

Abstract
Laparoscopic ovariohysterectomy using single-portal access was performed in nine selected owned dogs admitted for elective ovariohysterectomy and the surgical technique and outcomes were detailed. A multiport device (SILS Port, Covidien, USA) was placed at the umbilical area through a single 3 cm incision. Three cannulae were introduced in the multiport device through the access channels and laparoscopic ovariohysterectomy was performed using a 5-mm sealing device, a 5-mm articulating grasper and a 5-mm 30° laparoscope. The mean total operative time was 52.66±15.20 minutes and the mean skin incision during surgery was 3.09±0.20 cm. Of the nine cases examined, in the one with an ovarian tumour, the technique was converted to multiport laparoscopy introducing an additional 5-mm trocar. No surgical complications were encountered and intraoperative blood loss was minimum in all animals. Clashing of the instruments and reduced triangulation were the main limitations of this technique. The combination of articulated and straight instruments facilitated triangulation towards the surgical field and dissection capability. One month after surgery a complete wound healing was observed in all animals. The present data showed that ovariohysterectomy performed with a single-port access is technically feasible in dogs. The unique abdominal incision minimises the abdominal trauma with good cosmetic results.
Keywords: Surgery, Small animals, Obstetrics, Laparoscopy, Fertility, Clinical practice
Introduction
Ovariohysterectomy is one of the most common surgical procedures performed in veterinary practice (Bloomberg 1996). Although different techniques have been described, the most widely utilised approach to remove ovaries and uterus is a midline coeliotomy (Howe 2006). More recently, laparoscopic ovariohysterectomy (Austin and others 2003, Davidson and others 2004, Hancock and others 2005, Freeman and MacFarlane 2007, Gower and Mayhew 2008) and laparoscopy-assisted ovariohysterectomy (Devittand others 2005, Mayhew and Brown 2007, Gower and Mayhew 2008, Adamovich-Rippe and others 2013) have been described as surgical alternatives to conventional ovariohysterectomy (OVH) in female dogs. Laparoscopic surgery is associated with less postoperative pain, reduced time of hospitalisation and shorter recovery time when compared with conventional ovariohysterectomy in dogs (Davidson and others 2004, Devitt and others 2005, Hancock and others 2005).
Moreover, single-port laparoscopy, also called laparoendoscopic single-site surgery, single-incision laparoscopy and single-site laparoscopy, has been presented in the last few years as a minimally invasive approach in veterinary medicine to perform ovariectomy in dogs (Manassero and others 2012, Runge and others 2012, Emerson and others 2013), ovariectomy in cats (Coisman and others 2014) and in tigers (Emerson and others 2013), as well as ovariectomy and gastropexy (Runge and Mayhew 2013), splenectomy (Khalaj and others 2012), cryptorchidectomy (Runge and Holt 2012, Runge and others 2014) and intestinal surgery (Case and Ellison 2013) in small animals.
The main purpose of this novel approach is to minimise the surgical trauma compared with multiport laparoscopy by reducing the number of incisions in the abdominal wall and by determining the optimum laparoscopic approach to only one entrance. The multichannel device allows the use of up to four instruments through a single 2–3-cm incision (Manassero and others 2012). In addition, this novel minimally invasive approach may offer advantages over laparoscopic surgery in assisted procedures regarding the enlargement of the performed incision (Case and Ellison 2013) and the exteriorisation of organs in extracorporeal procedures. Sometimes this novel approach requires additional specialised laparoscopic instruments (prebent or articulating instruments) and angled telescopes (Runge and Mayhew 2013). However, disadvantages related to the use of these devices (lack of triangulation and collision of the instruments) must be taken into consideration (Mayhew 201,4). Furthermore, an adequate training would be necessary in order to handle the instruments skillfully and to obtain suitable results in the initial stages of this approach (Sanchez-Margallo and others 2014).
The authors hypothesised that single-port ovariohysterectomy would be feasible in dogs through a single multitrocar device facilitating the organ retrieval through a single incision. The purpose of this study was to investigate the feasibility of single-port ovariohysterectomy in dogs and to discuss the technical aspects in this preliminary report.
Materials and methods
Accomodation of the animals and their handling were done in accordance with ARRIVE guidelines (Kilkenny and others 2010). Nine owned entire female dogs underwent elective single-port ovariohysterectomy. Physical evaluation, complete blood count and serum biochemical profile were performed preoperatively.
Food was withheld from all dogs 12 hours before surgery. Dogs were premedicated using 0.02 mg/kg intramuscular acetylpromazine and after preoxygenation with Hall face mask, anaesthesia was induced intravenously with propofol dosed to effect (1–4 mg/kg) and maintained with sevoflurane via endotracheal intubation. Volume controlled mechanical ventilation was carried out in order to maintain normocapnia (end tidal CO2 from 35 cm H2O to 40 cm H2O), leading to a respiratory rate of 20 breaths per minute. Ringer's lactate was administered as intravenous fluidotherapy and maintained at 5 ml/kg/hour. After extubation, 1 mg/kg intravenous ketorolac tromethamine, 2 mg/kg intravenous tramadol and 15 mg/kg intramuscular long-acting (48 h) amoxicillin were administered. Continuous respiratory and cardiac rate, pulse oximetry, FiO2, end tidal CO2, tidal volume per minute, inhaled and exhaled anaesthetic agent and airway peak pressure were monitored with a multiparametrical monitor (Dash 3000, General Electric Healthcare, Milwaukee, Wisconsin, USA). Before surgery, the urinary bladder was emptied by catheterisation, the animals were placed in dorsal recumbency without Trendelenburg positioning and the ventral abdomen was clipped and aseptically prepared for laparoscopic surgery.
