

Abstract
Please cite this paper as: Basurto‐Dávila et al. (2012) Household economic impact and attitudes toward school closures in two cities in Argentina during the 2009 influenza A (H1N1) pandemic. Influenza and Other Respiratory Viruses. DOI: 10.1111/irv.12054.
Background School closures were widely implemented in Argentina during the 2009 H1N1 influenza virus pandemic.
Objectives To assess the economic impact of school closures on households, their effectiveness in preventing children from engaging in social group activities, and parental attitudes toward them.
Methods Three schools that closed for 2 weeks in response to the pandemic were identified in two socioeconomically distinct cities in Argentina. All households with children enrolled in these schools were surveyed. Direct and indirect costs attributable to closures were estimated from the household perspective. Other information collected included children activities during the closures and parental attitudes toward the intervention.
Results Completed questionnaires were returned by 45% of surveyed households. Direct and indirect costs due to closures represented 11% of imputed monthly household income in the city with lower socioeconomic status, and 3% in the other city (P = 0·01). Non‐childcare expenses and loss of workdays were more common in the city with lower socioeconomic status. Childcare expenses were less common and were experienced by a similar percentage of households in both cities. About three‐quarters of respondents in both cities agreed with the closures. The main concern among those who disagreed with closures was their negative impact on education. Children in more than two‐thirds of affected households left their home at least once during the closures to spend time in public places.
Conclusion School closures may more significantly impact low‐income households. Authorities should consider the range of economic impacts of school closures among families when planning their implementation.
Keywords: Costs and cost analysis, healthcare economics, human, influenza, pandemics, prevention and control
Introduction
Influenza transmission rates are high in schools and school‐aged children contribute to the spread of disease in the wider community. 1 , 2 , 3 In Argentina, as in much of the world, 2009 pandemic influenza A (H1N1) virus (pH1N1) outbreaks occurred among the school‐aged population. 4 , 5 , 6 As part of their pandemic response, the Argentinean Ministry of Health (MOH) recommended several measures to reduce disease transmission, including antiviral treatment for confirmed cases and their contacts, quarantine of symptomatic cases, and 2‐week closures of schools with a laboratory‐confirmed pH1N1 case, in addition to a general recommendation to keep children from closed schools at home and avoid outside personal contacts. 4 Individual school closures were frequent during the months of May and June, and a nationwide closure of all schools was implemented during the first 2 weeks of July. Thereafter, the recommendation to close schools with confirmed cases for 2 weeks was kept in place through the duration of the pandemic. In addition to the closures, recommendations on social distancing measures of their children were given to families.
The socioeconomic impact of school closures and their and effectiveness in preventing children sent home from engaging in other social activities are not well documented. 7 , 8 , 9 We studied three schools in two Argentinean cities with significantly different socioeconomic profiles and examined (i) the economic impact of school closures on households; (ii) the opinions and attitudes of households toward closures; and (iii) household compliance during the school closures with the recommendation of preventing social contact among children.
Methods
Setting, study design, and data collection
In September 2009, after winter pandemic influenza activity had largely subsided in Argentina, we conducted a survey among households with children attending one of three public schools. Two of them (school A: ages 6–12; and school B: ages 13–15) were located in the city of Ushuaia, province of Tierra del Fuego, and the third (school C: ages 6–15) in the city of San Salvador de Jujuy, province of Jujuy. Tierra del Fuego is the southernmost province in Argentina and has one of the lowest poverty rates in the country. In contrast, Jujuy is located in the extreme northwest of the country and has among the highest poverty rates in the nation. 10 All three schools closed for 2 weeks in response to confirmed cases of pH1N1 among pupils; schools A and B closed in mid‐June, and school C in early September.
Written explanation of the study, a consent form guaranteeing anonymity and confidentiality, and questionnaires were provided to children to take home to their parents during the week of September 7–11 in schools A and B and during the week of September 14–18 in school C. The questionnaire asked about household demographic characteristics; health conditions of adults and children; economic costs due to the closures; children activities during closures; and parental attitudes toward the intervention. We sent follow‐up reminders after 2 days to parents who had not returned the questionnaire. Local health authorities collected completed questionnaires at schools, removed identifiable information, and sent them to MOH in Buenos Aires, who forwarded them to the US Centers for Disease Control and Prevention (CDC). The investigation protocol was reviewed by institutional review boards at CDC and MOH and was deemed to be part of the emergency public health response to the pandemic and not research.
