

Abstract
Background:
Nurses constitute the most providers of health care systems. Their mental health can affect the quality of services and patients’ satisfaction. General Health Questionnaire (GHQ-12) is a general screening tool used to detect mental disorders. Scoring method and determining thresholds for this questionnaire are debatable and the cut-off points can vary from sample to sample. This study was conducted to estimate the prevalence of mental disorders among Iranian nurses using GHQ-12 and also compare Latent Class Analysis (LCA) and K-means clustering with traditional scoring method.
Methodology:
A cross-sectional study was carried out in Fars and Bushehr provinces of southern Iran in 2014. Participants were 771 Iranian nurses, who filled out the GHQ-12 questionnaire. Traditional scoring method, LCA and K-means were used to estimate the prevalence of mental disorder among Iranian nurses. Cohen’s kappa statistic was applied to assess the agreement between the LCA and K-means with traditional scoring method of GHQ-12.
Results:
The nurses with mental disorder by scoring method, LCA and K-mean were 36.3% (n=280), 32.2% (n=248), and 26.5% (n=204), respectively. LCA and logistic regression revealed that the prevalence of mental disorder in females was significantly higher than males.
Conclusion:
Mental disorder in nurses was in a medium level compared to other people living in Iran. There was a little difference between prevalence of mental disorder estimated by scoring method, K-means and LCA. According to the advantages of LCA than K-means and different results in scoring method, we suggest LCA for classification of Iranian nurses according to their mental health outcomes using GHQ-12 questionnaire
Keywords: Mental health, GHQ-12, Latent Class Analysis, K-means clustering, nurses, Iran
1. INTRODUCTION
Mental health, as the first rank in terms of causing disability compared to other diseases, is crucial in human’s life (1). Nevertheless, most of middle and low-income countries devote less than 1% of their health expenditure to mental health programs (2). About 13% of total global burden of disease in the year 2004 was mental, neurological and substance use disorders (3). Worldwide, about 450 million people suffer from mental, neurological or behavioral disorders, and nearly one-fifth of people will experience a mental disorder at least once a year (4, 5). Prevalence of mental disorders in Iran varies from 11.9% to 50.0% (6-8).
In recent years, prevalence of mental disorders has been systematically increased in various groups of population (3). Nurses constitute the most providers of health care system and their mental health can affect the quality of services and patients’ satisfaction. Nurses, working in psychiatric and emergency services wards, are especially in great risk of physical aggression and threats (9). Nursing is the most stressful profession among 130 jobs and ranked 27th among the 130 jobs with high prevalence of mental disorders (10). Nurses are confronted with a number of sources of stress, such as time pressure, long time work, shift work, sleep problems, visionary with the reality of death and malignant disease, high patients’ expectations from nurses, and a low tolerance for error (10, 11). Job stress in this profession could lead to disorders that seriously put nurses at risk of mental health disorders.
Mental health can be measured by different instruments such as General Health Questionnaire (GHQ), subscales Mental Health Inventory of the Short Form-36 (MHI-5), Strengths and Difficulties Questionnaire (SDQ), Minnesota Multiphasic Personality Inventory (MMPI), Affect Balance Scale (ABS), and Symptom Checklist (SC) (12). GHQ-12 consists of 12 items is one of the most well-known instruments that assess the severity of mental problems (minor psychiatric disorders) in the last month (13).
To determine the cut-off points for the scores of GHQ-12 based on the scoring method is challengeable and can vary according to region, population and time of study (13-16). Differences in the choice of cut-off points lead to different and sometimes contradictory results; however, scoring method is still the best and most popular method to detect mental disorder by GHQ-12.
In this study, we used the latent class analysis (LCA) and K-means, two competing methods to traditional scoring method, which are based on the nature of the data (e.g. responses to GHQ-12 questionnaire) and do not depend on the cut-off points. In both methods, allocation of objects to classes should be optimal according to some criteria. These criteria usually involve minimizing the within-cluster variation or, equivalently, maximizing the between-cluster variation. To the best of our knowledge, this is the first direct comparison without complicated mathematical details of these models in the applied mental health literature. The first objective of this study was to estimate the prevalence of mental disorders among Iranian nurses according to their mental health outcomes measured by GHQ-12 using three methods. The second objective was to compare LCA and K-means clustering with traditional scoring method.
