

Abstract
Background:
Having pleasurable sexual intercourses plays a major role in marital life satisfaction. Many of the medical and psychiatric disorders may affect the sexual function of the patients. The present study aims to investigate the relative frequency of sexual dysfunctions in the patients hospitalized in psychiatric wards and that of the patients in other specialized wards.
Materials and Methods:
This study is a descriptive-analytical, cross-sectional one, carried out on 900 patients hospitalized in psychiatric, cardiac, orthopedic, ophthalmology, and dermatology and plastic surgery wards of 5 hospitals in Isfahan. Data collection tools included demographic questionnaire and Arizona Sexual Experiences Scale (ASEX).
Results:
Sexual dysfunction in the patients hospitalized in psychiatric wards (38%) was significantly higher than in the patients in other wards (27%), (P = 0.00). Among the patients hospitalized in psychiatric wards, those with bipolar disorder (37.3%) had the highest prevalence rate of sexual dysfunction. The patients with schizophrenia, major depression, substance abuse, and anxiety disorders had the following rates respectively. Among the patients in non-psychiatric wards, those in cardiac wards (37.1%) had the highest prevalence rate of sexual dysfunction. There was a significant relationship between the drug uses, mostly psychiatric drugs especially anti-psychotics, and the occurrence of sexual dysfunction.
Conclusion:
Considering the significant relative frequency of sexual dysfunction in psychiatric patients and undesired effects of simultaneous occurrence of both of these disorders in the patients, more emphasis is recommended to be placed on the prevention and proper treatment of these disorders in the patients.
Keywords: Psychiatric disorders, psychiatric wards, sexual dysfunction
INTRODUCTION
Having pleasurable sexual intercourses plays a major role in marital life satisfaction. Dissatisfaction of the couples in this respect may have the root of various physical, mental, and social problems.[1,2] According to the definitions available in the most reliable classifications of World Health Organization (WHO) and American Psychiatric Association, sexual dysfunction implies sexual response cycle dysfunction in sexual desire, arousal and resolution, and orgasm during sexual intercourse in such a way that the individual is deprived of a desired sexual intercourse. The continuity of this deficiency existing in most cases of sexual intercourse leads to obvious discomforts in sufferers and their interpersonal relationships with their sex partners.[3,4]
Such dysfunctions exist in all societies.[5] Also, studies conducted in Iran exert the significant prevalence of these dysfunctions in such a manner that among 400 divorce applicants referring to judicial complexes in Tehran, 66.7% of men and 68.4% of women have been dissatisfied with sexual life with their spouses.[6] Similarly, in another study, carried out on married men and women referring to a family health clinic in Tehran, the prevalence rate of these dysfunctions has been significant, and 30.2% of the patients with these dysfunctions have been suffering from either different degrees of mental problems or some physical diseases.[7]
Various studies have reported the prevalence rate of sexual dysfunctions to be higher in the patients with mental illnesses than in the entire population. Simultaneous existence of both of these dysfunctions may have severe undesired effects on the patients’ life quality and their spouses. Mutual effects of mental illnesses and sexual dysfunction on one another and the complexity of the factors effective in causing them are of the treatment difficulties of the patients developing these two disorders.[8,9] In spite of the prevalence and great importance of these disorders, mental health providers pay little attention to discover and treat them. One of the most important reasons of this fact is, perhaps, that sexual issues in different societies and in particular in eastern culture are considered as taboo and that yet sufficient knowledge on the quantity and quality of the evaluation and treatment of these disorders is not obtained.[10,11]
Since simultaneous occurrence of mental and physical diseases and sexual dysfunctions can multiply the side effects resulted from these disorders, the results of the present study may respond some questions on the prevalence rates of these disorders in psychiatric patients compared to medical patients and the factors influencing them.
MATERIALS AND METHODS
The present study with a cross-sectional design was conducted on 900 patients hospitalized in psychiatric wards of the hospitals “Noor,” “Modarres,” and “Farabi” and cardiac, orthopedic, ophthalmology, and dermatology and plastic surgery wards of the hospitals “Al-Zahra,” “Farabi,” and “Imam mousa kazem” using convenience sampling.
