

Abstract
Purpose:
To explore the quality of life in hemodialysis patients.
Material and Methods:
The sample studied consisted of 320 patients undergoing hemodialysis in one-day dialysis center. Data were collected by the completion of a specially designed questionnaire which apart from the sociodemographic and clinical variables, it also included the scale Missoula-VITAS Quality of Life Index (MVQOLI) for assessing quality of life.
Results:
Of the 320 hemodialysis patients, 57,2% were men while 28,1% of the participants were 71-80 years old. The average total score of quality of life was found to be 17.43 (in a range 0-30). The total score of quality of life was found to be higher in participants <60 years (p= 0,009), of higher educational level (p=0.001), being very informed about the health problem (p=0,013), complied with therapeutic recommendations and the proposed diet (p=0,025 & p=0,012, respectively), having very good relations with the medical and nursing staff or other patients (p<0,001), not experiencing difficulties with social or family environment (p=0,001), had help at home (p <0,001) and in those who did not conceal their health problem from the social environment (p<0.001). Furthermore, it was found that the increasing duration of hemodialysis session entailed poorer quality of life (p<0,001). These results were largely confirmed by multiple linear regression.
Conclusions:
Sociodemographic and clinical characteristics seems to influence the quality of life in hemodialysis patients.
Keywords: hemodialysis, quality of life, sociodemographic characteristics
1. INTRODUCTION
End stage renal failure is a chronic disease that exerts a great negative impact on patients’ health-related quality of life mainly due to the accompanied impairment or to the imposed limitations in almost all domains of their daily lives.(1, 2)
Hemodialysis consists a complex procedure for patients that requires frequent hospital or dialysis centers visits, mainly three times a week, thus implying substantial changes in the normal way of patients’ living.(4-7)
Assessment of health-related quality of life is a predictive indicator of the outcome of the disease as well as a valuable research tool in assessing the effectiveness of therapeutic intervention, patients’ survival and hospitalizations.(1, 2)
The aim of the present study was to explore the quality of life of Hemodialysis patients
2. MATERIALS AND METHODS
2.1. Participants
The sample of the present study consisted of 320 patients (183 men and 137 women) undergoing hemodialysis. This sample was a convenience sample. The study included all patients undergoing HD at dialysis centers during the period January 2015– March 2015. Participants were selected according to the following criteria: a) diagnosis of end-stage renal disease, b) current hemodialysis treatment, c) native language-Greek, d) age above 20 and 5) volunteer participation.
Patients who met the entry criteria, gave their consent after having being informed by the researcher about the purpose of the research. All participants were informed of their rights to refuse or discontinue their participation, according to the ethical standards of the Helsinki Declaration of 1983. The study was approved by the Medical Research Ethics Committee of each center.
2.2. Data-Variables
Data were collected by the completion of a specially designed questionnaire which apart from the sociodemographic and clinical variables, it also included the scale Missoula-VITAS Quality of Life Index (MVQOLI) was completed for assessing quality of life.
2.3. Assessment of Quality of life
The scale Missoula-VITAS Quality of Life Index-15 (MVQOLI-15) was used for the assessment of quality of life (QoL). This scale 15 questions has been translated and cultural adapted in Greek people by Theofilou et al, (Cronbach’s alpha 0.74) (8). The questionnaire consisted of five dimensions: symptoms, functioning, interpersonal relationships, wellness, spirituality. In each area, three types of information were collected in:
(a) Evaluation (subjective measurement of the actual situation or state) (b) Satisfaction (degree of acceptance or knowledge of the actual state) (c) Significance (the degree to which a given dimension has an impact on the overall quality of life).
Questions of each dimension expressing “evaluation” graded on a 5-point Likert scale from -2 to +2. Questions expressing “satisfaction” rating from -4 to +4 and questions that reflect the “significance” rating from 1-5.
