

Abstract
Context:
A clinical case of a tibia plateau fracture is presented which was treated with balloon osteoplasty and arthroscopy guidance. Balloon Tibioplasty has been shown to be a very useful method for the management of tibial plateau fractures. The use of calcium phosphate has been described in the literature for management and restoration of bone defects in tibial plateau fractures.
Case Report:
A 45-years-old Caucasian woman was presented after a fall from a ladder. The patient sustained a lateral tibia plateau fracture which was classified as Shatzker type III (AO 41-B2) with posterolateral depression of the joint surface. Surgical treatment was applied using a minimal approach which included percutaneous reduction of the fracture under arthroscopy and fluoroscopy guidance. The bone defect was filled with calcium phosphate via injection. The clinical outcome at the 6, 12 and 24 weeks was excellent with full-range of motion of the knee joint.
Conclusion:
Arthroscopy assisted balloon osteoplasty seems to be a safe and effective method for the treatment of depressed tibia plateau fractures. Further study is needed for the proper evidence based use and application of this method.
Keywords: Arthroscopy, balloon osteoplasty, calcium phosphate, tibial plateau
Introduction
Depression tibia plateau fractures are considered one of the most difficult to manage. The classical approach for the treatment of these fractures is open reduction and internal fixation with the use of autologous cancellous grafting.[1] In many cases there is a doubt regarding the decision making because of the complexity and the difficulty in anatomical reduction. Recent advances have showed the use of calcium phosphate for the treatment of bone defects.[1,2] The use of balloon kyphoplasty, for the treatment of depressed vertebrae fractures, show that split and cracked fractures can be managed with the eggshell technique.[3] Balloon tibioplasty can be used in the same way for the treatment of similar fracture patterns as literature dictates.[4]
In our study we present a clinical case of a Schatzker III tibial plateau fracture with depression of the posterior articular surface (AO 41-B2) which was treated with arthroscopy assisted balloon osteoplasty. The authors have obtained the patient's informed written consent for print and electronic publication of the case report.
Case Presentation
A 45-year-old Caucasian woman presented to the emergency department of the University Hospital of Heraklion, Crete after a fall from a ladder. The patient occupied in everyday activities as a house wife and a farmer. There were no concomitant injuries. Thorough clinical examination and radiological imaging revealed a depression fracture of the lateral tibia plateau which was classified as Schatzker III/AO 41-B2 [Figure 1]. Radiological examination by a computed tomography (CT) scan was performed [Figure 2], which showed the details and personality of this specific fracture to assist in decision making.
Figure 1.
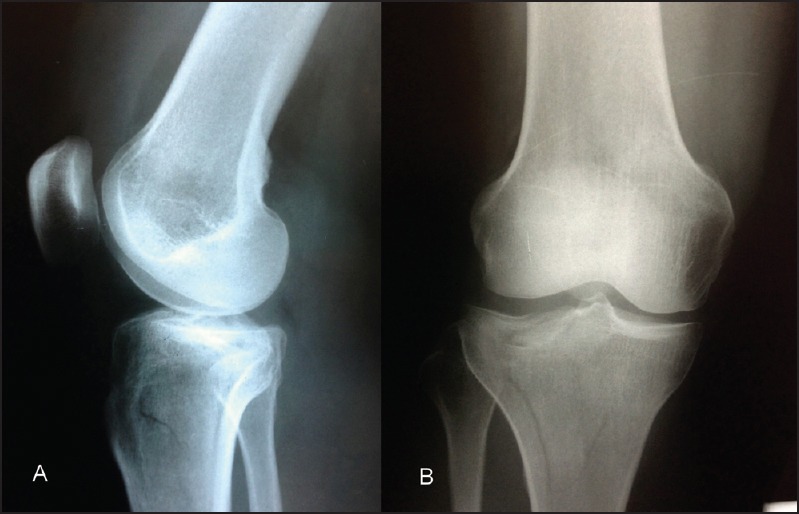
Initial radiological imaging (a) lateral and (b) PA view demonstrating the minimal displacement and the difficulty in proper viewing of the fracture
Figure 2.
