

Abstract
Aims:
To suggest the best predictor/s for determining the mesio-distal widths (MDWs) of canines (C) and premolars (Ps), and propose regression equation/s for hitherto unreported population.
Methods:
Impressions of maxillary and mandibular arches were made for 201 children (100 boys and 101 girls; age range: 11–15 years) who met the inclusion criteria and poured with dental stone. The maximum MDWs of all the permanent teeth were measured using digital vernier caliper. Thirty-three possible combinations (patterns) of permanent maxillary and mandibular first molars, central and lateral incisors were framed and correlated with MDWs of C and Ps using Pearson correlation test.
Results:
There were significant correlations between the considered patterns and MDWs of C and Ps, with difference noted between girls (range of r: 0.34–0.66) and boys (range of r: 0.28–0.77). Simple linear and multiple regression equations for boys, girls, and combined sample were determined to predict MDW of C and Ps in both the arches.
Conclusions:
The accuracy of prediction improved considerably with the inclusion of as many teeth as possible in the regression equations. The newly proposed equations based on the erupted teeth may be considered clinically useful for space analysis in the considered population.
Keywords: Analysis, mixed dentition, regression
Introduction
Mixed dentition analysis (MDA) is imperative for diagnosis and timely intervention of arch length discrepancies.[1,2] It calculates the difference between the amount of dental arch space available and that required to accommodate tooth material in perfect alignment.[3,4] The available space in the arch can be equal to, greater or smaller than the un-erupted teeth dimensions, which becomes fundamental in determining the treatment plan, that might involve, serial extractions, tooth eruption guidance, space maintenance, space gain, or simple monitoring of the occlusion.[5] Thus, predicting the size of un-erupted teeth during the mixed dentition period is a critical factor in managing the developing occlusion of a growing child.
As an initial attempt to estimate mesio-distal widths (MDWs) of permanent canine (C) and premolars (Ps), tables are suggested based on the average dimensions of teeth.[6] However, these approximations are unreliable clinically due to great variability in tooth sizes among people. Hence, prediction methods based on the measurement of teeth on radiographs,[7] estimation based on the dimensions of primary and erupted permanent teeth using prediction tables[8] (that employ simple or multiple linear regression equations) and a combination of these approaches[9,10] are popular. Among these, radiographic methods are less commonly employed clinically due to the radiation exposures and image distortion problems. Therefore, nonradiographic methods such as Moyers’ (based on American white population),[3] Tanaka Johnston's (TJ) analysis[8] (based on Northwest European population), and Melgaco's prediction equations[11] (based on Brazilian population) are frequently practiced. Nevertheless, the major drawback of these methods is the question of reliability when applied to other populations for which they were derived.[5,12] Studies on various other populations proved that these methods either overestimate or underestimate the actual widths of permanent C and Ps.[5,12,13,14,15,16,17,18,19] Another question is the applicability of these equations that are based on pooled data (irrespective of gender) to both boys and girls.[5,20] To avoid these inconveniences, many authors proposed prediction tables and regression equations for their populations.[13,19,21] Studies pertaining to this topic on Indian population are also reported in the literature,[12,19,22,23,24,25,26] but, the population in south-east part of India is overlooked.
The existence of a significant linear association between the width of mandibular permanent incisors and un-erupted permanent C and Ps is reported; hence, suggested as the best predictor.[3,8] In the later studies, high values of correlation and determination coefficients are observed on adding the MDWs of the mandibular first permanent molars to the mandibular permanent incisors.[13,19] Also, different combinations of maxillary/mandibular first permanent molars with maxillary/mandibular permanent incisors were suggested for high prediction values to establish multiple regression equations.[11,13,15,19,20,21,27,28] However, a study, on a single sample population, to compare the capability of tooth/teeth combination to predict the MDWs of C and Ps, is not available in literature.
Evidence of dimensional change of teeth due to secular trends is also reported,[5] which projects the necessity to progressively modify MDA. Hence, the present study is an attempt to suggest the best predictor/s for determining the MDWs of C and Ps and propose new regression equation/s for boys and girls in hitherto unreported population.
Methods
The present study has been carried out in the Department of Pedodontics and Preventive Dentistry for a period of 6 months (from January 2014 to June 2014) after obtaining clearance from the Institutional Ethical Committee.
Sample
The children attending the department and school dental health programs were recruited; those who fulfilled below-mentioned inclusion criteria along with their assent and parental written informed consent to participate were included in the study.
Age range of 11–15 years (applying gender-stratified random sampling)
Belonging to the local area (south-east part of India) ancestry, at least from one previous generation
Presence of fully erupted permanent dentition (except third molars) with intact proximal surfaces, marginal ridges, incisal edges and contact points
Class I canine and molar relationship
Minimal wear.
Children with the following factors were excluded from the study:
Inter-proximal caries or restorations
Congenitally missing teeth or supernumerary teeth (abnormalities in number)
Abnormalities in shape, size, or structure
History of orthodontic treatment
Facial disharmony and/or congenital craniofacial anomalies
Transverse discrepancies such as cross bite
Apparent loss of tooth substance due to attrition, trauma, massive caries, or artificial crowns on teeth.
