

Abstract
The fractures of sesamoid bones of the hand are rare, sometimes the diagnosis is missed. We report a case of fracture of both the ulnar and radial sesamoids of the metacarpophalangeal (MCP) joint of the thumb. The trauma (hyperextension of the thumb during a soccer match) also caused a lesion of the volar plate. The diagnosis was made by ultrasound (US) and confirmed by CT scan.
Riassunto
Le fratture dei sesamoidi della mano sono eventi rari, talvolta non diagnosticati. Presentiamo il caso di una frattura che ha interessato sia il sesamoide radiale che ulnare della articolazione metacarpofalangea (MCP) del pollice. Il trauma (iperestensione del pollice durante una partita di calcio) ha inoltre causato la lesione della placca volare. La diagnosi è stata fatta con l’ecografia (US) e confermata alla TC.
Introduction
A sesamoid is a bone embedded within a tendon. This name derives from the oval seeds of the plant “sesamum indicum” [1].
Sesamoid bones are located where a tendon passes over a joint, such as the hand, wrist, knee, and foot. The main function of the sesamoid is to decrease friction and to protect the tendon.
The patella is the largest sesamoid in the human and its invariably present, while in the hand there is variability in the population. Usually, there are five sesamoids in the hand, localized in the palmar surface of joints. There are two sesamoids at the metacarpophalangeal (MCP) joint of the thumb (these are present in 99 % of the population), less common are the other: one at the interphalangeal joint of the thumb, one at the MCP joint of the index finger, and one at the MCP joint of the small finger [2].
The radial and ulnar sesamoids of the MCP joint of the thumb are interposed between the thenar muscles (flexor pollicis brevis and adductor pollicis), and the insertion of those muscles into the proximal phalanx of the thumb. This configuration gives support to the joint [3].
The volar plate (VP) is a fibrocartilagineous structure present at the volar aspect of the finger joint, deep to the flexor tendon. The VP gives insertions to the capsule [3].
The VP is important for the articular stability and limits hyperextension.
In the thumb the VP connects the radial and ulnar sesamoids by transverse fibers [4].
We report a case of a fracture of both the sesamoids of the MCP joint, associated with a lesion of the VP.
Case report
A 17-year-old boy suffered a hyperextension of the thumb of his left hand during a soccer game, in which he was playing as a goalkeeper.
For persistent pain, both on pressure at the volar aspect of the MCP joint and in hyperextension of the thumb, a week after the trauma he had an X-ray examination of the thumb (Fig. 1): no clear fracture was reported, but a sesamoid involvement was suspected and further imaging options were suggested.
Fig. 1.

X-ray. Left image AP view of the thumb. No fracture can be clearly seen. On the right lateral view of the thumb. The fracture of the thumb sesamoid was suspected
An ultrasound (US) examination was performed. The exam was carried out with an iU22 system (Philips Medical Systems, Bothell, WA) and a 12–5 MHz linear transducer.
It was focused on the site of clinical pain: gray-scale and Color-Doppler images of the volar and dorsal aspect of the MCP joint of the thumb were obtained.
The ulnar collateral ligament (UCL), which is frequently involved in case of MCP joint trauma and mainly in valgus stress—the so-called gamekeeper’s thumb—was regular [5, 6].
At the volar aspect of the MCP joint the US scan showed the irregularity of both the ulnar sesamoid and the radial one, with interruption of the bony cortex, due to fracture. Pressure with the probe over that region was painful. There was a lesion of the VP too.
A CT examination of the hand was made to confirm the fracture of the two sesamoid bones and for a detailed localization of the bony fragments.
CT was performed with a spiral 64-channel scanner (Philips Brilliance 64). Axial, sagittal, coronal reconstructed images and three-dimensional reconstructed images were obtained from the volumetric data.
Below there are the US scans in parallel with the corresponding CT image, showing how the images of the two methods are overlapping (Figs. 2, 3, 4, 5, 6).
Fig. 2.
