

Abstract
We sought to examine the concordance of two suicidal ideation items from the Patient Health Questionnaire-9 (PHQ-9) and the Edinburgh Postnatal Depression Scale (EPDS), to evaluate the prevalence of suicidal ideation among pregnant women, and to assess the co-occurrence of suicidal ideation with antepartum depressive symptoms. A cross-sectional study was conducted among 1,517 pregnant women attending prenatal care clinics in Lima, Peru. Item 9 of the PHQ-9 assesses suicidal ideation over the last 14 days while item 10 of the EPDS assesses suicidal ideation in the past 7 days. The two suicidal ideation items have a high concordance rate (84.2%) but a moderate agreement (the Cohen's kappa = 0.42). Based on the PHQ-9 and the EPDS, 15.8% and 8.8% of participants screened positive for suicidal ideation, respectively. Assessed by the PHQ-9, 51% of participants with suicidal ideation had probable depression. In prenatal care clinics, screening for suicidal ideation is needed for women with and without depressive symptoms. Future studies are needed to identify additional predictors of antepartum suicidality, determine the appropriate duration of reporting period for suicidal ideation screening, and assess the percentage of individuals with positive responses to the two suicidal ideation items at high risk of planning and attempting suicide.
Keywords: Suicidal ideation, antepartum depressive symptoms, PHQ-9, EPDS
Introduction
Globally, suicide is one of the leading causes of death during the perinatal period (Chang et al. 2005; Gavin et al. 2011; Lindahl et al. 2005; Shadigian and Bauer 2005). Suicidal ideation, a cause for concern (Howard et al. 2011), is considered a precursor and distal predictor of later suicidal death (Joiner et al. 2000; Lindahl et al. 2005), and also presents an opportunity for interventions prior to physical self-harm (Lindahl et al. 2005). During the perinatal period, the prevalence of suicidal ideation ranges from 5% to 14% (Lindahl et al. 2005). Specific attention should be paid to suicidal ideation during pregnancy because of fetal consequences and many non-fatal adverse outcomes for both mothers and infants (Bowen et al. 2009; Chaudron et al. 2001; Copersino et al. 2008; Eggleston et al. 2009; Gausia et al. 2009; Gavin et al. 2011; Lindahl et al. 2005; Newport et al. 2007; Paris et al. 2009; Stallones et al. 2007). Screening is an important approach to detect patients at risk for suicide. However, during pregnancy, systematic screening for suicidal ideation is rare (Gavin et al. 2011) due to time constraints in prenatal care clinics, the lack of proper screening instruments, and stigmatization of suicide in certain cultural settings (Tadros and Jolley 2001).
As a result of the comorbid nature of suicidal ideation and depression (Gavin et al. 2011; Nock et al. 2012), suicidal ideation is usually assessed along with depression screening rather than separately (Beck et al. 1961; Cox et al. 1987; Hamilton 1960; Kroenke et al. 2001; Spitzer et al. 1999), and consequently, there is no preferred screening instrument for assessing suicidal ideation (Brown 2001; Stallones et al. 2007). Of the available instruments, the two most widely used antepartum depression screening instruments are the Patient Health Questionnaire-9 (PHQ-9) (Kroenke et al. 2001; Spitzer et al. 1999) and the Edinburgh Postnatal Depression Scale (EPDS) (Cox et al. 1987). Item 9 of the PHQ-9 and item 10 of the EPDS assess suicidal ideation. There is no clear consensus as to which instrument is recommended for screening antepartum depression (Flynn et al. 2011), and the evidence of the comparability of the two suicidal ideation items is scarce, especially among pregnant women. To date, only one study (Yawn et al. 2009) has compared the concordance and discordance of reports of suicidal ideation when these two items were included in a study of 481 postpartum women in the U.S. During the postpartum period, Yawn et al. reported that the prevalence estimates for suicidal ideation assessed by the PHQ-9 and the EPDS was 6.4% and 7.3%, respectively. The authors also reported that 93.8% of the participants had concordant responses for the two items.
Given the paucity of research evaluating the comparability of two suicidal ideation items from the PHQ-9 and EPDS during pregnancy and a growing body of evidence documenting antepartum depression as one of the major causes of morbidity in low- and middle-income countries (Bennett et al. 2004; Ferrari et al. 2013), we conducted the present study to examine the concordance of the two suicidal ideation items among pregnant Peruvian women. Considering the lack of updated information among this population, the prevalence of suicidal ideation was assessed using the PHQ-9 and the EPDS. To provide a clearer understanding of the association between antepartum depression and suicidal ideation, we further sought to examine the co-occurrence of antepartum depressive symptoms with suicidal ideation.
Methods
Study Population
This cross-sectional study was a part of the Pregnancy Outcomes, Maternal and Infant Study (PrOMIS) Cohort, an ongoing prospective cohort study of pregnant women enrolled in prenatal care clinics at the Instituto Nacional Materno Perinatal (INMP) in Lima, Peru. The INMP, overseen by the Peruvian Ministry of Health, is the primary referral hospital for maternal and perinatal care. From February 2012 to March 2013, we recruited women who started their first prenatal care visit in the INMP. The study population included pregnant women who were 18-49 years with a gestational age ≤ 16 weeks and who spoke and understood Spanish. All participants provided informed consent. The Institutional Review Boards from the INMP and the Human Research Administration Office at Harvard School of Public Health approved all procedures used in this study.
Data Collection and Variable Specification
Using a structured questionnaire, participants were interviewed by trained research personnel in a private setting. Information regarding maternal socio-demographics, lifestyle characteristics, medical and reproductive history, childhood abuse and lifetime intimate partner violence, and depressive symptoms was collected. For all participants, we first administered the PHQ-9 then the EPDS. Of the 1,810 eligible participants, 1,556 completed the interview. With 39 participants excluded because of missing information on the PHQ-9 and EPDS, 1,517 participants remained in the present analysis.
