

Abstract
Previous studies showed that psychiatric disorders such as major depression, bipolar disorders, and alcohol misuse are associated with an increased risk of ischemic stroke. However, the link between psychiatric disorders and stroke in the young population is rarely investigated.
Using the Taiwan National Health Insurance Research Database, 2063 young adults aged between 18 and 45 years with ischemic stroke and 8252 age- and sex-matched controls were enrolled in our study between 1998 and 2011. Participants who had preexisting psychiatric disorders were identified.
After adjusting for preexisting physical disorders and demographic data, patients with ischemic stroke had an increased risk of having preexisting psychiatric disorders, including bipolar disorder (odds ratio [OR]: 2.23, 95% confidence interval [CI]: 1.06∼4.67), unipolar depression (OR: 2.15, 95% CI: 1.62∼2.86), anxiety disorders (OR: 2.63, 95% CI: 1.87∼3.69), and alcohol use disorders (OR: 2.86, 95% CI: 1.79∼4.57). Young ischemic stroke (age ≥30 years) was related to the risk of preexisting unipolar depression (OR: 1.49, 95% CI: 1.05∼2.11), anxiety disorders (OR: 1.99, 95% CI: 1.33∼2.97), and alcohol use disorders (OR: 2.54, 95% CI: 1.55∼4.14); very young stroke (age <30 years) was only associated with the risk of preexisting unipolar depression (OR: 4.15, 95% CI: 1.47∼11.72).
Patients who had experienced ischemic stroke at age younger than 45 years had a higher risk of having pre-existing bipolar disorder, unipolar depression, anxiety disorders, and alcohol use disorders than those who did not after adjusting for demographic data and stroke-related medical comorbidities.
Ischemic strokes in adults younger than 45 years of age were regarded as a relatively uncommon event in the proportion of <5% of all ischemic strokes.1 However, other epidemiological studies have shown a higher proportion of approximately 10% of all ischemic strokes occurring in young adults.2,3 Compared with stroke in the elderly, stroke in the young adult resulted in a disproportionately great personal, familial, and socioeconomic impacts and consequences by leaving patients disabled before their most productive years.4,5 The most significantly established risk factors for young ischemic stroke included hypertension, dyslipidemia, diabetes mellitus, and smoking.5–7
The association between psychiatric disorders and stroke has gained the clinical and scientific attention in the past decade.8–10 For example, Tsai et al11 followed 80,569 patients with schizophrenia for 5 years, and revealed that those with schizophrenia were 1.13 times more likely to have a stroke (95% confidence interval [CI]: 1.05∼1.22). Li et al12 followed 1003 patients with major depression and 4012 controls for 9 years and found that patients with major depression had a higher risk of stroke (odds ratio [OR]: 1.55, 95% CI: 1.08∼2.211) than the control group during the follow-up. Dong et al8 reported a significant positive association between depression and subsequent risk of stroke (relative risk [RR]: 1.34, 95% CI: 1.17∼1.54). Prieto et al's10 meta-analysis study composed of 27,092 bipolar patients showed that the risk of stroke in bipolar disorder was significantly increased (RR: 1.74, 95% CI 1.29∼2.35). The First National Health and Nutrition Examination Survey in United States demonstrated that more anxiety symptoms at baseline were associated with increased risk of incident stroke (hazard ratio [HR]: 1.14, 95% CI: 1.03∼1.25).9 Following 19,544 men aged 40 to 59 years for 11 years, Iso et al13 determined that alcohol consumption was positively associated with the risk of stroke with a 68% excess risk among drinkers of ≥450 g ethanol per week compared with occasional drinkers. However, stroke in the above studies occurred in the late mid-life or in old age but not in the younger age groups. The association between young stroke and psychiatric disorders was less investigated and still unclear.
In our study, using the Taiwan National Health Insurance Research Database (NHIRD) with a large sample size and a retrospective study design, we investigated the association between the young ischemic stroke and the risk of preexisting psychiatric disorders, including schizophrenia, bipolar disorder, major depression, anxiety disorders, and alcohol use disorder.
