

Abstract
Introduction
Denture ingestion or aspiration is a problem requiring awareness of different specialists including dentists, surgeons, otolaryngologists, anesthesiologists etc. in terms of prevention, early diagnosis and adequate treatment. Complications of swallowed dentures include hollow viscus necrosis, perforation, penetration to neighbor organs leading to fistulae, bleeding and obstruction.
Presentation of cases
First case is a 54-year-old female who accidentally swallowed retractable one-tooth denture during fall about 22 h before admission and clinical manifestation of acute small bowel obstruction developed. The patient underwent laparotomy, enterotomy with retrieval of the foreign body. The second case is a 31-year-old male who accidentally ingested fixed one-tooth prosthesis while eating which impacted in the ileocaecal valve. During the preparation to colonoscopy the denture spontaneously passed out with stools.
Discussion
Denture ingestion is more common among patients with psychoneurologic deficit, alcohol and drug abusers. Among healthy and younger population denture ingestion is rare. Both reported patients are not elder. Thus dislodgement of removable or fixed dentures is another risk factor of denture ingestion. Most common site of denture impaction is esophagus; small bowel impaction is rare. Moreover, in most reported cases, small bowel impaction of ingested dentures leads to small bowel perforation. In our first case the complication of denture ingestion appeared to be bowel obstruction what is even rarer.
Conclusion
Fixed dentures can be accidentally ingested as well as removable dentures. Denture loosening leads to accidental denture ingestion. Patients with denture loosening should be recommended to visit dentist as soon as possible.
Keywords: Denture ingestion, Denture aspiration, Swallowed denture, Foreign bodies of gastrointestinal tract, Small bowel obstruction
Highlights
-
•
Denture ingestion or aspiration is a multidisciplinary problem.
-
•
Fixed dentures are also at high risk of ingestion or aspiration in case of their spontaneous or traumatic dislodgement.
-
•
Clinical presentation of denture ingestion is very different depending on the site of impaction and complications.
-
•
Patients with loose dentures should visit dentist as early as possible.
1. Introduction
The problem of inhaled or swallowed dentures is a multidisciplinary problem which concerns to surgery, dentistry, endoscopy, otolaryngology, anesthesiology, psychiatry, neurology, thoracic surgery, emergency medicine. From the viewpoint of surgeons, anesthesiologists, otolaryngologists inhaled or ingested denture is a foreign body of respiratory or gastrointestinal tract. From dentists' viewpoint aspiration and ingestion are complications of dentures. This makes swallowed dentures a special kind of foreign bodies distinct from needles, coins, batteries etc. So collaborative decisions are crucial for prevention, early diagnosis and adequate treatment of denture aspiration or ingestion. About 80% of all ingested foreign bodies pass out through entire gastrointestinal tract spontaneously and 20% of them can impact at different levels of gastrointestinal tract [1], [2]. The most common site of impaction of ingested denture is esophagus [3]; denture impaction in small bowel is rare. Dentures impacted in different parts of gastrointestinal tract lead to various surgical complications including perforation, penetration to neighbor organs, bleeding and obstruction. The most common surgical complication is perforation; bleeding, obstruction and penetration are rare.
2. Presentation of cases
2.1. Case 1
A 54-year-old female was admitted to Vladimir City Clinical Hospital of Emergency Medicine with 6 h history of abdominal colicky pain, nausea, vomiting. She had accidentally swallowed her one-tooth removable denture (left mandibular M2; Kennedy class III removable partial denture) during accidental fall at home about 22 h before admission. During the first 12 h the patient was asymptomatic, so she was waiting for passing the denture out through faeces. The denture was constructed about 4 years before admission. Last 6 months she noticed loosening of the denture and had not gone back to her dentist for check-up. The patient's past medical history was unremarkable. On admission she was hemodynamically stable. There were no sites of significant trauma. On abdominal physical exam tenderness on left iliac fossa and suprapubic region and succussion splash was noticed. Abdominal plain X-ray revealed small bowel liquid gas levels and a foreign body (denture) in left iliac fossa (Fig. 1). The patient underwent laparotomy after IV crystalloids infusion during 1 h (total volume- 1 L) and nill by mouth. Denture impacted in middle ileum leading to bowel obstruction was found and enterotomy with retrieval of the foreign body was performed (Fig. 2). The denture was cleaned and returned to the patient. Postoperatively, oral feeds resumed on the second postoperative day. The patient recovered uneventfully and discharged on 8th postoperative day.