Analysis
Survey data were entered into an Access database (Microsoft Corporation, Redmond, WA, USA) and analyzed using stata 11 (StataCorp LP, College Station, TX, USA). We combined the data from the schools in the city of Ushuaia and compared these responses to those from the school in Jujuy. Statistical analyses were conducted using bootstrapping, a methodology in which the original sample is resampled multiple times to produce a larger sample that has a distribution with similar characteristics to the original. 11 We generated 2000 bootstrapped samples and tested differences between the two cities in household characteristics and illness rates during the school period using Pearson chi‐squared tests. For the variables of interest, we used the same samples to generate 95% confidence intervals of their means and used Wald tests to determine the statistical significance of differences in means between the two cities.
From the perspective of the household, direct (out‐of‐pocket) and indirect (income losses) costs due to school closures in the two cities were compared. Additionally, opinions regarding school closures and adherence to social‐distancing recommendations during the closures were compared. Because household income was higher in Ushuaia than in Jujuy, household costs due to closures were compared both in absolute terms and relative to household income. Monthly household income information was aggregated into four categories (<Arg$1000; Arg$1001–Arg$2000; Arg$2001–Arg$3000; and >Arg$3000); actual monthly household income was imputed using this categorical information and the 2009 Encuesta Permanente de los Hogares (EPH) survey (see Appendix). 12 Then, among all households, average costs due to the closures as a proportion of imputed income were calculated.
Results
Demographic characteristics and illness
Questionnaires were sent to 499 households, and 226 were completed and returned (45% overall response rate, 49% in Ushuaia, and 41% in Jujuy). Clear socioeconomic differences among respondents existed between the two cities (Table 1). Households in Jujuy were larger on average than those in Ushuaia. Household income, parental education, and full‐time employment were higher in Ushuaia than in Jujuy. Prevalence of medical conditions with high risk of serious complications with influenza infection was similar in Ushuaia and Jujuy. Incidence of influenza‐like illness (ILI; defined as the presence of fever with cough or sore throat) during the time of the school closures was higher in Jujuy: ILI symptoms among adults were reported in 17% of households in Ushuaia and 26% in Jujuy (P = 0·20), while ILI symptoms among children were reported in 22% of households in Ushuaia and 30% in Jujuy (P = 0·31).
Table 1.
Household characteristics and illness during school closure*
| Ushuaia no. (%) | Jujuy no. (%) | P‐value** | |
|---|---|---|---|
| Total households (n = 226) | 145 | 81 | |
| Adults in household (n = 225) | |||
| One | 12 (8) | 11 (14) | 0·020 |
| Two | 89 (61) | 30 (38) | |
| Three or more | 44 (30) | 39 (49) | |
| Children ages 4 or younger (n = 223) | |||
| None | 107 (75) | 46 (57) | 0·027 |
| One | 28 (20) | 21 (26) | |
| Two or more | 7 (5) | 14 (17) | |
| Children ages 5–12 (n = 223) | |||
| None | 50 (35) | 4 (5) | <0·001 |
| One | 50 (35) | 27 (33) | |
| Two or more | 42 (30) | 50 (62) | |
| Children ages 13–16 (n = 223) | |||
| None | 88 (62) | 42 (52) | 0·053 |
| One | 44 (31) | 26 (32) | |
| Two | 10 (7) | 13 (16) | |
| Total Household Income (n = 205)*** | |||
| ARG$1000 or less | 4 (3) | 49 (65) | <0·001 |
| ARG$1001–$2000 | 3 (2) | 18 (24) | |
| ARG$2001–$3000 | 13 (10) | 4 (5) | |
| ARG$3001 or more | 110 (85) | 4 (5) | |
| Education, head of household (n = 217)† | |||
| Primary school or less | 17 (12) | 50 (67) | <0·001 |
| Secondary school | 51 (36) | 21 (28) | |
| Tertiary school | 26 (18) | 4 (5) | |
| University | 48 (34) | 0 (0) | |
| Employment, head of household (n = 217) | |||
| Public sector | 65 (45) | 14 (19) | 0·001 |
| Private sector | 29 (21) | 15 (20) | |
| Self‐employed | 31 (22) | 24 (32) | |
| Business owner | 6 (4) | 0 (0) | |
| Family business, no fixed income | 2 (1) | 9 (12) | |
| Unemployed, retired, stay at home | 10 (7) | 12 (16) | |
| Work schedule, head of household (n = 214) | |||
| Full‐time | 103 (73) | 25 (35) | <0·001 |
| Part‐time | 6 (4) | 11 (15) | |
| No fixed schedule | 23 (16) | 24 (33) | |
| Does not work | 10 (7) | 12 (17) | |
| Adults available to care for children (n = 220) | |||
| Unemployed/retired /stay at home | 34 (24) | 39 (51) | 0·003 |
| Part‐time work | 23 (16) | 18 (25) | 0·248 |
| Flexible schedule | 32 (23) | 43 (59) | <0·001 |
| Student (age 16 or older) | 41 (28) | 19 (25) | 0·462 |
| Only one adult in household (n = 226) | |||
| Yes | 12 (8) | 11 (14) | 0·307 |
| Health conditions of high risk during influenza infection (n = 226)†† | |||
| Adults | 30 (21%) | 15 (19%) | 0·486 |
| Children | 11 (8%) | 10 (12%) | 0·329 |
| Influenza‐like illness symptoms during closures††† | |||
| Among adults (n = 220) | 24 (17%) | 21 (26%) | 0·204 |
| Among children (n = 222) | 32 (22%) | 24 (30%) | 0·310 |
*Two schools were surveyed in Ushuaia (grades 1–6 and 7–9) and one school in Jujuy (grades 1–9). Schools in Ushuaia closed in May 2009 and the school in Jujuy closed in September 2009.
