of the anterior cruciate ligament with hamstrings and patellar tendon. A cadaveric study comparing anterior tibial and rotational loads. J Bone Joint Surg Am. 2002;84(6):907–14. doi: 10.2106/00004623-200206000-00003. [DOI] [PubMed] [Google Scholar]
- 63.Gillquist J, Odensten M. Arthroscopic reconstruction of the anterior cruciate ligament. Arthroscopy. 1988;4(1):5–9. doi: 10.1016/s0749-8063(88)80003-3. [DOI] [PubMed] [Google Scholar]
- 64.Howell SM, Clark JA, Farley TE. A rationale for predicting anterior cruciate graft impingement by the intercondylar roof. A magnetic resonance imaging study. Am J Sports Med. 1991;19(3):276–82. doi: 10.1177/036354659101900312. [DOI] [PubMed] [Google Scholar]
- 65.Zhu Y, Tang RK, Zhao P, Zhu SS, Li YG, Li JB. Double-bundle reconstruction results in superior clinical outcome than single-bundle reconstruction. Knee Surg Sports Traumatol Arthrosc. 2012;21(5):1085–96. doi: 10.1007/s00167-012-2073-8. [DOI] [PubMed] [Google Scholar]
- 66.Aglietti P, Giron F, Losco M, Cuomo P, Ciardullo A, Mondanelli N. Comparison between single-and double-bundle anterior cruciate ligament reconstruction: a prospective, randomized, single-blinded clinical trial. Am J Sports Med. 2010;38(1):25–34. doi: 10.1177/0363546509347096. [DOI] [PubMed] [Google Scholar]
- 67.Siebold R, Dehler C, Ellert T. Prospective randomized comparison of double-bundle versus single-bundle anterior cruciate ligament reconstruction. Arthroscopy. 2008;24(2):137–45. doi: 10.1016/j.arthro.2007.11.013. [DOI] [PubMed] [Google Scholar]
- 68.van Eck CF, Kopf S, Irrgang JJ, Blankevoort L, Bhandari M, Fu FH, et al. Single-bundle versus double-bundle reconstruction for anterior cruciate ligament rupture: a meta-analysis-does anatomy matter? Arthroscopy. 2012;28(3):405–24. doi: 10.1016/j.arthro.2011.11.021. [DOI] [PubMed] [Google Scholar]
- 69.Karlsson J, Irrgang JJ, van Eck CF, Samuelsson K, Mejia HA, Fu FH. Anatomic single- and double-bundle anterior cruciate ligament reconstruction, part 2: clinical application of surgical technique. Am J Sports Med. 2011;39(9):2016–26. doi: 10.1177/0363546511402660. [DOI] [PubMed] [Google Scholar]
- 70.Gersoff WK, Clancy WG., Jr Diagnosis of acute and chronic anterior cruciate ligament tears. Clin Sports Med. 1988;7(4):727–38. [PubMed] [Google Scholar]
- 71.Noyes FR, Barber SD, Simon R. High tibial osteotomy and ligament reconstruction in varus angulated, anterior cruciate ligament-deficient knees. A two- to seven-year follow-up study. Am J Sports Med. 1993;21(1):2–12. doi: 10.1177/036354659302100102. [DOI] [PubMed] [Google Scholar]
- 72.Yasuda K, Kitamura N, Kondo E, Hayashi R, Inoue M. One-stage anatomic double-bundle anterior and posterior cruciate ligament reconstruction using the autogenous hamstring tendons. Knee Surg Sports Traumatol Arthrosc. 2009;17(7):800–5. doi: 10.1007/s00167-009-0800-6. [DOI] [PubMed] [Google Scholar]
- 73.Lo YP, Hsu KY, Chen LH, Wang CJ, Yeh WL, Chan YS, et al. Simultaneous arthroscopic reconstruction of the anterior and posterior cruciate ligament using hamstring and quadriceps tendon autografts. J Trauma. 2009;66(3):780–8. doi: 10.1097/TA.0b013e31815d9b88. [DOI] [PubMed] [Google Scholar]
