

Abstract
Introduction:
A great number of clinical studies has indicated that the patients with calcium urolithiasis have a reduced mineral bone density.
Aim:
The aim of our research was to establish representation of osteoporosis, by measuring mineral bone density using the DEXA method, in patients with calcium urolithiasis, by gender.
Material and methods:
The research was a prospective one, performed at the University Hospital of the Clinical Center of Banja Luka, at the Urology Clinic and Clinic for Endocrinology, Diabetes and Metabolic Diseases. The material in this research were the patients divided into two groups: a working group (the patients suffering from calcium urolithiasis) and a control group (the patients without calcium urolithiasis). One hundred and twenty (120) patients were included in both these groups, divided in three age subgroups: 20-40, 40-60 and over 60. The total working group consisted of 63 men (52.2%) and 57 (47.5%) women. In the control group, the number of women was 72 (60%) and 48 (40%) of men. Establishing of mineral bone density at L2-L4 of lumbal spine vertebrae and hip was done for the patients in both these groups, using DEXA method.
Results:
Analysis of mineral bone density using DEXA method in patients by gender of working and control groups has shown that osteoporosis and osteopenia in patients of the working group is significantly more present in women (14% and 22.8%) compared to men (1.6% and 17.5%). When compared by gender in the control group, osteoporosis was present a lot more in women (36.1%) compared to men (2.1%). When observed for the total sample of both the working and control group, there was a statistically significant difference (p<0,01) related to gender structure, where the share of women with osteoporosis/osteopenia was significantly higher (36.1%) compared to men (4.2%).
Conclusion:
Representation of osteoporosis in women with urolithiasis, particularly of older age, is very expressed and this is why prevention measures should start as soon as possible, so as to avoid severe complications of this illness.
Keywords: Osteoporosis; urolithiasis,DEXA
1. INTRODUCTION
Osteoporosis and urolithiasis are two pathological entities presenting today all the more significant place in the epidemiological sense, for the reason of increased incidence rate and recidivism. As metabolic and chronic diseases, they are characterized with high morbidity and complications that may easily be followed with high mortality, a severe degree of disability, particularly in older population, which has significant medical, economical and social consequences to individuals and the overall society (1-4). Clinical research have discovered an increased bone disintegration and lower bone mass in the patients with urolithiasis, particularly when it comes to idiopathic calcium urolithiasis. Women in menopause are in a much higher risk to suffer because of a negative balance of calcium and reduced level of estrogen compared to men (5-8). Pathogenic mechanisms, which are connected to the occurrence of these diseases, are still in the phase of clinical research (9, 10). It is necessary to develop consciousness of the population about the risk factors related to the occurrence of these diseases and prevention measures that may contribute to their reduction (11).
2. RESEARCH AIM
Having in mind a great significance of these diseases, the aim of this work was to evaluate representation of osteoporosis, as established by the DEXA method, in patients with calcium osteoporosis with a special reflection onto the patients’ gender.
3. MATERIAL AND METHODS
The research was a prospective one and it was performed at the University Hospital of the Clinical Center of Banja Luka, at the Urology Clinic and Clinic for Endocrinology, Diabetes and Metabolic Diseases. The material in this research consisted of the patients divided into three age sub-groups: 20-40, 40-60 and over 60. Ultrasonography was done for all the patients and the patients with ultrasonography findings, establishing urolithiasis, were candidates for the working group. They underwent additional diagnostic procedures of native X-ray scans of the urinary tract, intravenous urography and laboratory checks. Excluding factors were increased value of uric acid (uric stones), infectious (struvite) calculosis, taking of biophosphonates, hyperparathyroidism, the patients with malign diseases who were receiving hormone therapy (Ca of the prostate, Ca of the breast). The control group consisted of the population of patients, for whom, using initial ultrasound diagnostics, it was established that they do not suffer from urolithiasis. After that, the patients of the working and control group underwent densitometry using the instrument LUNAR DPX Product Division Americus GE Healthcare (GENERAL ELECTRIC COMPANY 2006), with the aim to measure mineral bone density, DXA L2-L4 of the lumbal spine and hip – upper part of the femur, including the femur neck.
4. RESULTS
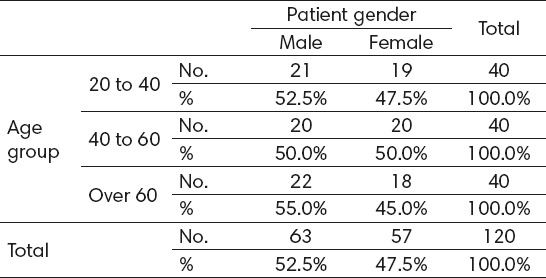
Demographically observed, in the working group of 120 patients there were 40 persons in the three age categories: 20-40, 40-60 and over 60. The share of men was 52.5% and the share of women was 47.5%. Namely, the total number of men in the working group was 63, whereas the total number of women was 57, with an average age of 50.19.