**P‐values were calculated using Pearson chi‐squared tests from 2000 bootstrapped samples.
***Exchange rate on 1 September 2009 was 3·8 Argentine pesos per U.S. dollar.
†Primary school refers to basic education, grades 1–6; secondary school refers to the 6 years following primary school; tertiary school refers to post‐secondary education, usually technical and of shorter duration than a university degree.
††High‐risk conditions include asthma, chronic respiratory conditions, chronic heart conditions, diabetes, renal disease, pregnancy status (only adults), and immune system conditions.
†††The case definition for ILI was the presence of fever with cough or sore throat.
Childcare arrangements and direct costs
Most households, 82% in Ushuaia and 88% in Jujuy, were able to make arrangements for either a family member or a friend to care for children. About 14% of households hired a babysitter or made other special childcare arrangements, and 3% reported that children were left alone (Table 2). Not all households with special childcare arrangements had childcare expenses: only 6% of households in Ushuaia and 4% in Jujuy reported these expenses. In contrast, although most households in both cities reported zero costs from other types of expenses – food, transportation, or other miscellaneous expenses –, these were more common, especially in Jujuy where 44% of households had at least one of these types of expenses, compared with 21% in Ushuaia (P < 0·001).
Table 2.
Childcare arrangements and household costs due to school closures*,**
| Ushuaia n (%; 95% CI) | Jujuy n (%; 95% CI) | P‐value | |
|---|---|---|---|
| Childcare arrangements (n = 202) | |||
| Relative or family friend cared for children | 103 (82; 75–88) | 67 (88; 81–95) | 0·196 |
| Hired nanny | 16 (13; 7–18) | 5 (7; 1–12) | 0·123 |
| Other special arrangement | 4 (3; 0–6) | 3 (4; 0–8) | 0·777 |
| Children were left alone | 3 (2; 0–5) | 1 (1; 0–4) | 0·564 |
| Households with costs due to the closures | |||
| Childcare expenses (n = 214) | 8 (6; 2–10) | 3 (4; 0–8) | 0·561 |
| Other expenses (n = 194) | 27 (21; 14–29) | 30 (44; 32–56) | <0·001 |
| Transportation | 7 (6; 2–10) | 13 (19; 10–29) | 0·009 |
| Food | 8 (6; 2–11) | 18 (26; 16–37) | 0·001 |
| Other miscellaneous | 21 (17; 10–23) | 21 (31; 20–42) | 0·029 |
| Lost workdays (n = 198) | 36 (27; 20–34) | 7 (11; 3–19) | 0·002 |
| Lost work income (n = 192) | 4 (3; 0–6) | 4 (6; 0–13) | 0·329 |
| Ushuaia # days (95% CI) | Jujuy # days (95% CI) | ||
|---|---|---|---|
| Average number of workdays lost | |||
| Workdays lost, all households (n = 191) | 2·3 (1·6–3·1) | 0·3 (0·0–0·5) | <0·001 |
| Workdays lost, only those with lost days (n = 36) | 9·7 (8·6–10·9) | 3·2 (2·3–4·1) | <0·001 |
| Ushuaia ARG$ (95% CI) | Jujuy ARG$ (95% CI) | ||
|---|---|---|---|
| Direct and indirect costs: all households | |||
| Childcare expenses (n = 214) | 36 (6–66) | 7 (0–15) | 0·062 |
| Other expenses (n = 176) | 48 (26–69) | 86 (31–140) | 0·201 |
| Lost work income (n = 192) | 35 (0–72) | 13 (0–26) | 0·293 |
| Direct and indirect costs: only households with expenses or lost workdays | |||
| Childcare (n = 11) | 625 (406–843) | 170 (77–263) | <0·001 |
| Other expenditures (n = 39) | 273 (210–336) | 277 (127–426) | 0·935 |
| Lost work income (n = 37) | 141 (0–293) | 156 (40–272) | 0·872 |
*Confidence intervals and P‐values were estimated using 2000 bootstrapped samples.
