

Abstract
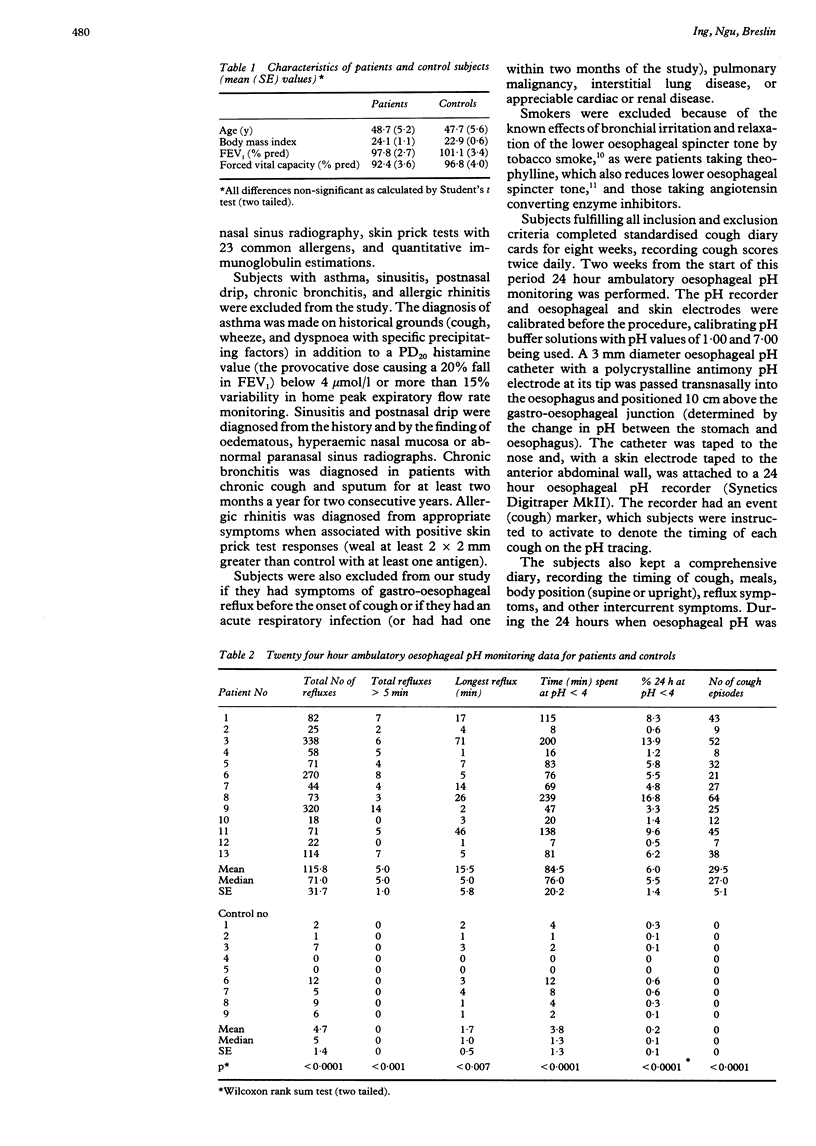
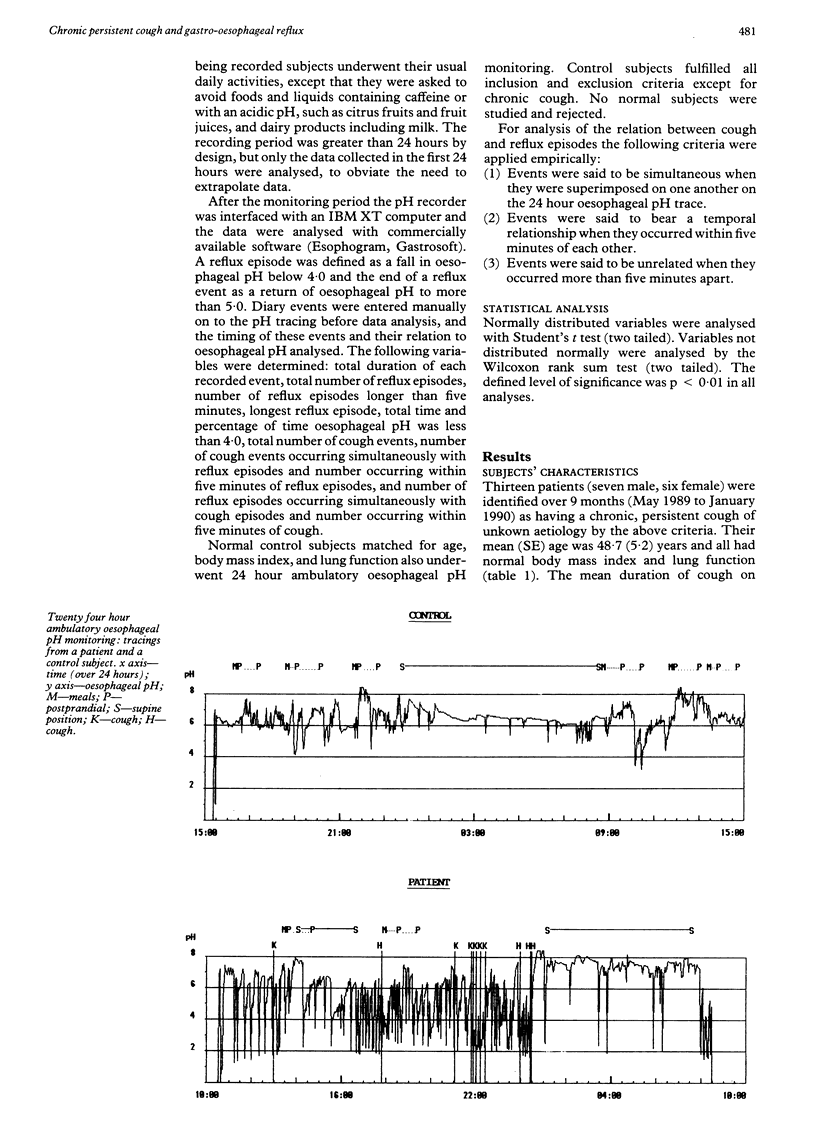
Chronic cough persisting for two months or more that remains unexplained after extensive investigations is a common clinical problem. The purpose of this study was to determine whether such cough is associated with otherwise asymptomatic gastro-oesophageal reflux. Thirteen patients with chronic persistent cough that was unexplained after a standard diagnostic assessment were identified. All were non-smokers. The mean (SE) duration of cough was 17.8 (8.0) months. Ten had never had reflux symptoms and three had had mild symptoms only after the onset of the cough. All the patients completed standardised cough diary cards for eight weeks and underwent 24 hour ambulatory oesophageal pH monitoring. A reflux episode was defined as a fall in oesophageal pH to below 4.0. Nine control subjects were matched for age, lung function, and body mass index. The patients experienced significantly more episodes of reflux per 24 hours than the controls (115.8 (SE 31.7) versus 4.7 (1.4) and longer reflux episodes (15.5 (5.8) versus 1.7 (0.5) minutes), and the oesophageal pH was below 4.0 considerably longer (84.5 (20.2) versus 3.8 (1.3) minutes). Cough occurred simultaneously with 13% (2.2%) of reflux episodes and within five minutes in another 35% (5.8%) of episodes, whereas gastro-oesophageal reflux occurred simultaneously with 78% (5.5%) of cough episodes and within five minutes in another 12% (2.3%) of episodes. It is concluded that chronic persistent cough that remains unexplained after a standard diagnostic assessment is associated with otherwise asymptomatic gastro-oesophageal reflux. It is suggested that a self perpetuating mechanism may exist whereby acid reflux causes cough via a local neuronal oesophageal-tracheo-bronchial reflex, and the cough in turn amplifies reflux via increased transdiaphragmatic pressure or by inducing transient lower oesophageal sphincter relaxation. Further study of this mechanism and the role of specific antireflux treatment in chronic persistent cough is warranted.