Fig. 1.
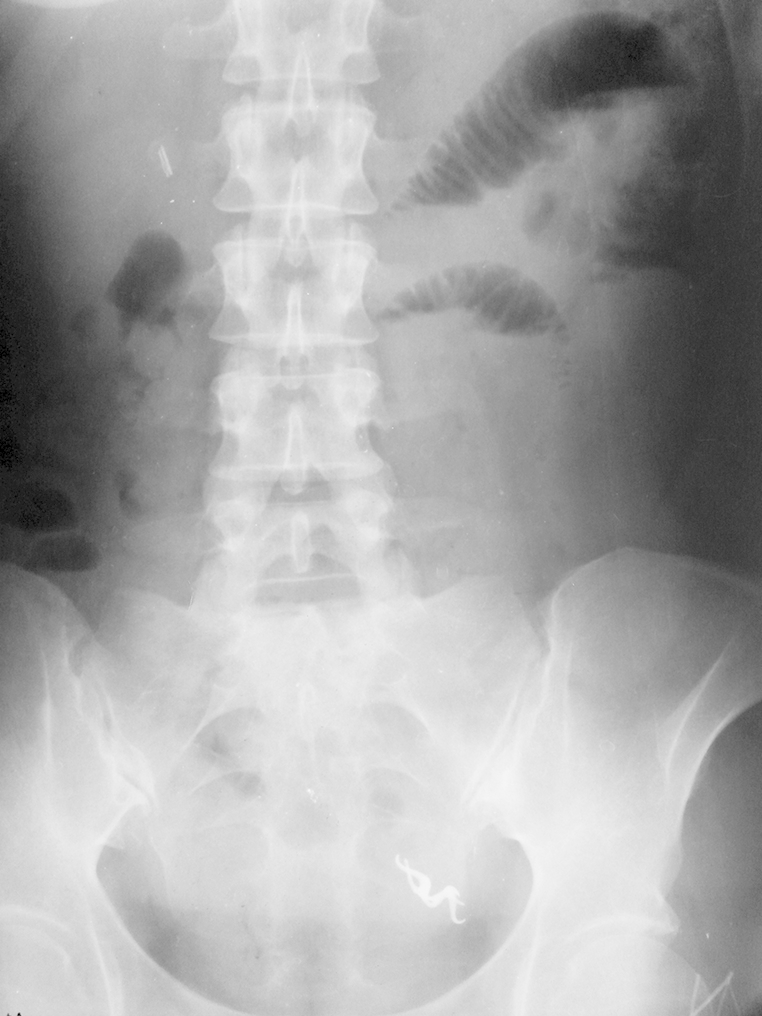
Plain abdominal X-ray: air/fluid levels and denture in left lower quadrant.
Fig. 2.

Ingested removable one-tooth denture (left mandibular M2).
2.2. Case 2
A 31-year-old male came to Vladimir City Clinical Hospital of Emergency Medicine after 2 h of fixed one-tooth denture ingestion during eating. The patient's past medical history was unremarkable. His denture (right maxillary P1, metal core fixed denture) was constructed 6 years before admission and he noticed its loosening a month before ingestion and had not gone back to his dentist for check-up. The first plain abdominal X-ray showed the ingested denture to be in the stomach (Fig. 3-a). EGD was unsuccessful because his stomach was full of ingested food. After 12 h the ingested denture was in right iliac fossa (Fig. 3-b) and the patient had no complaint. During the next 48 h the ingested denture remained in right iliac fossa and the patient started to complain of pain in right lower quadrant without peritoneal signs (Fig. 3-c and 3-d). On Fig. 3-d small bowel dilation is seen what seems to be the reason of developed abdominal pain due to partial obstruction of ileocecal valve. After that, abdominal CT was performed. On CT the denture was impacted in ileocecal valve (Fig. 4). It was decided to prepare the patient for a colonoscopy with further foreign body removal. During preparation with laxatives the ingested denture passed out with stools (Fig. 5). After 3 days of out-patient follow-up the patient was well.