- 74.Zhao J, Huangfu X, He Y, Yang X, Zhu Y. Simultaneous double-bundle anterior cruciate ligament and posterior cruciate ligament reconstruction with autogenous hamstring tendons. Arthroscopy. 2008;24(11):1205–13. doi: 10.1016/j.arthro.2008.06.018. [DOI] [PubMed] [Google Scholar]
- 75.Kurosaka M, Yoshiya S, Andrish JT. A biomechanical comparison of different surgical techniques of graft fixation in anterior cruciate ligament reconstructions. Am J Sports Med. 1987;15(3):225–9. doi: 10.1177/036354658701500306. [DOI] [PubMed] [Google Scholar]
- 76.Steiner ME, Hecker AT, Brown CH, Jr, Hayes WC. Anterior cruciate ligament graft fixation. Comparison of hamstring and patellar tendon grafts. Am J Sports Med. 1994;22(2):240–6. doi: 10.1177/036354659402200215. [DOI] [PubMed] [Google Scholar]
- 77.Gertel TH, Lew WD, Lewis JL, Stewart NJ, Hunter RE. Effect of anterior cruciate ligament graft tensioning direction, magnitude, and flexion angle on knee biomechanics. Am J Sports Med. 1993;21(4):572–81. doi: 10.1177/036354659302100415. [DOI] [PubMed] [Google Scholar]
- 78.Yoshiya S, Andrish JT, Manley MT, Bauer TW. Graft tension in anterior cruciate ligament reconstruction. An in vivo study in dogs. Am J Sports Med. 1987;15(5):464–70. doi: 10.1177/036354658701500506. [DOI] [PubMed] [Google Scholar]
- 79.Arnold MP, Lie DT, Verdonschot N, de Graaf R, Amis AA, van Kampen A. The remains of anterior cruciate ligament graft tension after cyclic knee motion. Am J Sports Med. 2005;33(4):536–42. doi: 10.1177/0363546504269938. [DOI] [PubMed] [Google Scholar]
- 80.Arneja S, McConkey MO, Mulpuri K, Chin P, Gilbart MK, Regan WD, et al. Graft tensioning in anterior cruciate ligament reconstruction: a systematic review of randomized controlled trials. Arthroscopy. 2009;25(2):200–7. doi: 10.1016/j.arthro.2008.07.010. [DOI] [PubMed] [Google Scholar]
- 81.Brown HR, Steiner ME. Anterior cruciate ligament injuries. In: Siliski JM, editor. Traumatic disorders of the knee. New York: Springer-Velarg; 1994. pp. 193–284. [Google Scholar]
- 82.Burks RT, Friederichs MG, Fink B, Luker MG, West HS, Greis PE. Treatment of postoperative anterior cruciate ligament infections with graft removal and early reimplantation. Am J Sports Med. 2003;31(3):414–8. doi: 10.1177/03635465030310031501. [DOI] [PubMed] [Google Scholar]
- 83.Poolman RW, Abouali JA, Conter HJ, Bhandari M. Overlapping systematic reviews of anterior cruciate ligament reconstruction comparing hamstring autograft with bone-patellar tendon-bone autograft: why are they different? J Bone Joint Surg Am. 2007;89(7):1542–52. doi: 10.2106/JBJS.F.01292. [DOI] [PubMed] [Google Scholar]
- 84.Kartus J, Stener S, Lindahl S, Eriksson BI, Karlsson J. Ipsi- or contralateral patellar tendon graft in anterior cruciate ligament revision surgery. A comparison of two methods. Am J Sports Med. 1998;26(4):499–504. doi: 10.1177/03635465980260040401. [DOI] [PubMed] [Google Scholar]
- 85.Shelbourne KD, O’Shea JJ. Revision anterior cruciate ligament reconstruction using the contralateral bone-patellar tendon-bone graft. Instr Course Lect. 2002;51(1):343–6. [PubMed] [Google Scholar]