METHODS
Data Source
Taiwan's National Health Insurance (NHI) is a mandatory universal health insurance program that was implemented in 1995 and offers comprehensive medical care coverage to all Taiwanese residents. The National Health Research Institute (NHRI) is in charge of the entire insurance claims database, namely the NHIRD, which consists of healthcare data from >97% of the entire Taiwan population (http://www.nhi.gov.tw/). The NHRI audits and releases the NHIRD for scientific and study purposes. Individual medical records included in the NHIRD are anonymous to protect patient privacy. Comprehensive information on insured individuals is included in the database, including demographic data, dates of clinical visits, disease diagnoses, and evaluation procedures. The diagnostic codes used were based on the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM). The NHIRD has been used extensively in many epidemiologic studies in Taiwan.12,14–17
Inclusion Criteria for Individuals With Young Ischemic Stroke and the Control Group
Adult subjects aged between 18 and 45 years were identified as having a diagnosis of ischemic stroke (ICD-9-CM codes: 433, 434, 435) given by board-certificated neurologists, neurosurgeons, internal medicine physicians, and emergency room physicians after brain image examinations (brain computed tomography or brain magnetic resonance imaging) between January 1, 1998 and December 31, 2011, were enrolled as the stroke cohort. The time of ischemic stroke diagnosis was defined as the time of ischemic stroke event and the time of enrollment. The age-, sex-, and time of enrollment-matched (1:4) control cohort was randomly identified after eliminating the study subjects and those who had been given a diagnosis of any stroke (ICD-9-CM code: 430 ∼ 438) at any time. Preexisting psychiatric disorders before the ischemic stroke or the enrollment given by psychiatrists were identified, including schizophrenia (ICD-9-CM code: 295), bipolar disorder (ICD-9-CM codes: 296.0, 296.1, 296.4–296.7, 296.80, 296.81, 296.89), unipolar depression (ICD-9-CM codes: 296.2, 296.3, 300.4, 311), obsessive-compulsive disorder (ICD-9-CM code: 300.3), anxiety disorders (ICD-9-CM codes: 300 except 300.3, 300.4), alcohol use disorders (ICD-9-CM codes: 291, 303, 305.0), and substance use disorders (ICD-9-CM codes: 292, 304, 305.1 ∼ 305.9). Preexisting stroke-related physical comorbidities, including hypertension, dyslipidemia, diabetes mellitus, obesity, chronic renal diseases, ischemic heart diseases, and arrhythmia, were also assessed in our study. All medical and psychiatric diagnoses were given at least twice by corresponding physicians to achieve improved diagnostic validity. Level of urbanization (level 1 to level 5; level 1: most urbanized region; level 5: least urbanized region) was also assessed for our study.18 This study was approved by the Taipei Veterans General Hospital institutional review board.
Statistical Analysis
For between-group comparisons, the independent t test was used for continuous variables and Pearson χ2 test for nominal variables, where appropriate. The logistic regression analysis was used to investigate the odds ratio (OR) with a 95% CI of each preexisting psychiatric disorder among subjects with ischemic stroke and the control group. Two regression models were performed: the first model adjusted for demographic data and physical comorbidities, and the second model adjusted for demographic data, physical comorbidities, and other psychiatric comorbidities. To clarify the impact of psychiatric disorder in the different age groups of young stroke, we investigated the preexisting psychiatric disorders with the risk of very young (<30 years) and young (30∼45 years) ischemic stroke in our study. A 2-tailed P value of <0.05 was considered statistically significant. All data processing and statistical analyses were performed with Statistical Package for Social Science (SPSS) version 17 software (SPSS Inc.) and Statistical Analysis Software (SAS) version 9.1 (SAS Institute, Cary, NC).