The Patient Health Questionnaire (PHQ-9)
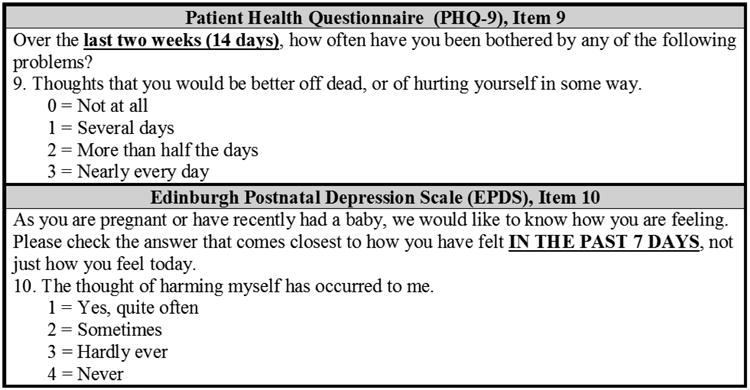
The PHQ-9 is a 9-item, depression-screening scale (Kroenke et al. 2001; Spitzer et al. 1999). In our study, this questionnaire assesseed 9 depressive symptoms experienced by participants in the 14 days prior to evaluation. Each item was rated on the frequency of a depressive symptom. The PHQ-9 score was calculated by assigning a score of 0, 1, 2, or 3 to the response categories of “not at all,” “several days,” “more than half the days,” or “nearly every day,” respectively. We categorized participants as exhibiting minimal (PHQ-9 score 0-4), mild (PHQ-9 score 5-9), moderate (PHQ-9 score 10-14), and moderately severe/severe (PHQ-9 score ≥ 15) depressive symptoms. In particular, item 9, “thoughts that you would be better off dead, or of hurting yourself,” assessed suicidal ideation over the last 14 days (Figure 1). Suicidal ideation was defined on the basis of particiants' response to item 9. If the response was “several days,” “more than half the days,” or “nearly every day,” suicidal ideation was coded as “yes.” Participants responding “not at all” were classified as “no” for suicidal ideation.
Figure 1. Suicidal Ideation Items on Depression Scales.
The Edinburgh Postnatal Depression Scale (EPDS)
The EPDS is a 10-item, widely used screening scale for antepartum and postpartum depression (Cox et al. 1987). The EPDS items asked participants to rate how they felt during the previous 7 days. Response categories were scored 0, 1, 2, or 3 for each item according to increased severity of the symptoms. Items 3 and 5-10 were reversed scored. We assessed participants' severity of depression at cutoff scores of 10, 12, and 16, representing the thresholds for “normal,” “slightly increased risk,” “increased risk,” and “marked risk” for depression (Cox et al. 1987; Yawn et al. 2009). Item 10 (Figure 1) asked participants to rate the frequency of “the thought of harming myself has occurred to me” in the past 7 days as “yes, quite often,” “sometimes,” “hardly ever,” or “never.” Suicidal ideation was defined based on item 10. For suicidal ideation, participants who gave a response of “yes, quite often,” “sometimes,” or “hardly ever” were categorized as “yes,” but categorized as “no” when endorsing the response category “never.”
Statistical Analysis
We examined the frequency distribution of maternal socio-demographic characteristics and reproductive history. For participants with and without suicidal ideation assessed by each scale, the chi-square test for categorical variables and the Student's t-test for continuous variables were conducted to determine statistically significant differences. In addition, the frequency distribution of maternal socio-demographic characteristics was assessed by the endorsement of two suicidal ideation items and classified into 4 groups: (1) positive responses to both item 9 of the PHQ-9 and item 10 of the EPDS; (2) positive response to only item 9 of the PHQ-9; (3) positive response to only item 10 of the EPDS; and (4) negative responses to both items. Across these 4 groups, we conducted the chi-square test for categorical variables and the one-way analysis of variance (ANOVA) for continuous variables to determine whether there were statistically significant differences in the distribution of socio-demographic, reproductive characteristics, the PHQ-8 score (the PHQ-9 total score excluding item 9), and the EPDS total score excluding item 10. Using the Cohen's Kappa, the agreement between item 9 of the PHQ-9 and item 10 of the EPDS was evaluated. Using the Student's t-tests, the mean scores of the PHQ-9 and the EPDS (included/excluded suicidal ideation items) were compared between participants with and without suicidal ideation. The chi-square test for trend was performed to detect the difference in proportions of suicidal ideation across the total scores of the PHQ-9 and the EPDS. The odds ratios (ORs) and 95% confidence intervals (CIs) were calculated to assess the association between antepartum depressive symptoms and suicidal ideation. All statistical analyses were performed using SAS 9.3 (SAS Institute, Cary, NC, USA). The level of statistical significance was set at p < 0.05, and all tests were two-sided.
Results
Socio-demographic and reproductive characteristics of the study population are presented in Table 1. The mean age of the participants was 28 years (standard deviation = 6.2 years); the majority of the participants were married or living with a partner (81.3%), had at least 7 years of education (95.5%), and self-identified race/ethnicity as Mestizo (75.3%). The average gestational age of participants was 9.8 weeks (standard deviation = 3.4 weeks). On the structured questionnaire, 56.4% of the participants reported that they were unemployed, and 51.3% felt that paying for the very basic food items was “hard” or “somewhat hard.” With respect to the history of abuse, 68.5% of participants have experienced childhood abuse (physical or sexual abuse), and 59.1% experienced lifetime intimate partner violence (physical, sexual or emotional abuse).
Table 1. Socio-demographics and Reproductive Characteristics of the Study Population (N = 1517).