All the men and women between 18 and 50 years old hospitalized in forenamed wards during 2012 to 2013, since the hospitalization of who 2 weeks were passed, entered the study. Single, divorced, and widow patients and all those who were not able to respond the questions for different reasons including cognitive disorders were excluded from the study. The information needed on the reasons of conducting this study and on the confidentiality of the information was explained to the patients. Finally, after the informed consent was obtained from the patients, the questionnaires were filled in by a clinical psychologist and a psychiatric resident responsible for the present study and in compliance with the patients’ gender.
Data collection tools were demographic data questionnaire including age, gender, level of education, type of the drug received, type of mental and physical disease and hospitalization ward, and Arizona Sexual Experiences Scale (ASEX) to evaluate the patients’ sexual function. Reliability and Validity of the ASEX scale in various studies carried out in Iran have been obtained by Cronbach's alpha = 0.836 and Pearson correlation coefficient for men's sexual questions r = 0.832.[12,13]
Statistical analyses were done by “SPSS-20.” Data are reported as number (percent). Assessed variables in the study were compared applying Chi-square test, and the level of significance is considered to be less than 0.05.
RESULTS
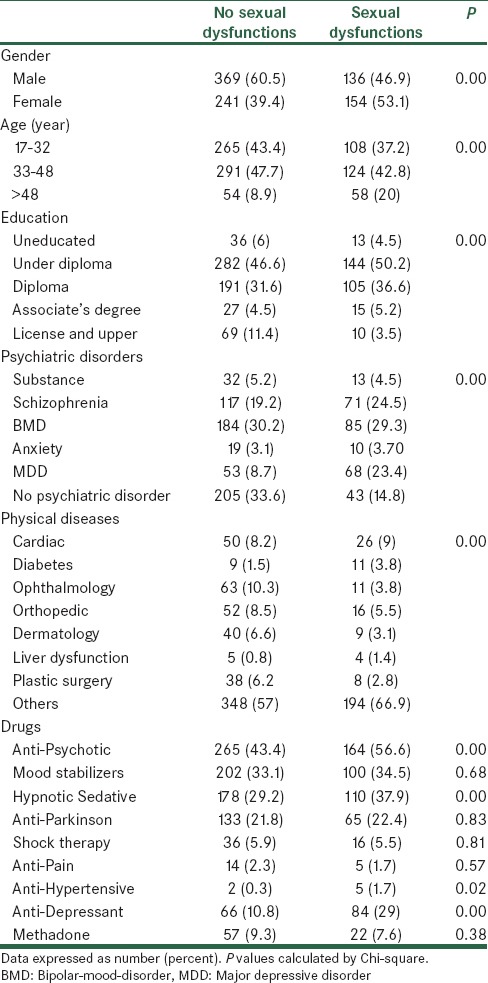
Of the total of 900 patients hospitalized in different wards, 395 were females and 505 were males. Sexual dysfunction in women was, totally, to a greater extent than in men (P = 0.00). The age group of 33 to 48 had the highest rate of sexual dysfunction (P = 0.00). The majority of the sufferers› level of education was junior high school (P = 0.00). Sexual dysfunction rate in the patients using anti-psychotic (P = 0.00), hypnotic and sedative (P = 0.009), anti-depressant (P = 0.00), and anti-hypertensive (P = 0.02) drugs was higher than in those using other drugs [Table 1].
Table 1.
Characteristics of all studied patients
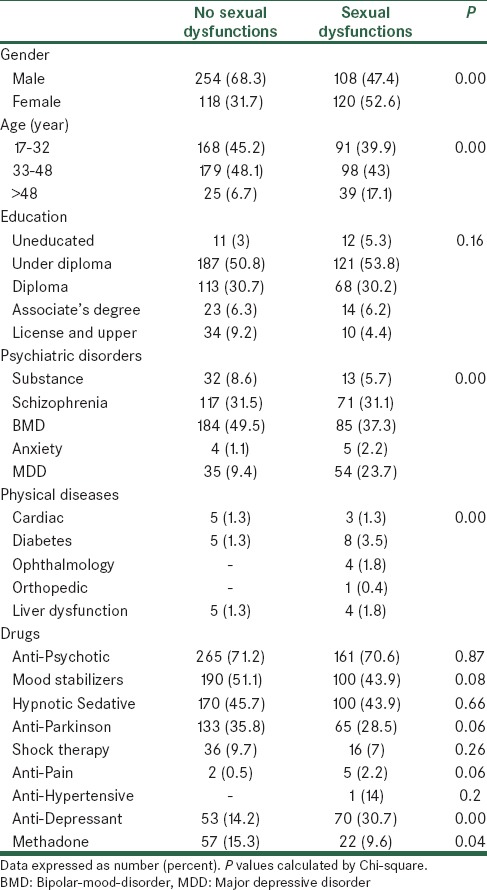
Of the patients hospitalized in psychiatric wards, 38% were suffering from sexual dysfunction. The patients with bipolar disorder (37.3%), schizophrenia (31.1%), major depression (23.7%), substance abuse (5.7%), and anxiety disorders (2.2%) had the highest rates of development, respectively. There was a significant relationship between mental disorder and sexual dysfunction (P = 0.00), [Table 2].