RESULTS
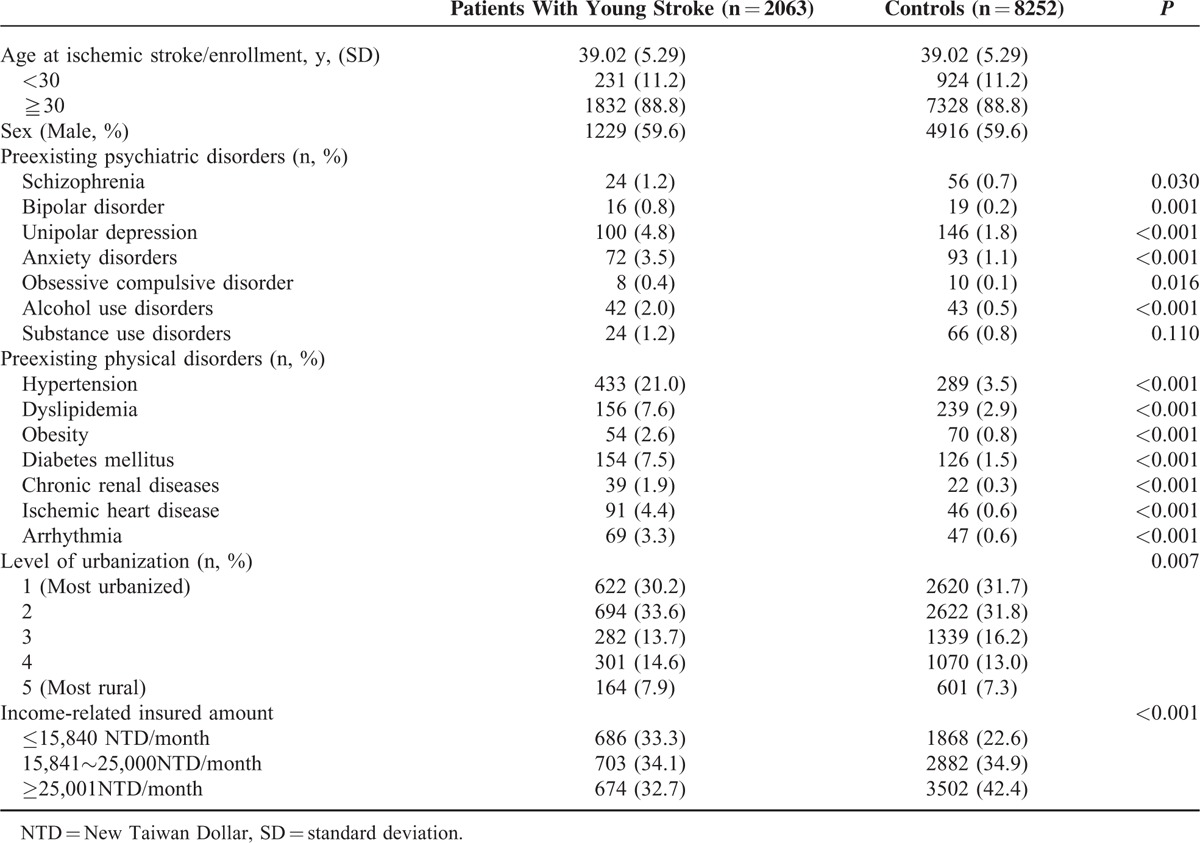
In all, 2063 young adults aged 39.02 ± 5.29 years with ischemic stroke and 8252 age- and sex-matched controls were enrolled in our study. Among young stroke patients, 231 (11.2%) had ischemic stroke before age of 30 years, and 1832 (88.8%) did at age of 30 years and older (Table 1). Subjects with ischemic stroke had an elevated prevalence of preexisting psychiatric disorders, including schizophrenia (1.2% vs 0.7%, P = 0.030), bipolar disorder (0.8% vs 0.2%, P = 0.001), unipolar depression (4.8% vs 1.8%, P < 0.001), obsessive-compulsive disorder (0.4% vs 0.1%, P = 0.016), anxiety disorders (3.5% vs 1.1%, P < 0.001), and alcohol use disorders (2.0% vs 0.5%, P < 0.001), compared with the controls (Table 1). Also, preexisting physical comorbidities, including hypertension (21.0% vs 3.5%, P < 0.001), dyslipidemia (7.6% vs 2.9%, P < 0.001), obesity (2.6% vs 0.8%, P < 0.001), diabetes mellitus (7.5% vs 1.5%, P < 0.001), chronic renal diseases (1.9% vs 0.3%, P < 0.001), ischemic heart diseases (4.4% vs 0.6%, P < 0.001), and arrhythmia (3.3% vs 0.6%, P < 0.001), were higher in the subjects with ischemic stroke than in those without stroke (Table 1).
TABLE 1.