Fig. 3.

a- Denture is in the stomach, b- Denture is in right iliac fossa, c- Denture is in right iliac fossa, d- Denture in right iliac fossa, dilatation of small bowel loops.
Fig. 4.

CT scans showing denture impacted in ileocecal valve.
Fig. 5.

Ingested fixed one-tooth denture (right maxillary P1).
3. Discussion
3.1. Background
Foreign bodies of aerodigestive tract is not an uncommon problem, especially among pediatric population. The peak of incidence of foreign body ingestion and aspiration is at the age range of 6 months to 6 years [1]. Among adults foreign body ingestion is less frequent and varies in different populations. In Western countries the most common foreign body is non-bony food bolus [2] while in Asia chicken and fish bones are more frequent [3]. According to the data of statistical departments of Vladimir City Clinical Hospital of Emergency Medicine and Vladimir Oblast Clinical Hospital, In Vladimir city, Russia the most common foreign body among adults in otolaryngology practice (pharynx and cervical esophagus) is fish bone (about 55% of all foreign bodies). In surgical practice the most common foreign body among adults is needle; however, the most common foreign body complicated with perforation of gastrointestinal tract (mostly small bowel) and requiring surgery is fish bone again (68% of all foreign bodies leading to small bowel perforation). Foreign body aspiration and ingestion is mostly encountered among patients with psycho-neurological deficit, alcohol intoxication, drug overdose, general anesthesia [4], [5] and maxillofacial trauma [6]. Edentulous people are also at higher risk of foreign body ingestion including dentures due to reduced sensation of the oral mucosa and poor motor control of laryngopharynx [7]. Another important issue increasing the risk of denture ingestion is lack of patient awareness about the need in regular check-ups and denture change or compliance [8], [9]. Most guidelines of Russian national institutions and international societies recommend immediate dental recall in case of denture dislodgement (especially with vertical mobility).
Dentures, being medical prosthetic devices for the improvement of mastication, esthetics, articulation and self-esteem, are a special type of foreign bodies. The key point in this problem is that denture ingestion per-se is a complication of denture wearing warning us to improve prevention as well as early diagnosis and treatment, i.e., dentists have to be aware of this potential problem as well as otolaryngologists, surgeons and anesthesiologists.
Acute disorders of consciousness (craniofacial trauma, stroke, convulsion, intoxication) increase the risk of denture aspiration or ingestion as well as stomach content aspiration. In conscious patients activities during which denture aspiration or ingestion can occur are well-described [8]: fall, eating, drinking, sleep and anesthesia [4], [5]. Our patients ingested dentures during fall and eating.
3.2. Sites of denture impaction
In about 70% of all reported cases the site of denture impaction is the esophagus. The incidence of denture impaction in the esophagus varies from 0.4% [3] to 17.6% [8]. The commonest sites of foreign body impaction in gastrointestinal tract are physiologic constrictions, angulations or stenoses [10], [11]. The three physiologic constrictions of the esophagus, therefore, appear to be frequent location of impacted denture, the upper constriction being the narrowest portion of the esophagus and the commonest site of denture impaction (15 cm from upper incisors; where the esophagus commences at the cricopharyngeal sphincter). Most of reported cases demonstrate ingestion of removable dentures especially partial ones; however, fixed dentures also become a subject of ingestion in case of spontaneous or traumatic dislodgement what requires awareness of anesthesiologists who ask patients only about removable dentures before anesthesia [12]. Denture impaction in small bowel is rare; and in almost all reported cases the site of impaction appeared to be terminal ileum [13], [14]. Padav PH et al. reported a case of denture impaction in middle ileum what we also faced in our first case [15]. Denture impaction in large bowel and its possible consequences are uncommon because of its larger diameter and solid consistency of its contents what helps to avoid trauma of bowel wall. Theoretically, denture passed through ileocecal valve should pass through large bowel uneventfully and the only cause of denture impaction can become colonic stenosis such as in colon cancer [16]. Nonetheless, several cases of colon perforation, especially sigmoid colon perforation, were reported [11], [17].