Table 2.
Characteristics of studied patients with psychiatric patients
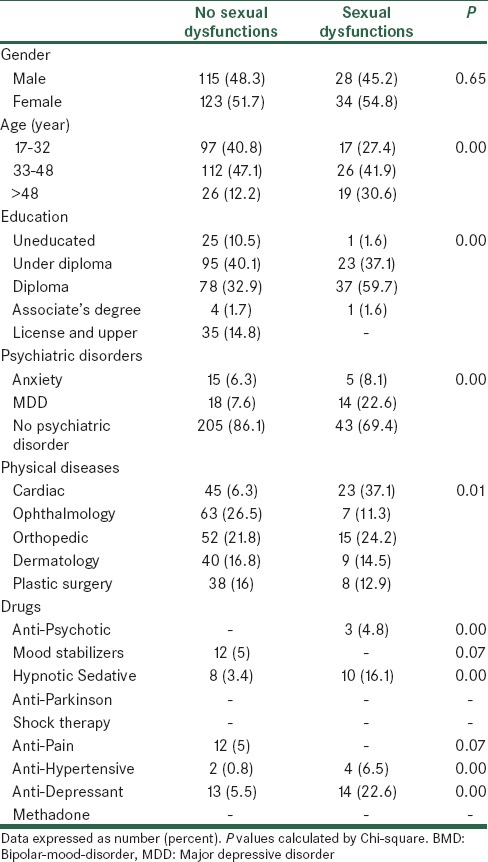
Of those patients hospitalized in non-psychiatric wards, 20.7% were suffering from sexual dysfunction, and on the contrary to the patients in psychiatric wards, no significant association was found between the patients’ gender and sexual dysfunction. The patients hospitalized in non-psychiatric wards, like those patients in psychiatric wards, had the highest rate of sexual dysfunction in the age group of 33 to 48, and the education level of the patients in this age group was diploma [Table 3].
Table 3.
Characteristics of studied patients with physical diseases
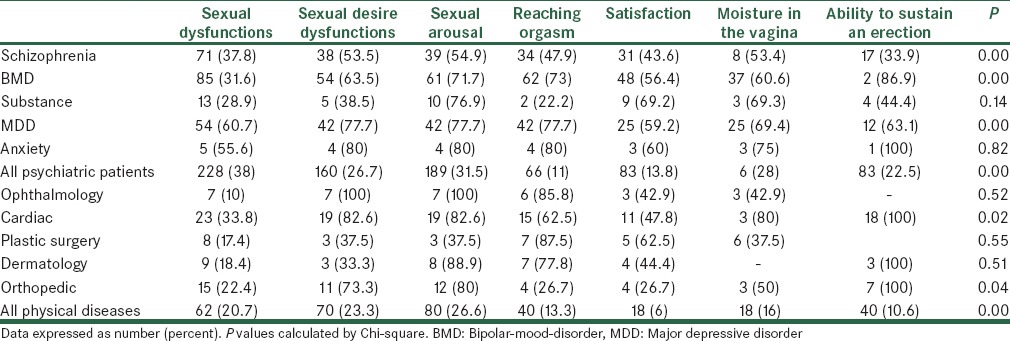
Sexual dysfunction in the patients hospitalized in psychiatric wards was significantly higher than in the patients in other specialized wards (P = 0.00). Different parameters of sexual function, also, significantly associated the type of mental illness in a way that the patients with schizophrenia, bipolar disorder, and major depression, respectively, were more suffering from lack of sexual arousal (P = 0.00), lack of reaching orgasm (P = 0.00), sexual desire disorder and failure to reach sexual arousal and orgasm (P = 0.00). In patients with anxiety disorder and substance abuse, no significant relationship between the disorder and different parameters of sexual dysfunction was observed. The patients hospitalized in cardiac ward (37.1%) had the highest rate of sexual dysfunction among the patients in non-psychiatric wards. The patients in orthopedic (24.2%), dermatology (14.5%), plastic surgery (12.9%), and ophthalmology (11.3%) wards had the following rates respectively. The non-psychiatric patients had their greatest number of sexual problems in the parameters of sexual desire and sexual arousal [Table 4].