| Characteristic | Participants (N=1517) | Suicidal ideation assessed by PHQ-9b | Suicidal ideation assessed by EPDSb | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|||||||||||
| Yes (n = 239) | No (n = 1278) | p-value | Yes (n = 134) | No (n = 1383) | p-value | |||||||
|
|
|
|
|
|
||||||||
| n | % | n | % | n | % | n | % | n | % | |||
| Age (years) a | 28.0 ± 6.2 | 27.6 ± 6.4 | 28.1 ± 6.2 | 0.24 | 27.4 ± 6.7 | 28.1 ± 6.2 | 0.20 | |||||
| Age (years) | ||||||||||||
| 18-20 | 91 | 6.0 | 18 | 7.5 | 73 | 5.7 | 0.48 | 12 | 9.0 | 79 | 5.7 | 0.42 |
| 20-29 | 856 | 56.4 | 140 | 58.6 | 716 | 56 | 77 | 57.5 | 779 | 56.3 | ||
| 30-34 | 305 | 20.1 | 42 | 17.6 | 263 | 20.6 | 24 | 17.9 | 281 | 20.3 | ||
| ≥35 | 265 | 17.5 | 39 | 16.3 | 226 | 17.7 | 21 | 15.7 | 244 | 17.6 | ||
| Mestizo race/ethnicity | 1142 | 75.3 | 168 | 70.3 | 974 | 76.2 | 0.13 | 92 | 68.7 | 1050 | 75.9 | 0.02 |
| Education (years) | ||||||||||||
| ≤6 | 68 | 4.5 | 14 | 5.9 | 54 | 4.2 | 0.002 | 7 | 5.2 | 61 | 4.4 | 0.08 |
| 7-12 | 851 | 56.1 | 154 | 64.4 | 697 | 54.5 | 86 | 64.2 | 765 | 55.3 | ||
| >12 | 593 | 39.1 | 69 | 28.9 | 524 | 41.0 | 40 | 29.9 | 553 | 40.0 | ||
| Married or living with a partner | 1233 | 81.3 | 185 | 77.4 | 1048 | 82.0 | 0.11 | 107 | 79.9 | 1126 | 81.4 | 0.69 |
| Unemployed | 855 | 56.4 | 147 | 61.5 | 708 | 55.4 | 0.23 | 85 | 63.4 | 770 | 55.7 | 0.18 |
| How hard to pay for the very basics | ||||||||||||
| Very hard/hard | 286 | 18.9 | 69 | 28.9 | 217 | 17 | <0.0001 | 39 | 29.1 | 247 | 17.9 | <0.0001 |
| Somewhat hard | 492 | 32.4 | 76 | 31.8 | 416 | 32.6 | 42 | 31.3 | 450 | 32.5 | ||
| Not very hard | 738 | 48.7 | 94 | 39.3 | 644 | 50.4 | 53 | 39.6 | 685 | 49.5 | ||
| Nulliparous | 765 | 50.4 | 116 | 48.5 | 649 | 50.8 | 0.52 | 63 | 47.0 | 702 | 50.8 | 0.41 |
| Gestational age at interview (weeks) a | 9.8 ± 3.4 | 10.2 ± 3.5 | 9.7 ± 3.3 | 0.05 | 10.1 ± 3.4 | 9.7 ± 3.4 | 0.29 | |||||
| Unplanned pregnancy | 875 | 57.7 | 171 | 71.5 | 704 | 55.1 | <0.0001 | 98 | 73.1 | 777 | 56.2 | 0.0001 |
| Any childhood abuse c | 1039 | 68.5 | 203 | 84.9 | 836 | 65.4 | <0.0001 | 112 | 83.6 | 927 | 67.0 | <0.0001 |
| Any lifetime intimate partner violence d | 897 | 59.1 | 190 | 79.5 | 707 | 55.3 | <0.0001 | 119 | 88.8 | 778 | 56.3 | <0.0001 |
Due to missing data, percentages may not add up to 100%.
mean ± standard deviation
The Patient Health Questionnaire (PHQ-9) assesses suicidal ideation experienced by participants in the 14 days prior to evaluation. The Edinburgh Postnatal Depression Scale (EPDS) assesses suicidal ideation experienced by participants in the 7 days prior to evaluation.
Including physical or sexual abuse
Including physical, sexual or emotional abuse
Compared with participants without suicidal ideation, participants with suicidal ideation were more likely to have difficulty paying for very basic foods and to experience an unplanned pregnancy. They were also more likely to experience childhood abuse and intimate partner violence (Table 1).
Across 4 suicidal ideation groups, we observed significant differences for the frequency distribution of educational attainment, difficulty purchasing very basic foods, unplanned pregnancy, childhood abuse, and intimate partner violence (Table 2). In addition, significant differences were observed for the PHQ-8 score and the EPDS total score excluding item 10.
Table 2. Socio-demographics and Reproductive Characteristics of the Study Population by Endorsement of Suicidal ideation Assessed by the Patient Health Questionnaire (PHQ-9) and the Edinburgh Postnatal Depression Scale (EPDS) a (N=1517).
| Characteristics | Suicidal Ideationb | p-value | |||||||
|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||
| PHQ-9 (+) EPDS (+) n = 105 | PHQ-9 (+) EPDS (-) n = 134 | PHQ-9 (-) EPDS (+) n = 29 | PHQ-9 (-) EPDS (-) n = 1249 | ||||||
|
|
|
||||||||
| n | % | n | % | n | % | n | % | ||
| Age (years)c | 27.4 ± 6.9 | 27.8 ± 6.0 | 27.3 ± 6.4 | 28.1 ± 6.2 | 0.56 | ||||
| Age (years) | |||||||||
| 18-20 | 11 | 10.5 | 7 | 5.2 | 1 | 3.4 | 72 | 5.8 | 0.56 |
| 20-29 | 60 | 57.1 | 80 | 59.7 | 17 | 58.6 | 699 | 56.0 | |
| 30-34 | 16 | 15.2 | 26 | 19.4 | 8 | 27.6 | 255 | 20.4 | |
| ≥35 | 18 | 17.1 | 21 | 15.7 | 3 | 10.3 | 223 | 17.9 | |
| Mestizo race/ethnicity | 73 | 69.5 | 95 | 70.9 | 19 | 65.5 | 955 | 76.5 | 0.06 |
| Education (years) | |||||||||
| ≤6 | 6 | 5.7 | 8 | 6.0 | 1 | 3.4 | 53 | 4.2 | 0.04 |
| 7-12 | 68 | 64.8 | 86 | 64.2 | 18 | 62.1 | 679 | 54.4 | |
| >12 | 30 | 28.6 | 39 | 29.1 | 10 | 34.5 | 514 | 41.2 | |
| Married or living with a partner | 83 | 79.0 | 102 | 76.1 | 24 | 82.8 | 1024 | 82.0 | 0.41 |
| Unemployed | 68 | 64.8 | 79 | 59.0 | 17 | 58.6 | 691 | 55.3 | 0.40 |
| How hard to pay for the very basics | |||||||||
| Very hard/hard | 33 | 31.4 | 36 | 26.9 | 6 | 20.7 | 211 | 16.9 | 0.0009 |
| Somewhat hard | 35 | 33.3 | 41 | 30.6 | 7 | 24.1 | 409 | 32.7 | |
| Not very hard | 37 | 35.2 | 57 | 42.5 | 16 | 55.2 | 628 | 50.3 | |
| Nulliparous | 48 | 45.7 | 68 | 50.7 | 15 | 51.7 | 634 | 50.8 | 0.80 |
| Gestational age at interview (weeks)c | 10.3 ± 3.4 | 10.1 ± 3.5 | 9.3 ± 3.3 | 9.7 ± 3.3 | 0.23 | ||||
| Unplanned pregnancy | 77 | 73.3 | 94 | 70.1 | 21 | 72.4 | 683 | 54.7 | <0.0001 |
| Any childhood abuse | 91 | 86.7 | 112 | 83.6 | 21 | 72.4 | 815 | 65.3 | <0.0001 |
| Any lifetime intimate partner violence | 96 | 91.4 | 94 | 70.1 | 23 | 79.3 | 684 | 54.8 | <0.0001 |
| PHQ-8 score c, d | 11.7 ± 6.0 | 9.6 ± 5.4 | 8.8 ± 6.5 | 7.0 ± 4.8 | <0.0001 | ||||
| EPDS score (9 item)c, e | 14.3 ± 4.6 | 10.5 ± 5.5 | 10.8 ± 4.5 | 5.4 ± 4.5 | <0.0001 | ||||
The Patient Health Questionnaire (PHQ-9) assesses suicidal ideation experienced by participants in the 14 days prior to evaluation. The Edinburgh Postnatal Depression Scale (EPDS) assesses suicidal ideation experienced by participants in the 7 days prior to evaluation.