**Boldface indicates point estimates for percentages and is used only for easier reading of the table.
Average childcare expenditures were higher in Ushuaia than in Jujuy: Arg$36 vs. Arg$7 (P = 0·06). Mean non‐childcare expenditures were higher in households in Jujuy, although not statistically significant: Arg$48 vs. Arg$86 (P = 0·20). When average expenditures were calculated only among households that had expenses, similar expenditure patterns were observed.
Indirect costs
In Ushuaia, 27% of households reported adults missing workdays, compared with 11% in Jujuy (P = 0·002, Table 2). The average number of workdays lost in the household was also significantly higher in Ushuaia than in Jujuy: 2·3 days vs 0·3 days, respectively (P < 0·001). In Ushuaia, only 11% of households with lost workdays also reported lost work income, compared with 57% in Jujuy. Average income lost due to missed workdays was Arg$35 in Ushuaia and Arg$13 in Jujuy (P = 0·293). Two households in Ushuaia and one in Jujuy (data not shown) reported employment loss due to closure‐related work absences. We do not include job loss in our calculations of economic costs summarized below.
Costs of closures relative to monthly household income
Childcare expenses as a percentage of household income were higher in Jujuy (1·4%) than in Ushuaia (0·5%), but the difference was not statistically significant (P = 0·31). Work‐related lost income as percentage of household income was also higher in Jujuy (1·8%) than in Ushuaia (0·5%), but this difference was not statistically significant (P = 0·26). Non‐childcare expenses as a share of household income were significantly larger in Jujuy than in Ushuaia (8·4% vs. 1·6%, P = 0·01). Total household costs due to the closures in Ushuaia represented about 2·6% of monthly household income, while in Jujuy they amounted to 11·3% of monthly household income (P = 0·01) (Figure 1).
Figure 1.
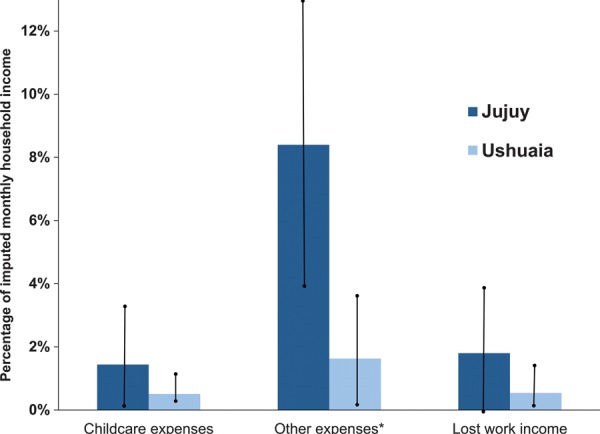
Average household costs, as a percentage of household income, due to closures of three schools during the 2009 pH1N1 pandemic in two Argentinean cities. Household income was imputed (see Appendix) Whiskers represent 95% confidence intervals, estimated using 2000 bootstrapped samples. Statistical significance for differences between the two cities: *P < 0·05.
Household opinions regarding school closures
Most respondents (70%) reported that school closures did not affect their household’s economy (Table 3). This percentage, however, was larger in Ushuaia than in Jujuy: 75% vs. 61%, respectively (P = 0·04). Similarly, while only 6% of households in Ushuaia reported that the closures affected them “considerably”, 18% of households in Jujuy reported they had been affected as such (P = 0·02).
Table 3.