3.3. Clinical presentation and complications
Clinical presentation of denture ingestion correlates with the site of impaction and complication emerged. Complications of denture ingestion are necrosis, perforation, penetration to adjacent organs, bleeding and obstruction. Complications according to sites of denture impaction and their clinical presentations are described in Table 1. Most common complication is perforation of gastrointestinal tract. Perforation due to impacted denture per-se can cause secondary fatal complications such as deep neck infections, mediastinitis and peritonitis. Penetration to adjacent organs is a rare complication leading to fistulae formation such as broncho-esophageal fistula [18] and entero-colic fistula [19]. Gastrointestinal bleeding is a result of ulceration and vessel erosion; the reported cases demonstrate esophageal [20] and gastric bleeding [21] caused by swallowed denture. Obstruction is also very rare and almost all reported cases of gastrointestinal tract obstruction are esophageal obstruction. To the best of our knowledge, this is the second report on small bowel obstruction caused by ingested denture [15]. Our first patient developed small bowel obstruction and underwent laparotomy; the second patient also developed ileocecal valve obstruction, however, resolved during colonoscopy preparation.
Table 1.
Complications, clinical presentation and treatment modalities according to the site of denture impaction.
| Site of denture impaction | Primary complication | Secondary complication | Clinical presentation | Treatment modalities |
|---|---|---|---|---|
| Pharynx | Necrosis Perforation |
Retropharyngeal abscess Deep neck infection Mediastinitis |
Hoarseness, choking sensation, cough, hypersalivation, dysphagia, odynophagia, hyperthermia | Endoscopic removal [30] Surgery (transcervical approach) [31], [32] |
| Esophagus: Cervical Thoracic Abdominal |
Necrosis Perforation Penetration Obstruction Bleeding |
Deep neck infection Mediastinitis Sepsis Esophagorespiratory fistula |
Hoarseness, choking sensation, cough, hypersalivation, dysphagia, odynophagia, hyperthermia, retrosternal pain, weakness, lethargy, hemoptysis, hematemesis | Endoscopic removal [8], [9], [10] Transcervical esophagotomy [8] Esophagectomy [33] |
| Stomach | Ulceration Bleeding |
Anemia | Hematemesis, melena, epigastric pain | Endoscopic removal [5] Gastrotomy (laparotomy or laparoscopy [34]) |
| Small bowel | Necrosis Perforation Obstruction Penetration |
Peritonitis Sepsis Entero-colic fistula |
Abdominal pain, nausea, vomiting, diarrhea, constipation, peritoneal signs, septic signs | Endoscopic removal [35] Enterotomy, retrieval [14] Small bowel resection [15] Ileocecal resection [15] |
| Large bowel | Perforation Obstruction |
Peritonitis Sepsis |
Abdominal pain, nausea, vomiting, diarrhea, constipation, peritoneal signs, septic signs | Endoscopic removal [36] Colic resection, anastomosis [37] Colic resection, colostomy [17] |
3.4. Management of denture impaction
Denture ingestion as well as all other foreign bodies can be accidental and intentional [22]. The key questions in the management of denture ingestion are:
-
1.
The fact of denture ingestion (a-history, b-assessment of mental status, c-oral exam, assessment of denture)
-
2.
The site of denture impaction (a-clinical presentation, b-complication, c-assessment of denture itself, d-diagnosis)
-
3.
Treatment modality
3.5. Diagnosis
In the diagnosis of denture ingestion thorough and attentive history taking is important [23]. However, not always patients are mentally or neurologically competent to notice, remember or accent the fact of denture ingestion or at least suspicion to that. Therefore, if a patient is suspicious for denture ingestion mental exam provides information about possible suicide attempts or cognitive disorders. Oral exam is another important point for fixing the fact of denture ingestion showing the absence of dentures and providing information about denture ingested [24]. Oral exam is especially crucial for patients with psycho-neurological deficit and as a part of perioperative anesthesiology assessment [25]. Denny et al. proposed a new scheme of perioperative management including photo documentation and removal of unstable dentures, thus minimizing the risk of denture aspiration and ingestion during anesthesia [12].