PHQ-9 (+) EPDS (+): positive response to both item 9 of the PHQ-9 and item 10 of the EPDS; PHQ-9 (+) EPDS (-): positive response to only item 9 of the PHQ-9; PHQ-9 (-) EPDS (+): positive response to only item 10 of the EPDS; PHQ-9 (-) EPDS (-): negative responses to both item 9 of the PHQ-9 and item 10 of the EPDS.
mean ± standard deviation
PHQ-8 score was calculated by excluding item 9 from the PHQ-9.
EPDS score (9 item) was calculated by excluding item 10 from the EPDS total score.
In Table 3, the rate of concordance is 84.2% (n = 1,277) for the two suicidal ideation items (PHQ-9 item 9; EPDS item 10). In particular, 27 participants (1.8%) chose response categories of “more than half the days” or “nearly every day” on the PHQ-9, but “never” on the EPDS. In addition, 19 participants (1.3%) chose the response category “not at all,” but “sometimes” or “often” on the EPDS. The agreement (weighted Cohen's kappa) of the two suicidal ideation items was 0.42 (95% CI: 0.37, 0.48).
Table 3. Responses to Suicidal Ideation Items on the Patient Health Questionnaire (PHQ-9) and the Edinburgh Postnatal Depression Scale (EPDS)a (N = 1517).
| EPDS “The thought of harming myself has occurred to me” | PHQ-9 “Thoughts that you would be better off dead, or of hurting yourself in some way” | Total | |||
|---|---|---|---|---|---|
|
| |||||
| Not at all | Several days | More Than Half the Days | Nearly Every Day | ||
| Never | 1249 (82.33) | 107 (7.05) | 20 (1.32) | 7 (0.46) | 1383 (91.17) |
| Hardly Ever | 10 (0.66) | 13 (0.86) | 2 (0.13) | 1 (0.07) | 26 (1.71) |
| Sometimes | 18 (1.19) | 60 (3.96) | 11 (0.73) | 10 (0.66) | 99 (6.53) |
| Often | 1 (0.07) | 3 (0.20) | 1 (0.07) | 4 (0.26) | 9 (0.59) |
| Total | 1278 (84.25) | 183 (12.06) | 34 (2.24) | 22 (1.45) | 1517 |
The Patient Health Questionnaire (PHQ-9) assesses suicidal ideation experienced by participants in the 14 days prior to evaluation. The Edinburgh Postnatal Depression Scale (EPDS) assesses suicidal ideation experienced by participants in the 7 days prior to evaluation.
After combining response categories for the two suicidal ideation items, 1,354 participants (89.3%) had concordant classifications (Table 4). Of note, 105 participants (6.9%) had suicidal ideation on both the PHQ-9 and the EPDS, whereas 1,249 (82.3%) had no suicidal ideation on either scale. The agreement assessed by the Cohen's Kappa was 0.51 (95% CI: 0.44, 0.57). Given that 26 participants (1.71%) reported that they “hardly ever” thought of harming themselves (item 10 of the EPDS), we repeated analyses after classifying these subjects with those who reported “never” having thoughts of harming themselves. From these sensitivity analyses we noted that 1,348 participants (88.9%) had concordant classifications; and the agreement assessed by Cohen's Kappa was 0.46 (95% CI: 0.39, 0.53) (data not shown).
Table 4. Responses to Suicidal Ideation Items on the Patient Health Questionnaire (PHQ-9) and the Edinburgh Postnatal Depression Scale (EPDS)a (N = 1517).
| EPDS “The thought of harming myself has occurred to me” | PHQ-9 “Thoughts that you would be better off dead, or of hurting yourself in some way” | Total | |
|---|---|---|---|
|
| |||
| Suicidal ideationc | No suicidal ideationc | ||
| Suicidal ideationb | 105 | 29 | 134 |
| No suicidal ideationb | 134 | 1249 | 1383 |
| Total | 239 | 1278 | 1517 |
The Patient Health Questionnaire (PHQ-9) assesses suicidal ideation experienced by participants in the 14 days prior to evaluation. The Edinburgh Postnatal Depression Scale (EPDS) assesses suicidal ideation experienced by participants in the 7 days prior to evaluation.
Participants who gave a response of “yes, quite often,” “sometimes,” or “hardly ever” were categorized as “yes,” but categorized as “no” when endorsing the response category “never.”
Participants who gave a response of “several days,” “more than half the days,” or “nearly every day” were categorized as “yes,” but categorized as “no” when endorsing the response category “not at all.”
Overall, based on item 9 of the PHQ-9, 15.8% (n = 239) of participants reported experiencing suicidal ideation in the 14 days prior to evaluation. A total of 134 (8.8%) participants had suicidal ideation over the past 7 days assessed by item 10 of the EPDS. Among participants who screened positive for item 9 of the PHQ-9, 76.6% reported that they were bothered by the thoughts of suicidal ideation for “several days,” 14.2% for “more than half the days,” and 9.2% for “nearly every day.” Among those who screened positive for item 10 of the EPDS, 6.7% reported that thoughts of harming themselves had “hardly ever” occurred, 73.9% for “sometimes,” and 19.4% for “quite often.”