Household opinion regarding school closures*,**
| Ushuaia n (%; 95% CI) | Jujuy n (%; 95% CI) | P‐value | |
|---|---|---|---|
| Do you think school closure affected your household’s economy? (n = 209) | |||
| No | 101 (75; 68–82) | 45 (61; 50–72) | 0·039 |
| Yes, somewhat | 26 (19; 13–26) | 16 (22; 13–31) | 0·693 |
| Yes, considerably | 8 (6; 2–10) | 13 (18; 9–26) | 0·016 |
| Do you agree with the closure? (n = 221) | |||
| Yes | 109 (78; 71–84) | 58 (72; 62–81) | 0·295 |
| No | 21 (15; 9–21) | 20 (25; 15–34) | 0·090 |
| Unsure | 10 (7; 3–11) | 3 (4; 0–8) | 0·259 |
| If you do not agree or unsure, why? (n = 47)*** | |||
| My child’s education would be affected | 13 (52; 31–73) | 18 (82; 65–99) | 0·024 |
| Closures do not protect against influenza | 11 (44; 24–64) | 7 (32; 11–52) | 0·381 |
| Economic impact of closure | 1 (4; 0–12) | 1 (5; 0–14) | 0·922 |
| Did not have alternatives for childcare | 0 (0; –) | 1 (5; 0–14) | 0·286 |
| My child would not get school lunches | 0 (0; –) | 1 (5; 0–14) | 0·286 |
| Another reason | 7 (28; 10–46) | 1 (5; 0–14) | 0·020 |
*Confidence intervals and P‐values were estimated using 2000 bootstrapped samples.
**Boldface indicates point estimates for percentages and is used only for easier reading of the table.
***Households in the bottom panel are those who either disagreed with the closures or were not sure they agreed with them and gave a reason for it. Multiple answers were allowed.
About 78% of households in Ushuaia and 72% in Jujuy (P = 0·29) reported agreement with school closures. Among those that did not agree or were uncertain, the most common reason was concern about the impact of closures on children’s education, reported by 52% of these households in Ushuaia and 82% in Jujuy. The next most important reason was skepticism about their effectiveness in protecting children, reported by 44% of households who did not agree with closures in Ushuaia and 32% in Jujuy. Only two households, one in each province, reported concerns about an economic impact of the closures as a reason to disagree with them.
Compliance with social distancing recommendations
Overall, 67% of households reported that children visited public places at least once during the 2 weeks schools were closed, and 45% left the house several times. The most commonly visited place was the supermarket. Other commonly visited places were plazas and recreation areas, shopping malls, and indoor gatherings with groups of four or more friends. There were a few differences between the two cities in places visited by children. For example, children in Jujuy were more likely to attend religious events, use public transportation, and go to plazas and recreation areas than children in Ushuaia. Children in Ushuaia were more likely to go to the movie theater and restaurants than children in Jujuy were (Figure 2). The frequency of ILI reported by children in either city who visited public places was not different to the frequency among those who did not visit such places (data not shown).
Figure 2.
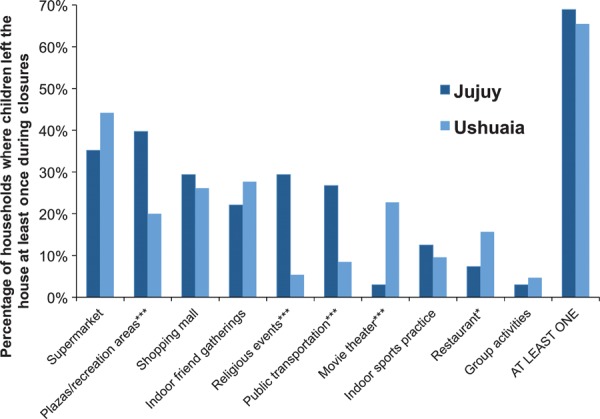
Places visited by children during the closures of three schools in the 2009 pH1N1 pandemic in two Argentinean cities. Statistical significance for difference between the two cities: *P < 0·1, **P < 0·05, ***P < 0·01.
Discussion
In our study of school closures during the 2009 pandemic in two socioeconomically diverse cities in Argentina, we found differences in the economic impact of this intervention between the two cities. In Ushuaia (the wealthier city), the total costs and workdays lost due to the closures were higher than in Jujuy; yet, as a percentage of income, households in Jujuy experienced the greater economic impact. This result was also reflected in subjective household opinions regarding the impact of closures, where a larger proportion of households in Jujuy reported they were affected by the intervention. Interestingly, the proportion of households in the wealthier city (75%) that considered the closures did not affect them was similar to the proportion of households that did not consider closures a problem in a recent report in the United States. 13 This finding suggests that local contexts are important in assessing the impact of school closures. Although few households had childcare‐related expenses during the closures, we found that non‐childcare expenses, such as food and transportation, were common. Nearly half the households in the city with lower socioeconomic status were affected by these expenses, probably in large part due to higher dependence on school‐provided meals than households in Ushuaia (Jujuy school staff, personal communication, September 2010). Studies of the economic costs of school closures often focus on childcare expenses and lost work income, but our findings suggest that – at least in middle‐income countries like Argentina, where households are larger, and thus, adults are more likely to be available to care for children – other types of expenses may be a more important burden for households.