Demographic Data of Patients With Young Ischemic Stroke and the Control Group
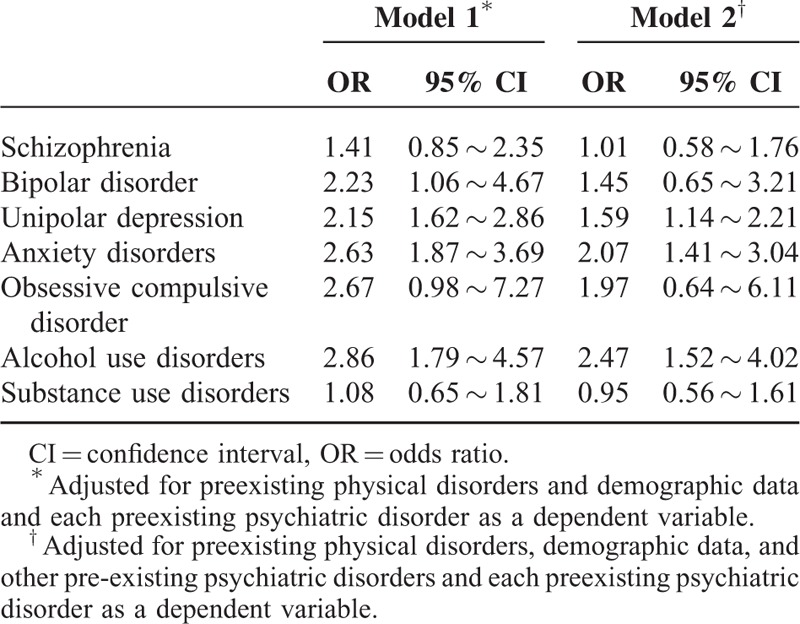
Logistic regression analysis model 1 with an adjustment of preexisting physical disorders and demographic data demonstrated that patients with ischemic stroke had an increased risk of having preexisting psychiatric disorders, including bipolar disorder (OR: 2.23, 95% CI: 1.06∼4.67), unipolar depression (OR: 2.15, 95% CI: 1.62∼2.86), anxiety disorders (OR: 2.63, 95% CI: 1.87∼3.69), and alcohol use disorders (OR: 2.86, 95% CI: 1.79∼4.57), compared with the control group (Table 2). Model 2 further adjusting for other preexisting psychiatric comorbidities showed that patients with ischemic stroke were prone to having preexisting psychiatric disorders, including unipolar depression (OR: 1.59, 95% CI: 1.14∼2.21), anxiety disorders (OR: 2.07, 95% CI: 1.41∼3.04), and alcohol use disorders (OR: 2.47, 95% CI: 1.52∼4.02) (Table 2).
TABLE 2.
Risk of Preexisting Psychiatric Disorders Among Patients With Young Ischemic Stroke and the Control Group
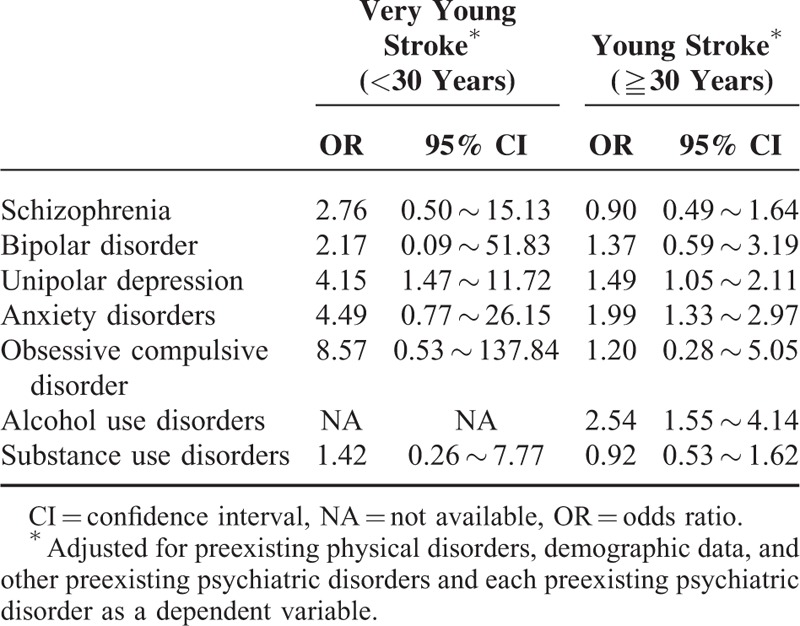
We investigated the association between the age (very young: <30 years and young: ≧30 years) of ischemic stroke and the risk of pre-existing psychiatric disorders. Young ischemic stroke was related to the risk of preexisting unipolar depression (OR: 1.49, 95% CI: 1.05∼2.11), anxiety disorders (OR: 1.99, 95% CI: 1.33∼2.97), and alcohol use disorders (OR: 2.54, 95% CI: 1.55∼4.14); very young stroke was only associated with the risk of preexisting unipolar depression (OR: 4.15, 95% CI: 1.47∼11.72) (Table 3).