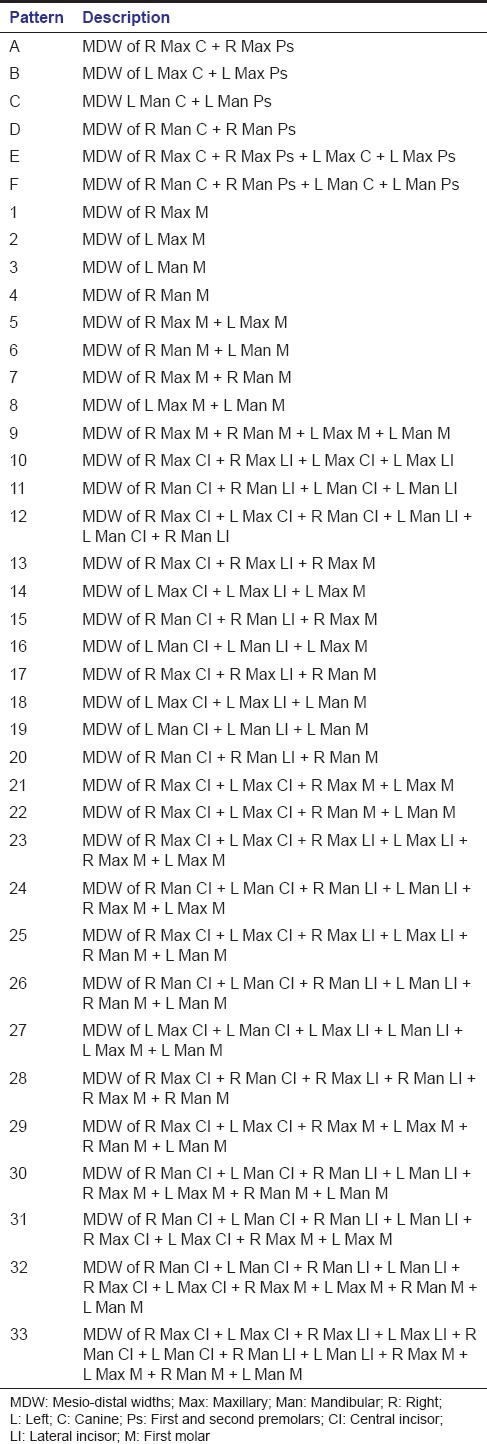
Various patterns of tooth/teeth combinations with permanent maxillary and mandibular first molars, central and lateral incisors were framed [Table 1]. Patterns A to F are based on different combinations of permanent C and Ps widths; patterns 1–9 on the maxillary and mandibular first molars, patterns 10–12 on central and lateral incisors, whereas 13–33 are based on the combinations of first molars, central and lateral incisors.
Table 1.
Description of patterns
Impressions of maxillary and mandibular arches were made with dentulous, perforated, impression trays (Zhermack® Spa, Italy) using irreversible hydrocolloid, tropicalgin (Chromic Alginate, Zhermack® Spa, Italy), mixed as per manufacturer's recommendations. The impressions were rinsed in running tap water, disinfected with 2% glutaraldehyde, poured with hard dental stone (Goldstone®, Asher Technologies, Kozhikode, Kerala, India) immediately to avoid any dimensional changes, and vibrated manually. The dental casts were neither soaped nor waxed; and each model pair was assigned an identification number to ensure examiner masking for gender.
The maximum MDWs of all the permanent teeth were measured using electronic digital vernier caliper (Aerospace 0–150 mm with a resolution of 0.01 mm, Bearing and Tools Centre, Ahmedabad, Gujarat, India) following the Moorrees and Reed's standard method.[29] This method measures the distance between anatomic contact points (from mesial to distal) at their greatest inter-proximal distance, with the help of sharp end calipers on the buccal or occlusal side. The tooth dimensions were recorded, transferred to the data sheets, tabulated, and analyzed.
The intra-examiner calibration procedure consisted of the primary investigator (KV) measuring 20 randomly selected model pairs twice, separated by 1-week. The inter-examiner calibration was done against a second examiner (RK) who also measured the 20 model pairs twice, separated by 1-week.
Sample size determination
Based on the lowest correlation value in the data obtained from the pilot study (sample of 21 model pairs), taking alpha error as 0.05, power of 95% and considering 10% for errors, a total sample size of 189 was determined.
Statistical analysis
Statistical analysis was carried out using the SPSS statistical package (SPSS Statistics for Windows, Version 17.0. Chicago: SPSS Inc) with the level of significance set at 0.05. The mean, standard deviation and range of tooth dimensions for boys, girls, and combined sample were tabulated, and the normality of the data was tested using Shapiro–Wilk test. As the data were found to be normally distributed, the difference between the dimensions of boys and girls was analyzed using unpaired t-test. The correlation between the considered patterns and the MDWs of C and Ps was done, using Pearson correlation test. Linear regression was used to derive equations for the prediction of the sum of the widths of C and Ps for both maxilla and mandible. The best combinations of independent variables were determined, and multiple linear regression equations derived. The predicted (both from simple and multiple regression equations) and actual values were analyzed for difference using paired t- test.
Results
The intra-examiner and inter-examiner reliability calculated, using Cohen's Kappa, from twenty randomly selected model pairs and were found to be 0.98 and 0.95, respectively, showing consistency of the tooth measurements.
A total of 432 children were screened, of which 201 (100 boys and 101 girls) met the inclusion criteria. The mean and standard deviation of the MDW of individual teeth in boys, girls and combined sample are represented in Table 2; boys showing significantly larger teeth than girls in both the arches.
Table 2.