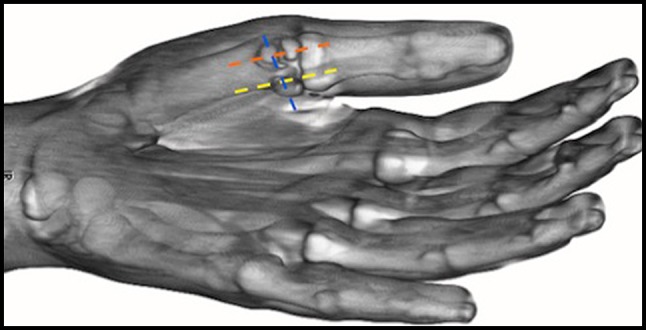
Three-dimensional reconstruction of the CT exam. Dashed lines indicate US scan planes
Fig. 3.
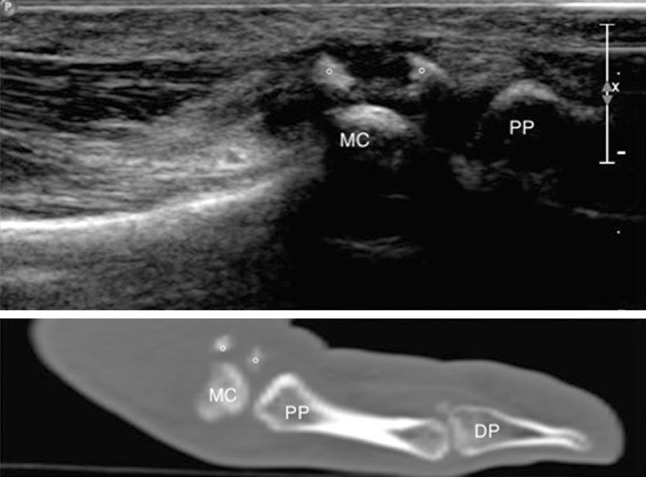
Longitudinal US scan (on top) with corresponding CT image (below) over the radial sesamoid of the MCP joint of the thumb demonstrates the fragments (open circle) of the sesamoid. MC first metacarpal, PP proximal phalanx, DP distal phalanx
Fig. 4.
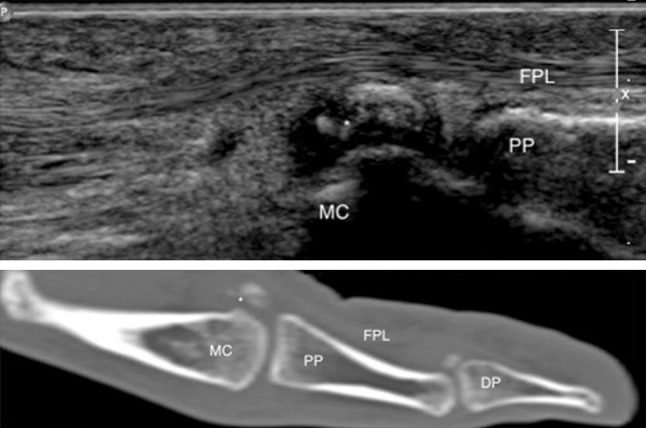
Longitudinal US scan (on top) with corresponding CT image (below) over the ulnar sesamoid of the MCP joint of the thumb demonstrates the fragments (asterisk) of the sesamoid. MC first metacarpal, PP proximal phalanx, DP distal phalanx, FPL flexor pollicis longus
Fig. 5.
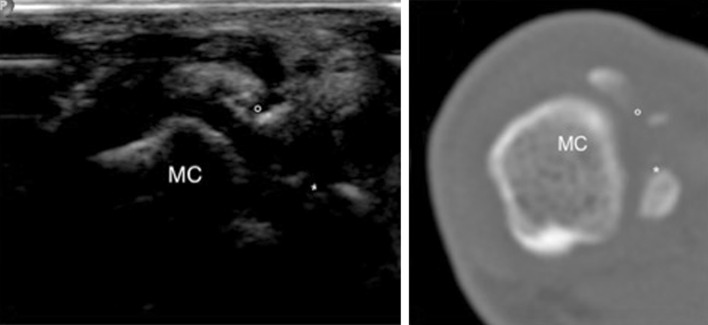
Fracture of the sesamoids of the MCP joint. Transverse US scan over the MCP joint (on the left) with corresponding CT image (right). MC first metacarpal, Asterisk fragments of the ulnar sesamoid, Open circle fragments of the radial sesamoid
Fig. 6.
