

Abstract
Aim:
Tobacco use is the major cause of oral cancer, which is the sixth most common form of malignancy globally. Even in the absence of clinical manifestations, early changes in the oral mucosa can be detected microscopically by exfoliative cytology. The present study aimed to study and compare the cellular changes in the oral mucosa of tobacco users using cytomorphometry.
Materials and Methods:
A total of 80 subjects were included: 20 without any tobacco use habits, 20 tobacco chewers, 20 smokers, and 20 mishri users. Smears were collected from each subject, fixed, and stained using Papanicolaou stain. All slides were evaluated for nuclear and cytoplasmic changes using image analysis software.
Results:
Statistically significant decrease in cytoplasmic area and an increase in nuclear area and nuclear-cytoplasmic ratio were observed in tobacco users.
Conclusion:
Tobacco in any form causes significant cellular changes, which could be the earliest indicators of developing malignant pathology. Exfoliative cytology can be used to detect such changes.
Keywords: Cytomorphometry, exfoliative cytology, oral cancer, Papanicolaou stain
INTRODUCTION
Oral cancer is one of the most widely prevalent malignancies in developing countries and is caused largely due to tobacco use.[1] Different forms of tobacco usage, endemic to certain areas, are prevalent in India. The habit of placing tobacco mixed with lime; usually in the canine — premolar region of the mandibular sulcus is widespread in the rural population of central Maharashtra, India.[2,3] Masheri, also called Mishri, is made at home by roasting tobacco flakes on a hot griddle until it turns brown or black. It is applied to gums and teeth and retained in the mouth for variable time period.[2] Despite the easy accessibility of oral cancer to self-examination, it is usually diagnosed at advanced stages, resulting in poor prognosis, and survival rate among patients. The morbidity and mortality rates of oral cancer have not decreased despite advances in therapeutic techniques, leading to increased treatment costs, and complications. Hence, the early diagnosis of oral cancers is critical for successful treatment.[1]
Exfoliative cytology is a noninvasive technique that is well accepted by patients and is a good diagnostic modality for the early diagnosis of oral mucosal lesions.[3] Oral exfoliative cytology is particularly valuable for mass screening purposes; with a sensitivity of 94%, and specificity of 100%.[4] Recent advances in technology facilitates the use of reliable quantitative techniques such as cytomorphometry, histometry, and computer-assisted image analyzer.[4] The evaluation of parameters such as nuclear area (NA), cytoplasmic area (CA), and ratio of NA/CA (N/C), may increase the sensitivity of exfoliative cytology for early diagnosis since these are precise, objective, and reproducible.[5,8]
MATERIALS AND METHODS
Eighty subjects were included in the study and divided into following 4 groups. Group 1: Subjects without any tobacco habits (control)-20; Group 2: Tobacco chewers-20; Group 3: Smokers-20; Group 4: Mishri users-20.
After approval from Institutional Ethical Committee, written informed consent was obtained from subjects. This study was carried out in the Department of Oral and Maxillofacial Pathology, YMT Dental College and Hospital, Kharghar, Navi Mumbai, India.
Inclusion criteria for tobacco users
Tobacco users without any clinically evident lesions.
Tobacco users with a habit for more than 5 years.
Exclusion criteria
Patients with mixed habits.
Patients with any systemic diseases.
After routine oral examination, subjects were asked to rinse their mouth with a normal saline solution for 2 min to eliminate debris and excess of saliva. Oral mucosal cells were scrapped from the buccal mucosa and gingiva (in mishri users) using moistened wooden spatula. Smear was prepared on the precleaned microscopic slide. Just prior to drying, the smears were fixed with commercially available alcohol fixative (Biofix). The slides were then stained with Papanicolaou stain (RAPID PAP Kit). The slide was studied in stepwise manner, moving the slide from left upper corner to the right and then down in order to avoid measuring the same cell again. Photomicrographs were obtained at ×40 magnification for individual unfolded cells with a clear outline. Fifty cells per slide were analyzed for CA, NA, and NA/CA (N/C) ratio using Motic, Image Plus, version 2.0 software [Figures 1a, b and 2]. Statistical analysis was done using ANOVA test followed by post-hoc analysis using Tukey's honestly significant difference test.