Table 4.
Frequency of sexual dysfunctions in studied patients
During study period, three patients in case group reported side effects (nausea and vomiting and tachycardia), whereas in control groups, side effect was not observed. However, difference in the incidence of side effects have been shown between both studied groups (P = 0.21).
DISCUSSION
The aim of the present study was to determine the prevalence rate of sexual dysfunction in the patients hospitalized in psychiatric wards in comparison with those patients in other wards. The results of the study were indicative of higher prevalence rate of sexual dysfunction in the patients of psychiatric wards compared to those in non-psychiatric wards. These results were in accord with the results of other studies, which have reported the prevalence rate of these dysfunctions to be higher in psychiatric patients.[9,10]
The higher rate of sexual dysfunction in psychiatric patients is influenced by different factors such as the type of medical and mental illness together with the drugs used, marital and relationship problems between the patients and their spouses, and cultural and social issues.[14,15]
As the causes of sexual dysfunctions are multi-factorial and due to using different tools to measure these dysfunctions, the rate of these dysfunctions in various studies has been reported from 17% to 80%.[8,16] Moreover, other studies exert an increase in the prevalence rate of mental disorders in those patients with sexual dysfunction. One third of the women and one fourth of the men, who, due to their sexual dysfunctions, were undergoing couples therapy, were diagnosed to develop at least a psychiatric disorder, mostly in the form of mood or anxiety disorders. In addition, two third of the men referring to an andrology clinic, also, have been suffering from psychiatric disorders.[17]
The higher rate of sexual dysfunction in women than in men has also been approved in other studies and one of the reasons, perhaps, is the higher prevalence rate of many of mental disorders, especially mood and anxiety disorders in women.[17,18,19] Compared to men, women cite their sexual problems to a lesser extent and try to look for the treatment. This may cause the chronicity of the problem and a vicious cycle of the sexual problem and mental disorder. In a study conducted on the women in two provinces of Iran, it has been shown that the prevalence of this disorder in women is significant. The women with sexual dysfunction, however, have received no therapeutic help. The most common cause of not referring to the healthcare system is that most of the women misbelieved that the disorder exists not only in them, but also in most women typically.[20,21]
The age group of 33 to 48 had the highest rate of sexual dysfunction. Considering the sex life of the people in this age group being more active than other people, the fact seems expectable. However, other studies have reported sexual dysfunction in the patients between 35 and 64 years old to be higher than in the patients between 18 and 34 years old.[16]
In the present study, there was a relationship between junior high school education level and sexual dysfunction, while some other studies show a direct association between the increase in the prevalence rate of sexual dysfunction and the people with higher education level.[16] On the other hand, lower education level and less information on sexual issues make the sufferers to refer and look for the treatment to a lesser extent.