Assessment of ingested denture itself (dimensions; configuration; type-partial or complete, removable or fixed; materials used) is also essential for determining potential site of impaction, potential complication, potential diagnostic value of radiology and treatment modality. Dimensions and configuration of denture are equally important, so that a horseshoe shaped denture swallowed ‘end-on’ and vertically can well rotate into hypopharynx and esophagus [20]. To the best of our knowledge, all reported cases of swallowed dentures are partial dentures. Moreover, most reported cases demonstrate ingestion of removable dentures. Fixed unstable dentures are also at high risk of aspiration and ingestion during eating as demonstrated in our second case, drinking [8], anesthesia [12]. Materials commonly used in denture fabrication are acrylic resins, porcelain, gold, nickel-chrome alloy, cobalt-chrome alloy and zirconium. Acrylic resins, poly-methyl-methacrylate and porcelain are radiolucent materials what makes X-ray non-informative in case when a denture consists completely of these materials. However, air entrapment around the denture and increase in the prevertebral soft tissues as a result of local inflammatory response on plain X-rays could be observed [8], [26]. Acrylic dentures can be imaged on CT, since X-ray attenuation rather than plain radiography is sensitive for small changes [27]. They also can be imaged on MRI, the problem being the limitation of access to that in an emergency setting [28]. Desiring to find radio-opaque plastic material to fabricate dentures, Brauer found none to have physical properties, appearance and ease of handling equivalent to those in radiolucent materials; moreover, the incorporation of heavy metal salts and glass fillers to make a denture radio-opaque weakens the denture, thus, increasing the risk of its fracture and aspiration or ingestion of its parts [29]. Metal components in dentures, such as major and minor connectors, clasps, wire retainers or metal core, allows the denture be localized on X-ray. Besides this, X-ray helps us to determine primary and secondary complications of denture ingestion, such as emphysema of soft tissues of the neck, pneumomediastinum, pneumothorax, pneumoperitoneum, small and large bowel dilatation with or without air/fluid levels etc.
3.6. Treatment
Three modalities of the management of denture ingestion are available: observation (wait and watch), endoscopy and surgery. Observation is possible only in cases when the dimensions of ingested denture are small, the configuration does not assume trauma of gastrointestinal tract (not long and pointed, without sharp edges) and in case when the denture at the time of presentation is distal to the ligament of Treitz. Endoscopy is the modality of choice but is not always possible [8], [9], [10]. The main contraindication for endoscopic removal of ingested denture is a high risk or the evidence of primary and secondary complications. Foreign bodies impacted in the hypopharynx can be removed by hypopharyngoscopy and direct laryngoscopy [30]. In cases of complications, such as perforation of pharynx leading to retropharyngeal abscess [31], or failure of endoscopic removal open surgery via transcervical approach is indicated [32]. Dentures impacted in the esophagus can also be successfully removed endoscopically-either by rigid or by flexible esophagoscopy [8], [9], [32]; however, its failure or emerging complications are indications for open surgery: transcervical esophagotomy, transthoracic esophagotomy or esophagectomy [8]. Dentures impacted in small and large bowel, depending on the dimensions, configuration, presence of bowel wall perforation risk or any complication can be observed, removed endoscopically [35] or by surgery (laparotomy or laparoscopy). The gold standard for dentures impacted in upper gastrointestinal tract without any complications is endoscopy, in complicated cases surgery is inevitable. For dentures impacted in lower gastrointestinal tract in uncomplicated cases the most common strategy seems to be observation (wait and watch) and for complicated cases again surgery. Overall, the success of the treatment of denture ingestion is early diagnosis, prompt and proper decision-making and treatment started without delay.
