

Abstract
Background:
This study was conducted to explore the prevalence of medical error underreporting and associated barriers.
Methods:
This cross-sectional study was performed from September to December 2012. Five hospitals, affiliated with Hamadan University of Medical Sciences, in Hamedan, Iran were investigated. A self-administered questionnaire was used for data collection. Participants consisted of physicians, nurses, midwives, residents, interns, and staffs of radiology and laboratory departments.
Results:
Overall, 50.26% of subjects had committed but not reported medical errors. The main reasons mentioned for underreporting were lack of effective medical error reporting system (60.0%), lack of proper reporting form (51.8%), lack of peer supporting a person who has committed an error (56.0%), and lack of personal attention to the importance of medical errors (62.9%). The rate of committing medical errors was higher in men (71.4%), age of 50–40 years (67.6%), less-experienced personnel (58.7%), educational level of MSc (87.5%), and staff of radiology department (88.9%).
Conclusions:
This study outlined the main barriers to reporting medical errors and associated factors that may be helpful for healthcare organizations in improving medical error reporting as an essential component for patient safety enhancement.
Keywords: Iran, medical error, patient safety, reporting system
INTRODUCTION
Medical error is a serious public health problem that can pose a threat to patient safety. Currently, reducing medical errors has become an international concern.[1] Medical error is defined as “an act of omission or commission in planning or execution that contributes or could contribute to an unintended result.”[2] A medical error occurs when a health-care provider chooses an inappropriate method of care or improperly executes an appropriate method of care.[3]
Currently, there is a growing awareness regarding the importance of medical error and its consequences on both the healthcare quality and the patient safety.[4] Therefore, medical error reduction, as the first step of patient safety enhancement, has rapidly become a strategic priority for most healthcare organizations.[5] We can covert threats into opportunities if we learn from our mistakes. Most often, neither healthcare providers nor healthcare organizations advise others when a medical error takes happen. Unfortunately, they do not share what they have learned when an investigation has been conducted either. Consequently, the same mistakes occur many times in different settings and patients continue to be injured by preventable errors.[1]
One solution to this problem is that everybody reports errors in any setting. An efficient reporting system is the cornerstone of patient safety enhancement and a measure of progress toward achieving a safety culture.[1] One of the major problems to error-reduction efforts in healthcare organizations is the lack of data on the incidence rate of medical errors. Despite the high occurrence of medical errors, they are frequently underreported in healthcare organizations.[6,7,8]
Reporting errors is fundamental to error prevention.[1] Therefore, the presence of a well-organized reporting system is essential for effective prevention programs.[9] A majority of investigation in low and middle-income settings have focused on identifying the causes of medical errors rather than the barriers to reporting errors.[10] The incidence and type of barriers may vary across countries and regions because different policies are adopted by the institutes. Until reliable information on the barriers to medical reporting is collected, it is difficult to design effective intervention strategies to progress toward a comprehensive prevention program. Accordingly, this study was designed and conducted to identify the main barriers to medical error reporting in a middle-income country.
METHODS
This cross-sectional study was conducted in teaching hospitals affiliated with Hamadan University of Medical Sciences, in Hamadan city, the West of Iran, from September to December 2012. The hospitals which were recruited in this study included Besat, Ekbatan, Fatemieh, Shahid Beheshti, and Farshchian. The study population consisted of medical specialists, general practitioners, nurses, midwives, physiotherapists, and staffs of laboratory and radiology. Of 2183 study population, 348 participants were enrolled voluntarily in this study. Verbal rather than written informed consent was taken from the participants because no intervention was done in this observational study. Participants were only asked to fill out a self-administered questionnaire. At the beginning of the questionnaire, the participants were told that “If you dislike participating in the study and answering to the questions, you can avoid filling out the questionnaire.” The Research Committee of Hamadan University of Medical Sciences approved both the consent procedure and the whole study (No. 920204269).
In order to calculate sample size, assuming probability of medical error (P) equals to 0.5 and considering significance levels of 0.05 and error level of 0.2, we arrived at a sample of 171. Since we run a cluster random sampling, we doubled the sample size to save the statistical power. A stratified cluster random sampling method was carried out considering hospitals as strata and job categories as clusters. Then, the samples were taken proportion to the study population in each hospital.
The questionnaire, which was developed by the authors and used for data collection, composed of two parts. The first part included demographic and individual characteristics of the participants. The second part focused on the reasons for underreporting medical errors. A clear definition of medical error was provided at the beginning of the second part so that all participants had a unique understanding of the concept of medical error. Then, the participants were asked to announce their agreements to the potential relevant factors that might act as barriers for medical error reporting. The validity of the questionnaire was evaluated by two analysts and interpreters of medical error reporting as well as an epidemiologist. The reliability of the questionnaire was 84.47% using Cronbach's alpha coefficient. The Chi-square test was used for assessing the correlation between dichotomous variables. All statistical analysis was performed at 0.05 significant levels using statistical software Stata version 11.2 (StataCorp, College Station, TX, USA).