To assess the total score of each dimension of QoL, scores of ‘’evaluation’’ and ‘’satisfaction’’ are added. Then, this sum multiply by the score of ‘’significance’’ (evaluation + satisfaction) x significance). The score of each dimension express the degree to which the particular dimension affects the QoL of patients. The higher total score the highest level of QoL.
2.4. Statistical analysis
Normality test of continuous variables were carried using Kolmogorov-Smirnov criterion. The categorical data were presented in absolute and relative (%) frequencies, while continuous data were presented with mean values, with ± standard deviations when they followed a normal distribution and median (interquartile range) when they did not follow the normal curve.
One –way ANOVA test was used in order to control the correlation between a quantitative continuous variable which followed the normal curve and a qualitative variable with > 2 categories. Kruskal-Wallis test was used for controlling the correlation between a quantitative continuous variable that did not follow the normal curve and a qualitative variable with > 2 categories. The problem of multiple controls was overcome by performing correction Bonferroni. Independent samples t-test was used to test the correlation between a quantitative continuous variable that follows a normal curve and a qualitative with two categories. Mann-Whitney was used to test the correlation between a quantitative continuous variable that did not follow a normal curve and a qualitative with two categories. Correlations test between two continuous variables were performed using Pearson correlation coefficient if both variables followed a normal curve. In the case which both continuous variables did not follow the normal curve, correlations test between two continuous variables were performed using Spearman correlation coefficient.
Multiple linear regression was performed in order to investigate the possible relationship of sociodemographic factors as well as data related to the underlying disease and the current health status of the participants with their QoL. Results were presented with b-coefficients and 95% confidence interval (95% CI). Also, R2 of each model was used in order to state the percentage of variability of the dependent variable explained by each model.
A p-value lower than 0.05 were considered as statistically significant. To perform the statistical analysis the IBM SPSS Statistics version 13 (SPSS Inc., 2003, Chicago, USA) software was used.
2.5. Limitations of the study
The study sample was not representative of hemodialysis patients in Greece, but a convenience sample. The relevant sampling method limits the generalizability of results. Also, the study was cross-sectional thus not allowing the causal relation between quality of life and sociodemographic and clinical variables.
3. RESULTS
3.1. Descriptive characteristics
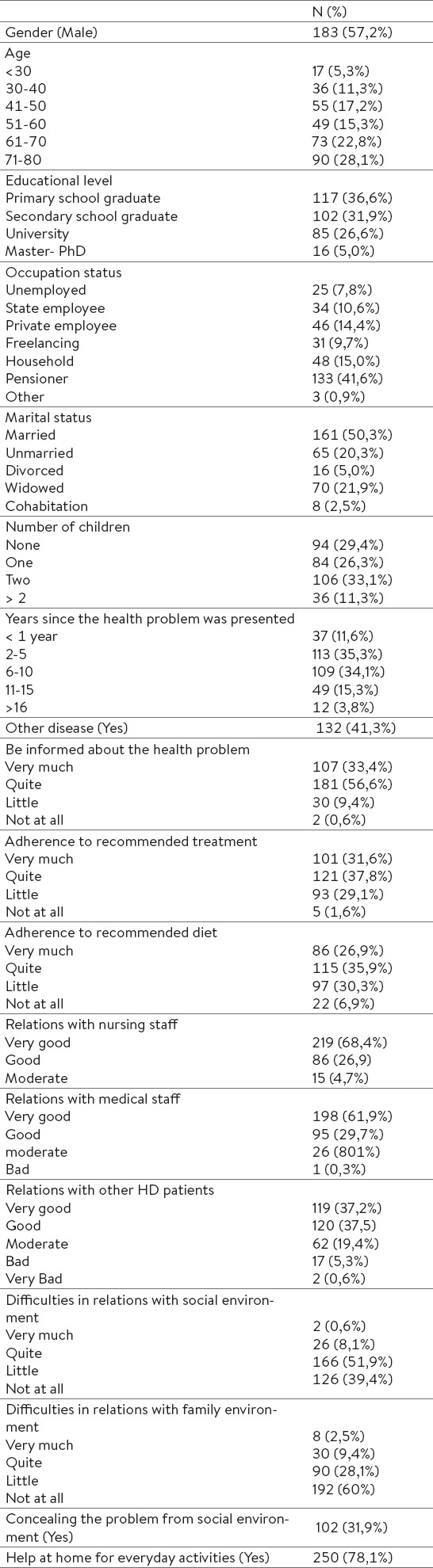
Table 1 presents the descriptive characteristics of the sample.