Mesio-distal widths of permanent teeth in boys, girls, and combined sample
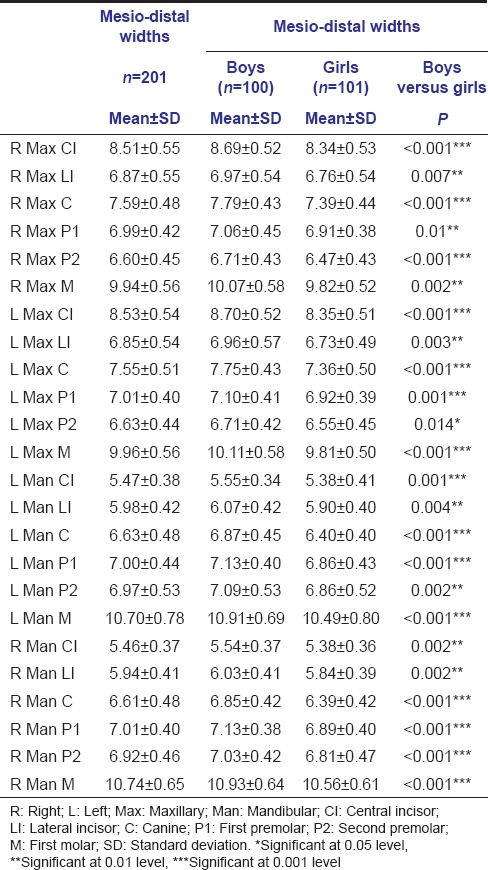
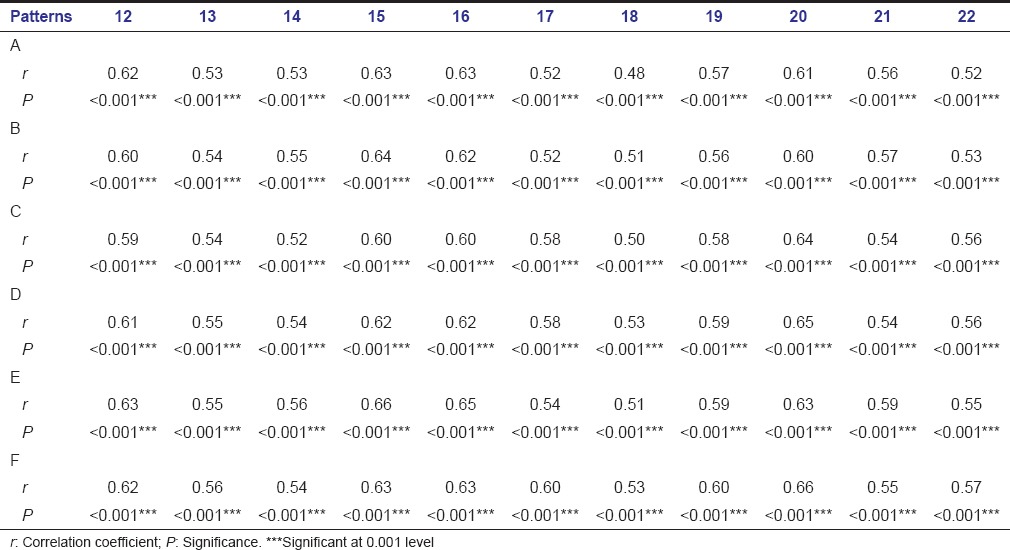
Table 3a–c shows the correlation between the considered patterns and MDWs of C and Ps in the combined sample. The lowest correlation coefficients observed were with pattern 3 (r = 0.38–0.48) and highest coefficients with the pattern 28 (r = 0.66–0.74). However, all the patterns were correlating significantly with MDW of C and Ps. Table 4a–c shows the correlation between the considered patterns and MDWs of C and Ps in boys, whereas Table 5a–c shows for girls. There are significant correlations in both boys and girls, though the correlation coefficients were less in girls, compared to boys.
Table 3a.
Correlation of framed patterns in combined sample (boys and girls)
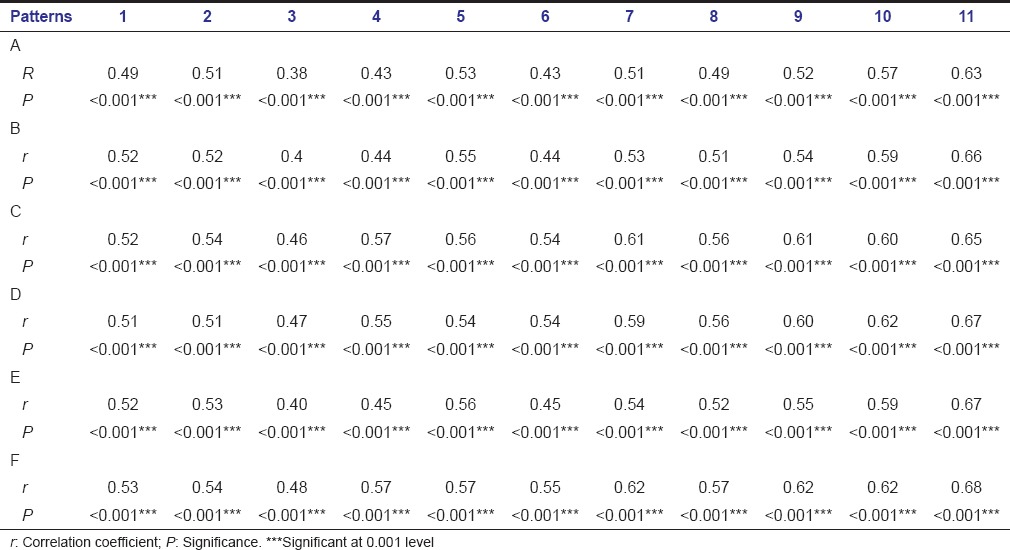
Table 3c.
Correlation of framed patterns in combined sample (boys and girls)
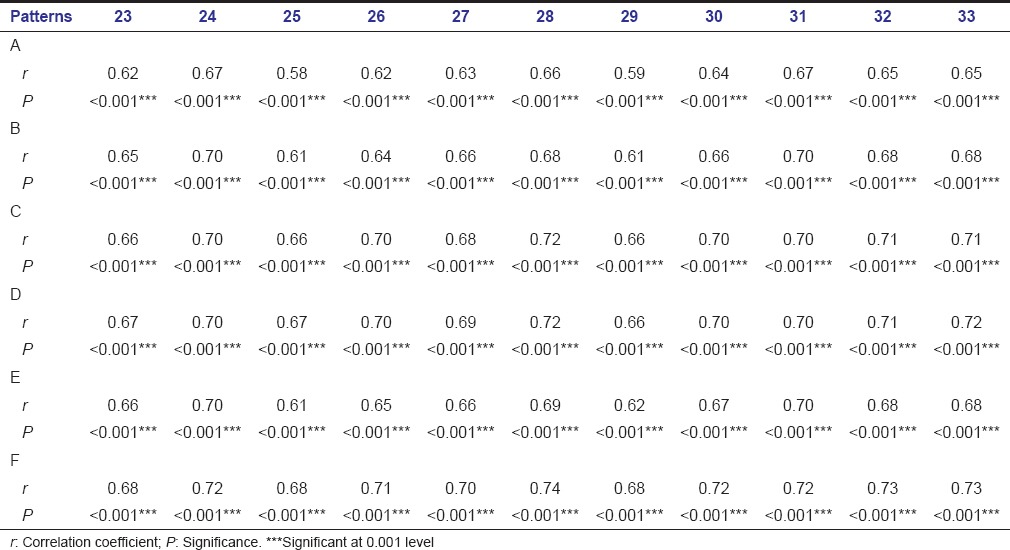
Table 4a.