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Boyle J. T., Tuchman D. N., Altschuler S. M., Nixon T. E., Pack A. I., Cohen S. Mechanisms for the association of gastroesophageal reflux and bronchospasm. Am Rev Respir Dis. 1985 May;131(5):S16–S20. doi: 10.1164/arrd.1985.131.S5.S16. [DOI] [PubMed] [Google Scholar]
- Castell D. O. Asthma and gastroesophageal reflux. Chest. 1989 Jul;96(1):2–3. doi: 10.1378/chest.96.1.2. [DOI] [PubMed] [Google Scholar]
- Dennish G. W., Castell D. O. Inhibitory effect of smoking on the lower esophageal sphincter. N Engl J Med. 1971 May 20;284(20):1136–1137. doi: 10.1056/NEJM197105202842007. [DOI] [PubMed] [Google Scholar]
- Dent J. Recent views on the pathogenesis of gastro-oesophageal reflux disease. Baillieres Clin Gastroenterol. 1987 Oct;1(4):727–745. doi: 10.1016/0950-3528(87)90016-9. [DOI] [PubMed] [Google Scholar]
- Holinger L. D. Chronic cough in infants and children. Laryngoscope. 1986 Mar;96(3):316–322. doi: 10.1288/00005537-198603000-00015. [DOI] [PubMed] [Google Scholar]
- Irwin R. S., Corrao W. M., Pratter M. R. Chronic persistent cough in the adult: the spectrum and frequency of causes and successful outcome of specific therapy. Am Rev Respir Dis. 1981 Apr;123(4 Pt 1):413–417. doi: 10.1164/arrd.1981.123.4.413. [DOI] [PubMed] [Google Scholar]
- Irwin R. S., Curley F. J., French C. L. Chronic cough. The spectrum and frequency of causes, key components of the diagnostic evaluation, and outcome of specific therapy. Am Rev Respir Dis. 1990 Mar;141(3):640–647. doi: 10.1164/ajrccm/141.3.640. [DOI] [PubMed] [Google Scholar]