Jujuy households appear to have experienced higher income loss than Ushuaia households when working adults stayed home to care for the children. Although households in Ushuaia were more likely to report lost workdays, only 11% of households that lost workdays also reported lost work income, compared with 57% in Jujuy. In our sample, the percent of householders in Jujuy who worked with no fixed schedule is twice as large as in Ushuaia (33% vs. 16%, Table 1), indicating that adults in Ushuaia may be more likely to have salaried jobs where a lost workday may not lead to income loss, while adults in Jujuy may be more likely to earn income on a per hour or day worked basis.
Although we found broad support for school closures in both cities (76%), despite the differential economic impact, this was lower than the support recently reported in the United States (90%). 13 However, this difference might be attributed to the fact that only 26% of closures in the United States survey lasted 4 days or longer. 13 Concern about the educational impact of the intervention was particularly high among Jujuy households, perhaps because they have lower access to means to minimize this impact (e.g., private tutors) than households in Ushuaia. This is consistent with findings that the impact of summer school breaks on learning is larger among children from disadvantaged backgrounds. 14 In addition, of those who disagreed with the closures, 38% cited a lack of belief that they protect children from influenza.
In both cities, despite recommendations from MOH, children in more than two‐thirds of households left their home during the school closures to spend time in public places. This is consistent with previous findings in Australia and the United States that school closures do not pre‐empt children from gathering in alternative locations such as markets, friends’ houses, or shopping malls. 13 , 15 , 16 However, the impact of lack of compliance on the effectiveness of the intervention is not clear because contact patterns may be lower during the closure, thus reducing virus transmission even if children visit public places. 17 A recent study estimated the influenza reproduction number decreased by 35% during holidays due to lower contact rates. 18 Moreover, empirical studies have found significant impacts of school closures in reducing influenza transmission among school‐aged children and the community, 19 , 20 , 21 including studies conducted in Argentina. 4 , 22 . Additionally, a recent Australian study found high compliance with social isolation recommendations during school closures in the early stages of the 2009 pandemic, perhaps due to high awareness and uncertainty about health risks. 23
There are several limitations to our study. First, we have a small, convenience sample of households and a low response rate, so our results may not be representative of households in the cities where these schools were located. Second, schools were selected based on their willingness to participate in the study, resulting in households in Ushuaia being surveyed 3 months after the school closures, while households in Jujuy were surveyed only 1 week after the closure; thus, some of the estimated differences between the two cities may be due to recall bias. Research suggests recall bias for earnings is small within 1 year and higher earnings relative to income are easier to recall; however, it is unclear how this result may apply to recall of costs that represent only a fraction of household income. 24 Third, a large number of heads of household in Ushuaia were employed in the public sector. Estimates from the 2001 Argentinean National Census indicate that the proportion of public employees in Tierra del Fuego is larger than in Jujuy, 25 but the difference (37% vs. 30%) is not as large as in our sample. Public workers may be more likely than part‐time or self‐employed workers to receive paid sick leave. Fourth, there were significant differences between the two cities in the ages of children living in households affected by the closures; this might explain, at least partially, the differences in costs. Finally, we may have underestimated household costs because we did not have interviewers explaining questions to parents or guardians; for example, several respondents who said their children went to restaurants, movie theaters, or used public transportation during the closure also reported zero non‐childcare expenses; some of those expenses might not have occurred without the closure and should have been reported. In addition, because we used the household perspective, we did not estimate societal costs such as expenses to plan and implement the closures and productivity losses due to lost workdays.
Our results indicate that school closures may disproportionately affect low‐income households. It is not clear whether this impact (11% of imputed monthly household income on average) is significant, but 20% of households in the lower‐income city subjectively considered the impact to be substantial. Policymakers should consider how to minimize the negative effects of closures on households, especially in low‐income areas; for example, strategies used to cope with large disasters could be adopted to ensure the continuity of school lunch programs during school closures. 26 Legislation may also be needed to guarantee job security for parents staying home to care for children during a mandated school closure. Policies to reduce the educational impact of closures should be considered as well, as this was the most important concern expressed by parents; for example, measures used to ensure continuity of school lunch programs could be modified to accommodate giving instructions to parents on lessons or readings to assign to their children. Distance learning could also be used, although it may not be feasible in middle‐ and lower‐income settings. Finally, authorities should develop a communication strategy to help parents understand the benefits of school closures and the importance of practicing social distancing during the closures.