Correlation of framed patterns in boys
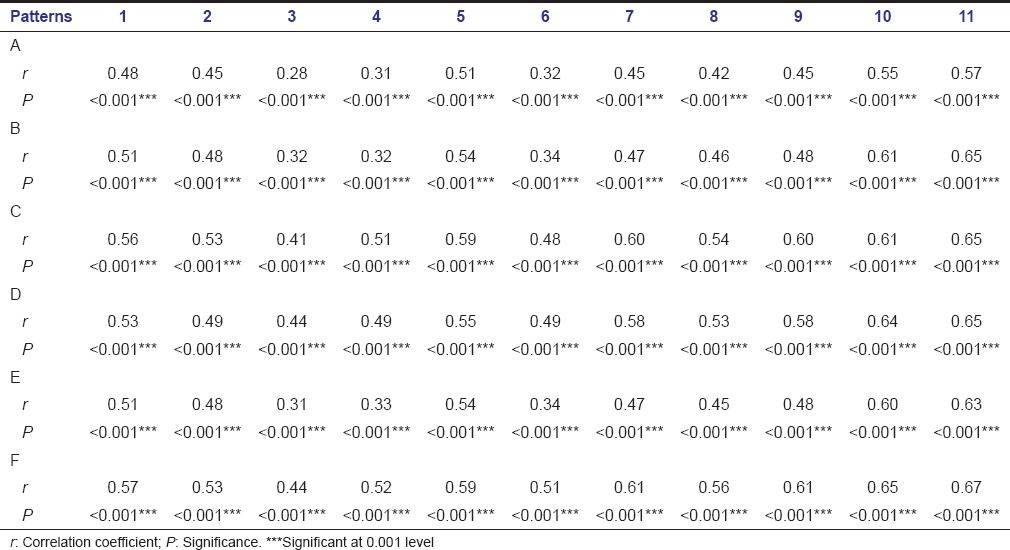
Table 4c.
Correlation of framed patterns in boys
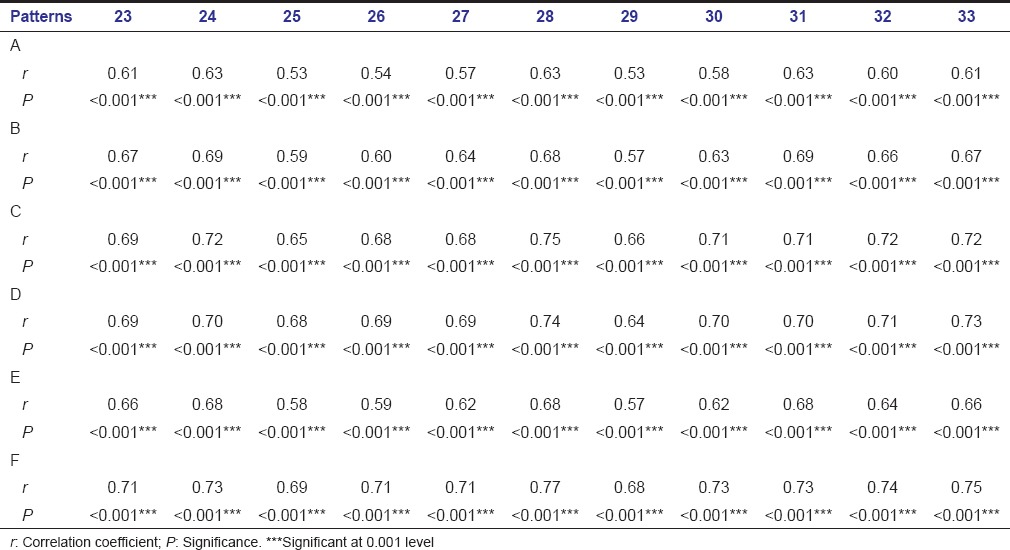
Table 5a.
Correlation of framed patterns in girls
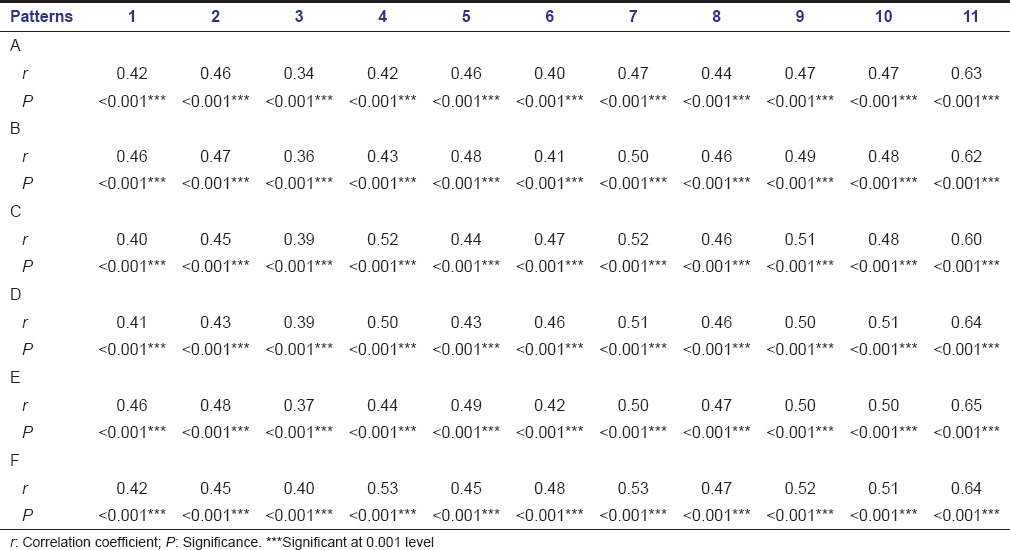
Table 5c.