TABLE 3.
Risk of Preexisting Psychiatric Disorders Among Patients With Young Ischemic Stroke and the Control Group Stratified by Age Onset of Stroke Group
DISCUSSION
The study results supported our study hypothesis that young adults younger than 45 years who experienced ischemic stroke had an around 1.5∼2.5 times elevated risk of having preexisting psychiatric disorders, including unipolar depression, anxiety disorders, and alcohol use disorders, than the control group after adjusting for demographic data and medical comorbidities. We also noted that patients with ischemic stroke at age <30 years were around 4 times more likely to have preexisting unipolar depression.
Young Ischemic Stroke and Unipolar Depression
Previous studies have shown the association between unipolar depression and the risk of ischemic stroke.8,12 Salaycik et al19 determined that depressive symptoms were associated with a 4-fold increased risk of ischemic stroke in midlife adults younger than 65 years but not in those aged 65 years and older. Seifert et al20 further confirmed that the relationship between depression and risk of ischemic stroke only occurred in the patients aged between 55 and 64 years but not in those aged ≧65 years. The studies regarding the risk of stroke among young depressed population younger than 45 years were still lacking. But, Salaycik et al's and Seifert et al's results may imply the different age-effect of depression in the risk of ischemic stroke.19–20 Our studies found that young ischemic stroke younger than 45 years was related to the elevated risk of having a preexisting unipolar depression.
Young Ischemic Stroke and Bipolar Disorder
Some studies established the association between bipolar disorder and ischemic stroke, although most of them were conducted in the midlife and elderly patients.10,21 However, studies specifically targeting the link between bipolar disorder and young stroke were lacking. Wu et al22 reported that bipolar patients with stroke were younger than those without stroke, although the stroke event still occurred at a mean age over 45 years.22 Another large-scale study showing the link between bipolar disorder and stroke (prevalence ratio 3.14, CI = 2.42∼4.06) had 46% of its bipolar group younger than age 40 (1873/4067 patients), but no stratified data were available.23 In our study, model 1 adjusting for demographic data and medical comorbidities, but not model 2 with an additional adjustment with other psychiatric comorbidities, showed a significant relationship between bipolar disorder and young ischemic stroke. It may indicate that the increased risk of young ischemic stroke among patients with bipolar disorder was indirectly via the effect of other psychiatric comorbidities, such as alcohol use disorder and anxiety disorders.
Young Ischemic Stroke and Anxiety Disorders
The National Health and Nutrition Examination Survey in United States demonstrated that more anxiety symptoms at baseline were associated with an elevated risk of incident stroke (HR: 1.14, 95% CI: 1.03∼1.25).9 However, the study population had a mean age of >45 years, and the study only demonstrated the link between stroke and anxiety symptom scores from a questionnaire rather than from a diagnosis of anxiety disorders.9 A population study showed the higher risk of stroke among patients with panic disorder (HR = 1.38, 95% CI 1.12∼1.71) with 42% of the study population under the age of 40, but stratified data was not available.24 The literature review determined that the link between anxiety disorders and young ischemic stroke has never been adequately investigated. In our study, we found that young patients who had an ischemic stroke had a higher risk of preexisting anxiety disorders than the control group.
Young Ischemic Stroke and Alcohol Use Disorders
Alcohol consumption was a known risk factor for young stroke in a dose-dependent association between the excessive amount of alcohol consumption and the risk of young stroke.13,25,26 Romelsjo et al27 further identified that binge-drinking increased the stroke likelihood compared with non-binge drinking. Compatible with previous findings, our study supported the association between alcohol use disorder and the risk of young ischemic stroke.