Figure 1.
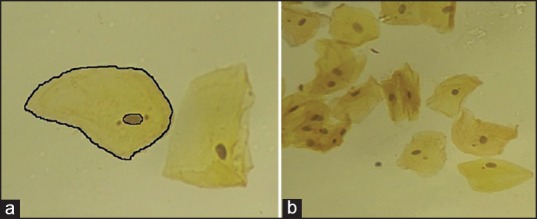
(a) Nuclear and cellular outline marked for cytomorphometry. (b) Cytological smear of normal oral mucosa stained with Papanicolaou stain (×40)
Figure 2.
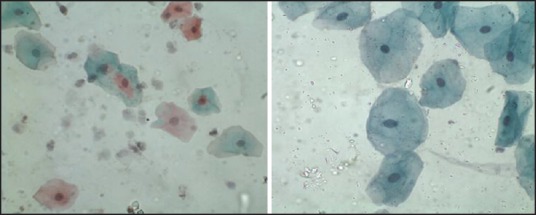
Cytological smear of tobacco users stained with Papanicolaou stain (×40)
RESULTS
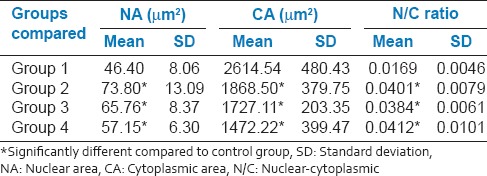
All patients were between 25 and 60 years of age. All tobacco chewers and smokers were male whereas all mishri users were female, as these habits are more prevalent in the respective genders. The mean values for NA, CA and the nuclear cytoplasmic ratio for all four groups are shown in Table 1. A statistically significant difference (P < 0.5) was observed in all parameters between control group and tobacco users [Table 1]. There was a decrease in CA and an increase in NA in Group 2, Group 3, and Group 4. NA was largest in-group 2 followed by Group 3 and Group 4. On the other hand, CA was least in-Group 3 followed by Group 2 and Group 4. The present study also indicated that there was a maximum increase in N/C ratio in-Group 4 followed by Group 2 and Group 3 [Table 1].
Table 1.
Mean of NA, CA and N/C ratio
DISCUSSION
Oral exfoliative cytology is a simple and noninvasive diagnostic technique that can be used for early detection of potentially malignant lesions. Cytomorphology assesses parameters such as cellular diameter (CD), nuclear diameter (ND), NA, CA, N/C ratio, nuclear shape, nuclear membrane continuity, optical density, and nuclear texture.[6] These quantitative techniques may increase the sensitivity of exfoliative cytology for the early diagnosis of oral cancers, as they are precise, objective, and reproducible.[6,7]
All of the major forms of tobacco such as cigarettes, cigars, pipes, and smokeless tobacco (chewing tobacco and snuff) are known to cause oral cancer. During malignant transformation, changes occur at the cellular level before clinical changes become evident. Identification of high-risk oral premalignant lesions and intervention is one of the keys to reducing the mortality, morbidity, and cost of treatment associated with oral squamous cell carcinoma.[3] Cytomorphological alterations in the form of a reduction in CD and increase in ND is reported in buccal squames of tobacco users in the South Indian population.[2] ND of oral mucosal cells in cigarette smokers and betel quid users was significantly greater than nonusers while the cytoplasmic diameter among tobacco users was significantly lesser than the control group.[9] A 5-16.5% average increase in the NA is reported among smokers when compared to non-smokers.[10,11] In the present study, significantly altered values were observed for all the three measured parameters (NA, CA, and N/C ratio) in the group using various forms of tobacco [Table 1]. These changes were directly related to the duration and frequency of habit.
