

Abstract
Background:
Chronic renal failure is among the chronic disease which due to persistence of the disease and long treatment process has various effects on the physiological, psychological, functional ability, lifestyle changes, and independence status of the patient and his family. This may result in the burden feeling in caregivers. According to the importance of the subject, this study is to assess the level of caregiver burden in caregivers of hemodialysis patients.
Methods:
This is a cross-sectional analytical descriptive study that was conducted in 2014 on the caregivers of hemodialysis patients. Research instruments were consisted of two parts: demographic data check list and caregiver burden questionnaire. Data were analyzed by SPSS statistical software and Pearson correlation coefficient tests. A p value of less than 0.05 was considered statistically significant.
Results:
In this study, 72.5% of caregivers reported moderate to severe levels of caregiver burden. A significant relationship was observed between gender of the patient with caregiver burden score of (p=0.031) and type of the income with caregiver burden score of (p=0.000). Caregivers of male patients and patients with inadequate income had a higher caregiver burden score.
Conclusions:
Our results showed that more than half of the caregivers of hemodialysis patients had moderate to severe levels of caregiver burden, therefore it is worthy that health officials and nurses pay special attention to this issue by communicating with these patients and their caregivers.
Keywords: Caregiver Burden, Caregivers, Hemodialysis Patients
1. INTRODUCTION
Chronic renal failure is an aggravated and incorrectable condition in renal function in which the body will lose its ability to maintain electrolyte and metabolic balance leading to increased blood urea and its retention in the body (1). Dialysis is a method of removing unnecessary fluids and wastes when the kidneys are unable to perform their task due to impairment (2). The number of patients with renal failure is doubled every 7 years (3). According to the statistics of 1387, 16600 patients are dialyzed in 355 hemodialysis units of the country and each year this figure is increased to approximately 20% (4). The advancement of knowledge and treatment technologies as well as the increase in life expectancy has enhanced the longevity of many patients with chronic renal failure. Chronic disease is proposed throughout the world as a major health problem. Chronic renal failure is among the chronic disease which due to persistence of the disease and long treatment process has various effects on the physiological, psychological, functional ability, lifestyle changes, and independence status of the patient and his family (5). In longer terms, it will also cause the reduction of living standards, physical and psychological problems, as well as the restrictions in recreational, social and employment activities (6). Meanwhile, despite such challenges, caregivers often feel Disappointment, Isolation and failure due to the lack of support, training and experience (7).
Caregivers are people who have the greatest involvement in patient care and assistance during the course of the disease in order to adapt and manage the patient (8). Families of patients with chronic renal failure should perform supportive and care functions at home or in outpatient centers, such as dialysis units of hospitals. This can affect their mental health to varying degrees.
Caregivers often receive little attention and the main focus is on the patient. Frequent hospitalizations of the patients and factors associated with the disease can lead to the deterioration of depression and reduction of caregiver’s quality of life (9). Therefore, the evaluation of caregiver’s status and determination of their needs are very important.
Caregiver burden is a general term used to describe physical, emotional and financial cost of the care (10). Caregiver burden is defined as permanent difficulty, stress or negative experiences resulted from providing care by caregiver (11).
Burden is definable subjectively and objectively. Objective burden is defined as the changes and disruptions appeared in life as a result of care. Subjective burden definition is the reaction or attitude of caregiver against care experience (12).
Family is the best source for taking care of hemodialysis patients. Considering the long process of chronic renal failure, various complications of hemodialysis, new requirements, and major changes in lifestyle, family members are experiencing great tensions (13). Timely identification of these pressures in caregivers plays a decisive role in the promotion of their mental health. The aim of this study was to assess the scale of caregiver burden in caregivers of hemodialysis patients.
2. MATERIALS AND METHODS
This is a descriptive study which was designed and completed in 2014 to assess caregiver burden in the caregivers of patients undergoing hemodialysis. Research community was the caregivers of patients with chronic renal failure who referred to hemodialysis units of in two government hospitals in southern Iran. A total of 69 patients were under hemodialysis. After obtaining approval of relevant authorities, the researcher referred to hemodialysis units and studied all caregivers of patients by census method (caregiver is a person who lives with the patient and has the key role in patient care). After explaining the purpose of the study and obtaining the approval, research instruments were available for the caregivers. Questionnaire was completed at the presence of the researcher to answer the questions as needed (Illiterate caregivers answered the questionnaire verbally).
2.1. Collection tools characteristics
Research tools were consisted of two sections, including demographic data checklist of patients and their caregivers, and caregiver burden questionnaire. Patients demographic data checklist was consisted of age, sex, marital status, education, job, history of the disease, duration of dialysis, weekly dialysis frequency and the ability to perform daily activities, comorbidities (such as hypertension, diabetes, etc.), and caregivers demographic information was included age, sex, marital status, education, job, income, support from governmental agencies, and relativity with the patient.