RESULTS
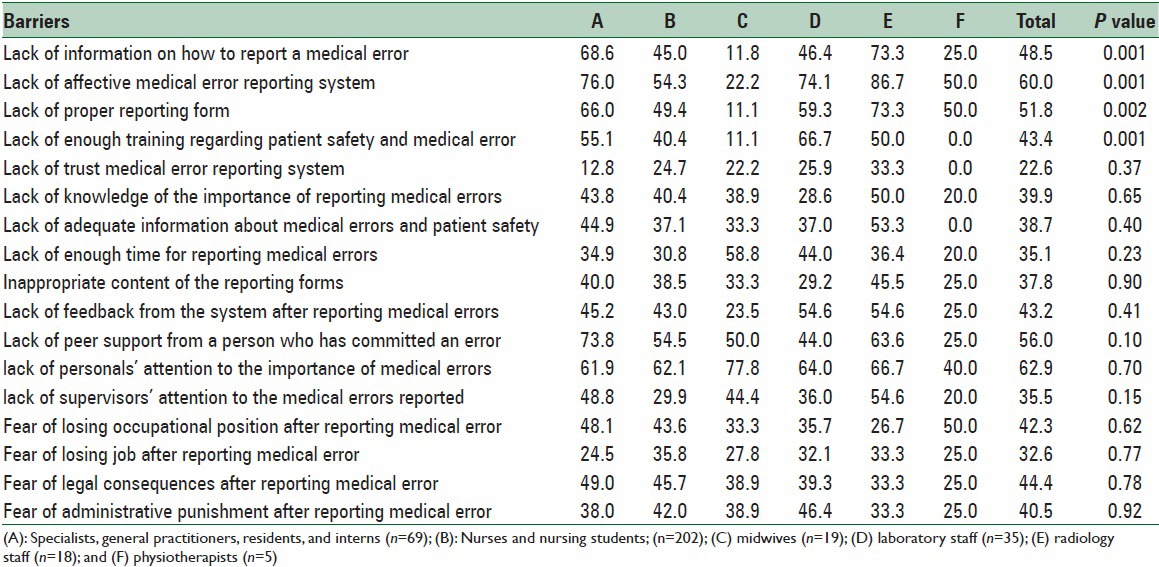
The proportion of the participants’ positive answers given to the purposed reasons for medical error underreporting is shown in Table 1. The main reasons with which majority of the participants agreed were: Lack of effective medical error reporting system (60.00%), lack of reporting properly (51.84%), lack of supporting a person who has committed an error (55.97%), and lack of personal attention to the importance of medical errors (62.86%).
Table 1.
Proportion (%) of the participants’ positive answers given to the purposed reasons of medical-error underreporting by job categories using Chi-squared test
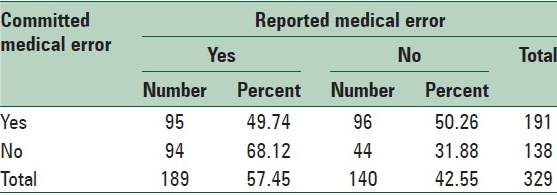
The proportion of participants who had committed and reported medical errors against those who had committed but had not reported medical error is shown in Table 2. According to these results, 50.26% of subjects had committed but had not reported medical errors.
Table 2.
Distribution of reporting medical errors among those who had committed and those who had not committed medical error (Chi-square test: 11.0688; P=0.001)
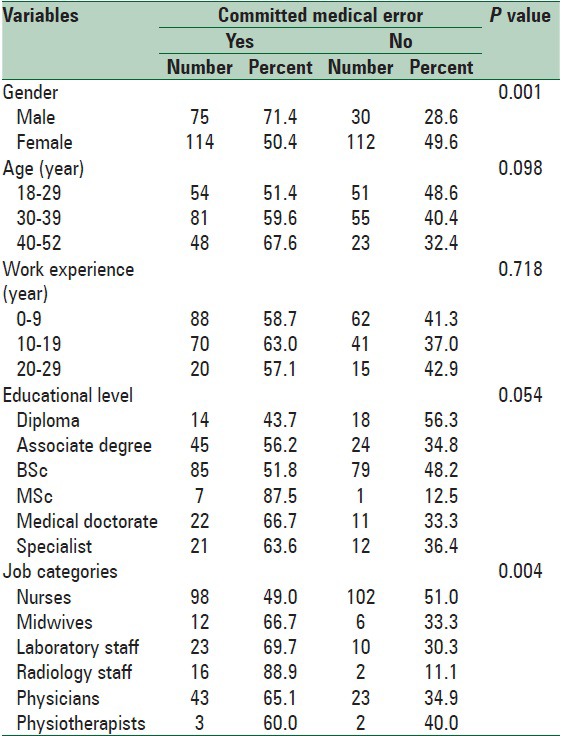
The relationship between participants’ individual characteristics and committing medical error is shown in Table 3. According to these results, the incidence rate of committing medical errors was higher in men (71.4%) than in women (50.4%), in the age group of 50–40 years (67.6%), among subjects with 0–9-year working experience (58.7%), in subjects with the educational level of MSc (87.5%), and among staffs of radiology (88.9%).