2. METHOD
2.1. Sampling Method
This cross-sectional study was conducted on nurses working in the hospitals of southern (Fars and Bushehr provinces) Iran, in 2014. Data were collected by means of questionnaires from 771 nurses who were selected through multi-stage cluster sampling. Simulation study shows that the sample sizes with more than 500 individual have enough power to fit LCA (17)702151</custom2></record></Cite></EndNote>. Forty seven hospitals of 20 cities (out of 39) of Fars and Bushehr provinces were selected randomly. Proportional to the number of nurses working in each hospital, they were invited to participate in our study.
2.2. Instrument Study
The bimodal GHQ score method (item as 0-0-1-1) was used to score the questionnaires. In Iran, studies have shown that this method is useful (14). A participant could score between 0 and 12 and score of cut-off point or higher shows the one who might have mental disorder. In Iran, according to region, population and time of study, two cut-off points of 3.7 and 4 are most commonly used for threshold (14, 18). The reported Cronbach’s alpha coefficient for the GHQ-12 in Iran was calculated as 0.87 (14).
2.3. Data analysis
Data were analyzed in the following phases: 1) descriptive analysis (mean±SD, and proportions) was performed to examine the distributions of the variables and t-student, analysis of variance and logistic regression was used to compare GHQ-12 score in subgroups and to evaluate independent variables (gender, marital status, education, age and work experience); 2) To cluster mental health level of nurses using traditional scoring method of GHQ-12, LCA and K-means 3) To measure agreement between LCA and K-means with traditional scoring method of GHQ-12.
LCA is another method to classify each nurse into a latent class whose members report similar patterns of responses (GHQ-12). LCA is an analytical method that models the relationship between categorical observed variables and a categorical latent variable (19). LCA enables investigators to classify individuals into latent classes that are mutually exclusive (i.e. each class is conceptually different from the others) and exhaustive (i.e. all response patterns are accounted for and grouped into a class) (19). Latent Class Regression (LCR) was used to assess the association between latent class membership and each of the covariates using bivariate models and demographic adjusted models. The LCR is a generalization of the LCA in which a covariate for optimizing latent classes and evaluating the effect of classification is entered into the model. LCR assumes both conditional independence and non-differential measurement; within class, the measured indicators are non correlated with each other, and the covariates do not influence the indicators given class membership, respectively (19).
K-means was used to cluster the nurses based on mental health level into k (in this study k=2) groups. K-means, a typical partitioned clustering method with minimum required assumptions, is simple and generally very fast. This is a data-driven method that partitions a set of points into clusters and the distance between the members of each cluster is minimized while the distance between the members of different clusters is maximized. The most generally used distance measure is the squared Euclidean distance variables (20). We used k-means with two classes based on comparability and interpretability.
The agreement between LCA and K-means with traditional scoring method of GHQ-12 was estimated by calculating the percentage of agreement and Cohen’s Kappa coefficient. The agreement was interpreted none to slight when the calculated values ranged between 0.01–0.20, fair between 0.21–0.40, moderate between 0.41– 0.60, substantial between 0.61–0.80, and 0.81–1.00 as almost perfect agreement. Negative values and zero indicate no agreement (21).
All analyses were performed using SPSS for windows© (SPSS Inc., Chicago, IL) and package poLCA in R software. P-value of less than 0.05 was considered as significant.
3. RESULTS
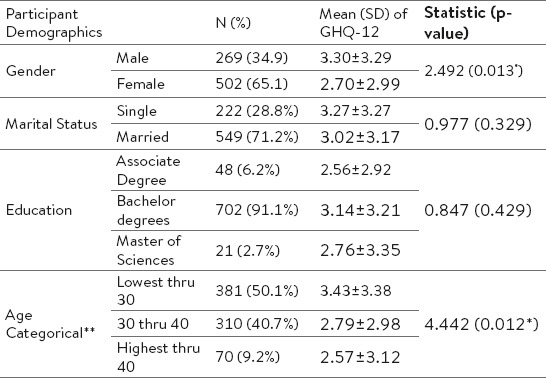
The mean±SD of age was estimated as 32.06±6.28 years. The total number of years of work experience among nurses was 7.74±5.79. Over 65% (n=502) of the nurses were women. The majority had at least Bachelors’ degree. The mean GHQ-12 score was 3.09±3.20. There were significant differences between nurses’ GHQ-12 scores regarding the categorical age and gender (p-value=0.012). Table 1 summarizes the demographic characteristics of participants and descriptive findings. From total number in our sample, 36.3% (n=280) of the nurses scored above 3.7 and 26.6% (n=205) above 4 threshold.