The Pathophysiology Linking Psychiatric Disorders With Risk of Young Ischemic Stroke
We proposed 2 hypotheses to explain the association between the psychiatric disorders and the risk of young ischemic stroke. First, some previous studies have shown that the risk factors of young ischemic stroke included hypertension, diabetes mellitus, dyslipidemia, obesity, and alcohol use disorders.28,29 The prevalence of those stroke-related disorders in the young population increased gradually in the last decades.29 Furthermore, a growing body of evidence also found the significant association between psychiatric disorders (ie, schizophrenia, bipolar disorder, unipolar depression, and anxiety disorders) and the stroke-related risk factors mentioned above.30–32 In our study, young patients with ischemic stroke had a higher prevalence of those stroke-related medical comorbidities, including hypertension, dyslipidemia, diabetes mellitus, and heart diseases, and psychiatric comorbidities, including unipolar depression, anxiety disorders, and alcohol use disorders, compared with those without ischemic stroke. Cox regression model also suggested an independent effect of psychiatric comorbidities (ie, unipolar depression, anxiety disorders, and alcohol use disorders) with the elevated risk of ischemic stroke in young adults. Second, previous studies suggested that the dysregulated inflammatory process and over-secreted proinflammatory cytokines, such as C-reactive protein (CRP), interleukin (IL)-6, and tumor necrosis factor (TNF)-α, were associated with the increased risk of ischemic stroke. Kaptoge et al33 found that CRP concentration was log-linearly correlated with ischemic stroke (risk ratio [RR]: 1.46, 95% CI: 1.32∼1.61). Cui et al34 reported that the polymorphisms of rs1800629 (G>A)(OR: 1.56, 95% CI: 1.09∼2.23) in the promoter region of the TNF-α gene were associated with an increased risk of developing ischemic stroke after adjusting for age, sex, hypertension, dyslipidemia, and diabetes. They also showed that the TNF-α level was positively associated with stroke-related risk factors (total cholesterol level and systolic blood pressure).34 Tong et al35 also reported that IL-6-572GC was an independent risk factor for developing ischemic stroke. Past studies have supported that psychiatric disorders were associated with long-term inflammation and altered proinflammatory cytokines. For example, 2 recent meta-analysis studies reported a significantly higher concentration of TNF-α and IL-6 in depressive subjects than in the controls.36,37 Kim et al38 found that bipolar patients had an increased level of TNF-α and IL-6 and a higher ratio of TNF-α/IL-4, IL-2/IL-4, and IFN-γ/IL-4 than controls. Vogelzangs et al39 reported the elevated levels of CRP among patients with a current anxiety disorder compared wiith controls. In our study, we supported an independent effect of several preexisting psychiatric disorders, including unipolar depression, anxiety disorders, and alcohol use disorder, with the risk of young ischemic stroke.
Some study limitations should be addressed. First, the prevalence of preexisting psychiatric disorders should be underestimated because only those who sought medical consultation and treatment would be included in our study. However, preexisting psychiatric disorders were diagnosed by board-certificated psychiatrists, yielding an improved diagnostic validity. Second, the medications for preexisting psychiatric disorders were not analyzed in our study because the medications would be very complicated during the follow-up and were difficultly adjusted in the regression model. Third, certain information, including life style, smoking, family history, and severity of psychiatric disorders, was not available in the NHIRD, so we cannot investigate their impact in our study. Further clinical studies would be required to overcome the above limitations and to elucidate the role of each factor on the risk of stroke among young population.
In conclusion, patients who developed ischemic stroke at age younger than 45 years had a higher risk of having pre-existing unipolar depression, anxiety disorders, and alcohol use disorder than those who did not after adjusting for demographic data and stroke-related medical comorbidities. Further studies may be required to elucidate the underlying pathophysiology between psychiatric disorders and the subsequent risk of ischemic stroke among young adults and to investigate whether the prompt intervention to psychiatric disorders may reduce the risk of young ischemic stroke.
Acknowledgments
We thank Mr I-Fan Hu for his friendship and support.
We thank Drs Yu-Chuan Chiu and Mu-Hong Chen, who designed the study, wrote the protocol and manuscripts, Drs Ya-Mei Bai and Tung-Ping Su, who assisted with the preparation and proof-reading of the manuscript, and Dr Tzeng-Ji Chen, who advised our group with statistical analysis.
Footnotes
Abbreviations: CRP = C-reactive protein, IL-6 = interleukin-6, NHIRD = National Health Insurance Research Database, TNF-α = tumor necrosis factor-α.
The study was supported by a grant from Taipei Veterans General Hospital (V103E10-001).
All authors declare no conflict of interest.