Caregiver burden questionnaire was designed by Elmstahl et al in 1996 (14). Reliability and validity of the tool were verified by the research team at Kerman Razi School of Nursing in order to be used in a thesis entitled as “Investigating the relationship between social support and caregiver burden feeling in mothers with premature babies hospitalized in NICU”. Its reliability (82%) and reliability were obtained based on the internal correlation coefficient and using Cronbach’s alpha of 86% (15). The instrument of caregiver burden contains 22 items; this instrument evaluates the burden experience resulting from taking care of a patient with chronic disease. The average score of 22 items represents the total score of caregiver burden and the highest score represents the greatest caregiver burden. The total score of caregiver burden can be divided into three levels: low burden (1.00-1.99), medium burden (2.00-2.99), and severe caregiver burden (3.00-4.00). Therefore, the score of 22-43 is accounted as low burden, 44-65 as medium burden, and 65-88 is considered as severe burden.
This instrument covers 5 areas including:
-
*
General strain (8 items), which indicates the lack of freedom for the caregiver and the burden of the care;
-
*
Isolation (3 items), that shows the limited social interaction and the lack of special time for the caregiver himself;
-
*
Disappointment (5 items) which represents the Isolation, physical pain tolerance, the impact of financial difficulties and the feeling that life is unfair;
-
*
Emotional involvement (3 items) that reflects the feelings of anger and shame because of the presence of the patient;
-
*
Environmental (3 items), indicating the lack of caring experience and inability to deal with patient’s problems.
Scoring system is based on the Likert approach (never, rarely, sometimes, often) receiving the scores of 1, 2, 3, and 4, respectively (16).
2.2. Data analysis
Data analysis was performed using SPSS 21 software. Descriptive statistics in the forms of frequency tables and some indicators such as mean and standard deviation were used to describe the demographic characteristics and caregiver burden. T-test and Anova were used to determine the relationship between caregiver burden and demographic characteristics. A p value of less than 0.05 was considered statistically significant.
3. RESULTS
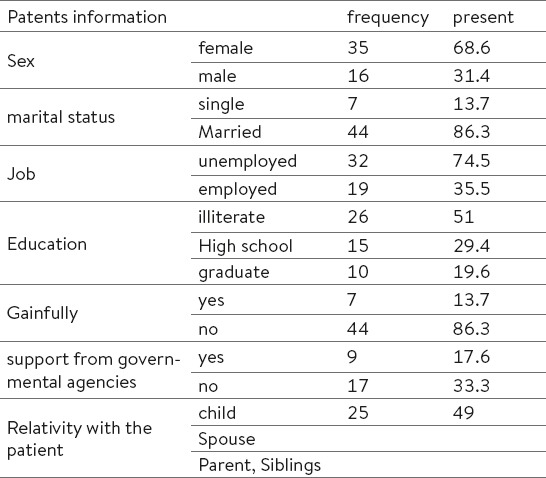
In this study, 69 caregivers of the patients with chronic renal failure undergoing hemodialysis in Iranian population were investigated. Because 10 caregivers were not willing to cooperate, and also 8 incomplete questionnaires were excluded from the study, thus 51 caregivers were entered to the study. Minimum and maximum age of the patients was 22 and 87 years with the mean age of 53.07 and standard deviation of 17.90. Caregivers’ minimum and maximum age were 18 and 80 years with an average age of 42.11 and SD of 14.78. Tables 1 and 2 show demographic data for the patients and their caregivers.
Table 1.
Demographic data of patients
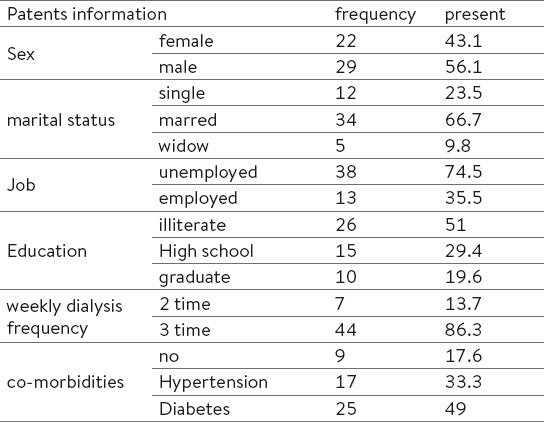
Table 2.