Correlation of framed patterns in girls
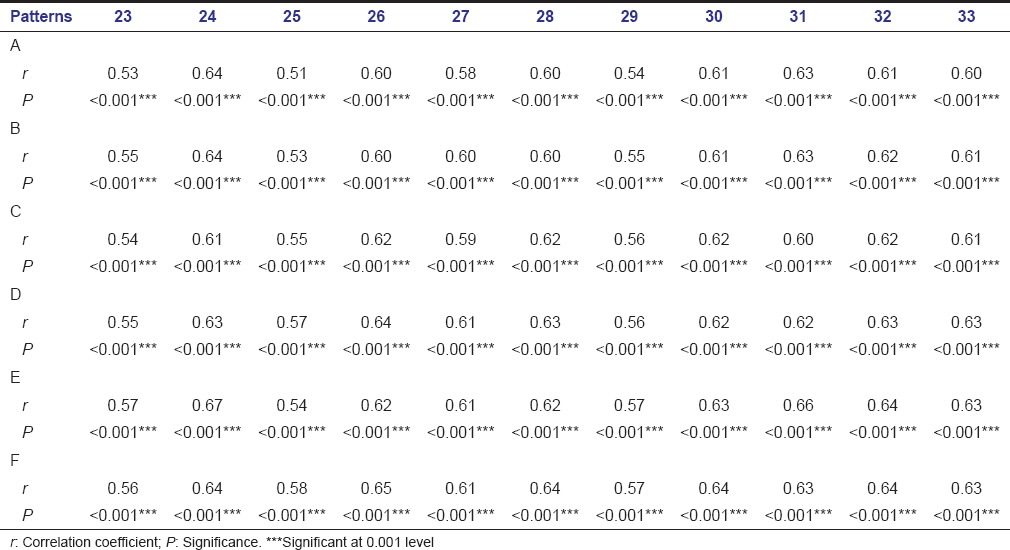
Table 3b.
Correlation of framed patterns in combined sample (boys and girls)
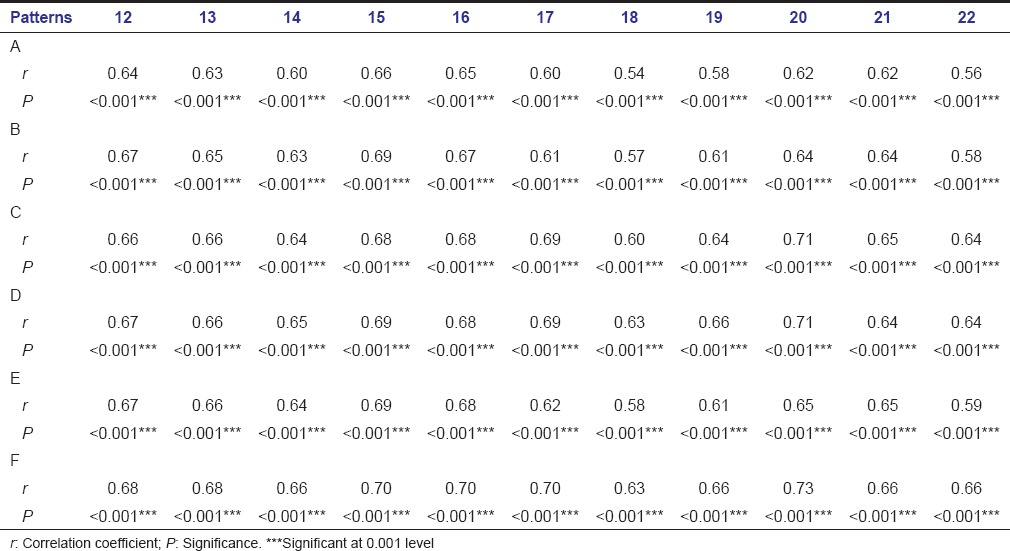
Table 4b.
Correlation of framed patterns in boys
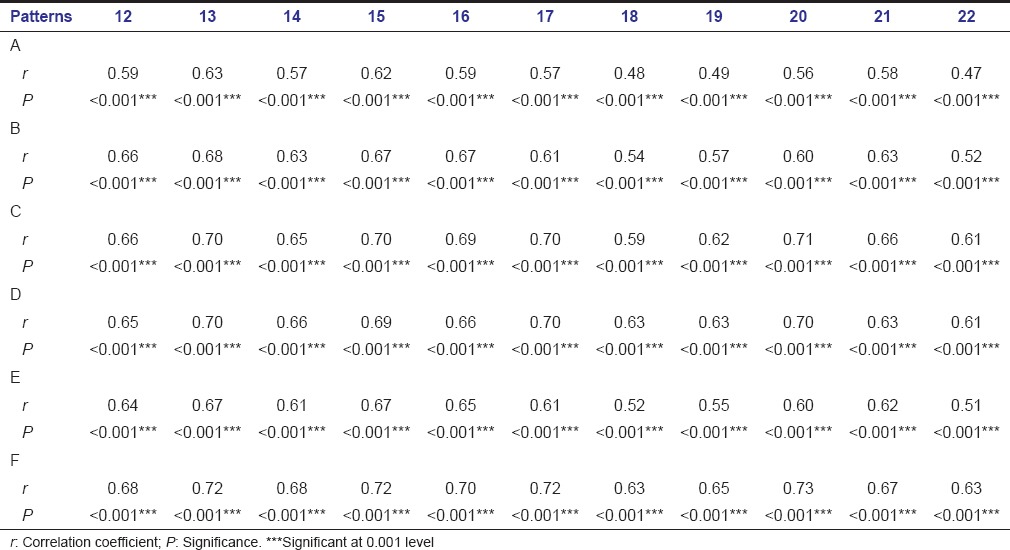
Table 5b.
Correlation of framed patterns in girls
Comparison of the tooth dimensions on the right and left sides did not show significant difference between any two contralateral teeth in maxilla, whereas significant differences were observed in the dimensions of right and left lateral incisors and second premolars in mandible. Comparison of the differences in the contralateral teeth between boys and girls did not show significant differences in boys, whereas significant differences in dimensions of right and left mandibular lateral incisors and maxillary second premolars were found in girls.
For regressions, the average values of right and left contralateral teeth, in both maxilla and mandible were considered. As all the framed patterns were correlating significantly; only simple patterns were considered, following the sequence of eruption. Simple linear regression equations for boys, girls, and combined sample were determined to predict MDW of C and Ps in both the arches, which are represented in Table 6. All the equations were calculated as y = a + bx, where y is the dependent variable (sum of the mandibular/maxillary C and Ps); x is the independent variable (the considered pattern). Multiple linear equations were calculated as y = ax1 + bx2+…; and the determined equations for boys, girls and combined sample are represented in Table 7.