3.7. Prevention
The prevention of denture ingestion or aspiration to a great extent is a subject for anesthesiologists, psychiatrists, dentists and emergency room physicians rather than surgeons and otolaryngologists. Anesthesiologists, psychiatrists and emergency physicians deal with the patients with high risk of denture ingestion or aspiration. Dentists should recommend patients to visit them for planned check-ups or revisit them in case of denture dislodgement, loosening within the first month of noticing the problem.
4. Conclusions
Denture is a special type of foreign body requiring awareness of different specialists. Fixed dentures are also at high risk of aspiration and ingestion as well as removable dentures, especially unstable ones. Early diagnosis and treatment is vital in the management of swallowed dentures. Patients with loose removable or fixed dentures should be recommended to revisit their dentists immediately.
Ethical approval
None.
Funding
None.
Author contribution
Gachabayov Mahir.
-
(1)
The conception and design of the study, acquisition of data, analysis and interpretation of data.
-
(2)
Drafting the article and revising it critically for important intellectual content.
-
(3)
Final approval of the version to be submitted.
Isaev Mubariz.
-
(1)
The conception and design of the study and analysis and interpretation of data.
-
(2)
Drafting the article or revising it critically for important intellectual content.
-
(3)
Final approval of the version to be submitted.
Orujova Lala.
-
(1)
The conception and design of the study, acquisition of data, analysis and interpretation of data.
-
(2)
Drafting the article or revising it critically for important intellectual content.
-
(3)
Final approval of the version to be submitted
Isaev Emin.
-
(1)
The conception and design of the study, analysis and interpretation of data.
-
(2)
Drafting the article or revising it critically for important intellectual content.
-
(3)
Final approval of the version to be submitted
Yaskin Evgeniy.
-
(1)
Analysis and interpretation of data.
-
(2)
Revising the article critically for important intellectual content.
-
(3)
Final approval of the version to be submitted.
Neronov Dmitriy.
-
(1)
Analysis and interpretation of data.
-
(2)
Drafting the article or revising it critically for important intellectual content.
-
(3)
Final approval of the version to be submitted.
Conflicts of interest
None.
Guarantor
Gachabayov Mahir, MD, Attending surgeon, Department of abdominal surgery, Vladimir City Clinical Hospital of Emergency Medicine, Address: 600022, Stavrovskaya street, 6–73, Vladimir/Russia. e-mail: gachabayovmahir@gmail.com. Tel.: +7(915)7901632.
Contributor Information
Mahir Gachabayov, Email: gachabayovmahir@gmail.com.
Mubariz Isaev, Email: boris-isaev@inbox.ru.
Lala Orujova, Email: oruceva.lala@yahoo.com.
Emin Isaev, Email: emin_isaev@mail.ru.
Evgeniy Yaskin, Email: e.yaskin@mail.ru.
Dmitriy Neronov, Email: drneronov@gmail.com.
References
- 1.Cheng W., Tam P.K. Foreign-body ingestion in children: experience with 1265 cases. J. Pediatr. Surg. 1999;34:1472–1476. doi: 10.1016/s0022-3468(99)90106-9. [DOI] [PubMed] [Google Scholar]
- 2.Webb W.A. Management of foreign bodies of the upper gastrointestinal tract: update. Gastrointest. Endosc. 1995;41:39–51. doi: 10.1016/s0016-5107(95)70274-1. [DOI] [PubMed] [Google Scholar]
- 3.Nandi P., Ong G.B. Foreign body in the esophagus: review of 2394 cases. Br. J. Surg. 1978;65:5–9. doi: 10.1002/bjs.1800650103. [DOI] [PubMed] [Google Scholar]