- 86.Colosimo AJ, Heidt RS, Jr, Traub JA, Carlonas RL. Revision anterior cruciate ligament reconstruction with a reharvested ipsilateral patellar tendon. Am J Sports Med. 2001;29(6):746–50. doi: 10.1177/03635465010290061301. [DOI] [PubMed] [Google Scholar]
- 87.Karns DJ, Heidt RS, Jr, Holladay BR, Colosimo AJ. Case report: revision anterior cruciate ligament reconstruction. Arthroscopy. 1994;10(2):148–51. doi: 10.1016/s0749-8063(05)80082-9. [DOI] [PubMed] [Google Scholar]
- 88.LaPrade RF, Hamilton CD, Montgomery RD, Wentorf F, Hawkins HD. The reharvested central third of the patellar tendon. A histologic and biomechanical analysis. Am J Sports Med. 1997;25(6):779–85. doi: 10.1177/036354659702500609. [DOI] [PubMed] [Google Scholar]
- 89.Proctor CS, Jackson DW, Simon TM. Characterization of the repair tissue after removal of the central one-third of the patellar ligament. An experimental study in a goat model. J Bone Joint Surg Am. 1997;79(7):997–1006. doi: 10.2106/00004623-199707000-00005. [DOI] [PubMed] [Google Scholar]
- 90.Woods GW, Fincher AL, O’Connor DP, Bacon SA. Revision anterior cruciate ligament reconstruction using the lateral third of the ipsilateral patellar tendon after failure of a central-third graft: a preliminary report on 10 patients. Am J Knee Surg. 2001;14(1):23–31. [PubMed] [Google Scholar]
- 91.Rubinstein RA, Jr, Shelbourne KD, VanMeter CD, McCarroll JC, Rettig AC. Isolated autogenous bone-patellar tendon-bone graft site morbidity. Am J Sports Med. 1994;22(3):324–7. doi: 10.1177/036354659402200305. [DOI] [PubMed] [Google Scholar]
- 92.Greis PE, Johnson DL, Fu FH. Revision anterior cruciate ligament surgery: causes of graft failure and technical considerations of revision surgery. Clin Sports Med. 1993;12(4):839–52. [PubMed] [Google Scholar]
- 93.Noyes FR, Barber SD. The effect of a ligament-augmentation device on allograft reconstructions for chronic ruptures of the anterior cruciate ligament. J Bone Joint Surg Am. 1992;74(7):960–73. [PubMed] [Google Scholar]
- 94.Amendola A, Fowler P. Allograft anterior cruciate ligament reconstruction in a sheep model. The effect of synthetic augmentation. Am J Sports Med. 1992;20(3):336–46. doi: 10.1177/036354659202000318. [DOI] [PubMed] [Google Scholar]
- 95.Thompson WO, Harner CD, Jamison J. Immunologic response to fresh frozen patellar tendon allograft for anterior cruciate reconstruction. Trans Orthop Relat Sci. 1994;19(6):624. [Google Scholar]
- 96.Buck BE, Malinin TI. Human bone and tissue allografts. Preparation and safety. Clin Orthop Relat Res. 1994;303(2):8–17. [PubMed] [Google Scholar]
- 97.Rasmussen TJ, Feder SM, Butler DL, Noyes FR. The effects of 4 Mrad of gamma irradiation on the initial mechanical properties of bone-patellar tendon-bone grafts. Arthroscopy. 1994;10(2):188–97. doi: 10.1016/s0749-8063(05)80092-1. [DOI] [PubMed] [Google Scholar]
- 98.Olson EJ, Kang JD, Fu FH, Georgescu HI, Mason GC, Evans CH. The biochemical and histological effects of artificial ligament wear particles: in vitro and in vivo studies. Am J Sports Med. 1988;16(6):558–70. doi: 10.1177/036354658801600602. [DOI] [PubMed] [Google Scholar]