Addendum
Ricardo Basurto‐Dávila is the principal investigator (PI). He contributed to study conception and design, questionnaire design, data collection, data entry, data analysis, and manuscript drafting and revision; Roberto Garza is the co‐PI. He contributed to study conception and design, questionnaire design, data entry, interpretation of results, and manuscript drafting and revision; Martin I. Meltzer contributed to study design, questionnaire design, data analysis, interpretation of results, and manuscript revision; Oreste L. Carlino led the Argentinean MOH team. He contributed to study conception and design, questionnaire design, and manuscript revision; Rachel Albalak contributed to study design, questionnaire design, interpretation of results, and manuscript revision; Pablo W. Orellano led the investigation efforts in Tierra del Fuego. He contributed to school recruitment and training, data collection, and manuscript revision; Osvaldo Uez contributed to coordination efforts with authorities in Jujuy, school recruitment and training, data collection, and manuscript revision; David K. Shay contributed to study design, interpretation of results, and manuscript revision; Cora Santandrea contributed to study design, questionnaire design, school recruitment, data collection, and manuscript revision; María del Carmen Weis contributed to study design, questionnaire design, school recruitment, and manuscript revision; Francisco Averhoff contributed to study conception and design, questionnaire design, interpretation of results, and manuscript revision; Marc‐Alain Widdowson contributed to study conception and design, questionnaire design, interpretation of results, and manuscript revision.
Biographical sketch
Dr. Basurto‐Dávila is an Economist and the Los Angeles County Department of Public Health. He was a Prevention Effectiveness Fellow at the U.S. Centers for Disease Control and Prevention when this work was conducted. His research interests include health economics, burden of illness, and control of infectious diseases.
Disclosure of competing interests
The authors have no competing interests.
Supporting information
Data S1. Parental consent form and questionnaire.
Supporting info item
Acknowledgements
We would like to thank study participants for providing data and school administrators and staff for collaborating in our data collection efforts. We also thank provincial health and education authorities in Jujuy and Tierra del Fuego for their assistance and advice in the planning and implementation of the project. Finally, we thank officials from the Pan American Health Organization for their assistance with the logistics of this project. This work was supported by the U.S. Centers for Disease Control and Prevention and the Pan American Health Organization.
Appendix: Imputation of monthly household income
In our survey, we asked households to provide information on their total monthly income by classifying such income in one of four brackets (in Argentine pesos): $1000 or less, between $1001 and $2000, between $2001 and $3000, and more than ARG$3000. To calculate household expenditures due to school closures as a percentage of household income, we applied an imputation procedure to get estimates of monthly household income.
For the imputation, we combined the categorical income information described above with data from the 2009 EPH, a quarterly survey of households in Argentina that collects detailed income data for a large sample of households in 31 urban centers in Argentina, including the cities of Ushuaia and Jujuy. The imputation procedure consisted of the following steps: first, we removed from EPH’s data sets households with no children under 16 years of age and households in cities other than Ushuaia or Jujuy; we then classified EPH’s Ushuaia and Jujuy households in four groups, according to the monthly income brackets available in our survey data; finally, average monthly household income was computed for each city‐income group combination using EPH’s sampling weights, and this group‐average income was assigned to households in our survey, according to their corresponding city and income brackets. Imputation was performed only for households that provided information on their income bracket, 90 percent of households in Ushuaia and 91 percent of households in Jujuy. Although the imputation method is simple, it incorporates information on the income distribution within each bracket and thus represents an improvement over the common practice of using bracket midpoints.
References
- 1. Cauchemez S, Bhattarai A, Marchbanks TL et al. Role of social networks in shaping disease transmission during a community outbreak of 2009 H1N1 pandemic influenza. Proc Natl Acad Sci USA 2011; 108:2825–2830. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Loeb M, Russell M, Moss L et al. Effect of influenza vaccination of children on infection rates in hutterite communities. JAMA 2010; 303:943–950. [DOI] [PubMed] [Google Scholar]
- 3. Glass LM, Glass RJ. Social contact networks for the spread of pandemic influenza in children and teenagers. BMC Public Health 2008; 8:61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Orellano PW, Grassi A, Reynoso JI, Palmieri A, Uez O, Carlino O. Efecto del cierre de las escuelas sobre el brote de influenza A H1N1 en Tierra del Fuego, Argentina. Rev Panam Salud Pública 2010; 27:226–229. [DOI] [PubMed] [Google Scholar]
- 5. Fraser C, Donnelly CA, Cauchemez S et al. Pandemic potential of a strain of influenza A (H1N1): early findings. Science 2009; 324:1557–1561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Kar‐Purkayastha I, Ingram C, Maguire H, Roche A. The importance of school and social activities in the transmission of influenza A(H1N1)v: England, April–June 2009. Euro Surveill 2009; 14:pii=19311. [DOI] [PubMed] [Google Scholar]
- 7. Fukuda K, Harmanci H, Park K et al. Pandemic Influenza Preparedness and Response. Geneva, Switzerland: Global Influenza Programme, World Health Organization, 2009. [Google Scholar]
- 8. President Council of Advisors on Science and Technology . Report to the President on U.S. Preparations for 2009 – H1N1 Influenza. Washington, DC: President Executive Office, 2009. [Google Scholar]
- 9. Monto A. The risk of seasonal and pandemic influenza: prospects for control. Clin Infect Dis 2009; 48:S20–S25. [DOI] [PubMed] [Google Scholar]
- 10. IADER . La pobreza en las provincias se acerca al 50% de la población, 2008. Available at http://www.iader.org.ar/?x=pobreza_pais (Accessed 15 January 2010).