Table 1.
The mean of GHQ-12 score is based on scoring method. *significant at 5% ** significant differences between Lowest thru 30 and 30 thru 40 years (p-value for Tukey HSD: 0.025)
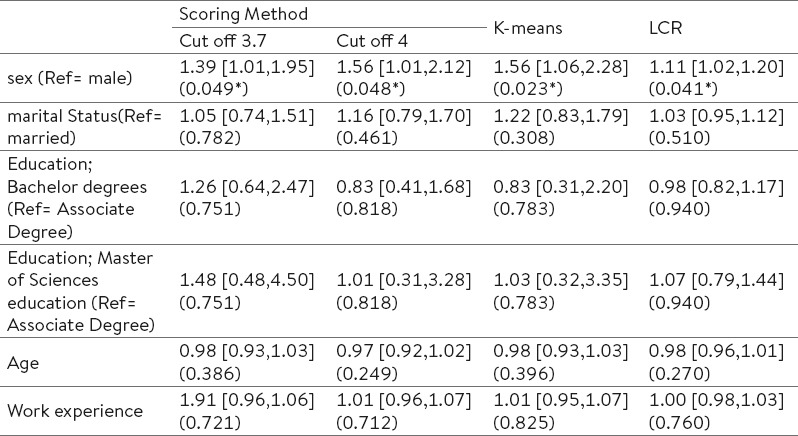
We used LCA with two classes based on Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC) criterion, and interpretability. LCR, logistic regression analysis based on scoring method and k-means clustering indicated that gender was significant among independent variables in predicting mental disorder among nurses. Female nurses had 0.39, 0.56, 0.56 and 0.11 times more probability than men of detecting mental disorder based on scoring method with 3.7, 4 threshold, k-means and LCR, respectively. The results are shown in Table 2.
Table 2.
Result logistic regression based on scoring method, K-means and LCR; OR [95% CI] (p-value). *significant at 5%
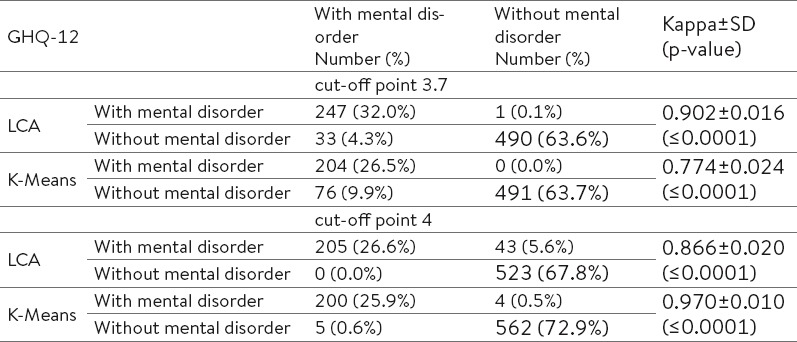
The nurses with mental health by scoring method, LCA and K-mean were 36.3% (n=280), 32.2% (n=248), and 26.5% (n=204), respectively. If the cut-off point in scoring method was 3.7, the Cohen’s Kappa coefficient between LCA with traditional scoring method (0.902) indicated the perfect agreement and between K-means with traditional scoring (0.774) indicated substantial agreement. With 4 as the cut-off point, there were almost perfect agreement between the clustering methods and traditional scoring method. Table 3 provides more detailed information about it.
Table 3.
Compare agreement LCA and K-means with scoring method
4. DISCUSSION
Mental disorder in nurses will result in decreased quality of health care system. So, estimating the prevalence of mental disorder in nurses leads to some attempts to prevent decreasing the quality of services. In this study, we estimated the prevalence of mental disorders among Iranian nurses using GHQ-12 and we compared LCA and K-means clustering with traditional scoring method.