- 99.Pinkowski JL, Reiman PR, Chen SL. Human lymphocyte reaction to freeze-dried allograft and xenograft ligamentous tissue. Am J Sports Med. 1989;17(5):595–600. doi: 10.1177/036354658901700501. [DOI] [PubMed] [Google Scholar]
- 100.Gibbons MJ, Butler DL, Grood ES, Bylski-Austrow DI, Levy MS, Noyes FR. Effects of gamma irradiation on the initial mechanical and material properties of goat bone-patellar tendon-bone allografts. J Orthop Res. 1991;9(2):209–18. doi: 10.1002/jor.1100090209. [DOI] [PubMed] [Google Scholar]
- 101.Ritchie JR, Parker RD. Graft selection in anterior cruciate ligament revision surgery. Clin Orthop Relat Res. 1996;325(16):65–77. doi: 10.1097/00003086-199604000-00008. [DOI] [PubMed] [Google Scholar]
- 102.Greis PE, Steadman JR. Revision of failed prosthetic anterior cruciate ligament reconstruction. Clin Orthop Relat Res. 1996;325(12):78–90. doi: 10.1097/00003086-199604000-00009. [DOI] [PubMed] [Google Scholar]
- 103.Klein W, Jensen KU. Synovitis and artificial ligaments. Arthroscopy. 1992;8(1):116–24. doi: 10.1016/0749-8063(92)90145-2. [DOI] [PubMed] [Google Scholar]
- 104.Noyes FR, Barber-Westin SD. Revision anterior cruciate ligament surgery: experience from Cincinnati. Clin Orthop Relat Res. 1996;325(4):116–29. doi: 10.1097/00003086-199604000-00013. [DOI] [PubMed] [Google Scholar]
- 105.Paulos LE, Rosenberg TD, Grewe SR, Tearse DS, Beck CL. The GORE-TEX anterior cruciate ligament prosthesis. A long-term followup. Am J Sports Med. 1992;20(3):246–52. doi: 10.1177/036354659202000302. [DOI] [PubMed] [Google Scholar]
- 106.Steadman JR, Seemann MD, Hutton KS. Revision ligament reconstruction of failed prosthetic anterior cruciate ligaments. Instr Course Lect. 1995;44(1):417–29. [PubMed] [Google Scholar]
- 107.Woods GA, Indelicato PA, Prevot TJ. The Gore-Tex anterior cruciate ligament prosthesis. Two versus three year results. Am J Sports Med. 1991;19(1):48–55. doi: 10.1177/036354659101900108. [DOI] [PubMed] [Google Scholar]
- 108.Arnoczky SP. Biology of ACL reconstructions: what happens to the graft? Instr Course Lect. 1996;45(5):229–33. [PubMed] [Google Scholar]
- 109.Muneta T, Yamamoto H, Takakuda K, Sakai H, Furuya K. Effects of postoperative immobilization on the reconstructed anterior cruciate ligament. An experimental study in rabbits. Am J Sports Med. 1993;21(2):305–13. doi: 10.1177/036354659302100223. [DOI] [PubMed] [Google Scholar]
- 110.Jackson DW, Grood ES, Goldstein JD, Rosen MA, Kurzweil PR, Cummings JF, et al. A comparison of patellar tendon autograft and allograft used for anterior cruciate ligament reconstruction in the goat model. Am J Sports Med. 1993;21(2):176–85. doi: 10.1177/036354659302100203. [DOI] [PubMed] [Google Scholar]
- 111.Rodeo SA, Arnoczky SP, Torzilli PA, Hidaka C, Warren RF. Tendon-healing in a bone tunnel. A biomechanical and histological study in the dog. J Bone Joint Surg Am. 1993;75(12):1795–803. doi: 10.2106/00004623-199312000-00009. [DOI] [PubMed] [Google Scholar]
- 112.Cullison TR, Muldoon MP, Gorman JD, Goff WB. The incidence of deep venous thrombosis in anterior cruciate ligament reconstruction. Arthroscopy. 1996;12(6):657–9. doi: 10.1016/s0749-8063(96)90166-8. [DOI] [PubMed] [Google Scholar]