Table 3.
Relationship between participants’ individual characteristics and committing medical error using chi-squared test
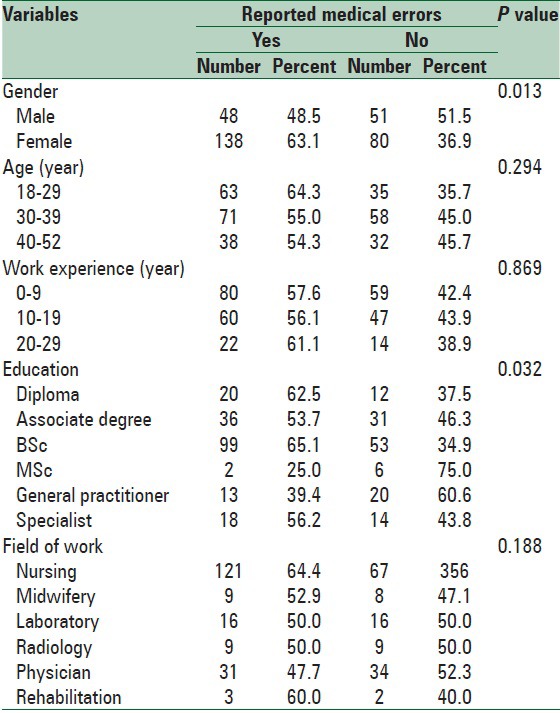
The relationship between participants’ individual characteristics and reporting medical errors is shown in Table 4. According to these results, the incidence rate of reporting medical errors was higher among women (63.1%), age group of 29–18 years (64.3%), subjects with 29–20-year work experience (61.1%), subjects with the educational level of BSc (65.1%), and nurses (64.4%).
Table 4.
Relationship between participants’ individual characteristics and reporting medical errors using Chi-square test
DISCUSSION
We indicated that the incidence rate of committing medical errors was high, but its reporting rate was low. This issue reveals the importance of establishing an effective reporting system for recording, analyzing, and managing medical errors in all organizations providing health care.
According to our results, the fear of legal consequences was 44.4%. This fear may be due to adverse consequences such as a malpractice lawsuit, losing patients’ trust, and emotional reactions of the patients and their relatives, or losing occupational position.[11,12]
Based on our findings, other reasons that participants have reported for medical error underreporting were lack of personals’ attention to the importance of medical errors and lack of effective medical error reporting system. Nursing administration's focus on the person who committed errors rather than a system in which medical errors can be registered and analyzed.[13] Such system can covert threats into opportunities to learn from the mistakes and prepare a cornerstone to eliminate the preventable causes of medical errors. Evidence has shown that an anonymous, nonpunitive critical incident reporting system can play as a powerful tool for identifying the majority of medical errors and risk factors and may help avoiding preventable adverse events.[14,15,16]
Gluck stated that some errors in health care were inevitable because of both human fallibility and the complexity of the systems. He suggested three strategies for improving patient safety as follows: (a) Prevent errors with estimating functions, reducing complexity, and providing reminders at the point of care; (b) everybody working in health care have to be alert to distinguish and eliminate potential errors before patients are harmed; (c) defensive barriers must be established to intercept those errors that still occur and prevent them from causing patient injury.[17]
An important limitation of this study was recall bias so that some participants might have committed a medical error, but they could not remember it. This might introduce information bias into the results and might lead to underestimation of the rate of medical error committed by the study population. Furthermore, we enrolled the participants into the study voluntarily and collected data anonymously in order to reduce the non-honest response rate. However, it is possible that some participants have avoided reporting the medical error that has been committed by them. This may again result in underestimation of the true rate of medical error committed by the study population. Despite it limitation, this study indicated the main barriers to medical error reporting in a high-middle income setting. Since factors affecting medical error reporting may vary between different settings, the results of this survey may help avoiding preventable adverse events caused by medical errors in such settings.