The effect of various drugs, especially psychiatric ones, on sexual function cycle has been approved in different studies. Of different psychiatric drugs, selective serotonin reuptake inhibitors may play the most major role in this respect. It has to be mentioned that a decrease in interests in different areas such as in sexual desire is one of the obvious symptoms of depression. But, whenever a depressed patient starts to develop a dysfunction in sexual response cycle, clearly after using anti-depressants and compared to the state before using drugs, this is likely to be resulted from drug side effects.[22,23] The role of other psychiatric drugs, however, cannot be ignored in this respect.[24,25]
For now, those using psychiatric drugs, for instance anti-psychotics, anti-depressants, and hypnotics in particular, have complained about the higher rate of sexual dysfunction. Among non-psychiatric drugs, anti-hypertensive drugs have been in a significant association with sexual dysfunction, which has been confirmed in other studies.[26]
Of the patients hospitalized in non-psychiatric wards, 20.7% were developing sexual dysfunction, which existed more in cardiac patients. On the one side, different medical diseases, in particular those leading to Coronary Atherosclerosis, are of the common factors causing sexual dysfunctions.[27] On the other side, high accompaniment of medical diseases with mental illnesses such as depression may result in doubled impact of the two diseases on the patient's sexual function.[28]
This study has a number of limitations. First, absence of directly comparable studies makes it difficult to establish the validity of our findings. This study was a cross-sectional; nature of this study limits the possibility to explore the cause and effect relationship between sexual dysfunctions and psychiatric diagnosis. Also, some subjects did not complete the ASEX because they did not engage in sexual activity in the month previous to enrollment. Therefore, further studies with better design are needed to be done comparing groups of patients with sexual dysfunctions from different cultural backgrounds and assessing the effect of the duration of disease on sexual functions, which may provide more insight into abovementioned issues.
In conclusion, considering the remarkable prevalence of sexual dysfunctions in psychiatric patients and doubled undesired effects of those dysfunctions on the patients’ life quality, especially on their marital relationships, more attention is recommended to be paid to these dysfunctions in psychiatric patients. Doctors’ insufficient familiarity with the evaluation, diagnosis, and treatment methods of these dysfunctions, sexual issues not being cited by patients and not being asked about by doctors because of being considered as taboo, and referring to patients’ sexual dysfunctions as less important than medical and mental illnesses are all of the major reasons why these dysfunctions are not properly diagnosed and treated. Using psychiatric drugs with lower doses if efficient, diagnosing the drugs with the least side effects, effective drugs to treat these dysfunctions, and also applying non-pharmacological techniques can fall effective in preventing and decreasing the prevalence of these dysfunctions.
Footnotes
Source of Support: Isfahan University of Medical Sciences
Conflict of Interest: None declared.
REFERENCES
- 1.Rahmani A, Merghati E, Alah Gholi L. Sexual satisfaction and its relation to marital happiness in Iranians. Iranian J Publ Health. 2009;38:77–82. [Google Scholar]
- 2.Dunn KM, Corft PR, Halkett GI. Association of sexual problems with social, psychological and physical problems in men and women. Epidemiol Community Health. 1999;53:144–8. doi: 10.1136/jech.53.3.144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.4th ed. TR. Washington DC: APA; 2000. American Psychiatric Association Diagnostic and statistical manual of mental disorder. [Google Scholar]
- 4.World Health Organization. WHO The ICD-10 International classification of mental and behavioral disorder. 1992 [Google Scholar]
- 5.Laumunn EO, Nicolas A. Sexual problems among women and men 40-8- years’ prevalence and correlates identified in the global study of sexual attitudes and behavior. Int J Impot Res. 2005;17:39–57. doi: 10.1038/sj.ijir.3901250. [DOI] [PubMed] [Google Scholar]