- 113.Safran MR, Harner CD. Technical considerations of revision anterior cruciate ligament surgery. Clin Orthop Relat Res. 1996;325(12):50–64. doi: 10.1097/00003086-199604000-00007. [DOI] [PubMed] [Google Scholar]
- 114.Williams JS, Jr, Hulstyn MJ, Fadale PD, Lindy PB, Ehrlich MG, Cronan J, et al. Incidence of deep vein thrombosis after arthroscopic knee surgery: a prospective study. Arthroscopy. 1995;11(6):701–5. doi: 10.1016/0749-8063(95)90113-2. [DOI] [PubMed] [Google Scholar]
- 115.Irrgang JJ, Harner CD. Loss of motion following knee ligament reconstruction. Sports Med. 1995;19(2):150–9. doi: 10.2165/00007256-199519020-00006. [DOI] [PubMed] [Google Scholar]
- 116.Strum GM, Friedman MJ, Fox JM, Ferkel RD, Dorey FH, Del Pizzo W, et al. Acute anterior cruciate ligament reconstruction. Analysis of complications. Clin Orthop Relat Res. 1990;253(10):184–9. [PubMed] [Google Scholar]
- 117.Paulos LE, Wnorowski DC, Greenwald AE. Infrapatellar contracture syndrome. Diagnosis, treatment, and long-term followup. Am J Sports Med. 1994;22(4):440–9. doi: 10.1177/036354659402200402. [DOI] [PubMed] [Google Scholar]
- 118.Mayr HO, Weig TG, Plitz W. Arthrofibrosis following ACL reconstruction-reasons and outcome. Arch Orthop Trauma Surg. 2004;124(8):518–22. doi: 10.1007/s00402-004-0718-x. [DOI] [PubMed] [Google Scholar]
- 119.Noyes FR, Mangine RE, Barber SD. The early treatment of motion complications after reconstruction of the anterior cruciate ligament. Clin Orthop Relat Res. 1992;277(17):217–28. [PubMed] [Google Scholar]
- 120.Noyes FR, Wojtys EM, Marshall MT. The early diagnosis and treatment of developmental patella infera syndrome. Clin Orthop Relat Res. 1991;265(6):241–52. [PubMed] [Google Scholar]
- 121.Shelbourne KD, Patel DV. Timing of surgery in anterior cruciate ligament-injured knees. Knee Surg Sports Traumatol Arthrosc. 1995;3(3):148–56. doi: 10.1007/BF01565474. [DOI] [PubMed] [Google Scholar]
- 122.Shelbourne KD, Trumper RV. Preventing anterior knee pain after anterior cruciate ligament reconstruction. Am J Sports Med. 1997;25(1):41–7. doi: 10.1177/036354659702500108. [DOI] [PubMed] [Google Scholar]
- 123.Weiss RA, Re LP, Rintz KG. Incidence of anterior knee pain after treatment for anterior cruciate ligament rupture. Arthroscopy. 1993;9(1):366–7. [Google Scholar]
- 124.Speer KP, Spritzer CE, Bassett FH, 3rd, Feagin JA, Jr, Garrett WE., Jr Osseous injury associated with acute tears of the anterior cruciate ligament. Am J Sports Med. 1992;20(4):382–9. doi: 10.1177/036354659202000403. [DOI] [PubMed] [Google Scholar]
- 125.Spindler KP, Schils JP, Bergfeld JA, Andrish JT, Weiker GG, Anderson TE, et al. Prospective study of osseous, articular, and meniscal lesions in recent anterior cruciate ligament tears by magnetic resonance imaging and arthroscopy. Am J Sports Med. 1993;21(4):551–7. doi: 10.1177/036354659302100412. [DOI] [PubMed] [Google Scholar]