Demographic data of caregiver’s
When investigating the total score of caregiver burden and the areas of (general strain, Isolation, Emotional involvement, Disappointment, and environmental), the results showed that 12 caregivers (23.5%) reported high levels of caregiver burden. Also 25 caregivers (49%) expressed medium and 14 persons (27.5%) reported low levels of caregiver burden, respectively (Table 3).
Table 3.
Frequency and present of Caregiver burden in caregiver’s
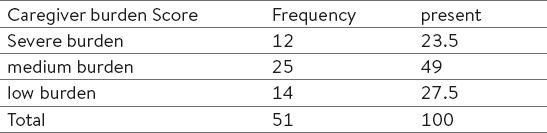
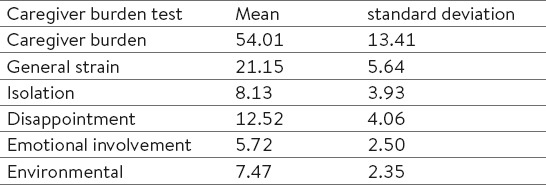
Table 4 presents mean and standard deviation of the scores for the caregivers of hemodialysis patients in the caregiver burden test and its areas. Anova and t-test were used to determine the relationship between demographic variables and the caregiver burden score.
Table 4.
The mean scores and standard deviation of caregiver’s on the test Caregiver burden
The results show that there is a significant relationship between the patient’s gender with caregiver burden score of (p=0.031) and the type of income with caregiver burden score of (p=0.000). Such that caregivers of male patients and patients with insufficient income had higher caregiver burden scores.
In the relationship between demographic variables with the areas of caregiver burden results showed that there is a relationship between the patient’s gender and the areas of general strain (p=0.016) and Disappointment (p=0.004). Single caregivers gained higher scores in these areas. There is a relationship between income and the areas of general strain (p=0.000), Isolation (p=0.022), Disappointment (p=0.039), and Emotional involvement (p=0.003). Patients with insufficient income had higher scores in these areas. No relationship was found between other demographic variables of patients and caregivers and the caregiver burden score and its areas (p>0.05).
4. DISCUSSION
This study has investigated the caregiver burden feeling in caregivers of hemodialysis patients. Most of the research has been focused on the hemodialysis patients, while their caregivers, spouse and partners who help in their treatment, and experience losses and potential changes were neglected (17).
The results of this study showed that 72.5% of caregivers had moderate to severe caregiver burden. Paradiso proposed that the incidence of changes in family functions is inevitable due to the chronic nature and long-term treatment of progressive renal failure (18). Belasco and Sesso study showed that taking care of dialysis patients may cause the feeling of stress and destructive effects in the caregivers. Thus, social support and psychological interventions should be executed in order to improve the lives of the caregivers and subsequently the patients (19).
Belasco and his colleagues in a study entitled “The caregiver burden and quality of life of caregivers to hemodialysis patients” reported that a significant relationship exists between caregiver burden and the quality of life, and caregivers of patients experience the burden resulted from caring which affects their quality of life (19).
In a study Matsuu et al. proposed that caregivers of hemodialysis patients might have a very important responsibility, because they have to play an important role in supporting dialysis patients (20). Habibzadeh and his colleagues in a survey to assess the level of life quality of caregivers of patients in Khoy reported that 52.5% of caregivers had moderate to low quality of life, 85% believed that society support is insufficient, and 65% found their lives devoid of recreation and entertainment (21). Abbasi and his colleagues reviewed the caregiver stress and its related factors in caregivers of hemodialysis patients in Gorgan and reported that 74.2% of caregivers suffered from extreme caregiver burden (13).
Therefore realizing the psychological characteristics and burden feeling resulted from care in caregivers is very important in planning and providing effective treatment interventions.
5. CONCLUSION
Based on the findings of this study it can be concluded that hemodialysis at different levels cause moderate to severe burden in the caregivers of patients. Thus, the provision of care plans to improve the mental health of these patients is necessary. It can be also concluded that considering the caring needs of other caregivers can have positive impacts on their mental health.
Acknowledgement
Researchers of the University of Jiroft Medical Sciences do appreciate the research assistant for their financial support of this research project. They also thank the heads of hospitals, authorities of hemodialysis units, and caregivers of patients who kindly participated in this study.
Footnotes
CONFLICT OF INTEREST: NONE DECLARED.