By age and gender structure, the patients of the working group are shown in Table 1.
Table 1.
Distribution of patients by age and gender structure (working group)
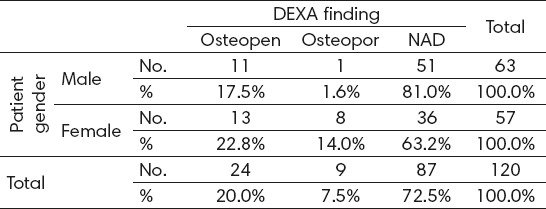
Having analyzed the obtained results for the working group patients, by age structure, osteoporosis was more represented in women (14%) compared to men (1.6%). A higher representation of osteopenia was also found in women and it amounts to 22.8% compared to men, that of men being 17.5%. NAD results of the DEXA finding in women was also lower (63.2%) compared to that of men (81.0%), which was shown in Table 2.
Table 2.
Results of the DEXA finding by gender (working group)
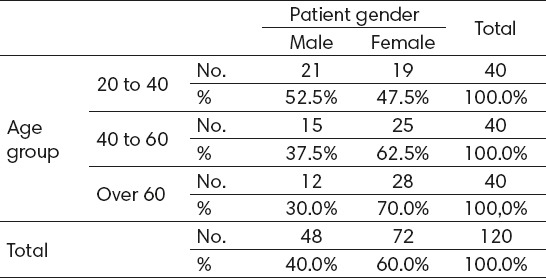
When observed in the total sample of the control group, where the patients, just as in the working group, were divided into three age categories (20-40, 40-60 and over 60), each having 40 patients, the share of women was somewhat higher, 60% (72 women), whereas the share of men was 40% (48 men), Table 3.
Table 3.
Distribution of patients by age and gender structure (control group)
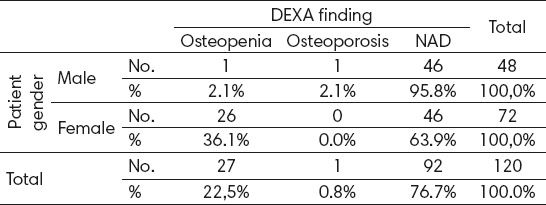
Having analyzed the control group results, by gender structure, representation of osteopenia is much more expressed in women 36.1% compared to men being 2.1%; osteoporosis was present in 2.1% men and 0.0% women. Still, generally, because of predomination of osteopenia in women, NAD results of DEXA finding in women in also lower (63.9%) compared to men (95.8%), Table 4.
Table 4.
Results of the DEXA findins by gender (control group)
Having observed the total sample of the working and control group, there was a statistically significant difference by gender representation of osteopenia and osteoporosis in women compared to men, that is, statistically, there was a much higher share of men with an NAD finding of DEXA, than it was the case with women, which is confirmed by the relation (p< 0.01).
5. DISCUSSION
Reference data confirm that clinical and epidemiological research have discovered in older patients with urolithiasis an increased bone remodeling and reduced mineral bone density (BMD). The reduced BMD is also supported by epidemic studies, which have shown that women in menopause with urolithiasis had a significantly higher incidence of low mineral bone density compared to male population, i.e. higher degrees of fracture compared to the control, primarily male, population (12). It is considered that a limited input of calcium in food and its increased loss through the kidney work contributes to the occurrence of osteopenia/osteoporosis (13). An additional problem in women, especially of older populations, presents a negative calcium balance, which is, during the menopause, doubled, as well as a surplus of hormones, such as parathyroid hormone (PTH) as well as a reduced estrogen level. All this may cause the loss of calcium with a consequential creation of calcium stones as well as increase of reduced mineral bone density (BMD) and development of osteopenia and osteoporosis of patients (14-16).
In line with the previously expressed positions and having analyzed the data of own research, our study has shown that in the total sample of the working group, by age structure, the representation of osteopenia/osteoporosis was much higher in women (22.8%, 14%) compared to men (17.5%, 1.6%); namely, NAD results of DEXA finding was much higher in men being 81% compared to that of women being 63.2%, which presents a statistically significant difference.
Having analyzed the obtained results of the DEXA finding in the control group of our study, by age representation, we can see that the share of women with osteopenia (36.1%) compared to men (2.1%), is significantly higher, which presents a statistically significant difference. Namely, NAD results of DEXA findings were much higher in men being 95.8% compared to women 63.9%.
6. CONCLUSION
On the whole, the results of the implemented research confirm that representation of osteoporosis is much higher in women suffering from urolithiasis than in men. This is why prevention and adequate therapy are very significant components that should be undertaken as early as possible in order to avoid severe complications and consequences of these diseases.
