

Abstract
Mycobacterium abscessus is a rapidly growing mycobacterium that has been affecting people undergoing invasive procedures, such as videosurgery and mesotherapy. This bacterium has global distribution, being found in numerous niches. The frequency of published reports of infection by rapidly growing mycobacteria associated with tattooing procedures has increased in recent years. However, in Brazil there were no case reports of M. abscessus after tattooing in the literature until now. In this paper, we describe the case of a patient with a nine-month history of lesion on a tattoo site. The diagnosis of infection with Mycobacterium abscessus was established by correlation between dermatological and histopathological aspects, culture and molecular biology techniques. The patient had significant improvement of symptoms with the use of clarithromycin monotherapy.
Keywords: Mycobacterium Infections, Nontuberculous; Nontuberculous Mycobacteria; Tattooing
INTRODUCTION
Mycobacterium abscessus is a rapidly-growing mycobacterium with global distribution, being found in numerous niches, including soil, water, dust and family and hospital settings.1
This mycobacterium was first described in 1953 by Moore and Frerichs. However, it was only in 1992, after its separation from the Mycobacterium chelonae group, that M. abscessus acquired the recognition that it is an important human pathogen responsible for a wide spectrum of soft tissue infections (after trauma or surgery), pulmonary infections and disseminated disease in immunocompromised patients.2,3
The incidence of infections by rapidly growing mycobacteria has increased in recent decades. This is partly attributed to the increased frequency of surgical procedures, immunosuppression in patients and the more efficient identification of the pathogen.4
In the literature, there are reports of infections by M. abscessus after mesotherapy, acupuncture, insulin injections in diabetic patients and other surgical procedures.1,5 We report an unusual case of primary skin inoculation by M. abscessus after tattooing.
CASE REPORT
A 42-year-old female patient, nurse, who lived in Manaus, Amazonas, had with a nine-month history of lesion on a tattoo site (lower third of the left leg), associated with mild itching and decreased tactile sensitivity. The tattooing had been done approximately two years earlier. Clinical examination evidenced a papule-nodular, floating injury, with an erythematous surface, little infiltrative capacity and imprecise limits on the tattoo site (Figure 1). There was no nerve enlargement and sensitivity tests performed on the injury site were unchanged. The patient denied comorbidities and had no systemic symptoms. She had already made use of topical treatments, but with no clinical improvement.
Figure 1.

Erythematous plaque little infiltrative capacity on the tattoo site
Histopathology showed a granulomatous inflammatory infiltrate composed of lymphocytes, histiocytes, epithelioid cells and giant Langerhans-type cells throughout the dermis and hypodermis (Figure 2). Special staining for AFB (acid fast bacilli alcohol) did not reveal bacilli.
Figure 2.
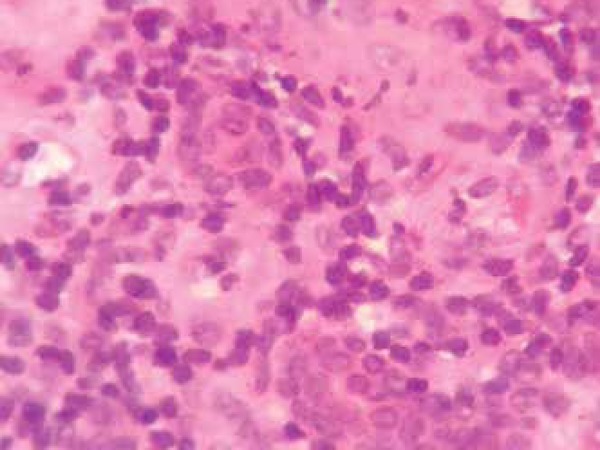
Inflammatory granulomatous process with presence of epithelioid cells and giant cells
A smear of the lesion was negative, but a culture in Loewenstein-Jensen medium showed isolation of fast-growing mycobacterium. M. abscessus was identified by PCR using hsp65 sequence.
The patient was treated with clarithromycin 500 mg twice daily. After five months of follow up, the patient showed clinical improvement, with reduction of the erythema and mild local atrophy.
DISCUSSION
Tattoos have become one of the most important aesthetic manifestations of our time. Complications occur in about 2% of cases and include infections (such as the report of the appearance of molluscum contagiosum on a tattoo seven months after the tattoo procedure), neoplasms and inflammatory dermatoses.6,7
The frequency of published reports of infection by rapidly growing mycobacteria associated with tattooing procedures has increased in recent years.3 This may be due to a more efficient identification of cases or may indicate an emerging problem caused by unsafe tattooing practices or by the increased popularity of tattoos.3 A search of the databases PubMed / Medline and Virtual Health Library (VHL) revealed that, in Brazil, there were no case reports of infection with M. abscessus after tattooing in the literature up to now.
There are reports of outbreaks involving contaminated devices such as needles and scalpels, after mesotherapy, multiple acupuncture treatments, and insulin injections in diabetic patients.1,6 There are only eight confirmed cases caused by M. abscessus after tattooing. The first case was reported in France in August 2010. A 51-year-old patient developed papular-pustules on a tattoo site 10 days after the tattoo procedure.2 In November of that year in Australia, M. abscessus was identified in papules on a tattoo site of a 25-year-old man 7-10 days after the procedure.8 In August 2012, the CDC (Centers for Disease Control and Prevention), in the United States, confirmed 3 cases of M. abscessus infection and in August 2013, in England, M. abscessus was identified in 3 of five cases caused by the rapidly growing mycobacteria.6 The probable responsible for the infections with fast-growing mycobacteria after tattooing could be contamination of ink or use of non-sterilized water for the dilution of ink or for washing equipments.3
The time elapsing between the tattooing and the appearance of skin manifestations varied between seven days and three months in the case reports. Patients also had variable clinical presentation, such as erythematous papules or pustules, nodules, ulcerated nodules, plaques lichenoid aspect.2 Symptoms include pain and itching.6 In the case presented here, a long time elapsed between the tattoo procedure and the onset of clinical manifestations, but this has also occurred in other reports of infections with M. abscessus.9 The link between the procedure and the injury was established by clinical history and by correlation between the clinical lesion, histopathological findings and the identification of M. abscessus, which was performed accurately, making any contaminant hypothesis untenable.