Table 1.
General characteristics of the sample
3.2. Quality of life and correlations
The average total score of QoL was found to be 17.43 (in the range 0-30) (Table 2).
Table 2.
Correlation between QoL and general characteristics. § Data are performed as mean (±τυπική απόκλιση). ‡ Correlation with correlation coefficient Spearman.
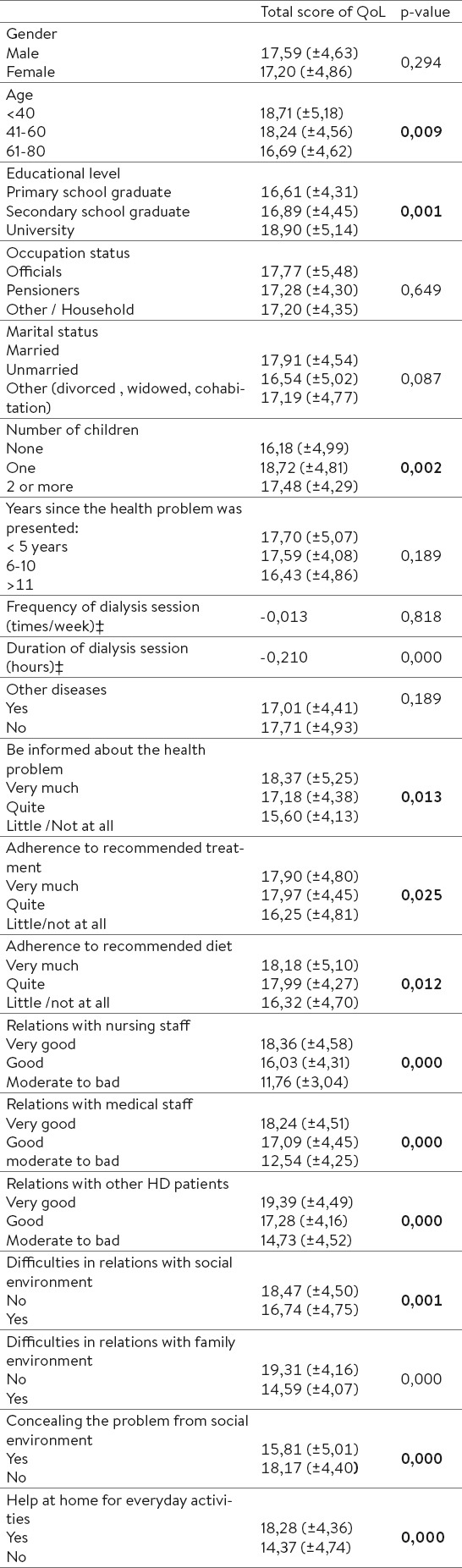
The average total score of QoL was higher in those <60 years (p=0,009), in participants of higher educational level (p=0,001). Additionally, there was a statistically significant correlation between the total score of QoL and patient information about the disease (p=0,013), the total score of QoL and adherence to treatment recommendations and proposed diet (p=0,025 & p=0,012, respectively) as well as between duration of HD session with the total score of QoL (p<0,001).
Statistically significant correlation was found between the total score of QoL and the relationships of HD patients with medical/nursing staff, as well as the other HD patients (p <0,001). Furthermore, the average QoL was higher for HD patients who did not face difficulties with family or social environment (p<0,001), for those who did not conceal the health problem from the community (p<0,001) and for those who had home help for handling everyday life (p<0,001).