Footnotes
CONFLICT OF INTEREST: NONE DECLARED.
REFERENCES
- 1.National Osteoporosis Foundation. Clinican's Guide to Prevention and Treatment of Osteoporosis. 2008. Available from:http:/www.nof.org./hcp/practice/ practice-and-clinical-guide-lines/clinicians-giude .
- 2.Milicevic S, Bijelic R, Krivokuca V, Bojic M, Popovic-Pejicic S, Bojanic N. Correlation of the Body Mass Index and calcium nephrolithiasis in adult population. Med Arh. 2013 Dec;67(6):417–421. doi: 10.5455/medarh.2013.67.423-427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wictorowicz ME, Goeree R, Papaioannou A, et al. Economic implications of hip fracture: health service use, institutional care and cost in Canada. Osteoporosis Int. 2001;12:271–278. doi: 10.1007/s001980170116. [DOI] [PubMed] [Google Scholar]
- 4.Lazić M, Spasojević G. Značaj kvantitativne ultrazvučne osteodenzitometrije u ranom otkrivanju osteoporoze. Biomedicinska istraživanja. 2012;3(2):18–25. [Google Scholar]
- 5.Li HL, Zhu HM. Relationship between the age of menarche, menopause and other factors and postmenopause osteoporosis. Zhonghua Fu Chan Ke Za Zhi. 2005;40:796–798. [PubMed] [Google Scholar]
- 6.Basiri A, Shakhssalim N, Knoshdel AR, et al. Familiar relations and recurrence pattern in nephrolithiasis: new words about old subjects. Urol. 2010 Jun 10;7(2):81–86. [PubMed] [Google Scholar]
- 7.Maalouf NM, Sato AH, Welch BJ, et al. Postmenopausal hormone use and the risk of nephrolithiasis: results from the Women's Health Initiative hormone therapy trials. Arch. Intern. Med. 2010;170(18):1678–1685. doi: 10.1001/archinternmed.2010.342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gallagher JC. Role of estrogens in the management of postmenopauzal bone loss. Rheum Dis Clin North Am. 2001;27:143–162. doi: 10.1016/s0889-857x(05)70191-5. [DOI] [PubMed] [Google Scholar]
- 9.Trinchieri A. Bone mineral content in calcium renal stone formers. Urol Res. 2005;33:247–253. doi: 10.1007/s00240-005-0498-y. [DOI] [PubMed] [Google Scholar]
- 10.Jakobsen A, Laurberg P, Vestergaard P, Andersen S. Clinical risk factors for Osteoporosisare common among erderly people in Nuuk, Greenland. Int J Cirkumpolar Health. 2013;72:195–196. doi: 10.3402/ijch.v72i0.19596. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Osteoporosis Foundation National. Washington DC: National Osteoporosis Foundation; 2010. Clinician's guide to prevention end treatment of osteoporosis. [Google Scholar]
- 12.Arrabal-Polo MA, Arrabal-Martin M, de Haro-Munoz T, et al. Mineral density and bone remodeling markers in patients with calcium lithiasis. BJU Int. 2010;108:1903–1908. doi: 10.1111/j.1464-410X.2011.10167.x. [DOI] [PubMed] [Google Scholar]
- 13.Sorensen MD, Chi T, Shara NM, Wang H, Hsi RS, Orchard T, Kahn AJ, Jackson RD, Miller J, Reiner AP, Stoller ML. Activity, energy intake, obesity, and the risk of incident kidney stones in postmenopausal women: a report from the Women's Health Initiative. J Am Soc Nephrol. 2014;25:362–369. doi: 10.1681/ASN.2013050548. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Heilberg IP, Weisinger JR. Bone disease in idiopathic hypercalciuria. Curr Opin Nephrol Hypertens. 2006;15:394–402. doi: 10.1097/01.mnh.0000232880.58340.0c. [DOI] [PubMed] [Google Scholar]
- 15.Milicevic S, Bijelic R, Jakovljevic B. Correlation of Parathormone and the Serum Values of Acidum Uricum with Calcium Nephrolithiasis Examined by Three Different Methods of Diagnostics. Acta Inform Med. 2015 Jun;23(3):132–134. doi: 10.5455/aim.2015.23.132-134. doi:10.5455/aim.2015.23.132-134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bijelic R, Milicevic S, Balaban J. Incidence of Osteoporosis in Patients with Urolithiasis. Med Arch. 2014 Oct;68(5):335–338. doi: 10.5455/medarh.2014.68.335-338. doi:10.5455/medarh.2014.68.335-338. [DOI] [PMC free article] [PubMed] [Google Scholar]