- 126.Shelbourne KD, Nitz PA. The O’Donoghue triad revisited. Combined knee injuries involving anterior cruciate and medial collateral ligament tears. Am J Sports Med. 1991;19(5):474–7. doi: 10.1177/036354659101900509. [DOI] [PubMed] [Google Scholar]
- 127.DeHaven KE. Diagnosis of acute knee injuries with hemarthrosis. Am J Sports Med. 1980;8(1):9–14. doi: 10.1177/036354658000800102. [DOI] [PubMed] [Google Scholar]
- 128.Indelicato PA, Bittar ES. A perspective of lesions associated with ACL insufficiency of the knee. A review of 100 cases. Clin Orthop Relat Res. 1985;198(3):77–80. [PubMed] [Google Scholar]
- 129.Keene GC, Bickerstaff D, Rae PJ, Paterson RS. The natural history of meniscal tears in anterior cruciate ligament insufficiency. Am J Sports Med. 1993;21(5):672–9. doi: 10.1177/036354659302100506. [DOI] [PubMed] [Google Scholar]
- 130.McDaniel WJ, Jr, Dameron TB., Jr Untreated ruptures of the anterior cruciate ligament. A follow-up study. J Bone Joint Surg Am. 1980;62(5):696–705. [PubMed] [Google Scholar]
- 131.Warren RF. Meniscectomy and repair in the anterior cruciate ligament-deficient patient. Clin Orthop Relat Res. 1990;252(5):55–63. [PubMed] [Google Scholar]
- 132.Cooper DE, Arnoczky SP, Warren RF. Arthroscopic meniscal repair. Clin Sports Med. 1990;9(3):589–607. [PubMed] [Google Scholar]
- 133.Allen CR, Wong EK, Livesay GA, Sakane M, Fu FH, Woo SL. Importance of the medial meniscus in the anterior cruciate ligament-deficient knee. J Orthop Res. 2000;18(1):109–15. doi: 10.1002/jor.1100180116. [DOI] [PubMed] [Google Scholar]
- 134.Levy IM, Torzilli PA, Warren RF. The effect of medial meniscectomy on anterior-posterior motion of the knee. J Bone Joint Surg Am. 1982;64(6):883–8. [PubMed] [Google Scholar]
- 135.Brophy RH, Wright RW, David TS, McComack RG, Sekiya JK, Svoboda SJ, et al. Association between previous meniscal surgery and the incidence of chondral lesions at revision anterior cruciate ligament reconstruction. Am J Sports Med. 2012;40(4):808–14. doi: 10.1177/0363546512437722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Johnson DS, Smith RB. Outcome measurement in the ACL deficient knee--what’s the score? Knee. 2001;8(1):51–7. doi: 10.1016/s0968-0160(01)00068-0. [DOI] [PubMed] [Google Scholar]
- 137.Wang D, Jones MH, Khair MM, Miniaci A. Patient-reported outcome measures for the knee. J Knee Surg. 2010;23(3):137–51. doi: 10.1055/s-0030-1268691. [DOI] [PubMed] [Google Scholar]
- 138.Wirth CJ, Kohn D. Revision anterior cruciate ligament surgery: experience from Germany. Clin Orthop Relat Res. 1996;325(5):110–5. doi: 10.1097/00003086-199604000-00012. [DOI] [PubMed] [Google Scholar]
- 139.Grossman MG, ElAttrache NS, Shields CL, Glousman RE. Revision anterior cruciate ligament reconstruction: three- to nine-year follow-up. Arthroscopy. 2005;21(4):418–23. doi: 10.1016/j.arthro.2004.12.009. [DOI] [PubMed] [Google Scholar]
- 140.Noyes FR, Barber-Westin SD. Revision anterior cruciate surgery with use of bone-patellar tendon-bone autogenous grafts. J Bone Joint Surg Am. 2001;83(8):1131–43. doi: 10.2106/00004623-200108000-00001. [DOI] [PubMed] [Google Scholar]
- 141.O’Neill DB. Revision arthroscopically assisted anterior cruciate ligament reconstruction with previously unharvested ipsilateral autografts. Am J Sports Med. 2004;32(8):1833–41. doi: 10.1177/0363546504264585. [DOI] [PubMed] [Google Scholar]