- 11. Horowitz JL. The bootstrap in econometrics. Stat Sci 2003; 18:211–218. [Google Scholar]
- 12. Instituto Nacional de Estadística y Censos . La nueva encuesta permanente de hogares de Argentina, 2003. Available at http://www.indec.gov.ar/nuevaweb/cuadros/4/Metodologia_EPHContinua.pdf (Accessed 5 July 2010).
- 13. Steelfisher GK, Blendon RJ, Bekheit MM et al. Parental attitudes and experiences during school dismissals related to 2009 influenza A (H1N1) – United States, 2009. Morb Mortal Wkly Rep 2010; 59:1131–1134. [PubMed] [Google Scholar]
- 14. Entwisle DR, Alexander KL. Summer setback: race, poverty, school composition, and mathematics achievement in the first two years of school. Am Sociol Rev 1992; 57:72–84. [Google Scholar]
- 15. Effler PV, Carcione D, Giele C, Dowse GK, Goggin L, Mak DB. Household responses to pandemic (H1N1) 2009‐related school closures, Perth, Western Australia. Emerg Infect Dis 2010; 16:205–211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Johnson AJ, Moore ZS, Edelson PJ et al. Household responses to school closure resulting from outbreak of influenza B, North Carolina. Emerg Infect Dis 2008; 14:1024–1030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Mossong J, Hens N, Jit M et al. Social contacts and mixing patterns relevant to the spread of infectious diseases. PLoS Med 2008; 5:e74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Eames KTD, Tilston NL, Brooks‐Pollock E, Edmunds WJ. Measured dynamic social contact patterns explain the spread of H1N1v influenza. PLoS Comput Biol 2012; 8:e1002425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Cauchemez S, Valleron A‐J, Boëlle P‐Y, Flahault A, Ferguson NM. Estimating the impact of school closure on influenza transmission from Sentinel data. Nature 2008; 452:750–754. [DOI] [PubMed] [Google Scholar]
- 20. Cauchemez S, Ferguson NM, Wachtel C et al. Closure of schools during an influenza pandemic. Lancet Infect Dis 2009; 9:473–481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Heymann A, Chodick G, Reichman B, Kokia E, Laufer J. Influence of school closure on the incidence of viral respiratory diseases among children and on health care utilization. Pediatr Infect Dis J 2004; 23:675–677. [DOI] [PubMed] [Google Scholar]
- 22. Garza R, Basurto‐Dávila R, Carlino LO et al. The impact of winter holidays on the incidence of influenza‐like illness in Argentina, 2005–2008. Paper presented at: International Conference on Options for the Control of Influenza VII; September 5, 2010, Hong Kong.
- 23. McVernon J, Mason K, Petrony S et al. Recommendations for and compliance with social restrictions during implementation of school closures in the early phase of the influenza A (H1N1) 2009 outbreak in Melbourne, Australia. BMC Infect Dis 2011; 11:257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. de Nicola F, Giné X. How accurate are recall data? Evidence from coastal India. World Bank Policy Research Working Paper , 2012. Available at http://go.worldbank.org/WRM8B5NJ50 (Accessed 8 August 2012).
- 25. Instituto Nacional de Estadística y Censos . Resultados Nacionales del Censo 2001, 2001. Available at http://www.indec.gov.ar/censo2001s2/ampliada_index.asp?mode=01 (Accessed 5 August 2012).
- 26. Berkman BE. Mitigating pandemic influenza: the ethics of implementing a school closure. J Public Health Manag Pract 2008; 14:372–378. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1. Parental consent form and questionnaire.
Supporting info item