- 6.Foroutan SK, Jadid Milani M. The prevalence of sexual dysfunction among divorce requested. Daneshvar. 2009;16:37–42. [Google Scholar]
- 7.Ghavami M, Tasbihsazan R. Prevalence and diversity of sexual dysfunction among male and female patients in family care clinic. Tehran-Iran. Usimia Med J. 2008;18:34–639. [Google Scholar]
- 8.Zemishlany Z, Weizman A. The impact of mental illness on sexual dysfunction. Adv Psychosom Med. 2008;29:89–106. doi: 10.1159/000126626. [DOI] [PubMed] [Google Scholar]
- 9.Bhui K, Puffet A, Herriot P. A survey of sexual problems among psychiatric inpatients. Soc Psychiatry Epidemiol. 1995;30:73–7. doi: 10.1007/BF00794946. [DOI] [PubMed] [Google Scholar]
- 10.Quinn C, Browne G. Sexuality of people living with a mental illness. Int J Ment Health Nurs. 2009;18:195–203. doi: 10.1111/j.1447-0349.2009.00598.x. [DOI] [PubMed] [Google Scholar]
- 11.Harley EW, Boardman J, Caring T. Sexual problems in schizophrenia. Soc Psychiatry Epidemiol. 2010;45:759–66. doi: 10.1007/s00127-009-0119-0. [DOI] [PubMed] [Google Scholar]
- 12.Mahiar A, Changiz A, Sima N. Sexual dysfunction and psychiatry status. Andisheh Raftar J. 2008;2:22–9. [in persian] [Google Scholar]
- 13.Bairami A, Satarzadeh N. Sexual dysfunction in women and its relation to pregnancy. Pregnancy J. 2008:272–7. [Google Scholar]
- 14.Qnek KF, Sallam AA, Chun CB. Prevalence of sexual problems and its association with social psychological and physical factors among men in Malaysian population. J Sex Med. 2005;5:70–76. doi: 10.1111/j.1743-6109.2006.00423.x. [DOI] [PubMed] [Google Scholar]
- 15.Laurent SM, Simons AD. Sexual dysfunction in depression and anxiety. Clin Psycholo Rev. 2009;29:673–85. doi: 10.1016/j.cpr.2009.06.007. [DOI] [PubMed] [Google Scholar]
- 16.Perlman CM, Martial L, Hirdes JP, Curtin-Telegdi N, Pérez E, Rabinowitz T. Prevalence and predictors of sexual dysfunction psychiatric inpatients. Psychomatic. 2007;48:309–18. doi: 10.1176/appi.psy.48.4.309. [DOI] [PubMed] [Google Scholar]
- 17.Wylie KR, Steward D, Seirewright N, Smit D, Walters S. Prevalence of sexual dysfunction in three psychiatric outpatient setting. Sex Relation Ther. 2002;17:149–61. [Google Scholar]
- 18.Rosen RC. Prevalence and risk factors of sexual dysfunction in men and women. Curr Psychiatry Rep. 2000;2:189–95. doi: 10.1007/s11920-996-0006-2. [DOI] [PubMed] [Google Scholar]
- 19.Read S, King M, Watson J. sexual dysfunction in primary medical care. Public Health Med. 1997;19:387–91. doi: 10.1093/oxfordjournals.pubmed.a024665. [DOI] [PubMed] [Google Scholar]
- 20.Vahdanini M, Montazeri A, Goshtasbi A. help seeking behavior for female sexual dysfunction: A cross survey from Iran. BMC Womens Health. 2009;9:3. doi: 10.1186/1472-6874-9-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bahraman SAM, Saki K. Sexual dysfunction in married women attending care centers in Khoram Abad, Iran. Iran J Endocrinol Metabol. 2000;1:294–8. [Google Scholar]
- 22.Osváth P, Fekete S, Vörös V, Vitrai J. Sexual dysfunction among patients treated with antidepressant. Eur Psychiatry. 2003;18:412–4. doi: 10.1016/j.eurpsy.2003.01.003. [DOI] [PubMed] [Google Scholar]
- 23.Clayton AH, Pradko JF, Croft HA, Montano CB, Leadbetter RA, Bolden-Watson C, et al. Prevalence of sexual dysfunction among newer antidepressant. J Clin Psychiatry. 2002;63:357–66. doi: 10.4088/jcp.v63n0414. [DOI] [PubMed] [Google Scholar]
- 24.Higgins A. Impact of psychotropic medication on sexuality. Br J Nurs. 2007;16:545–50. doi: 10.12968/bjon.2007.16.9.23433. [DOI] [PubMed] [Google Scholar]
- 25.Githn MJ. Psychotropic medication and their effects on sexual function: Diagnosis biology and treatments approaches. J Clin Psychiatry. 1994;55:406–13. [PubMed] [Google Scholar]
- 26.Blumentals WA, Brown PR, Gomez A. Antihypertensive treatment and erectile dysfunction in cohort type II diabet patients. Int J Impot Res. 2003;15:314–7. doi: 10.1038/sj.ijir.3901041. [DOI] [PubMed] [Google Scholar]
- 27.Lauman E, Paik A, Rosen R. Sexual dysfunction in US: Prevalence and predictors. JAMA. 1999;281:537–44. doi: 10.1001/jama.281.6.537. [DOI] [PubMed] [Google Scholar]
- 28.Roose SP, Seidman SN. Sexual activity and cardiac risk. Am J Cardiol. 2000;86:38–40. doi: 10.1016/s0002-9149(00)00891-2. [DOI] [PubMed] [Google Scholar]