The results showed that mental disorder in nurses was in the medium level in Iran (6-8, 22, 23). These results are similar to those reported by Najimi and his colleagues (10). As compared with the previous research, when the cut-off point in scoring method was 3.7, the prevalence rate in this survey (36.3%) was lower than in Nigeria (40.7%) and England (41%) but higher than those obtained by Tasmania (34%) and Wales (35.0%) surveys (24-27).
Several types of regression analysis show that females were more likely than men to have a mental disorder. According to physical and mental structure of women, females have higher rates of psychological distress, depression, and physical morbidity than men. Also, female nurses are affected by uncomfortable circumstances in hospitals. In almost all studies, the effect of gender has been demonstrated on mental health (6-8, 12, 24, 28). Nursing is a profession that requires a college education. However, its association with mental disorders was not significant in this study. One reason might be that nurses had mostly (91.1%) undergraduate degree. In a similar study on nurses, the level of education affected physical and environmental dimensions with no effect on the mental dimension (29). In our study, the effects of age, work experience and marital status were not significant and this is a contradictory result in different studies (6-8, 12, 24). Three variables mentioned are highly interdependent. Iranian nurses generally are young (83.6% between the ages of 25 and 40 years) and interpretation of our findings is slightly restricted because of the particularly selective nature of the investigated sample.
Differences in methods and instruments for screening used as well as different classification systems, time, age groups, regions and the population under the study may account for differences in results. Our results show that different cut off points (3.7 and 4) produced different estimations for the prevalence of mental disorders in nurses. Many different techniques have been developed to discover homogeneous groups (classes), e.g. cluster analysis. Some of clustering methods play a significant role in scientific studies, and in the case of practical applications (e.g. LCA and K-means method).
In the traditional method, logistic regression should be used after classification if the researcher is interested in studying the effect of independent variables. In LCR, the latent class (classification of nurses according to their mental health outcomes using GHQ-12) and regression components of the model are estimated simultaneously in order to reduce measurement error (30). Prevalence of mental disorders based on proposed methods vary from 26.5 to 36.3 percent. However, several regression analyses revealed the same results about the relationship between covariates and mental disorder classes.
Using the two cut-off point in scoring method, we achieved different results of prevalence of mental disorders in nurses. But, the used clustering methods are based on the data and do not depend on the thresholds. In other hand, LCA is model-based method can estimate and test the parameters and the number of classes was based on objective criteria. The k-means algorithm is completely non-parametric and does not take advantage of any valid parametric assumptions. Given the limitations of the k-means method such as scale-dependent, lack of goodness of fit indices, dependence on the starting value, clusters must be linearly separable and using the results of previous studies that showed LCA fitting a model better than K-means (31-36). According to the above mentioned advantages of the LCA than K-means and different results in scoring method we suggest LCA for classification of Iranian nurses according to their mental health outcomes using GHQ-12 questionnaire. The agreement between LCA and K-means with scoring method was depended the cut-off point. Our result showed that a little difference between prevalence of mental disorder estimated by scoring method, K-means and LCA.
In summary, this study used traditional scoring method, LCA and K-means clustering to estimate the prevalence of mental disorders among Iranian nurses. Agreement LCA and K-means clustering with traditional scoring method were acceptable. However, our results showed that choosing different cut off points could affect the agreement between the LCA and K-means with a scoring method. Statistical basics supported that LCA had a better fit than K-means. Measurement error in LCR was less than traditional method (classify by scoring method and assessment by logistic regression) to evaluate the effect of variables on mental disorder. GHQ scores in our study were higher than adult general population in Iran (8). One reason could be job stress, shift working, and sleeping disorders among nurses.
Abbreviations
- GHQ:
General Health Questionnaire
- LCA:
Latent Class Analysis
- LCR:
Latent Class Regression
Acknowledgements
We would like to thank the nurses who participated in the study. The authors would also like to thank Research Consultation Centre (RCC) and Mr. Erfan Sadeghi for his kindly editing services to this paper.
Footnotes
CONFLICT OF INTEREST: NONE DECLARED.