Table 6.
Simple linear regression equations for prediction of widths of canines and premolars
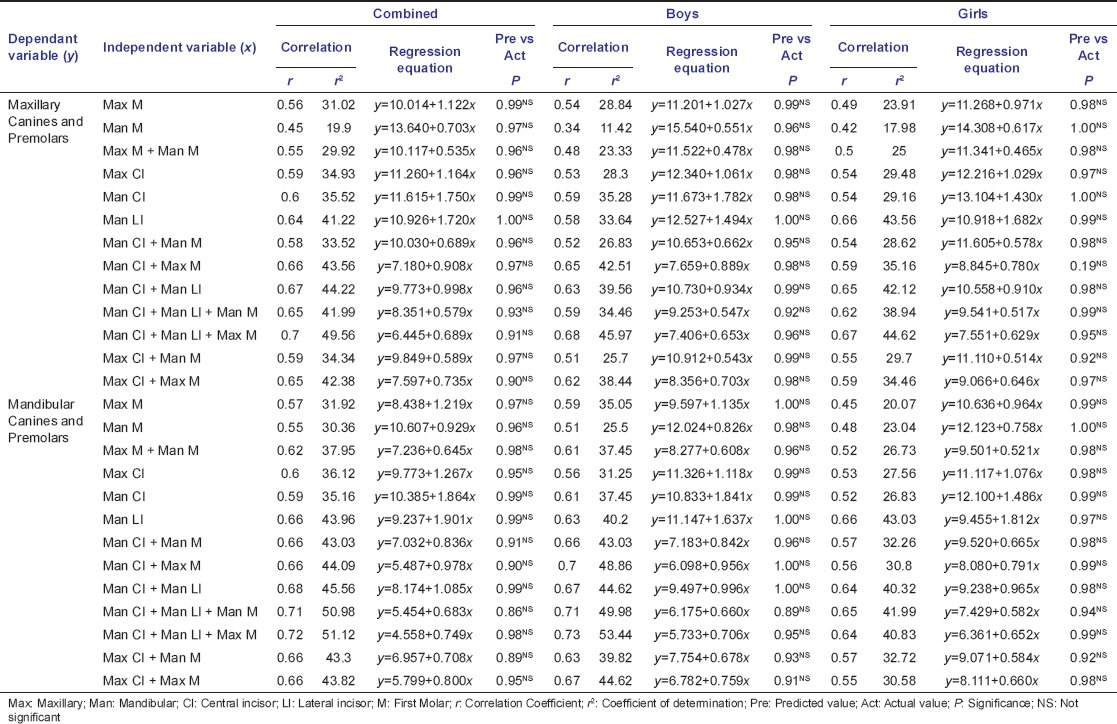
Table 7.
Multiple linear regression equations for prediction of widths of canines and premolars
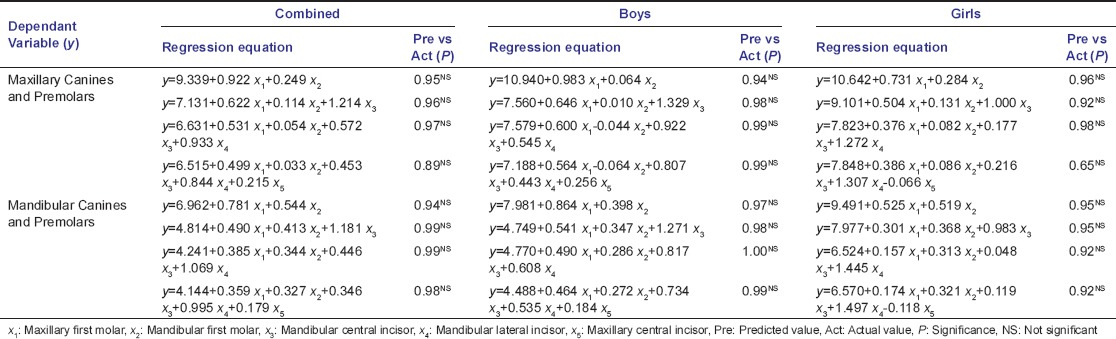
On comparing the actual values and predicted values from simple and multiple regression equations [Tables 6 and 7], no significant differences were observed.
Discussion
On reviewing the existing literature on MDA, Moyers’ and TJ analyses are observed to be popular, widely employed, and proven to be clinically valid.[3,8,17,30] They are based on the predictive capability of permanent mandibular central and lateral incisors; the reported reasons for selecting these teeth being, first in the sequence of eruption, less variability in shape and size, can be easily and accurately measured and high correlation of these teeth with others.[29] Thus, the major proposed advantage of these nonradiographic methods is the ease and speed of use by direct measurement of teeth in the oral cavity with minimum errors.[5,15] In due course, Melgaco analysis, proved to be a good predictor in Brazilian population, came into practice, which employs a combination of mandibular first molar and incisor teeth.[11] However, due to the thrust for a better predictive capability, various studies have projected other teeth like maxillary/mandibular first molars, maxillary central and lateral incisors and different combinations of all the above-mentioned teeth as means to determine the MDW of C and Ps.[11,13,15,19,20,21,27,28]
Another major drawback of the Moyers’ and TJ analyses is the development of these methods based on the data derived from population of North European descent.[1,2,7] Studies comparing these methods with their respective populations have observed either overestimation/underestimation.[3,8,11,16,17,18,30] Thus, regression equations for their populations were suggested by studies conducted on black Americans,[31] black Africans,[30] Asian-Americans,[32] Egyptians,[33] Mexicans,[33] Americans,[33] Peruvians,[34] Saudi Arabians,[35] Syrians,[15] Hong Kong Chinese,[36] Croatians,[27] Nigerians,[37] Thai,[20] and Senegalese[38] populations. Accordingly, several linear regression equations have been proposed for populations of different ethnic origins, assuming that the most accurate equation for prediction of tooth size should be based on measurements obtained from the population in question. Studies on Indian population are also reported with sample derived from western Uttar Pradesh,[12] Gujarat,[19] Haryana,[22] Central India,[24] Karnataka,[23] West Bengal,[25] and Himachal[26] population. Hence, the present study has been performed with the aim of developing population-specific regression equations that can be consistently applied to the population of south coastal Andhra Pradesh (part of southeast India).