3.3. Multiple linear regression
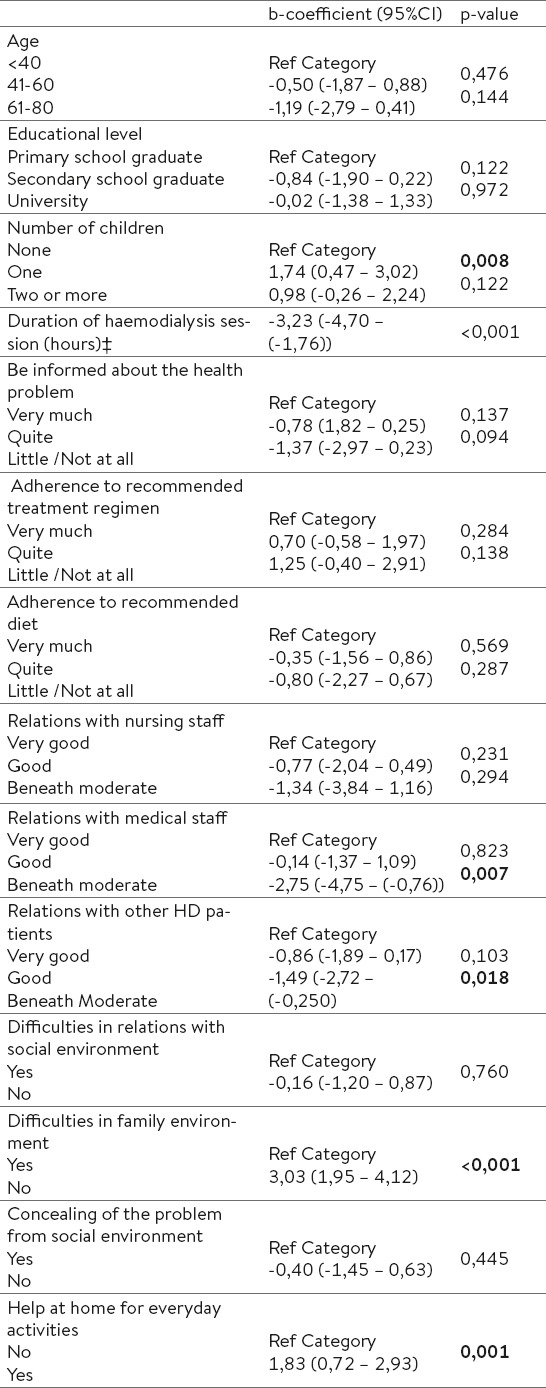
The multiple regression showed that the total score of QoL correlated significantly to number of children, duration of dialysis session, relationship with medical staff and other HD patients, the domestic constraints and the existence of home help for handling everyday activities (Table 3). More specifically, it was found that the overall QoL score is reduced by approximately 3 units after increasing the duration of dialysis session by 1 hour. Also, it was found that patients who reported that their relation with medical staff and other HD patients were below average, had lower scores on QoL by 2.75 and 1.5 points compared to patients who reported that they had very good relations with the medical staff and other patients, respectively. In addition, the total score of QoL of patients who reported that they had no difficulties in their relationships with family environment is about 3 points higher than those who had difficulties. Patients who reported that they had some help at home had by about 2 points higher overall QoL score than those who had no help. Furthermore, higher overall QoL scores was found for patients who had a child in relation to those who indicated that they had no children.
Table 3.
Factors related to QoL of Haemodialysis patients: results of multi linear regression
4. DISCUSSION
The results of the present study showed that the overall quality of life was correlated with age. A possible explanation is that patients of advanced age usually experience physical and cognitive impairment or may have lower expectations compared with younger individuals. Similarly, Mandoorah al.,(9) showed that patients older than 60 years had the worst report of the quality of life. Bayoumi et al., (10) supported that age, dialysis duration and male gender were negative predictors of quality of life. Seica al., (11) claimed that older age, female gender, lower socioeconomic status and higher educational level were associated with lower quality of life. Alshraifeen al., (12) demonstrated that advanced age was associated with better overall mental health but worse physical functionality.