REFERENCES
- 1.World Health Organization. The Global Burden of Disease. 2004. Available from: http://www.who.int/topics/global_burden_of_disease/en/
- 2.World Health Organization. WHO urges more investments, services for mental health. 2014. Available from: http://www.who.int/mental_health/who_urges_investment/en/
- 3.Mental health action plan 2013–2020. Geneva, Switzerland: WHO Document Production Services; 2013. World Health Organization. [Google Scholar]
- 4.Whiteford HA, Degenhardt L, Rehm J, Baxter AJ, Ferrari AJ, Erskine HE, et al. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. Lancet. 2013;382(9904):1575–1586. doi: 10.1016/S0140-6736(13)61611-6. [DOI] [PubMed] [Google Scholar]
- 5.World Health Organization. Global health risks: mortality and burden of disease attributable to selected major risks: World Health Organization. 2009 [Google Scholar]
- 6.Jafari N, Loghmani A, Montazeri A. Mental health of medical students in different levels of training. International journal of preventive medicine. 2012;3(Suppl 1):S107–112. [PMC free article] [PubMed] [Google Scholar]
- 7.Emami H, Ghazinour M, Rezaeishiraz H, Richter J. Mental health of adolescents in Tehran, Iran. The Journal of adolescent health: official publication of the Society for Adolescent Medicine. 2007;41(6):571–576. doi: 10.1016/j.jadohealth.2007.06.005. [DOI] [PubMed] [Google Scholar]
- 8.Noorbala AA, Bagheri Yazdi SA, Yasamy MT, Mohammad K. Mental health survey of the adult population in Iran. The British journal of psychiatry: the journal of mental science. 2004;184:70–73. doi: 10.1192/bjp.184.1.70. [DOI] [PubMed] [Google Scholar]
- 9.Magnavita N, Heponiemi T. Violence towards health care workers in a Public Health Care Facility in Italy: a repeated cross-sectional study. BMC health services research. 2012;12:108. doi: 10.1186/1472-6963-12-108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Najimi A, Goudarzi AM, Sharifirad G. Causes of job stress in nurses: A cross-sectional study. Iranian journal of nursing and midwifery research. 2012;17(4):301–305. [PMC free article] [PubMed] [Google Scholar]
- 11.Rutledge T, Stucky E, Dollarhide A, Shively M, Jain S, Wolfson T, et al. A real-time assessment of work stress in physicians and nurses. Health psychology: official journal of the Division of Health Psychology, American Psychological Association. 2009;28(2):194–200. doi: 10.1037/a0013145. [DOI] [PubMed] [Google Scholar]
- 12.Hoeymans N, Garssen AA, Westert GP, Verhaak PF. Measuring mental health of the Dutch population: a comparison of the GHQ-12 and the MHI-5. Health and quality of life outcomes. 2004;2:23. doi: 10.1186/1477-7525-2-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Goldberg DP, Gater R, Sartorius N, Ustun TB, Piccinelli M, Gureje O, et al. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychological medicine. 1997;27(1):191–197. doi: 10.1017/s0033291796004242. [DOI] [PubMed] [Google Scholar]
- 14.Montazeri A, Harirchi AM, Shariati M, Garmaroudi G, Ebadi M, Fateh A. The 12-item General Health Questionnaire (GHQ-12): translation and validation study of the Iranian version. Health and quality of life outcomes. 2003;1:66–69. doi: 10.1186/1477-7525-1-66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Newman SC, Bland RC, Orn H. A comparison of methods of scoring the General Health Questionnaire. Comprehensive psychiatry. 1988;29(4):402–408. doi: 10.1016/0010-440x(88)90021-1. [DOI] [PubMed] [Google Scholar]
- 16.Shelton NJ, Herrick KG. Comparison of scoring methods and thresholds of the General Health Questionnaire-12 with the Edinburgh Postnatal Depression Scale in English women. Public health. 2009;123(12):789–793. doi: 10.1016/j.puhe.2009.09.012. [DOI] [PubMed] [Google Scholar]