- 142.Noyes FR, Barber-Westin SD. Anterior cruciate ligament revision reconstruction: results using a quadriceps tendon-patellar bone autograft. Am J Sports Med. 2006;34(4):553–64. doi: 10.1177/0363546505281812. [DOI] [PubMed] [Google Scholar]
- 143.Wright RW, Gill CS, Chen L, Brophy RH, Matava MJ, Smith MV, et al. Outcome of revision anterior cruciate ligament reconstruction: a systematic review. J Bone Joint Surg Am. 2012;94(6):531–6. doi: 10.2106/JBJS.K.00733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144.Safran MR, Harner CD. Revision ACL surgery: technique and results utilizing allografts. Instr Course Lect. 1995;44(2):407–15. [PubMed] [Google Scholar]
- 145.Ciccotti MG, Lombardo SJ, Nonweiler B, Pink M. Non-operative treatment of ruptures of the anterior cruciate ligament in middle-aged patients. Results after long-term follow-up. J Bone Joint Surg Am. 1994;76(9):1315–21. doi: 10.2106/00004623-199409000-00006. [DOI] [PubMed] [Google Scholar]
- 146.McCarty L, Pearce I, Bach BR., Jr Rehabilitation after patellar tendon autograft anterior cruciate ligament reconstruction. Tech Orthop. 2005;20(4):439–51. [Google Scholar]
- 147.Wright R, Spindler K, Huston L, Amendola A, Andrish J, Brophy R, et al. Revision ACL reconstruction outcomes: MOON cohort. J Knee Surg. 2011;24(4):289–94. doi: 10.1055/s-0031-1292650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 148.Thomas NP, Kankate R, Wandless F, Pandit H. Revision anterior cruciate ligament reconstruction using a 2-stage technique with bone grafting of the tibial tunnel. Am J Sports Med. 2005;33(11):1701–9. doi: 10.1177/0363546505276759. [DOI] [PubMed] [Google Scholar]
- 149.Wilde J, Bedi A, Altchek DW. Revision Anterior Cruciate Ligament Reconstruction. Sports Health. 2014;6(6):504–18. doi: 10.1177/1941738113500910. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.Wright RW, Gill CS, Chen L, Brophy RH, Matava MJ, Smith MV, et al. Outcome of Revision Anterior Cruciate Ligament Reconstruction: a systematic review. J Bone Joint Surg Am. 2012;94(6):531–6. doi: 10.2106/JBJS.K.00733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151.Spindler KP, Kuhn JE, Freedman KB, Matthews CE, Dittus RS, Harrell FE., Jr Anterior cruciate ligament reconstruction autograft choice: bone-tendon-bone versus hamstring: does it really matter? A systematic review. Am J Sports Med. 2004;32(8):1986–95. doi: 10.1177/0363546504271211. [DOI] [PubMed] [Google Scholar]
- 152.Wright RW, Magnussen RA, Dunn WR, Spindler KP. Ipsilateral graft and contralateral ACL rupture at five years following ACL reconstruction: a systematic review. J Bone Joint Surg Am. 2011;93(12):1159–65. doi: 10.2106/JBJS.J.00898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Gifstad T, Drogset JO, Viset A, Grontvedt T, Sofie G, Hortemo GS. Inferior results after revision ACL reconstructions: a comparison with primary ACL reconstructions. Knee Surg Sports Traumatol Arthrosc. 2013;21(9):2011–8. doi: 10.1007/s00167-012-2336-4. [DOI] [PubMed] [Google Scholar]