CONCLUSIONS
This study indicated the main barriers to reporting medical and associated factors that may act as barriers to error reporting. The factors outlined in this study can assist healthcare providers and healthcare organizations in improving medical error reporting as an essential component for patient safety enhancement.
ACKNOWLEDGEMENTS
We would like to thank Vic-Chancellor of Research and Technology of Hamadan University of Medical Sciences for financial support of this study (No. 920204269).
Footnotes
Source of Support: This study was funded by the Vice-chancellery for Research and Technology, Hamadan University of Medical Sciences
Conflict of Interest: None declared.
REFERENCES
- 1.Geneva: WHO; 2005. World Health Organization. Draft Guidelines for Adverse Event Reporting and Learning Systems World Health Organization Alliance for Patient Safety. [Google Scholar]
- 2.Grober ED, Bohnen JM. Defining medical error. Can J Surg. 2005;48:39–44. [PMC free article] [PubMed] [Google Scholar]
- 3.Zhang J, Patel VL, Johnson TR. Medical error: Is the solution medical or cognitive? J Am Med Inform Assoc. 2008;6:75–7. doi: 10.1197/jamia.M1232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Rodrigues S, Brandão P, Nelas L, Neves J, Alves V. A logic programming approach to medical errors in imaging. Int J Med Inform. 2011;80:669–79. doi: 10.1016/j.ijmedinf.2011.06.005. [DOI] [PubMed] [Google Scholar]
- 5.Uribe CL, Schweikhart SB, Pathak DS, Dow M, Marsh GB. Perceived barriers to medical-error reporting: An exploratory investigation. J Healthc Manag. 2002;47:263–79. [PubMed] [Google Scholar]
- 6.Wu AW. Adverse drug events and near misses: Who's counting? Am J Med. 2000;109:166–8. doi: 10.1016/s0002-9343(00)00509-x. [DOI] [PubMed] [Google Scholar]
- 7.Antonow JA, Smith AB, Silver MP. Medication error reporting: A survey of nursing staff. J Nurs Care Qual. 2000;15:42–8. doi: 10.1097/00001786-200010000-00006. [DOI] [PubMed] [Google Scholar]
- 8.Barach P, Small SD. Reporting and preventing medical mishaps: Lessons from non-medical near miss reporting systems. BMJ. 2000;320:759–63. doi: 10.1136/bmj.320.7237.759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bayazidi S, Zarezadeh Y, Zamanzadeh V, Parvan K. Medication error reporting rate and its barriers and facilitators among nurses. J Caring Sci. 2012;1:231–6. doi: 10.5681/jcs.2012.032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bahadori M, Ravangard R, Aghili A, Sadeghifar J, Gharsi Manshadi M, Smaeilnejad J. The factors affecting the refusal of reporting on medication errors from the nurses’ viewpoints: A case study in a hospital in Iran. ISRN Nurs 2013. 2013:876563. doi: 10.1155/2013/876563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ghalandarpoorattar SM, Kaviani A, Asghari F. Medical error disclosure: The gap between attitude and practice. Postgrad Med J. 2012;88:130–3. doi: 10.1136/postgradmedj-2011-130118. [DOI] [PubMed] [Google Scholar]
- 12.Helmchen LA, Richards MR, McDonald TB. How does routine disclosure of medical error affect patients’ propensity to sue and their assessment of provider quality?. Evidence from survey data. Med Care. 2010;48:955–61. doi: 10.1097/MLR.0b013e3181eaf84d. [DOI] [PubMed] [Google Scholar]
- 13.Stratton KM, Blegen MA, Pepper G, Vaughn T. Reporting of medication errors by pediatric nurses. J Pediatr Nurs. 2004;19:385–92. doi: 10.1016/j.pedn.2004.11.007. [DOI] [PubMed] [Google Scholar]
- 14.Berghauser MA, Masjosthusmann K, Rellensmann G. Risikomanagement durch CIRS-analyse. Monatsschr Kinderheilkd. 2010;158:378–83. [Google Scholar]
- 15.Edrees HH, Paine LA, Feroli ER, Wu AW. Health care workers as second victims of medical errors. Pol Arch Med Wewn. 2011;121:101–8. [PubMed] [Google Scholar]
- 16.Bucknall TK. Medical error and decision making: Learning from the past and present in intensive care. Aust Crit Care. 2010;23:150–6. doi: 10.1016/j.aucc.2010.06.001. [DOI] [PubMed] [Google Scholar]
- 17.Gluck PA. Medical error theory. Obstet Gynecol Clin North Am. 2008;35:11–7. doi: 10.1016/j.ogc.2007.12.006. [DOI] [PubMed] [Google Scholar]