REFERENCES
- 1.Mcphee S J, Papadakis MA, Rabow MW, Education MH. Current Medical Diagnosis & Treatment 2012. McGraw-Hill Medical. 2010 [Google Scholar]
- 2.Brunner LS, Smeltzer SCC, Bare BG, Hinkle JL, Cheever KH. Brunner & Suddarth’s textbook of medical-surgical nursing. Lippincott Williams & Wilkins. 2010 [Google Scholar]
- 3.Nasiri M, Kheirkhah F, Rahimiyan B, Ahmadzadeh, et al. Stressful factors, coping mechanisms and quality of life in hemodialysis patients. Journal of Critical Care Nursing. 2013;(6):119–126. [Google Scholar]
- 4.Mottahedian Tabrizi E, Najafi Mehri S, Samiey S, et al. Effect of programmed nursing care in prevention of hemodialysis complications. Journal of Critical Care Nursing. 2009;2:55–59. [Google Scholar]
- 5.Pereira AA, Weiner DE, Scott T, Sarnak MJ. Cognitive function in dialysis patients. American Journal of Kidney Diseases. 2005;45:448–462. doi: 10.1053/j.ajkd.2004.10.024. [DOI] [PubMed] [Google Scholar]
- 6.Lindqvist R, Carlsson M, Sjöden PO. Coping strategies and health?related quality of life among spouses of continuous ambulatory peritoneal dialysis, haemodialysis, and transplant patients. Journal of Advanced Nursing. 2000;31:1398–1408. doi: 10.1046/j.1365-2648.2000.01404.x. [DOI] [PubMed] [Google Scholar]
- 7.Lim J, Zebrack B. Caring for family members with chronic physical illness: a critical review of caregiver literature. Health and quality of life outcomes. 2004;2:1–9. doi: 10.1186/1477-7525-2-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Black JM, Hawks JH, Keene AM. Medical-surgical nursing: Clinical management for positive outcomes. WB Saunders Co. 2001 [Google Scholar]
- 9.Quittner AL, Digirolamo AM. Family adaptation to childhood disability and illness. 1998 [Google Scholar]
- 10.Burden C, Quite NRS. A practical guide to caring for caregivers. Am Fam Physician. 2000;62:2613–2620. [PubMed] [Google Scholar]
- 11.Simon BS, Budó MDL, Garcia RP, et al. Social support network to the caregiving family of an individual with a chronic disease: integrative review. Journal of Nursing UFPE on line [JNUOL/DOI: 10.5205/01012007] 2013;7:4243–4250. [Google Scholar]
- 12.Robinson K. The relationships between social skills, social support, self-esteemand burden in adult caregivers Journal of advanced Nursing. 1990;15:788–795. doi: 10.1111/j.1365-2648.1990.tb01908.x. [DOI] [PubMed] [Google Scholar]
- 13.Abbas IA, Rahmani H, Shariati A, et al. The Burden on Cargivers from Hemodialysis Patients and Related Factors. Journal of Research Development in Nursing & Midwifery. 2011;8:27–33. [Google Scholar]
- 14.Elmståhl S, Malmberg B, Annerstedt L. Caregiver’s burden of patients 3 years after stroke assessed by a novel caregiver burden scale. Archives of physical medicine and rehabilitation. 1996;77:177–182. doi: 10.1016/s0003-9993(96)90164-1. [DOI] [PubMed] [Google Scholar]
- 15.Abolhadi F. The relationship between social support and Caregiver Burden of premature infant mothers admitted to neonatal intensive care unit in afzali poor hospital of kerman- Kerman University of Medical Sciences. 2013 [Google Scholar]
- 16.Chiou CJ, Chang HY, Chen IP, Wang HH. Social support and caregiving circumstances as predictors of caregiver burden in Taiwan. Archives of gerontology and geriatrics. 2009;48:419–424. doi: 10.1016/j.archger.2008.04.001. [DOI] [PubMed] [Google Scholar]
- 17.Beanlands H, Horsburgh ME, Fox S, et al. Caregiving by family and friends of adults receiving dialysis. Nephrology Nursing Journal. 2005;32:621–632. [PubMed] [Google Scholar]
- 18.Paradiso C. the dialysis patient, the family and home health nurse. home health nurse. 2004;4:26–34. doi: 10.1097/00004045-198607000-00004. [DOI] [PubMed] [Google Scholar]
- 19.Belasco AG, Sesso R. Burden and quality of life of caregivers for hemodialysis patients. American journal of kidney diseases. 2002;39:805–812. doi: 10.1053/ajkd.2002.32001. [DOI] [PubMed] [Google Scholar]
- 20.Matsuu K, Washio M, Arai Y, Higashi H, Saku Y, Tokunaga S, Ide S. Depression among caregivers of elderly patients on chronic hemodialysis. Fukuoka igaku zasshi=Hukuoka acta medica. 2001;92:319–325. [PubMed] [Google Scholar]
- 21.Habibzadeh H, Mohammadpo H, Kiani P. A survay on Quality of Life in hemodialysis patient caregivers. Journal of Urmia Nursing And Midwifery Faculty. 2009;7:128–135. [Google Scholar]