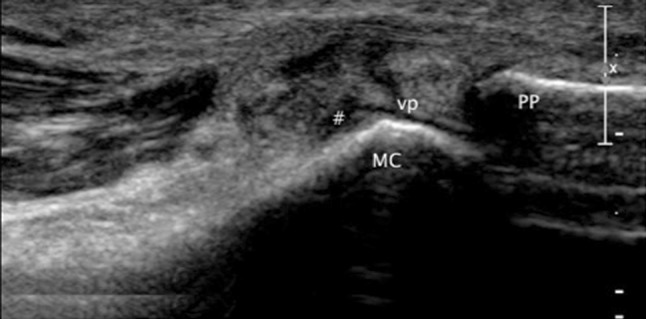
Longitudinal US scan (in an intermediate plane between the one in Fig. 3 and in Fig. 4) over the MCP joint of the thumb shows a lesion of the volar plate (vp): it is swollen, there is a hypoechoic cleft, reflecting the tear. There is also intra-articular fluid distension (Hash symbol) of the MCP joint. MC first metacarpal, PP proximal phalanx
Discussion
Fractures of the thumb MCP sesamoids are rare. The mechanism of injury is a sudden hyperextension of the joint. Sometimes it can be the result of a direct trauma [3, 4, 7].
Clinically, patients can have ecchymosis on the flexor side of the thenar eminence and tenderness at the MCP joint, at the level of one or both the sesamoid bones [3, 4].
This lesion is frequently missed: routine anteroposterior examination using conventional X-ray imaging may not reveal the fracture, therefore other views, like lateral or oblique, should be obtained to make the correct diagnosis [4]. Advanced imaging studies usually are not required. However, if clinically indicated, a precise assessment of a fracture pattern can be obtained with CT scan. US is not the modality of choice to evaluate bone fractures, but may be useful to detect sesamoid fractures, when clinically or radiographically overlooked. US findings require correlation with physical examination and patient’s history and have to be confirmed with accessory radiographic projections or CT [8–11].
US depicts the fracture showing the irregular shape of the sesamoid and the presence of fragment(s) close to it, reflecting cortical avulsion (Figs. 3, 4, 5). Haematoma and oedema of the surrounding tissue can be associated and Color-Doppler can show increased vascularity [9, 10].
The differentiation between bipartite sesamoids and fracture is possible because in the latter case there is an absence of rounded regular contours and from a clinical point of view there is pain when pressing that region [4, 8, 12].
VP injuries can be the result of hyperextension of the MCP joint too. In the thumb, VP lesions can be associated with UCL injury or sesamoid fracture [5].
The plate can be torn with or without an avulsion fracture: in case there is an avulsion of a bony fragment the injury can be diagnosed with X-ray. Intrasubstance tear of the VP can occur [8]: in this latter case arthrography can demonstrate contrast leakage from the volar aspect of the joint [7]. MR imaging of the fingers has been employed in the pathology of the VP to evaluate the state of the plate and to precisely identify its location and displacement [5, 12]. US might be an excellent imaging technique for the diagnosis of these injuries [5, 9, 10, 13]. At US, in sagittal scan over the palmar aspect of the MCP joint of the thumb, a normal VP appears as a triangular echogenic and homogeneous structure deep to the flexor pollicis longus tendon [5, 10].
In case of a tear of the VP US shows that the fibrocartilagineous structure is swollen and there is an intrasubstance hypoechoic cleft; these findings can be associated with fluid distension of the joint (Fig. 6). When an avulsion fragment is present, US can depict it and it is possible to measure its size and the amount of displacement [8, 10].
In our case, the ultrasonographic examination has established the correct diagnosis: fracture of both the sesamoids bones at the MCP joint of the thumb associated with injury to the VP at that level. In literature, there are some other similar cases diagnosed by arthrography [7, 14], but to the best of our knowledge there are no other cases reported of such an associated injury, in which the diagnosis was made by US.
US is a safe, well-tolerated and non-invasive imaging technique. It is cheap, easily accessible and it allows dynamic examination. The accuracy of musculoskeletal US depends on the experience of the physician and the equipment. Detailed knowledge of normal anatomy and anatomic variants is essential, as well as the skill to correlate imaging findings with clinical data. Higher frequencies transducer (17 or 18 MHz) could be helpful in the sonographic evaluation of the hand, but in our case diagnosis was possible with a 12-MHz transducer [5, 6, 8–10].