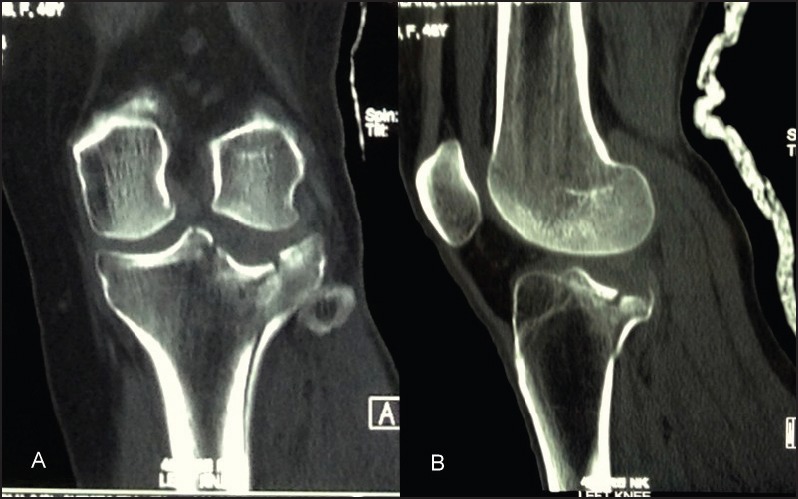
CT scan, (a) coronal view showing the depression of the articular surface and (b) sagittal view demonstrating the posterior placement of the fracture site
Estimated the clinical and radiological findings as well as the needs of the patient, surgical treatment was decided.
Taking into account that the position of the fracture was at the most posterior area of the lateral plateau and the difficulties from open reduction of the articular surface, closed reduction via a minimal incision arthroscopically and fluoroscopy assisted using balloon kyphoplasty instrumentation was performed [Figure 3]. After reduction of the articular surface confirmed by arthroscopy the bone defect was filled with calcium phosphate via injection [Figure 4]. The fracture was considered a stable one and no further support and fixation was needed.
Figure 3.
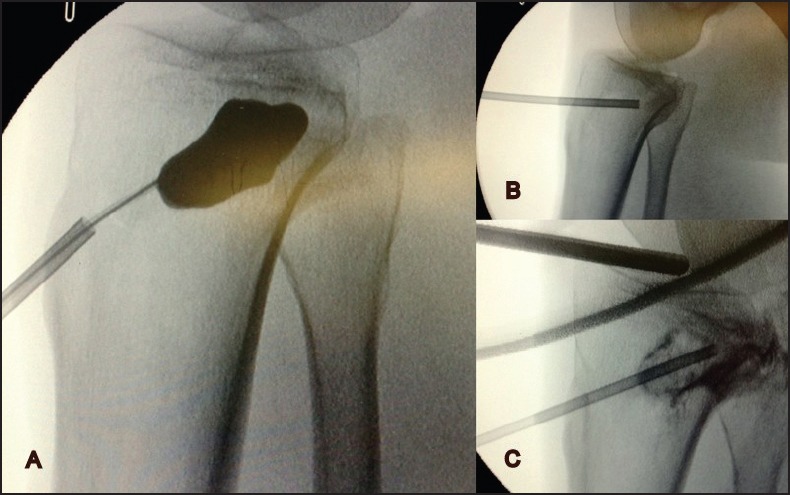
Fluoroscopy images, (a) widening of the bone defect at the fracture site using balloon, (b) proper placement of the trochar under the articular surface, (c) the cancellous cavity ready to be filled up with calcium phosphate
Figure 4.
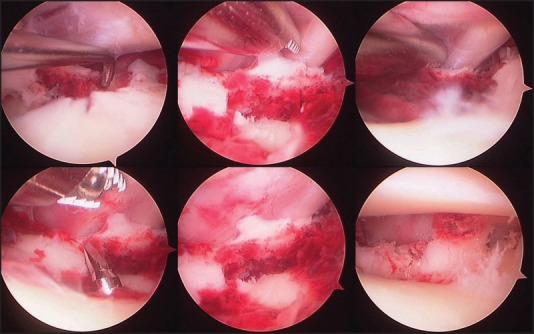
Continuous imaging from the arthroscopic camera showing the heamatoma formation at the fracture, the penetration of the trochar into the joint and the final image of the articular surface after the placement of calcium phosphate
Initial immobilization was obtained with a log leg cast for 2 days. Afterwards, continuous passive motion (CPM) was started with flexion and extension as tolerable. The patient started to walk with crutches and no weight bearing. A knee cast with goniometer was placed permitting knee exercises in flexion and extension. The patient was discharged from the hospital on the 5th postoperative day in a very good condition.
The patient was examined 6, 12 and 24 weeks after the operation regarding the movements of the joint and the muscle strength. A CT scan was ordered at the 6 week follow-up for a detailed evaluation and imaging of the tibial plateau [Figure 5]. The clinical outcome was excellent at the 6, 12 and 24 weeks follow-up with full range of motion of the knee joint. The patient didn’t report any issues regarding her rehabilitation. At the 12 week follow up partially weight bearing was started as tolerable. At the 24 week follow-up full weight bearing was already achieved by the patient with no reporting problems.
Figure 5.