Also, the results of the present study showed that participants of higher education had better quality of life, possibly because education allows deep understanding of the disease and compliance to the therapeutic regimen. Another alternative explanation is that higher education may reflect higher income and consequently ability to afford treatment. Other relevant studies have shown positive relationship between the level of education and quality of life (12, 13).
In addition, results demonstrated correlation between quality of life and patient information about their health problem. Interestingly, patients can not handle the disease adequately, if are not taught the basic principles of the treatment including dietary limitations, discipline, acceptance of machine and other necessary elements (14, 15, 16).
The finding of increased duration of dialysis and reduction of quality of life is consistent with Seica et al (11). It was also shown better quality of life in patients who had good relations with the medical-nursing staff. Indeed, a stable and sincere relation is a valuable tool for both sides. A good relation may also reflect that the medical team know to reduce the patient’s stress using the supportive techniques or proper intervention methods (17).
Low quality of life had patients not following the instructions. At least one-half of hemodialysis patients are likely to be noncompliant (18). Health professionals should develop individualized interventions to enhance patient’s adherence to the prescribed treatment regimen.
Higher quality of life had patients not facing difficulties with family or social environment and those not concealing the health problem of the community. According to Barnett et al., (19) chronic renal failure affects both patients and their families due to the extensive lifestyle changes as well as fluid and dietary restrictions. Ahrari et al., (20) showed a significant relation between social support and adherence to dietary and fluid restrictions and highlighted the family support as the highest level of perceived support. Moreover, Kara et al., (21) claimed that social support, by the spouse, family members, friends, colleagues or the community, is significantly associated with better quality of life.
5. CONCLUSIONS
The present study showed that sociodemographic and clinical variables are correlated to quality of life in hemodialysis patients. Deeper understanding of the factors affecting the quality of life in hemodialysis patients is useful to health professionals when developing individualized interventions based on their personal needs.
Acknowledgements
We thank the dialysis center: Iatriko therapeutirio Iliou, Athens, Greece.
Footnotes
CONFLICT OF INTEREST: NONE DECLARED.
REFERENCES
- 1.Unruh ML, Hess R. Assessment of health-related quality of life among patients with chronic kidney disease. Adv Chronic Kidney Dis. 2007;14(4):345–352. doi: 10.1053/j.ackd.2007.07.011. [DOI] [PubMed] [Google Scholar]
- 2.Kaufman SE. The increasing importance of quality of life research. Clin Res. 2001;1:18–22. [Google Scholar]
- 3.Fabrizi F, Messa P, Martin P. Health-related quality of life in dialysis patients with HCV infection. Int J Artif Organs. 2009;32(8):473–481. doi: 10.1177/039139880903200801. [DOI] [PubMed] [Google Scholar]
- 4.Avramovic M, Stefanovic V. Health-related quality of life in different stages of renal failure Artif Organs. 2012;36(7):581–589. doi: 10.1111/j.1525-1594.2011.01429.x. [DOI] [PubMed] [Google Scholar]
- 5.Cavalli A, Del Vecchio L, Manzoni C, Locatelli F, Cavalli A, Del Vecchio L, et al. Hemodialysis: yesterday, today and tomorrow. Minerva Urol Nefrol. 2010;62(1):1–11. [PubMed] [Google Scholar]