- Irwin R. S., Zawacki J. K., Curley F. J., French C. L., Hoffman P. J. Chronic cough as the sole presenting manifestation of gastroesophageal reflux. Am Rev Respir Dis. 1989 Nov;140(5):1294–1300. doi: 10.1164/ajrccm/140.5.1294. [DOI] [PubMed] [Google Scholar]
- Mansfield L. E., Hameister H. H., Spaulding H. S., Smith N. J., Glab N. The role of the vague nerve in airway narrowing caused by intraesophageal hydrochloric acid provocation and esophageal distention. Ann Allergy. 1981 Dec;47(6):431–434. [PubMed] [Google Scholar]
- Mansfield L. E., Stein M. R. Gastroesophageal reflux and asthma: a possible reflex mechanism. Ann Allergy. 1978 Oct;41(4):224–226. [PubMed] [Google Scholar]
- Poe R. H., Harder R. V., Israel R. H., Kallay M. C. Chronic persistent cough. Experience in diagnosis and outcome using an anatomic diagnostic protocol. Chest. 1989 Apr;95(4):723–728. doi: 10.1378/chest.95.4.723. [DOI] [PubMed] [Google Scholar]
- Poe R. H., Israel R. H., Utell M. J., Hall W. J. Chronic cough: bronchoscopy or pulmonary function testing? Am Rev Respir Dis. 1982 Jul;126(1):160–162. doi: 10.1164/arrd.1982.126.1.160. [DOI] [PubMed] [Google Scholar]
- Stein M. R., Towner T. G., Weber R. W., Mansfield L. E., Jacobson K. W., McDonnell J. T., Nelson H. S. The effect of theophylline on the lower esophageal sphincter pressure. Ann Allergy. 1980 Oct;45(4):238–241. [PubMed] [Google Scholar]
- Ward B. W., Wu W. C., Richter J. E., Lui K. W., Castell D. O. Ambulatory 24-hour esophageal pH monitoring. Technology searching for a clinical application. J Clin Gastroenterol. 1986;8 (Suppl 1):59–67. doi: 10.1097/00004836-198606001-00009. [DOI] [PubMed] [Google Scholar]
- Yan K., Salome C., Woolcock A. J. Rapid method for measurement of bronchial responsiveness. Thorax. 1983 Oct;38(10):760–765. doi: 10.1136/thx.38.10.760. [DOI] [PMC free article] [PubMed] [Google Scholar]