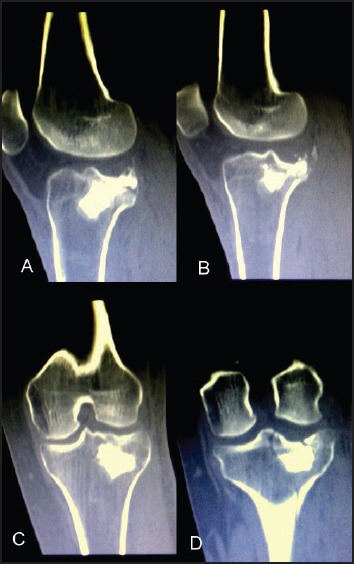
12w CT scan imaging, (a) and (b) sagittal views showing the support and maintenance of the reduction and (c), (d) coronal views showing the articular surface which is in anatomical position
Discussion
The use of calcium phosphate has been described in the literature for management and restoration of bone defects in tibial plateau fractures by many authors.[1,2,5] It has been found that these materials get stiff enough without producing heat, get stronger with the application of compression and restructure slowly in vivo.[2,6] Calcium phosphate has the ability to effectively replace autologous bone grafting for the treatment of tibial plateau fractures.[5,7] Arthroscopy has its specific role and has been used in such cases to assist in observation of the joint surface.[8] It has been found that arthroscopic assisted management of tibial plateau fractures allows early rehabilitation, short hospitals stay and low complications rate.[9] The open surgical technique demonstrated similar long term results and arthroscopy had no influence in the anatomical reduction.[10,11]
In the present case the tibial plateau fracture was a frank depression of the articular surface at the posterior area of the external tibial condyle. Reduction of the depressed segment of the subchondral bone restored the congruity of the joint. Fulfillment of bone cavity, created by balloon inflation during fracture reduction, with calcium phosphate supported the subchondral bone preventing fracture redisplacement during healing postoperative period.[4,12] Using balloïn tibioplasty arthroscopically assisted permits management of appropriate tibial plateau fractures with less surgical trauma assisting in better functional recovery.[12,13,14] This technique has been used for the treatment of other type of fractures in other anatomical regions.[15] Also, this method is coupled with the use of open reduction and internal fixation and showed very promising results.[16]
Our patient exhibited very good clinical results during the postoperative period with full-range of knee motion and return to previous functional activities. Other studies showed similar outcomes in relation to the reduced non-weight bearing postoperative period and the avoidance of the articular collapse.[17] In the same manner, superior results were shown with the use of the method in regard with the anatomic outcome than the use of buttress plating and bone grafting.[18,19]
Although there are complications by the use of arthroscopy for the treatment of tibial plateau fractures, such as compartment syndrome, those are infrequent but if they occur have the potential to be severe.[20] It must be noted that the pressure of the pump irrigator, for the evacuation of the hematoma and joint lavage, should not exceed 50 mmHg to minimize the risk of compartment syndrome.[21]
In conclusion, the use of calcium phosphate with arthroscopy assisted minimal invasive technique for the treatment of depressed tibial plateau fractures is a very promising method in appropriate fracture pattern cases. Our patient demonstrated great results with full functional recovery and no complications. Further study needs to be done for the assessment and clinical use of this method as established evidence based application for the treatment of intra-articular fractures. This technique can achieve reliable reduction and adequate stabilization which permits early mobilization and excellent functional results.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Goff T, Kanakaris NK, Giannoudis PV. Use of bone graft substitutes in the management of tibial plateau fractures. Injury. 2013;44:S86–94. doi: 10.1016/S0020-1383(13)70019-6. [DOI] [PubMed] [Google Scholar]
- 2.Larsson S, Bauer TW. Use of injectable calcium phosphate cement for fracture fixation: A review. Clin Orthop Relat Res. 2002;395:23–32. doi: 10.1097/00003086-200202000-00004. [DOI] [PubMed] [Google Scholar]
- 3.Bouza C, López T, Magro A, Navalpotro L, Amate JM. Efficacy and safety of balloon kyphoplasty in the treatment of vertebral compression fractures: A systematic review. Eur Spine J. 2006;15:1050–67. doi: 10.1007/s00586-005-0048-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Pizanis A, Garcia P, Pohlemann T, Burkhardt M. Balloon tibioplasty: A useful tool for reduction of tibial plateau depression fractures. J Orthop Trauma. 2012;26:e88–93. doi: 10.1097/BOT.0b013e31823a8dc8. [DOI] [PubMed] [Google Scholar]