REFERENCES
- 1.Kristensen B, Malm J, Carlberg B, et al. Epidemiology and etiology of ischemic stroke in young adults aged 18 to 44 years in northern Sweden. Stroke 1997; 28:1702–1709. [DOI] [PubMed] [Google Scholar]
- 2.Bogousslavsky J, Van Melle G, Regli F. The Lausanne Stroke Registry: analysis of 1,000 consecutive patients with first stroke. Stroke 1988; 19:1083–1092. [DOI] [PubMed] [Google Scholar]
- 3.Siqueira Neto JI, Santos AC, Fabio SR, et al. Cerebral infarction in patients aged 15 to 40 years. Stroke 1996; 27:2016–2019. [DOI] [PubMed] [Google Scholar]
- 4.Murray CJ, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012; 380:2197–2223. [DOI] [PubMed] [Google Scholar]
- 5.Smajlovic D. Strokes in young adults: epidemiology and prevention. Vasc Health Risk Manag 2015; 11:157–164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ji R, Schwamm LH, Pervez MA, et al. Ischemic stroke and transient ischemic attack in young adults: risk factors, diagnostic yield, neuroimaging, and thrombolysis. JAMA Neurol 2013; 70:51–57. [DOI] [PubMed] [Google Scholar]
- 7.Renna R, Pilato F, Profice P, et al. Risk factor and etiology analysis of ischemic stroke in young adult patients. J Stroke Cerebrovasc Dis 2014; 23:e221–e227. [DOI] [PubMed] [Google Scholar]
- 8.Dong JY, Zhang YH, Tong J, et al. Depression and risk of stroke: a meta-analysis of prospective studies. Stroke 2012; 43:32–37. [DOI] [PubMed] [Google Scholar]
- 9.Lambiase MJ, Kubzansky LD, Thurston RC. Prospective study of anxiety and incident stroke. Stroke 2014; 45:438–443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Prieto ML, Cuellar-Barboza AB, Bobo WV, et al. Risk of myocardial infarction and stroke in bipolar disorder: a systematic review and exploratory meta-analysis. Acta Psychiatr Scand 2014; 130:342–353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tsai KY, Lee CC, Chou YM, et al. The incidence and relative risk of stroke in patients with schizophrenia: a five-year follow-up study. Schizophrenia research 2012; 138:41–47. [DOI] [PubMed] [Google Scholar]
- 12.Li CT, Bai YM, Tu PC, et al. Major depressive disorder and stroke risks: a 9-year follow-up population-based, matched cohort study. PloS one 2012; 7:e46818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Iso H, Baba S, Mannami T, et al. Alcohol consumption and risk of stroke among middle-aged men: the JPHC Study Cohort I. Stroke 2004; 35:1124–1129. [DOI] [PubMed] [Google Scholar]
- 14.Chen MH, Pan TL, Li CT, et al. Risk of stroke among patients with post-traumatic stress disorder: nationwide longitudinal study. Br J Psychiatry 2015; 206:302–307. [DOI] [PubMed] [Google Scholar]
- 15.Chen MH, Su TP, Chen YS, et al. Attention deficit hyperactivity disorder, tic disorder, and allergy: is there a link? A nationwide population-based study. J Child Psychol Psychiatry 2013; 54:545–551. [DOI] [PubMed] [Google Scholar]
- 16.Shen CC, Tsai SJ, Perng CL, et al. Risk of Parkinson disease after depression: a nationwide population-based study. Neurology 2013; 81:1538–1544. [DOI] [PubMed] [Google Scholar]
- 17.Wang YP, Chen YT, Tsai CF, et al. Short-term use of serotonin reuptake inhibitors and risk of upper gastrointestinal bleeding. Am J Psychiatry 2014; 171:54–61. [DOI] [PubMed] [Google Scholar]
- 18.Liu CY, Hung YT, Chuang YL, et al. Incorporating development stratification of Taiwan townships into sampling design of large scale health interview survey. J Health Manag (Chin) 2006; 4:1–22. [Google Scholar]
- 19.Salaycik KJ, Kelly-Hayes M, Beiser A, et al. Depressive symptoms and risk of stroke: the Framingham Study. Stroke 2007; 38:16–21. [DOI] [PubMed] [Google Scholar]
- 20.Seifert CL, Poppert H, Sander D, et al. Depressive symptoms and the risk of ischemic stroke in the elderly-influence of age and sex. PloS one 2012; 7:e50803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lin HC, Tsai SY, Lee HC. Increased risk of developing stroke among patients with bipolar disorder after an acute mood episode: a six-year follow-up study. J Affect Disord 2007; 100:49–54. [DOI] [PubMed] [Google Scholar]