Another important aspect that should not be neglected in this field is the consideration of gender differences in the tooth dimensions. Studies conducted to determine the sexual dimorphism in populations of different ethnic origin considered so far, have revealed that the tooth dimensions were significantly high in boys, compared to girls,[5,7,8,10,11,16,17,27,28,30,35] which is supported by the findings of the present study. Hence, equations for both the genders separately were formulated in the present study.
Differences between contralateral teeth have been considered in many previous studies, with no significant difference noted.[11,14,16] However, in the present study, significant differences were noticed in mandibular lateral incisors and second premolars; only among the girls, with the left side showing larger dimensions than the right.
All the patterns formulated in the present study, using various tooth/teeth combinations, correlated significantly with the C and Ps MDW in both boys and girls. However, irrespective of the gender, the correlation coefficient values were high, as the number of teeth increased. This entails the significance of including as many teeth as possible for predicting MDW of C and Ps, rather than considering particular tooth/teeth. Thus, we can employ either simple/multiple regression equations depending on the status of dentition, as proposed in the present study. On comparing the actual and predicted values, no significant differences were noted for both simple and multiple linear regression equations, which highlight good applicability of all these equations to this specific population. The findings of the present study can be generalized for south eastern Indian population, derived from the same ethnic background.
Based on the following conclusions, this study thus focuses on the importance of framing particular equations for specific ethnic/racial population groups so that individualized treatment planning can be performed:
There was a gender discrepancy noticed in the present study, hence, gender separated, population specific new regression equations are proposed as good prediction methods to determine the MDW of C and Ps
The accuracy of prediction improved considerably by inclusion of as many teeth as possible in the regression equations
The newly proposed equations may be considered clinically useful for MDA in the contemporary population depending on the erupted teeth
This paper also demonstrates the necessity of determining distinctive regression equations for various populations.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Bolton WA. Disharmony in tooth size and its relation to the analysis in treatment of malocclusion. Angle Orthod. 1958;28:113–30. [Google Scholar]
- 2.Bolton WA. The clinical application of a tooth Size analysis. Am J Orthod. 1962;48:504–29. [Google Scholar]
- 3.Moyers RE. Handbook of Orthodontics for the Student and General Practitioner. 3rd ed. Chicago: Yearbook Medical Publisher Inc; 1973. pp. 369–79. [Google Scholar]
- 4.Kirschen RH, O’higgins EA, Lee RT. The Royal London Space Planning: An integration of space analysis and treatment planning: Part I: Assessing the space required to meet treatment objectives. Am J Orthod Dentofacial Orthop. 2000;118:448–55. doi: 10.1067/mod.2000.109031. [DOI] [PubMed] [Google Scholar]
- 5.Al-Bitar ZB, Al-Omari IK, Sonbol HN, Al-Ahmad HT, Hamdan AM. Mixed dentition analysis in a Jordanian population. Angle Orthod. 2008;78:670–5. doi: 10.2319/0003-3219(2008)078[0670:MDAIAJ]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 6.Memon S, Fida M. Development of a prediction equation for the estimation of mandibular canine and premolar widths from mandibular first permanent molar and incisor widths. Eur J Orthod. 2012;34:340–4. doi: 10.1093/ejo/cjr015. [DOI] [PubMed] [Google Scholar]
- 7.de Paula S, Almeida MA, Lee PC. Prediction of mesiodistal diameter of unerupted lower canines and premolars using 45º cephalometric radiography. Am J Orthod Dentofacial Orthop. 1995;107:309–14. doi: 10.1016/s0889-5406(95)70147-8. [DOI] [PubMed] [Google Scholar]
- 8.Tanaka MM, Johnston LE. The prediction of the size of unerupted canines and premolars in a contemporary orthodontic population. J Am Dent Assoc. 1974;88:798–801. [PubMed] [Google Scholar]
- 9.Hixon EH, Oldfather RE. Estimation of the sizes of unerupted cuspid and bicuspid teeth. Angle Orthod. 1958;28:236–40. [Google Scholar]
- 10.Staley RN, Kerber PE. A revision of the hixon and old father mixed-dentition prediction method. Am J Orthod. 1980;78:296–302. doi: 10.1016/0002-9416(80)90274-2. [DOI] [PubMed] [Google Scholar]
- 11.Melgaço CA, de Sousa Araújo MT, de Oliveira Ruellas AC. Mandibular permanent first molar and incisor width as predictor of mandibular canine and premolar width. Am J Orthod Dentofacial Orthop. 2007;132:340–5. doi: 10.1016/j.ajodo.2005.07.033. [DOI] [PubMed] [Google Scholar]
- 12.Srivastava B, Bhatia HP, Singh R, Singh AK, Aggarwal A, Gupta N. Validation of Tanaka and Johnston's analysis in western UP Indian population. J Indian Soc Pedod Prev Dent. 2013;31:36–42. doi: 10.4103/0970-4388.112405. [DOI] [PubMed] [Google Scholar]
- 13.Brito FC, Nacif VC, Melgaço CA. Mandibular permanent first molars and incisors as predictors of mandibular permanent canine and premolar widths: Applicability and consistency of the method. Am J Orthod Dentofacial Orthop. 2014;145:393–8. doi: 10.1016/j.ajodo.2013.01.024. [DOI] [PubMed] [Google Scholar]
- 14.Bherwani AK, Fida M. Development of a prediction equation for the mixed dentition in a Pakistani sample. Am J Orthod Dentofacial Orthop. 2011;140:626–32. doi: 10.1016/j.ajodo.2011.02.024. [DOI] [PubMed] [Google Scholar]