- 5.Yin X, Li J, Xu J, Huang Z, Rong K, Fan C. Clinical assessment of calcium phosphate cement to treat tibial plateau fractures. J Biomater Appl. 2013;28:199–206. doi: 10.1177/0885328212443295. [DOI] [PubMed] [Google Scholar]
- 6.Lobenhoffer P, Gerich T, Witte F, Tscherne H. Use of a injectable calcium phosphate bone cement in the treatment of tibial plateau fractures: A prospective study of twenty-six cases with twenty-month mean follow-up. J Orthop Trauma. 2002;16:143–9. doi: 10.1097/00005131-200203000-00001. [DOI] [PubMed] [Google Scholar]
- 7.McDonald E, Chu T, Tufaga M, Marmor M, Singh R, Yetkinler D, et al. Tibial plateau fracture repairs augmented with calcium phosphate cement have higher in situ fatigue strength than those with autograft. J Orthop Trauma. 2011;25:90–5. doi: 10.1097/BOT.0b013e3181e3e28f. [DOI] [PubMed] [Google Scholar]
- 8.Buchko GM, Johnson DH. Arthroscopy assisted operative management of tibial plateau fractures. Clin Orthop Relat Res. 1996;332:29–36. doi: 10.1097/00003086-199611000-00006. [DOI] [PubMed] [Google Scholar]
- 9.Evangelopoulos DS, Heitkemper S, Eggli S, Haupt U, Exadaktylos AK, Benneker LM. Percutaneous cement augmentation for the treatment of depression fractures of the tibial plateau. Knee Surg Sports Traumatol Arthrosc. 2010;18:911–5. doi: 10.1007/s00167-009-1003-x. [DOI] [PubMed] [Google Scholar]
- 10.Cassard X, Beaufils P, Blin JL, Hardy P. Osteosynthesis under arthroscopic control of separated tibial plateau fractures. 26 case reports. Rev Chir Orthop Reparatrice Appar Mot. 1999;85:257–66. [PubMed] [Google Scholar]
- 11.Horstmann WG, Verheyen CC, Leemans R. An injectable calcium phosphate cement as a bone-graft substitute in the treatment of displaced lateral tibial plateau fractures. Injury. 2003;34:141–4. doi: 10.1016/s0020-1383(02)00105-5. [DOI] [PubMed] [Google Scholar]
- 12.Mauffrey C, Roberts G, Cuellar DO, Herbert B, Hak D. Balloon tibioplasty: Pearls and pitfalls. J Knee Surg. 2014;27:31–7. doi: 10.1055/s-0033-1363516. [DOI] [PubMed] [Google Scholar]
- 13.Ahrens P, Sandmann G, Bauer J, König B, Martetschläger F, Müller D, et al. Balloon osteoplasty- a new technique for reduction and stabilisation of impression fractures in the tibial plateau: A cadaver study and first clinical application. Int Orthop. 2012;36:1937–40. doi: 10.1007/s00264-012-1592-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bansal MR, Bhagat SB, Shukla DD. Bovine cancellous xenograft in the treatment of tibial plateau fractures in elderly patients. Int Orthop. 2009;33:779–84. doi: 10.1007/s00264-008-0526-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Yu B, Han K, Ma H, Zhang C, Su J, Zhao J, et al. Treatment of tibial plateau fractures with high strength injectable calcium sulphate. Int Orthop. 2009;33:1127–33. doi: 10.1007/s00264-008-0611-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Broome B, Mauffrey C, Statton J, Voor M, Seligson D. Inflation osteoplasty: In vitro evaluation of a new technique for reducing depressed intra-articular fractures of the tibial plateau and distal radius. J Orthop Traumatol. 2012;13:89–95. doi: 10.1007/s10195-012-0185-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Oztürkmen Y, Caniklioğlu M, Karamehmetoğlu M, Sükür E. Calcium phosphate cement augmentation in the treatment of depressed tibial plateau fractures with open reduction and internal fixation. Acta Orthop Traumatol Turc. 2010;44:262–9. doi: 10.3944/AOTT.2010.2406. [DOI] [PubMed] [Google Scholar]
- 18.Yetkinler DN, McClellan RT, Reindel ES, Carter D, Poser RD. Biomechanical comparison of conventional open reduction and internal fixation versus calcium phosphate cement fixation of a central depressed tibial plateau fracture. J Orthop Trauma. 2001;15:197–206. doi: 10.1097/00005131-200103000-00009. [DOI] [PubMed] [Google Scholar]
- 19.Simpson D, Keating JF. Outcome of tibial plateau fractures managed with calcium phosphate cement. Injury. 2004;35:913–8. doi: 10.1016/S0020-1383(03)00109-8. [DOI] [PubMed] [Google Scholar]
- 20.Belanger M, Fadale P. Compartment syndrome of the leg after arthroscopic examination of a tibial plateau fracture: Case report and review of the literature. Arthroscopy. 1997;13:646–51. doi: 10.1016/s0749-8063(97)90196-1. [DOI] [PubMed] [Google Scholar]
- 21.Burdin G. Arthroscopic management of tibial plateau fractures: Surgical technique. Orthop Traumatol Surg Res. 2013;99:S208–18. doi: 10.1016/j.otsr.2012.11.011. [DOI] [PubMed] [Google Scholar]