- 17.Dziak JJ, Lanza ST, Tan X. Effect Size, Statistical Power, and Sample Size Requirements for the Bootstrap Likelihood Ratio Test in Latent Class Analysis. Structural Equation Modeling: A Multidisciplinary Journal. 2014;21(4):534–552. doi: 10.1080/10705511.2014.919819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Roohafza H, Ramezani M, Sadeghi M, Shahnam M, Zolfagari B, Sarafzadegan N. Development and validation of the stressful life event questionnaire. International journal of public health. 2011;56(4):441–448. doi: 10.1007/s00038-011-0232-1. [DOI] [PubMed] [Google Scholar]
- 19.Tarpey T, Petkova E. Latent Regression Analysis. Statistical modelling. 2010;10(2):133–158. doi: 10.1177/1471082X0801000202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Gan G, Ma C, Wu J. Data Clustering: Theory, Algorithms, and Applications. Philadelphia, PA: SIAM, Society for Industrial and Applied Mathematics; 2007. [Google Scholar]
- 21.McHugh ML. Interrater reliability: the kappa statistic. Biochemia medica. 2012;22(3):276–282. [PMC free article] [PubMed] [Google Scholar]
- 22.Noorbala A, Mohammad K, BagheriYazdi A, Yasamy M. A view of mental health in Iran. Tehran: Moalef; 2001. [Google Scholar]
- 23.Roustaei N, Ayatollahi SMT, Jamali J. Relationship between Minor Psychiatric Disorders and Job Stability among Southern Iranian Nurses: Using Latent Class Regression Model. Hayat. 2014;20(4):47–57. [Google Scholar]
- 24.Lasebikan VO, Oyetunde MO. Burnout among Nurses in a Nigerian General Hospital: Prevalence and Associated Factors. ISRN nursing. 2012:402157. doi: 10.5402/2012/402157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Fagin L, Brown D, Bartlett H, Leary J, Carson J. The Claybury Community Psychiatric Nurse Stress Study: is it more stressful to work in hospital or the community? Journal of advanced nursing. 1995;22(2):347–358. doi: 10.1046/j.1365-2648.1995.22020347.x. [DOI] [PubMed] [Google Scholar]
- 26.Farrell GA. The mental health of hospital nurses in Tasmania as measured by the 12-item General Health Questionnaire. Journal of advanced nursing. 1998;28(4):707–712. doi: 10.1046/j.1365-2648.1998.00735.x. [DOI] [PubMed] [Google Scholar]
- 27.Edwards D, Burnard P, Coyle D, Fothergill A, Hannigan B. Stressors, moderators and stress outcomes: findings from the All-Wales Community Mental Health Nurse Study. Journal of psychiatric and mental health nursing. 2000;7(6):529–537. doi: 10.1046/j.1365-2850.2000.00359.x. [DOI] [PubMed] [Google Scholar]
- 28.Jamali J, Roustaei N, Taghi Ayatollahi SM, Sadeghi E. Factors Affecting Minor Psychiatric Disorder in Southern Iranian Nurses: A Latent Class Regression Analysis. Nurs Midwifery Stud. 2015;4(2):e28017. doi: 10.17795/nmsjournal28017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Soric M, Golubic R, Milosevic M, Juras K, Mustajbegovic J. Shift work, quality of life and work ability among Croatian hospital nurses. Collegium antropologicum. 2013;37(2):379–384. [PubMed] [Google Scholar]
- 30.Bandeen-Roche K, Miglioretti DL, Zeger SL, Rathouz PJ. Latent variable regression for multiple discrete outcomes. J Amer Stat Asso. 1997;92(440):1375–1386. [Google Scholar]
- 31.Fahey MT, Thane CW, Bramwell GD, Coward WA. Conditional Gaussian mixture modelling for dietary pattern analysis. J Roy Stat Soc A STA. 2007;170(1):149–166. [Google Scholar]
- 32.Magidson J, Vermunt J. Latent class models for clustering: A comparison with K-means. Can J Marketing Res. 2002;20(1):36–43. [Google Scholar]
- 33.Xu B, Recker M, Qi X, Flann N, Ye L. Clustering Educational Digital Library Usage Data: A Comparison of Latent Class Analysis and K-Means Algorithms Journal of Educational Data Mining. 2013;5(2):38–68. [Google Scholar]
- 34.MacQueen J, editor. Proc of the fifth Berkeley Symposium on Mathematical Statistics and Probability. California, USA: University of California Press; Some methods for classification and analysis of multivariate observations; p. 1967. [Google Scholar]
- 35.Wagstaff K, Cardie C, Rogers S, Schrödl S. Constrained k-means clustering with background knowledge. ICML. 2001 [Google Scholar]
- 36.Dragovic M. Categorization and validation of handedness using latent class analysis. Acta Neuropsychiatrica. 2004;16(4):212–218. doi: 10.1111/j.0924-2708.2004.00087.x. [DOI] [PubMed] [Google Scholar]