We examined the co-occurrence of antepartum depressive symptoms with suicidal ideation. For participants with suicidal ideation, mean scores were significantly higher than those without suicidal ideation (all p < 0.0001) on both scales. For participants who reported suicidal ideation, mean scores (including suicidal ideation items) were 11.8 on the PHQ-9 and 15.5 on the EPDS. For participants who did not report suicidal ideation, mean scores were 7.0 on the PHQ-9 and 5.9 on the EPDS.
We evaluated the trends of the proportions of suicidal ideation for each score (included/excluded suicidal ideation items) of the PHQ-9 and the EPDS. The distribution of participants endorsing suicidal ideation in relation to PHQ-9 and EPDS scores that exclude suicidal ideation items are shown in Figure 2 and Figure 3. For both scales, results of the chi-square tests for trend indicated that with the increase of the total scores, the proportions of participants having suicidal ideation were also increased (both p < 0.0001). For the PHQ-8, among participants with PHQ-8 score ≥ 20, the lowest proportion of suicidal ideation was 42% with the score of 20 (Figure 2). For the EPDS, among participants with EPDS score (9 item) ≥ 16, the lowest proportion of suicidal ideation was 14% with the score of 17 and 20 (Figure 3).
Figure 2. Distribution of Suicidal Ideation in Relation to the Patient Health Questionnaire-8 (PHQ-8)*.
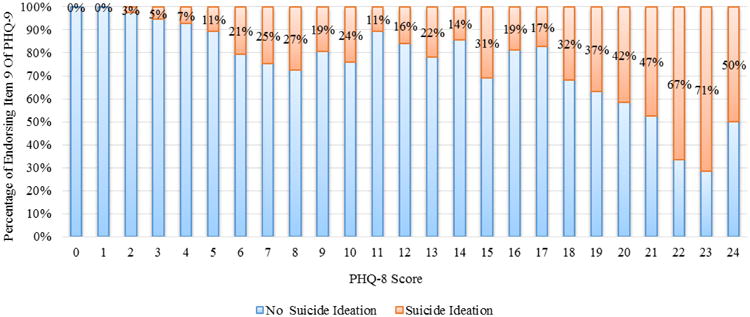
*PHQ-8 score was calculated by excluding item 9 from the PHQ-9.
Figure 3. Distribution of Suicidal Ideation in Relation to the Edinburgh Postnatal Depression Scale (EPDS) Score (9 item)*.
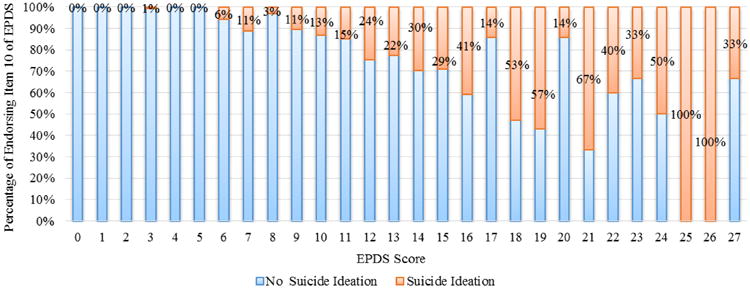
*EPDS score (9 item) was calculated by excluding item 10 from the EPDS total score.
Based on the PHQ-9, among participants with suicidal ideation, 122 participants (51.0%) had “moderate to severe” depressive symptoms (PHQ-9 score ≥ 10). Participants who had “moderate to severe” depressive symptoms had 3.07 times the odds (95% CI: 2.31, 4.08) of endorsing item 9 compared with those participants who had “minimum to mild” depressive symptoms (PHQ-9 score < 10). According to the EPDS, among those patients with suicidal ideation, 117 participants (87.3%) had “increased and marked risk” of depression (EPDS score ≥ 10). “Increased and marked risk” of depression was associated with a 24-fold increased odds (95% CI: 14.28, 40.74) of endorsing item 10 of the EPDS compared with “normal to slightly increased risk” of depression (EPDS score < 10).
Discussion
To our knowledge, this is the first study that compares item 9 of the PHQ-9 and item 10 of the EPDS for screening suicidal ideation among pregnant women. Overall, among pregnant Peruvian women, the concordance rate of these two items was high (84.2%). However, evaluated by the Cohen's kappa, the agreement was moderate (0.42). Among this population, the prevalence of suicidal ideation assessed by the PHQ-9 and the EPDS was 15.8% and 8.8%, respectively. For both scales, participants with suicidal ideation had higher mean scores for depressive symptoms. Additionally, with the increase of total scores, the proportions of participants having suicidal ideation were also increased. Based on the PHQ-9, 51% of participants with suicidal ideation had “moderate to severe” depressive symptoms (PHQ-9 ≥ 10). On the basis of the EPDS, the majority of participants (87.3%) who had suicidal ideation experienced “increased and marked risk” of depression (EPDS ≥ 10).
The two suicidal ideation items have a high concordance rate, but a moderate agreement based on the Cohen's Kappa. Compared with the EPDS, the PHQ-9 identifies more participants with suicidal ideation (15.8% vs. 8.8%). This discrepancy may be explained by the differences in the duration of reporting periods and wording of the two items. The PHQ-9 assesses suicidal ideation and depressive symptoms experienced by participants in the past 14 days, whereas the EPDS assesses suicidal ideation and depressive symptoms experienced by participants in the past 7 days. Item 9 of the PHQ-9 inquires about both “passive” (thoughts that you would be better off dead) and “active” (thoughts of hurting yourself in some way) thoughts for suicide, whereas item 10 of the EPDS only asks about the “active” thoughts of self-harm, which might not be limited to the construct of suicidality (Pope et al. 2013; Razykov et al. 2013b; Yawn et al. 2009). Several studies found that most of the responses to item 9 of the PHQ-9 appeared to endorse the passive thoughts of “being better off dead.” (Corson et al. 2004; Dube et al. 2010; Kroenke et al. 2010; Razykov et al. 2013a; Walker et al. 2011) Simon et al. (Simon et al. 2013) found that each higher response to item 9 of the PHQ-9 was associated with a stepwise increase in the cumulative risk of suicide attempt and suicide death over the following year (0.4% among outpatients reporting thoughts of death or self-harm “not at all” to 4% among those reporting “nearly every day”). To our best knowledge, no analogous data for the EPDS has been reported. Future studies should determine the appropriate duration of reporting period for suicidal ideation screening among pregnant women, evaluate the individuals who report thoughts of self-harm contemplating self-harm with lethal intent (Pope et al. 2013), and assess the percentage of individuals with positive responses to the two suicidal ideation items at high risk of planning and attempting suicide.