Even if X-ray examination usually is enough to diagnose the fracture of a sesamoid, in the setting of a trauma in hyperextension involving the MCP joint, US should be considered a complementary exam, showing not only the fracture itself, which might not have been evident on the X-ray, but also can be useful to evaluate other structures, like tendons, ligaments and the VP: this last structure was damaged in the case we presented.
Conflict of interest
The authors have no conflict of interest.
Informed consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. All patients provided written informed consent for enrolment in the study and for the inclusion in this article of information that could potentially lead to their identification.
Human and animal studies
The study was conducted in accordance with all institutional and national guidelines for the care and use of laboratory animals.
References
- 1.Wood VE. The sesamoid bones of the hand and their pathology. J Hand Surg. 1984;9B:261–264. doi: 10.1016/0266-7681(84)90038-X. [DOI] [PubMed] [Google Scholar]
- 2.Amar E, Rozenblat Y, Chechik O. Sesamoid and accessory bones of the hand—an epidemiologic survey in a Mediterranean population. Clin Anat. 2011;24:183–187. doi: 10.1002/ca.21077. [DOI] [PubMed] [Google Scholar]
- 3.Gibeault JD, Saba P, Hoenecke H, Graham A. The sesamoids of the metacarpophalangeal joint of the thumb: an anatomical and clinical study. J Hand Surg. 1989;14:244–247. doi: 10.1016/0266-7681(89)90139-3. [DOI] [PubMed] [Google Scholar]
- 4.Dong PR, Seeger LL, Shapiro MS, Levere SM. Fractures of the sesamoid bones of the thumb. Am J Sports Med. 1995;23:336–339. doi: 10.1177/036354659502300315. [DOI] [PubMed] [Google Scholar]
- 5.Ebrahim FS, De Maeseneer M, Jager T, Marcelis S, Jamadar DA, Jacobson JA. US diagnosis of UCL tears of the thumb and Stener lesions: technique, pattern-based approach and differential diagnosis. Radiographics. 2006;26:1007–1020. doi: 10.1148/rg.264055117. [DOI] [PubMed] [Google Scholar]
- 6.Melville D, Jacobson JA, Haase S, Brandon C, Kalume Brigido M, Fessell D. Ultrasound of displaced ulnar collateral ligament tears of the thumb: the Stener lesion revisited. Skelet Radiol. 2013;42:667–673. doi: 10.1007/s00256-012-1519-x. [DOI] [PubMed] [Google Scholar]
- 7.Bianchi S, Abdelwaha IF, Zwass A, Molini L. Fractures of the sesamoid bone of the thumb. Bull Hosp Jt Dis. 1993;53:7–10. [PubMed] [Google Scholar]
- 8.Bianchi S, Almusa E, Chick G, Bianchi E (2013) Ultrasound in wrist and hand sport injuries. Sports Med J pp 374–383
- 9.Bianchi S, Jacob D, Hoffman D, Almusa E. When to order specific radiological investigations. In: Chick G, editor. Acute and chronic finger injuries in ball sports. Paris: Springer; 2013. [Google Scholar]
- 10.Bianchi S, Martinoli C (2007) Hand. In: Ultrasound of the musculoskeletal system. Springer Berlin pp 495–548
- 11.Hoffman DF, Adams E, Bianchi S (2014) Ultrasonography of fractures in sports medicine. Br J Sports Med [DOI] [PubMed]
- 12.Clavero JA, Alomar X, Monill JM, et al. MR imaging of ligament and tendon injuries of the fingers. Radiographics. 2002;22(2):237–256. doi: 10.1148/radiographics.22.2.g02mr11237. [DOI] [PubMed] [Google Scholar]
- 13.Boutry N, Larde A, Demondion X, Cortet B, Cotten H, Cotten A. Metacarpophalangeal joints at US in asymptomatic volunteers and cadaveric specimens. Radiology. 2004;232:716–724. doi: 10.1148/radiol.2323031075. [DOI] [PubMed] [Google Scholar]
- 14.Bell MJ, McMurtry RY, Rubenstein J. Fracture of the ulnar sesamoid of the metacarpophalangeal joint of the thumb-an arthrographic study. J Hand Surg Br. 1989;10(3):379–381. doi: 10.1016/S0266-7681(85)80067-X. [DOI] [PubMed] [Google Scholar]