- 15.Nourallah AW, Gesch D, Khordaji MN, Splieth C. New regression equations for predicting the size of unerupted canines and premolars in a contemporary population. Angle Orthod. 2002;72:216–21. doi: 10.1043/0003-3219(2002)072<0216:NREFPT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 16.Arslan SG, Dildes N, Kama JD, Genç C. Mixed-dentition analysis in a Turkish population. World J Orthod. 2009;10:135–40. [PubMed] [Google Scholar]
- 17.nik Tahere H, Majid S, Fateme M, Kharazi fard, Javad M. Predicting the size of unerupted canines and premolars of the maxillary and mandibular quadrants in an Iranian population. J Clin Pediatr Dent. 2007;32:43–7. doi: 10.17796/jcpd.32.1.r066201525862144. [DOI] [PubMed] [Google Scholar]
- 18.Altherr ER, Koroluk LD, Phillips C. Influence of sex and ethnic tooth-size differences on mixed-dentition space analysis. Am J Orthod Dentofacial Orthop. 2007;132:332–9. doi: 10.1016/j.ajodo.2005.08.043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Shah S, Bhaskar V, Venkataraghvan K, Choudhary P, Mahadevan G, Trivedi K. Applicability of regression equation using widths of mandibular permanent first molars and incisors as a predictor of widths of mandibular canines and premolars in contemporary Indian population. J Indian Soc Pedod Prev Dent. 2013;31:135–40. doi: 10.4103/0970-4388.117962. [DOI] [PubMed] [Google Scholar]
- 20.Jaroontham J, Godfrey K. Mixed dentition space analysis in a Thai population. Eur J Orthod. 2000;22:127–34. doi: 10.1093/ejo/22.2.127. [DOI] [PubMed] [Google Scholar]
- 21.Boboc A, Dibbets J. Prediction of the mesiodistal width of unerupted permanent canines and premolars: A statistical approach. Am J Orthod Dentofacial Orthop. 2010;137:503–7. doi: 10.1016/j.ajodo.2008.04.031. [DOI] [PubMed] [Google Scholar]
- 22.Mittar M, Dua VS, Wilson S. Reliability of permanent mandibular first molars and incisors widths as predictor for the width of permanent mandibular and maxillary canines and premolars. Contemp Clin Dent. 2012;3:S8–12. doi: 10.4103/0976-237X.95094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Sholapurmath SM, Benni DB, Mandroli P. Applicability of two mixed dentition analyses in children of Jangam community of Belgaum city. World J Dent. 2012;3:324–9. [Google Scholar]
- 24.Nayak A, Hazarey PV. Evaluation of applicability of Moyer's mixed dentition analysis for central India population. J Indian Orthod Soc. 2004;37:154–9. [Google Scholar]
- 25.Dasgupta B, Zahir S. Comparison of two non-radiographic techniques of mixed dentition space analysis and evaluation of their reliability for Bengali population. Contemp Clin Dent. 2012;3:S146–50. doi: 10.4103/0976-237X.101069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kaur A, Singh R, Mittal S, Sharma S, Bector A, Awasthi S. Evaluation and applicability of Moyers mixed dentition arch analysis in Himachal population. Dent J Adv Stud. 2014;2:96–104. [Google Scholar]
- 27.Legovic M, Novosel A, Legovic A. Regression equations for determining mesiodistal crown diameters of canines and premolars. Angle Orthod. 2003;73:314–8. doi: 10.1043/0003-3219(2003)073<0314:REFDMC>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 28.Bernabé E, Flores-Mir C. Are the lower incisors the best predictors for the unerupted canine and premolars sums? An analysis of a Peruvian sample. Angle Orthod. 2005;75:202–7. doi: 10.1043/0003-3219(2005)075<0198:ATLITB>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 29.Moorrees CF, Reed RB. Correlations among crown diameters of human teeth. Arch Oral Biol. 1964;9:685–97. doi: 10.1016/0003-9969(64)90080-9. [DOI] [PubMed] [Google Scholar]
- 30.Schirmer UR, Wiltshire WA. Orthodontic probability tables for black patients of African descent: Mixed dentition analysis. Am J Orthod Dentofacial Orthop. 1997;112:545–51. doi: 10.1016/s0889-5406(97)70082-9. [DOI] [PubMed] [Google Scholar]
- 31.Ferguson FS, Macko DJ, Sonnenberg EM, Shakun ML. The use of regression constants in estimating tooth size in a Negro population. Am J Orthod. 1978;73:68–72. doi: 10.1016/0002-9416(78)90103-3. [DOI] [PubMed] [Google Scholar]
- 32.Lee-Chan S, Jacobson BN, Chwa KH, Jacobson RS. Mixed dentition analysis for Asian-Americans. Am J Orthod Dentofacial Orthop. 1998;113:293–9. doi: 10.1016/s0889-5406(98)70300-2. [DOI] [PubMed] [Google Scholar]
- 33.Bishara SE, Jakobsen JR, Abdallah EM, Fernandez Garcia A. Comparisons of mesiodistal and buccolingual crown dimensions of the permanent teeth in three populations from Egypt, Mexico, and the United States. Am J Orthod Dentofacial Orthop. 1989;96:416–22. doi: 10.1016/0889-5406(89)90326-0. [DOI] [PubMed] [Google Scholar]
- 34.Flores-Mir C, Bernabé E, Camus C, Carhuayo MA, Major PW. Prediction of mesiodistal canine and premolar tooth width in a sample of Peruvian adolescents. Orthod Craniofac Res. 2003;6:173–6. doi: 10.1034/j.1600-0544.2003.03251.x. [DOI] [PubMed] [Google Scholar]
- 35.al-Khadra BH. Prediction of the size of unerupted canines and premolars in a Saudi Arab population. Am J Orthod Dentofacial Orthop. 1993;104:369–72. doi: 10.1016/S0889-5406(05)81335-6. [DOI] [PubMed] [Google Scholar]
- 36.Yuen KK, Tang EL, So LL. Mixed dentition analysis for Hong Kong Chinese. Angle Orthod. 1998;68:21–8. doi: 10.1043/0003-3219(1998)068<0021:MDAFHK>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 37.Otuyemi OD, Noar JH. A comparison of crown size dimensions of the permanent teeth in a Nigerian and a British population. Eur J Orthod. 1996;18:623–8. doi: 10.1093/ejo/18.6.623. [DOI] [PubMed] [Google Scholar]
- 38.Diagne F, Diop-Ba K, Ngom PI, Mbow K. Mixed dentition analysis in a Senegalese population: Elaboration of prediction tables. Am J Orthod Dentofacial Orthop. 2003;124:178–83. doi: 10.1016/s0889-5406(03)00390-1. [DOI] [PubMed] [Google Scholar]