- 4.Lau G., Kulkarni V., Roberts G.K. Anesth. Analg. 2009;109(3):836–838. doi: 10.1213/ane.0b013e3181ae06c9. [DOI] [PubMed] [Google Scholar]
- 5.Neustein S., Beicke M. Ingestion of a fixed partial denture during general anesthesia. Anesth. Prog. 2007;54(2):50–51. doi: 10.2344/0003-3006(2007)54[50:IOAFPD]2.0.CO;2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hodges E.D., Durham T.M., Stanley R.T. Management of aspiration and swallowing incidents: a review of the literature and report of a case. ASDC J. Dent. Child. 1992;59:413–419. [PubMed] [Google Scholar]
- 7.Toshima T., Morita M., Sadanaga N. Surgical removal of a denture with sharp clasps impacted in the cervicothoracic esophagus: report of three cases. Surg. Today. 2011;41:1275–1279. doi: 10.1007/s00595-010-4467-x. [DOI] [PubMed] [Google Scholar]
- 8.Bandyopadhyay S.N., Das S., Das S.K. Impacted dentures in the oesophagus. J. Laryngol. Otol. 2014 Apr 23:1–7. doi: 10.1017/S002221511400070X. [DOI] [PubMed] [Google Scholar]
- 9.Okugbo S., Onyeagwara N. Oesophageal impacted dentures at the University of Benin Teaching Hospital, Benin city, Nigeria. J. West Afr. Coll. Surg. 2012;2(2):102–111. [PMC free article] [PubMed] [Google Scholar]
- 10.Ginsberg G.G. Management of ingested foreign objects and food bolus impactions. Gastrointest. Endosc. 1995;41:33–38. doi: 10.1016/s0016-5107(95)70273-3. [DOI] [PubMed] [Google Scholar]
- 11.Khadda S., Yadav A.K., Ali A. A rare case report of sigmoid colon perforation due to accidental swallowing of partial denture. Indian J. Surg. 2015;77(2):152–154. doi: 10.1007/s12262-015-1299-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Denny J.T., Yeh S., Mohiuddin A. Preventing “A Bridge Too Far”: promoting earlier identification of dislodged dental appliances during the perioperative period. J. Clin. Med. Res. 2015;7(2):115–117. doi: 10.14740/jocmr1981w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Rashid F., Simpson J., Ananthakrishnan G. Swallowed dental bridge causing ileal perforation: a case report. Cases J. 2008;1:392. doi: 10.1186/1757-1626-1-392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bunni J., Youssef F. Swallowed dental bridge perforating the terminal ileum. South Med. J. 2010;103:593–594. doi: 10.1097/SMJ.0b013e3181dfd8a0. [DOI] [PubMed] [Google Scholar]
- 15.Patel P.H., Slesser A.A., Idaikkadar P. Delayed presentation of a small bowel perforation secondary to an ingested denture. JRSM Short. Rep. 2012;3(9):60. doi: 10.1258/shorts.2012.012014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Candia-de la Rosa R.F., Candia-García R., Pérez-Martínez M.C. Intestinal obstruction due to foreign body in a patient with adenocarcinoma of the colon: case report. Cir. Cir. 2010;78(1):87–91. [PubMed] [Google Scholar]
- 17.Peison B., Benisch B., Lim E. Perforation of the sigmoid colon following ingestion of a dental plate. N. J. Med. 1995;92(7):452–453. [PubMed] [Google Scholar]
- 18.Odigie V.I., Yusufu L.M.D., Abur P. Broncho-Oesophageal Fistula (BOF) secondary to missing partial denture in an alcoholic in a low resource country. Oman Med. J. 2011;26(1):51–52. doi: 10.5001/omj.2011.13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Jüngling G., Wiessner V., Gebhardt C. Enterocolic fistula due to foreign body perforation. Dtsch. Med. Wochenschr. 1994;119(3):63–66. doi: 10.1055/s-2008-1058662. Article in German. [DOI] [PubMed] [Google Scholar]