- 22.Wu HC, Chou FH, Tsai KY, et al. The incidence and relative risk of stroke among patients with bipolar disorder: a seven-year follow-up study. PloS one 2013; 8:e73037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Hsieh MH, Tang CH, Lee IH, et al. Medical costs and vasculometabolic comorbidities among patients with bipolar disorder in Taiwan - a population-based and matched-control study. J Affect Disord 2012; 141:449–456. [DOI] [PubMed] [Google Scholar]
- 24.Chou PH, Lin CH, Loh el W, et al. Panic disorder and risk of stroke: a population-based study. Psychosomatics 2012; 53:463–469. [DOI] [PubMed] [Google Scholar]
- 25.Subha PP, Pillai Geethakumari SM, Athira M, et al. Pattern and risk factors of stroke in the young among stroke patients admitted in medical college hospital, Thiruvananthapuram. Ann Indian Acad Neurol 2015; 18:20–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.von Sarnowski B, Putaala J, Grittner U, et al. Lifestyle risk factors for ischemic stroke and transient ischemic attack in young adults in the Stroke in Young Fabry Patients study. Stroke 2013; 44:119–125. [DOI] [PubMed] [Google Scholar]
- 27.Romelsjo A, Allebeck P, Andreasson S, et al. Alcohol, mortality and cardiovascular events in a 35 year follow-up of a nationwide representative cohort of 50,000 Swedish conscripts up to age 55. Alcohol Alcohol 2012; 47:322–327. [DOI] [PubMed] [Google Scholar]
- 28.George MG, Tong X, Kuklina EV, et al. Trends in stroke hospitalizations and associated risk factors among children and young adults, 1995-2008. Ann Neurol 2011; 70:713–721. [DOI] [PubMed] [Google Scholar]
- 29.Maaijwee NA, Rutten-Jacobs LC, Schaapsmeerders P, et al. Ischaemic stroke in young adults: risk factors and long-term consequences. Nat Rev Neurol 2014; 10:315–325. [DOI] [PubMed] [Google Scholar]
- 30.Bai YM, Su TP, Chen MH, et al. Risk of developing diabetes mellitus and hyperlipidemia among patients with bipolar disorder, major depressive disorder, and schizophrenia: a 10-year nationwide population-based prospective cohort study. J Affect Disord 2013; 150:57–62. [DOI] [PubMed] [Google Scholar]
- 31.Butnoriene J, Bunevicius A, Saudargiene A, et al. Metabolic syndrome, major depression, generalized anxiety disorder, and ten-year all-cause and cardiovascular mortality in middle aged and elderly patients. Int J Cardiol 2015; 190:360–366. [DOI] [PubMed] [Google Scholar]
- 32.Malhotra N, Kulhara P, Chakrabarti S, et al. A prospective, longitudinal study of metabolic syndrome in patients with bipolar disorder and schizophrenia. J Affect Disord 2013; 150:653–658. [DOI] [PubMed] [Google Scholar]
- 33.Kaptoge S, Di Angelantonio E, Lowe G, et al. C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: an individual participant meta-analysis. Lancet 2010; 375:132–140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Cui G, Wang H, Li R, et al. Polymorphism of tumor necrosis factor alpha (TNF-alpha) gene promoter, circulating TNF-alpha level, and cardiovascular risk factor for ischemic stroke. J Neuroinflammation 2012; 9:235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Tong Y, Wang Z, Geng Y, et al. The association of functional polymorphisms of IL-6 gene promoter with ischemic stroke: analysis in two Chinese populations. Biochem Biophys Res Commun 2010; 391:481–485. [DOI] [PubMed] [Google Scholar]
- 36.Dowlati Y, Herrmann N, Swardfager W, et al. A meta-analysis of cytokines in major depression. Biol Psychiatry 2010; 67:446–457. [DOI] [PubMed] [Google Scholar]
- 37.Liu Y, Ho RC, Mak A. Interleukin (IL)-6, tumour necrosis factor alpha (TNF-alpha) and soluble interleukin-2 receptors (sIL-2R) are elevated in patients with major depressive disorder: a meta-analysis and meta-regression. J Affect Disord 2012; 139:230–239. [DOI] [PubMed] [Google Scholar]
- 38.Kim YK, Jung HG, Myint AM, et al. Imbalance between pro-inflammatory and anti-inflammatory cytokines in bipolar disorder. J Affect Disord 2007; 104:91–95. [DOI] [PubMed] [Google Scholar]
- 39.Vogelzangs N, Beekman AT, de Jonge P, et al. Anxiety disorders and inflammation in a large adult cohort. Transl Psychiatry 2013; 3:e249. [DOI] [PMC free article] [PubMed] [Google Scholar]