There is still no established treatment for skin infection with M. abscessus. Multiple treatment modalities are recommended, such as surgery, abscess drainage, removal of necrotic tissue and a long course of antibiotics. M. abscessus is generally susceptible to clarithromycin, amikacin, linezolid, tigecycline and haS variable susceptibility to cefoxitin and imipenem.5 In the 1990s, clarithromycin became the drug of choice for M. abscessus infections and it is indicated as monotherapy only in immunocompetent patients with localized lesion. Combination therapy (including parenteral drugs) is used in cases of disseminated infection, pulmonary infection or extensive skin disease.1,4 Recommendations regarding the duration of therapy are unclear, but, in some cases, treatment may be extended for more than six months. For localized disease, the recommendation is 4-6 months.1,6
The Brazilian National Health Surveillance Agency (ANVISA) has established technical standards for tattoo studios, including guidance on the appropriate physical structure, materials, devices and performance of procedures. However, there are no recommendations on the use of sterile water for washing the materials used or diluting the ink, as proposed by the CDC.10
To our knowledge, this is the first case report of isolation of M. abscessus from an injury on a tattoo site in Brazil. We emphasize the need to consider the possibility of clinical suspicion of infection with mycobacteria after tattooing and the need for public health measures to make this procedure safer.
Footnotes
Conflict of Interest: None.
Financial Support: None.
How to cite this article: Sousa PP, Cruz RCS, Schettini APM, Westphal DC. Mycobacterium abscessus skin infection after tattooing - case report. An Bras Dermatol. 2015;90(5):741-3.
Study conducted at the "Alfredo da Matta" Dermatology and Venereology Foundation(FUAM) – Manaus (AM), Brazil.
REFERENCES
- 1.Bates TR, Keenher T, O'Reilly LC, Heath CH, Flexman JP, Murray RJ. Extensive cutaneous Mycobacterium abscessus infection due to contaminated insulin delivery system. QJM. 2009;102:881–884. doi: 10.1093/qjmed/hcp129. [DOI] [PubMed] [Google Scholar]
- 2.Bechara C, Macheras E, Heym B, Pages A, Auffret N. Mycobacterium abscessus skin infection after tattooing: first case report and review of the literature. Dermatology. 2010;221:1–4. doi: 10.1159/000313974. [DOI] [PubMed] [Google Scholar]
- 3.Conaglen PD, Laurenson IF, Sergeant A, Thorn SN, Rayner A, Stevenson J. Systematic review of tattoo associated skin infection with rapidly growing mycobacteria and public health investigation of a cluster in Scotland, 2010. Euro Surveill. 2013;18:20553–20553. doi: 10.2807/1560-7917.es2013.18.32.20553. [DOI] [PubMed] [Google Scholar]
- 4.Nessar R, Cambau E, Reyrat JM, Murray A, Gicquel B. Mycobacterium abscessus: a new antibiotic nightmare. J Antimicrob Chemother. 2012;67:810–818. doi: 10.1093/jac/dkr578. [DOI] [PubMed] [Google Scholar]
- 5.Wongkitisophon P, Rattanakaemakorn P, Tanrattanakorn S, Vachiramon V. Cutaneous Mycobacterium abscessus infection associated with mesotherapy injection. Case Rep Dermatol. 2011;3:37–41. doi: 10.1159/000324766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Falsey RR, Kinzer MH, Hurst S, Kalus A, Pottinger PS, Duchin JS, et al. Cutaneous Inoculation of Nontuberculous Mycobacteria During Professional Tattooing: A Case Series and Epidemiologic Study. Clin Infect Dis. 2013;57:e143–e147. doi: 10.1093/cid/cit347. [DOI] [PubMed] [Google Scholar]
- 7.Molina L, Romiti R. Molluscum contagiosum on tattoo. An Bras Dermatol. 2011;86:352–354. doi: 10.1590/s0365-05962011000200022. [DOI] [PubMed] [Google Scholar]
- 8.Ricciardo B, Weedon D, Butler G. Mycobacterium abscessus infection complicating a professional tatoo. Australas J Dermatol. 2010;51:287–289. doi: 10.1111/j.1440-0960.2010.00659.x. [DOI] [PubMed] [Google Scholar]
- 9.Trupiano JK, Sebek BA, Goldfarb J, Levy LR, Hall GS, Procop GW. Mastitis Due to Mycobacterium abscessus after Body Piercing. Clin Infect Dis. 2001;33:131–134. doi: 10.1086/320885. [DOI] [PubMed] [Google Scholar]
- 10.Portal.anvisa.gov.br . Referência técnica para o funcionamento dos serviços de tatuagem e piercing, 2009. Dispõe sobre o funcionamento dos estabelecimentos que realizam procedimentos de pigmentação artificial permanente da pele e inserção de piercing. Brasília: Anvisa; 2009. [06 janeiro 2013]. Internet. Disponível em: http://portal.anvisa.gov.br/wps/wcm/connect/7259210047457ee38aacde3fbc4c6735/Tatuagem+e+Piercing.pdf?MOD=AJPERES. [Google Scholar]