- 6.Lewis AL, Stabler KA, Welch JL. Perceived informational needs, problems, or concerns among patients with stage 4 chronic kidney disease. Nephrol Nurs J. 2010;37(2):143–148. [PubMed] [Google Scholar]
- 7.Landreneau K, Lee K, Landreneau MD. Quality of life in patients undergoing hemodialysis and renal transplantation - a meta-analytic review. Nephrol Nurs J. 2010;37(1):37–44. [PubMed] [Google Scholar]
- 8.Theofilou P, Kapsalis F, Panagiotaki H. Greek version of MVQOLI–15: Translation and cultural adaptation International Journal of Caring Sciences. 2012;5(3):289–294. [Google Scholar]
- 9.Mandoorah QM, Shaheen FA, Mandoorah SM, Bawazir SA, Alshohaib SS. Impact of demographic and comorbid conditions on quality of life of hemodialysis patients: a cross-sectional study. Saudi J Kidney Dis Transpl. 2014;25(2):432–437. doi: 10.4103/1319-2442.128613. [DOI] [PubMed] [Google Scholar]
- 10.Bayoumi M, Al Harbi A, Al Suwaida A, Al Ghonaim M, Al Wakeel J, Mishkiry A. Predictors of quality of life in hemodialysis patients. Saudi J Kidney Dis Transpl. 2013;24(2):254–259. doi: 10.4103/1319-2442.109566. [DOI] [PubMed] [Google Scholar]
- 11.Seica A, Segall L, Verzan C, Văduva N, Madincea M, Rusoiu S, et al. Factors affecting the quality of life of haemodialysis patients from Romania: a multicentric study. Nephrol Dial Transplant. 2009;24(2):626–629. doi: 10.1093/ndt/gfn506. [DOI] [PubMed] [Google Scholar]
- 12.Alshraifeen A, McCreaddie M, Evans JM. Quality of life and well-being of people receiving haemodialysis treatment in Scotland: A cross-sectional survey. Int J Nurs Pract. 2014;20(5):518–523. doi: 10.1111/ijn.12194. [DOI] [PubMed] [Google Scholar]
- 13.Sathvik BS, Parthasarathi G, Narahani MG, Gurudev KC. An assessment of the quality of life in hemodialysis patients using the WHOQOL-BREF questionnaire. Indian J Nephrol. 2008;18(4):141–149. doi: 10.4103/0971-4065.45288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Polikandrioti M, Νtokou M. Needs of hospitalized patients. Health science journal. 2011;5(1):15–22. [Google Scholar]
- 15.Lewis AL, Stabler KA, Welch JL. Perceived informational needs, problems, or concerns among patients with stage 4 chronic kidney disease. Nephrol Nurs J. 2010;37(2):143–148. [PubMed] [Google Scholar]
- 16.Cohen SD, Kimmel PL. Quality of life and mental health related to timing, frequency and dose of hemodialysis. Semin Dial. 2013;26(6):697–701. doi: 10.1111/sdi.12124. [DOI] [PubMed] [Google Scholar]
- 17.Shafipour V, Jafari H, Shafipour L, Nasiri E. Assessment of the relationship between quality of life and stress in the hemodialysis patients in 2008. Pak J Biol Sci. 2010;13(8):375–379. doi: 10.3923/pjbs.2010.375.379. [DOI] [PubMed] [Google Scholar]
- 18.Kutner NG. Improving compliance in dialysis patients: does anything work? Semin Dial. 2001;14(5):324–327. doi: 10.1046/j.1525-139x.2001.00080.x. [DOI] [PubMed] [Google Scholar]
- 19.Barnett T, Li Yoong T, Pinikahana J, Si-Yen T. Fluids compliance among patients having hemodialysis: can an educational program make a difference? J Adv Nurs. 2008;61(3):300–306. doi: 10.1111/j.1365-2648.2007.04528.x. [DOI] [PubMed] [Google Scholar]
- 20.Ahrari S, Moshki M, Bahrami M. The Relationship Between Social Support and Adherence of Dietary and Fluids Restrictions among Hemodialysis Patients in Iran. J Caring Sci. 2014;3(1):11–19. doi: 10.5681/jcs.2014.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kara B, Caglar K, Kilic S. Nonadherence of with diet and fluids restrictions and peresived social support in patients receiving hemodialysis. J Nurs Scholarsh. 2007;39(3):243–248. doi: 10.1111/j.1547-5069.2007.00175.x. [DOI] [PubMed] [Google Scholar]