- 20.Hashmi S., Walter J., Smith W. Swallowed partial dentures. J. R. Soc. Med. 2004;97(2):72–75. doi: 10.1258/jrsm.97.2.72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Paulsen J.M., Aragon G.C., Jager D.L. Unusual cause of upper gastrointestinal bleed: gastric ulceration and bleed secondary to ingested dental bridge. Am. J. Gastroenterol. 2009;104(2):535–537. doi: 10.1038/ajg.2008.83. [DOI] [PubMed] [Google Scholar]
- 22.Price W.A., Giannini A.J. Attempted suicide by ingestion of dentures. J. Clin. Psychiatry. 1984;45(4):189. [PubMed] [Google Scholar]
- 23.Kim H.S., Kim C.H., Kim M.O. Forgotten denture in a hemiplegic patient. Am. J. Phys. Med. Rehabil. 2014;93(3):267–271. doi: 10.1097/PHM.0b013e3182a92f2f. [DOI] [PubMed] [Google Scholar]
- 24.Slade P.M., Larsen M.P. Dysphagia, dysphonia and sore throat following cerebral infarction: an unexpected cause. BMJ Case Rep. 2015 Jul;6:2015. doi: 10.1136/bcr-2015-210091. pii: bcr2015210091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Yasny J.S. Perioperative dental considerations for the anesthesiologist. Anesth. Analg. 2009;108(5):1564–1573. doi: 10.1213/ane.0b013e31819d1db5. [DOI] [PubMed] [Google Scholar]
- 26.Gionvannitti J.A. Aspiration of a partial denture during an epileptic seizure. J. Am. Dent. Assoc. 1981;103:895. doi: 10.14219/jada.archive.1981.0404. [DOI] [PubMed] [Google Scholar]
- 27.McLaughlin M.G., Dwayne L.C., Garuana V. Computed tomographic detection of swallowed dentures. Comput. Med. Imaging Graph. 1989;13:161–163. doi: 10.1016/0895-6111(89)90192-4. [DOI] [PubMed] [Google Scholar]
- 28.Chrcanovic B.R., Custódio A.L.N. Swallowed partial denture: a case report and a literature review. Arq. Bras. Odontol. 2010;6(1):19–24. [Google Scholar]
- 29.Brauer G.M. The desirability of using radio-opaque plastics in dentistry—a status report. J. Am. Dent. Assoc. 1981;102:347–349. doi: 10.14219/jada.archive.1981.0058. [DOI] [PubMed] [Google Scholar]
- 30.Sharma R.C., Dogra S.S., Mahajan V.K. Oro-pharyngo-laryngeal foreign bodies: some interesting cases. Indian J. Otolaryngol. Head. Neck Surg. 2012;64(2):197–200. doi: 10.1007/s12070-011-0473-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Singh B., Gady Har E.L., Kantu M. Complications associated with 327 foreign bodies of the pharynx, larynx and esophagus. Ann. Otol. Rhinol. Laryngol. 1997;106:301–304. doi: 10.1177/000348949710600407. [DOI] [PubMed] [Google Scholar]
- 32.Shreshtha D., Sikka K., Singh C.A. Foreign body esophagus: when endoscopic removal fails…. Indian J. Otolaryngol. Head. Neck Surg. 2013;65(4):380–382. doi: 10.1007/s12070-013-0662-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Singh P., Singh A., Kant P. An impacted denture in the oesophagus-an endoscopic or a surgical emergency-a case report. J. Clin. Diagn Res. 2013;7(5):919–920. doi: 10.7860/JCDR/2013/5337.2976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Furihata M., Tagaya N., Furihata T. Laparoscopic removal of an intragastric foreign body with endoscopic assistance. Surg. Laparosc. Endosc. Percutan Tech. 2004;14(4):234–237. doi: 10.1097/01.sle.0000136682.69871.db. [DOI] [PubMed] [Google Scholar]
- 35.Abe K., Miki A., Okamura T. Endoscopic removal of a denture with clasps impacted in the ileocecum. Clin. J. Gastroenterol. 2014;7(6):506–509. doi: 10.1007/s12328-014-0539-6. [DOI] [PubMed] [Google Scholar]
- 36.Segall M.M., Klein S.N., Bradley G.T. Colonoscopic extraction of dentures. Gastrointest. Endosc. 1983;29(2):142–143. doi: 10.1016/s0016-5107(83)72562-9. [DOI] [PubMed] [Google Scholar]
- 37.Cleator I.G., Christie J. An unusual case of swallowed dental plate and perforation of the sigmoid colon. Br. J. Surg. 1973;60(2):163–165. doi: 10.1002/bjs.1800600219. [DOI] [PubMed] [Google Scholar]