In a study of 481 women receiving postpartum care in Rochester, Minnesota, Yawn et al. (Yawn et al. 2009) reported that the prevalence estimates of suicidal ideation assessed by the PHQ-9 and the EPDS items was 8.8% and 7.3%, respectively. They also reported a very high concordance (93.8%) in the study population. In our study of Peruvian women receiving antepartum care, we noted somewhat higher prevalence estimates of suicidal ideation (the PHQ-9: 15.8%; the EPDS: 8.8%). In addition, a slightly lower degree of concordance in our study population (84.2%) was observed. Across these two studies, differences may be attributable to timing of suicidal assessment and possibly cultural and ethnic differences of the populations studied.
Among pregnant women, depending on screening instruments used, the prevalence of suicidal ideation ranges from 2.7% to 14.6% (Appleby 1991; Evans et al. 2001; Gausia et al. 2009; Gavin et al. 2011; Lindahl et al. 2005; Luoma et al. 2001; O'Connor et al. 2002). In the present study, the high prevalence of mood disorders and psychosocial stressors in Peru (e.g., antenatal depression, childhood abuse, and intimate partner violence) may account for the high prevalence of suicidal ideation (Cripe et al. 2010; Farber et al. 1996; Gavin et al. 2011; Lindahl et al. 2005; Perales et al. 2009; WHO 2005). Of note, Devries et al. (Devries et al. 2011) found that intimate partner violence was a consistent risk factor for suicide behaviors even after adjusting for probable common mental disorders. Future research on suicidality should carefully consider the social determinants of self-injurious behavior and the underlying psychological factors that may pose a continuous risk of suicide (Olfson et al. 2014), and explore the potential mechanisms for the association between traumatic experiences and suicidal behaviors.
During the perinatal period, the risk of suicide ideation is significantly higher among depressed women (Lindahl et al. 2005). In the current study, as the total scores from the PHQ-9 and the EPDS increased, we observed consistently increasing trends of the proportions of women endorsing suicidal ideation. Similar to previous studies (Gausia et al. 2009; Gavin et al. 2011; Harris and Barraclough 1997; Lindahl et al. 2005; Nock et al. 2012), we also observed a strong association between antepartum depressive symptoms and suicidal ideation. However, the results from the World Mental Health Surveys (Nock et al. 2012) reveal that only a small proportion of individuals (16.6%) with suicidal ideation have diagnosable depression. In the current study, assessed by the PHQ-9, 49% of participants who screened positive for suicidal ideation had the PHQ-9 score ≤ 10, indicating negative screening results for depressive symptoms. Participants with low PHQ-9 scores (e.g., 3, 4, and 5) still endorsed suicidal ideation (i.e., responded positively to item 9 of the PHQ-9). Clearly, depressive symptoms are highly associated with suicidal ideation; however, only a proportion of participants endorsing suicidal ideation experience the co-occurrence of depressive symptoms. The occurrence of suicidal ideation cannot completely be explained by the occurrence of depressive symptoms. In prenatal care clinics, considering the distinct nature between suicidal ideation and depression, specific attention should be paid to suicidal ideation (Lindahl et al. 2005). In addition, most previous studies of suicidality in pregnancy were limited to detecting suicidal behaviors in the presence of depression, which may have resulted in an artificially low prevalence of suicidal ideation (Lindahl et al. 2005). Given the adverse consequences for both maternal and fetal well-being during the prenatal period (Newport et al. 2007), screening for suicidal ideation is needed for women both with and without depression in prenatal care clinics.
Our study has several limitations. First, we do not have data from a structured diagnostic interview to confirm the diagnosis of depression and further establish the types of depression (e.g., unipolar or bipolar depression). Second, the PHQ-9 and the EPDS include only a single item asking about suicidal ideation to assess suicidality. For more precise risk assessment during pregnancy, other dimensions of suicidal behaviors and the context in which suicidal ideation occurs should also be examined. Third, among participants endorsing suicidal ideation in the current study, we were not able to identify for those at high risk of developing a suicide plan and/or attempting suicide. Longitudinal follow-up studies are warranted for specific inquiries into maternal suicidal behaviors including development of a plan and suicide attempt. Finally, because the two instruments were not administered in random order (Weobong et al. 2009), the order effect cannot be excluded.
Despite these limitations, this is the first study to carefully examine the concordance and agreement between the two suicidal ideation items from the PHQ-9 and the EPDS among pregnant women. Relative strengths of our study included the large sample size and suicidal ideation screening for all participants as opposed to only participants with depression. We have confirmed that only a proportion (51%) of participants endorsing suicidal ideation report the co-occurrence of depressive symptoms assessed by the PHQ-9. Furthermore, this study provided updated epidemiologic data for suicidality in Peru, laying the foundation for developing future mental health policy and health services programs for pregnant and reproductive aged women.
In conclusion, item 9 of the PHQ-9 and item 10 of the EPDS have high concordance (84.2%) but moderate agreement (Cohen's kappa = 0.42). Compared with item 10 of the EPDS, item 9 of the PHQ-9 identifies more participants with suicidal ideation. This discrepancy may be explained by the differences in the duration of reporting periods and wording of these two items. Item 9 of the PHQ-9 addresses suicidal ideation with both “passive” and “active” thoughts. However, item 10 of the EPDS only includes the active thoughts of self-harm, which can exist independently of suicidal ideation (Pope et al. 2013). Future studies are needed to identify additional predictors of antepartum suicidality, determine the appropriate duration of reporting period for suicidal ideation screening, evaluate the individuals who report thoughts of self-harm contemplating self-harm with lethal intent, and assess the percentage of individuals with positive responses to the two suicidal ideation items at high risk of planning and attempting suicide.