Increase in nuclear size is a cellular adaptation in response to an oral epithelial lesion. Oral epithelial cells have a decreased turnover, so cells remain in the cell cycle for longer periods resulting in a delayed cell division, which in turn increases the nuclear size. The sizes of the nucleus and cytoplasm decline with aging.[12] N/C ratio has the advantage of relating nuclear volume to cytoplasmic volume and possibly represents the significant changes that occur in the cell, which more accurately identified at a morphological level.[2] The cellular changes seen in the present study can be partly attributed to the fact that tobacco on consumption releases various byproducts such as nitrosamine and nitrosonornicotine, which can influence cellular morphometry. In tobacco chewers and mishri users, there is a close contact of these byproducts thus facilitating their infiltration into the mucosa, which may be responsible for the pronounced cellular changes. Our study emphasizes the importance of early recognition of cellular alterations caused by tobacco use. It showed a decrease in the CA and an increase in the NA and N/C ratio in cells isolated from the buccal mucosa and gingiva cells of tobacco users. These could be used as early indicators of dysplastic changes in the oral mucosa and should necessitate appropriate early preventive measures to avoid the development of oral malignancies.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Hashemipour MA, Aghababaie M, Mirshekari TR, Asadi-Shekaari M, Tahmasbi-Arashlow M, Tahmasbi-Arashlow F, et al. Exfoliative cytology of oral mucosa among smokers, opium addicts and non-smokers: A cytomorphometric study. Arch Iran Med. 2013;16:725–30. [PubMed] [Google Scholar]
- 2.Hande AH, Chaudhary MS. Cytomorphometric analysis of buccal mucosa of tobacco chewers. Rom J Morphol Embryol. 2010;51:527–32. [PubMed] [Google Scholar]
- 3.Buch AC, Patel SS, Chandanwale SS, Kumar H, Patel KM, Sunita A. Study of oral exfoliative cytology in tobacco chewers of western India. Int J Pharma Bio Sci. 2014;4:138–43. [Google Scholar]
- 4.Rajesh S, Reddy SB, Shriniwas K. Cytomorphometric analysis of obtained squamesobtained from normal oral mucosa and lesions of oral submucous fibrosis. J Indian Acad Oral Med Radiol. 2012;24:200–5. [Google Scholar]
- 5.Goregen M, Akgul HM, Gundogdu C. The cytomorphological analysis of buccal mucosa cells in smokers. Turk J Med Sci. 2011;41:205–10. [Google Scholar]
- 6.Einstein TB, Sivapathasundharm B. Cytomorphometric analyses of the buccal mucosa of tobacco users. Indian J Dent Res. 2005;16:42–46. [PubMed] [Google Scholar]
- 7.Ogden GR, Cowpe JG, Wight AJ. Oral exfoliative cytology: Review of methods of assessment. J Oral Pathol Med. 1997;26:201–5. doi: 10.1111/j.1600-0714.1997.tb01224.x. [DOI] [PubMed] [Google Scholar]
- 8.Bhonsle RB, Murti PR, Daftary DK, Mehta FS. An oral lesion in tobacco-lime users in Maharashtra, India. J Oral Pathol. 1979;8:47–52. doi: 10.1111/j.1600-0714.1979.tb01621.x. [DOI] [PubMed] [Google Scholar]
- 9.Ramaesh T, Mendis BR, Ratnatunga N, Thattil RO. The effect of tobacco smoking and of betel chewing with tobacco on the buccal mucosa: A cytomorphometric analysis. J Oral Pathol Med. 1999;28:385–8. doi: 10.1111/j.1600-0714.1999.tb02108.x. [DOI] [PubMed] [Google Scholar]
- 10.Babuta S, Garg R, Mogra K, Dagal N. Cytomorphometrical analysis of exfoliated buccal mucosal cells: Effect of smoking. Acta Med Int. 2014;1:22–7. [Google Scholar]
- 11.Seifi S, Feizi F, Mehdizadeh M, Khafri S, Ahmadi B. Evaluation of cytological alterations of oral mucosa in smokers and waterpipe users. Cell J. 2014;15:302–9. [PMC free article] [PubMed] [Google Scholar]
- 12.Bhisey RA. Chemistry and toxicology of smokeless tobacco. Indian J Cancer. 2012;49:364–72. doi: 10.4103/0019-509X.107735. [DOI] [PubMed] [Google Scholar]