Acknowledgments
This research was supported by an award from the National Institutes of Health (NIH), the Eunice Kennedy Shriver Institute of Child Health and Human Development (R01-HD-059835). The NIH had no further role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication. The authors wish to thank the dedicated staff members of Asociacion Civil Proyectos en Salud (PROESA), Peru and Instituto Especializado Materno Perinatal, Peru for their expert technical assistance with this research. The authors would like to thank Kathy Brenner for her help with revising this manuscript.
Footnotes
Conflict of Interest: No potential conflicts of interest were disclosed.
References
- Appleby L. Suicide during pregnancy and in the first postnatal year. Brit Med J. 1991:137–140. doi: 10.1136/bmj.302.6769.137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beck AT, Ward C, Mendelson M. Beck depression inventory (BDI) Arch Gen Psychiatry. 1961;4:561–571. doi: 10.1001/archpsyc.1961.01710120031004. [DOI] [PubMed] [Google Scholar]
- Bennett MHA, Einarson A, Taddio A, Koren G, Einarson TR. Depression during pregnancy. Clin Drug Invest. 2004;24:157–179. doi: 10.2165/00044011-200424030-00004. [DOI] [PubMed] [Google Scholar]
- Bowen A, Stewart N, Baetz M, Muhajarine N. Antenatal depression in socially high-risk women in Canada. J Epidemiol Commun H. 2009;63:414–416. doi: 10.1136/jech.2008.078832. [DOI] [PubMed] [Google Scholar]
- Brown GK. A review of suicide assessment measures for intervention research with adults and older adults. [Accessed June 26, 2014];2001 http://ruralccp.org/lyra-data/storage/asset/brown-nd-27cb.pdf.
- Chang J, Berg CJ, Herndon J, Saltzman LE. Homicide: a leading cause of injury deaths among pregnant and postpartum women in the United States, 1991-1999. Am J Public Health. 2005;95:471. doi: 10.2105/AJPH.2003.029868. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chaudron LH, Klein M, Remington P, Palta M, Allen C, Essex M. Predictors, prodromes and incidence of postpartum depression. J Psychosom Obstet Gynaecol. 2001;22:103–112. doi: 10.3109/01674820109049960. [DOI] [PubMed] [Google Scholar]
- Copersino ML, Jones H, Tuten M, Svikis D. Suicidal ideation among drug-dependent treatment-seeking inner-city pregnant women. J Maint Addict. 2008;3:53–64. doi: 10.1300/J126v03n02_07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Corson K, Gerrity MS, Dobscha SK. Screening for depression and suicidality in a VA primary care setting: 2 items are better than 1 item. Am J Manag Care. 2004;10:839–845. [PubMed] [Google Scholar]
- Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry. 1987;150:782–786. doi: 10.1192/bjp.150.6.782. [DOI] [PubMed] [Google Scholar]
- Cripe SM, Sanchez S, Lam N, Sanchez E, Ojeda N, Tacuri S, Segura C, Williams MA. Depressive symptoms and migraine comorbidity among pregnant Peruvian women. J Affect Disord. 2010;122:149–153. doi: 10.1016/j.jad.2009.07.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Devries K, Watts C, Yoshihama M, et al. Violence against women is strongly associated with suicide attempts: evidence from the WHO multi-country study on women's health and domestic violence against women. Soc Sci Med. 2011;73:79–86. doi: 10.1016/j.socscimed.2011.05.006. [DOI] [PubMed] [Google Scholar]
- Dube P, Kurt K, Bair MJ, Theobald D, Williams LS. The P4 screener: evaluation of a brief measure for assessing potential suicide risk in 2 randomized effectiveness trials of primary care and oncology patients. Prim Care Companion J Clin Psychiatry. 2010;12 doi: 10.4088/PCC.10m00978blu. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eggleston AM, Calhoun PS, Svikis DS, Tuten M, Chisolm MS, Jones HE. Suicidality, aggression, and other treatment considerations among pregnant, substance-dependent women with posttraumatic stress disorder. Compr Psychiat. 2009;50:415–423. doi: 10.1016/j.comppsych.2008.11.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Evans J, Heron J, Francomb H, Oke S, Golding J. Cohort study of depressed mood during pregnancy and after childbirth. Brit Med J. 2001;323:257–260. doi: 10.1136/bmj.323.7307.257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Farber EW, Herbert SE, Reviere SL. Childhood abuse and suicidality in obstetrics patients in a hospital-based urban prenatal clinic. Gen Hosp Psychiat. 1996;18:56–60. doi: 10.1016/0163-8343(95)00098-4. [DOI] [PubMed] [Google Scholar]
- Ferrari AJ, Charlson FJ, Norman RE, Flaxman AD, Patten SB, Vos T, Whiteford HA. The epidemiological modelling of major depressive disorder: application for the Global Burden of Disease Study 2010. PloS one. 2013;8:e69637. doi: 10.1371/journal.pone.0069637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flynn HA, Sexton M, Ratliff S, Porter K, Zivin K. Comparative performance of the Edinburgh Postnatal Depression Scale and the Patient Health Questionnaire-9 in pregnant and postpartum women seeking psychiatric services. Psychiatry Res. 2011;187:130–134. doi: 10.1016/j.psychres.2010.10.022. [DOI] [PubMed] [Google Scholar]
- Gausia K, Fisher C, Ali M, Oosthuizen J. Antenatal depression and suicidal ideation among rural Bangladeshi women: a community-based study. Arch Womens Ment Health. 2009;12:351–358. doi: 10.1007/s00737-009-0080-7. [DOI] [PubMed] [Google Scholar]
- Gavin AR, Tabb KM, Melville JL, Guo Y, Katon W. Prevalence and correlates of suicidal ideation during pregnancy. Arch Womens Ment Health. 2011;14:239–246. doi: 10.1007/s00737-011-0207-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23:56. doi: 10.1136/jnnp.23.1.56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harris EC, Barraclough B. Suicide as an outcome for mental disorders. A meta-analysis. Brit J Psychiat. 1997;170:205–228. doi: 10.1192/bjp.170.3.205. [DOI] [PubMed] [Google Scholar]
- Howard LM, Flach C, Mehay A, Sharp D, Tylee A. The prevalence of suicidal ideation identified by the Edinburgh Postnatal Depression Scale in postpartum women in primary care: findings from the RESPOND trial. BMC pregnancy and childbirth. 2011;11:57. doi: 10.1186/1471-2393-11-57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Joiner TE, Rudd MD, Rouleau MR, Wagner KD. Parameters of suicidal crises vary as a function of previous suicide attempts in youth inpatients. J Am Acad Child Adolesc Psychiatry. 2000;39:876–880. doi: 10.1097/00004583-200007000-00016. [DOI] [PubMed] [Google Scholar]
- Kroenke K, Spitzer RL, Williams JB, Löwe B. The patient health questionnaire somatic, anxiety, and depressive symptom scales: a systematic review. Gen Hosp Psychiat. 2010;32:345–359. doi: 10.1016/j.genhosppsych.2010.03.006. [DOI] [PubMed] [Google Scholar]
- Kroenke K, Spitzer RL, Williams JBW. The PHQ-9. J Gen Intern Med. 2001;16:606–613. doi: 10.1046/j.1525-1497.2001.016009606.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lindahl V, Pearson JL, Colpe L. Prevalence of suicidality during pregnancy and the postpartum. Arch Womens Ment Health. 2005;8:77–87. doi: 10.1007/s00737-005-0080-1. [DOI] [PubMed] [Google Scholar]
- Luoma I, Tamminen T, Kaukonen P, Laippala P, Puura K, Salmelin R, Almqvist F. Longitudinal study of maternal depressive symptoms and child well-being. J Am Acad Child Adolesc Psychiatry. 2001;40:1367–1374. doi: 10.1097/00004583-200112000-00006. [DOI] [PubMed] [Google Scholar]
- Newport DJ, Levey L, Pennell P, Ragan K, Stowe ZN. Suicidal ideation in pregnancy: assessment and clinical implications. Arch Womens Ment Health. 2007;10:181–187. doi: 10.1007/s00737-007-0192-x. [DOI] [PubMed] [Google Scholar]
- Nock MK, Borges G, Ono Y. Suicide: global perspectives from the who world mental health surveys. Cambridge University Press; Cambridge, United Kingdom: 2012. [Google Scholar]
- O'Connor TG, Heron J, Glover V. Antenatal anxiety predicts child behavioral/emotional problems independently of postnatal depression. J Am Acad Child Adolesc Psychiatry. 2002;41:1470–1477. doi: 10.1097/00004583-200212000-00019. [DOI] [PubMed] [Google Scholar]
- Olfson M, Marcus SC, Bridge JA. Focusing suicide prevention on periods of high risk. J Am Med Assoc. 2014;311:1107–1108. doi: 10.1001/jama.2014.501. [DOI] [PubMed] [Google Scholar]
- Paris R, Bolton RE, Weinberg MK. Postpartum depression, suicidality, and mother-infant interactions. Arch Womens Ment Health. 2009;12:309–321. doi: 10.1007/s00737-009-0105-2. [DOI] [PubMed] [Google Scholar]
- Perales MT, Cripe SM, Lam N, Sanchez SE, Sanchez E, Williams MA. Prevalence, types, and pattern of intimate partner violence among pregnant women in Lima, Peru. Violence Against Wom. 2009;15:224–250. doi: 10.1177/1077801208329387. [DOI] [PubMed] [Google Scholar]
- Pope CJ, Xie B, Sharma V, Campbell MK. A prospective study of thoughts of self-harm and suicidal ideation during the postpartum period in women with mood disorders. Arch Womens Ment Health. 2013;16:483–488. doi: 10.1007/s00737-013-0370-y. [DOI] [PubMed] [Google Scholar]
- Razykov I, Hudson M, Baron M, Thombs BD. Utility of the Patient Health Questionnaire-9 to assess suicide risk in patients with systemic sclerosis. Arthritis Care Res. 2013;65:753–758. doi: 10.1002/acr.21894. [DOI] [PubMed] [Google Scholar]
- Shadigian EM, Bauer ST. Pregnancy-associated death: a qualitative systematic review of homicide and suicide. Obstet Gynecol Surv. 2005;60:183–190. doi: 10.1097/01.ogx.0000155967.72418.6b. [DOI] [PubMed] [Google Scholar]
- Simon GE, Rutter CM, Peterson D, Oliver M, Whiteside U, Operskalski B, Ludman EJ. Does response on the PHQ-9 Depression Questionnaire predict subsequent suicide attempt or suicide death? Psych Serv. 2013;64:1195–1202. doi: 10.1176/appi.ps.201200587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. J Am Med Assoc. 1999;282:1737–1744. doi: 10.1001/jama.282.18.1737. [DOI] [PubMed] [Google Scholar]
- Stallones L, Leff M, Canetto SS, Garrett CJ, Mendelson B. Suicidal ideation among low-income women on family assistance programs. Women Health. 2007;45:65–83. doi: 10.1300/J013v45n04_04. [DOI] [PubMed] [Google Scholar]
- Tadros G, Jolley D. The stigma of suicide. The British Journal of Psychiatry. 2001;179:178. doi: 10.1192/bjp.179.2.178. [DOI] [PubMed] [Google Scholar]
- Walker J, Hansen CH, Butcher I, Sharma N, Wall L, Murray G, Sharpe M. Thoughts of death and suicide reported by cancer patients who endorsed the “suicidal thoughts” item of the PHQ-9 during routine screening for depression. Psychosomatics. 2011;52:424–427. doi: 10.1016/j.psym.2011.02.003. [DOI] [PubMed] [Google Scholar]
- Weobong B, Akpalu B, Doku V, Owusu-Agyei S, Hurt L, Kirkwood B, Prince M. The comparative validity of screening scales for postnatal common mental disorder in Kintampo, Ghana. J Affect Disord. 2009;113:109–117. doi: 10.1016/j.jad.2008.05.009. [DOI] [PubMed] [Google Scholar]
- World Health Organization. WHO multi-country study on women's health and domestic violence against women: summary report of initial results on prevalence, health outcomes and women's responses. [Accessed June 26, 2014];2005 http://whqlibdoc.who.int/publications/2005/924159358X_eng.pdf?ua=1.
- Yawn BP, Pace W, Wollan PC, Bertram S, Kurland M, Graham D, Dietrich A. Concordance of Edinburgh Postnatal Depression Scale (EPDS) and Patient Health Questionnaire (PHQ-9) to assess increased risk of depression among postpartum women. J Am Board Fam Med. 2009;22:483–491. doi: 10.3122/jabfm.2009.05.080155. [DOI] [PubMed] [Google Scholar]