A 3 cm midline skin incision was made at the infra-umbilical area. The linea alba was incised and a multiport access device (SILS Port, Covidien, Norwalk, Connecticut, USA) previously lubricated (KY, Johnson & Johnson, New Brunswick, New Jersey, USA) was placed in the abdominal wall using a Satinsky clamp (Fig 1). Three laparoscopic 5-mm cannulae were introduced through the access channels of the multitrocar device at the 3 o'clock, 6 o'clock and 10 o’clock positions. Pneumoperitoneum was established with an electronic CO2 insufflator (10 mm Hg with a flow rate of 1 L/m) attached to the appropriate cannula of the multiport device. The three cannulae were orientated in a triangular pattern placing a 5 mm 30° laparoscope 50 cm in length (Laparoscope HOPKINS II, Karl Storz GMBH, Germany) into the 3 o’clock trocar (Fig 2). Following initial abdominal exploration, the telescope was removed to prevent injury to viscera during position change and the animals were manually rotated into right lateral recumbency (25–30°) with a slight lumbar elevation to facilitate the exposure of the left ovary and uterine horn by displacement of the abdominal organs. Both surgeons were positioned on the same side of the operating table and under laparoscopic vision, the ovary and proper ligament were located.
FIG 1:
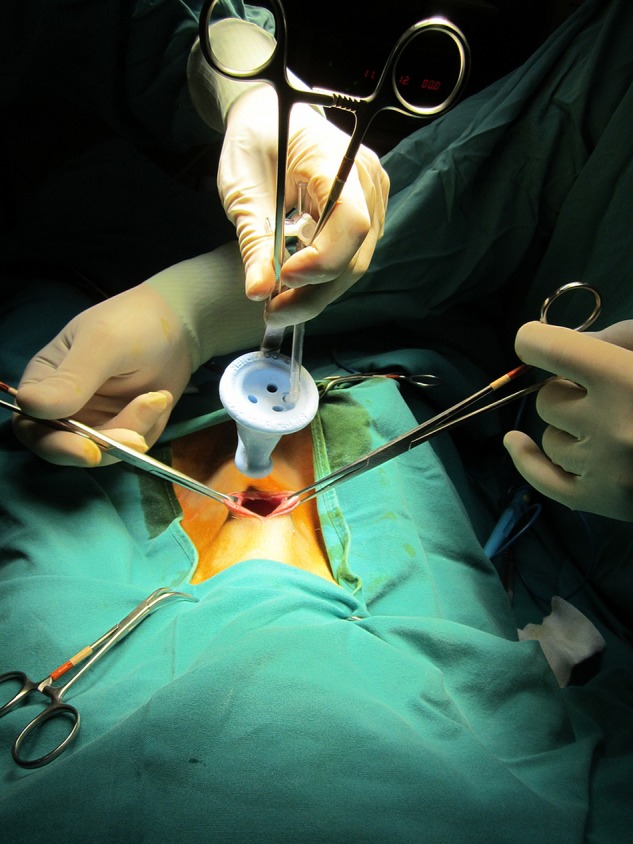
SILS instrument and cutaneous incision of the technique
FIG 2:

External view of SILS port fixed to abdominal skin with all instruments
The right proper ligament was grasped and the ovarian pedicle was exposed by articulating the tip of the laparoscopic grasper intra-abdominally (Endo Grasp single use instrument, Covidien, Mansfield, Massachusetts, USA) with the tip deflecting towards the ovary (Fig 3). This manoeuvre facilitates the handling of the straight forceps and avoids instrument collision. Dissection and vascular sealing of the ovarian pedicle were performed using a 5-mm LigaSure device (Valleylab, Tyco Healthcare UK, Gosport, UK). The articulating instrument and the 5 mm telescope created triangulation and a space to handle the sealing device in order to coagulate and transect the suspensory ligament of the ovary. The ovarian vasculature was cauterised and severed with the 5-mm sealing device, isolating the right ovary.
FIG 3:
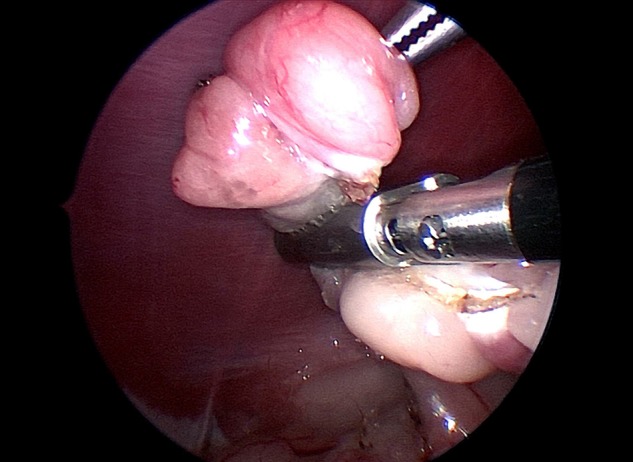
The exposure and coagulation of the ovarian pedicle are accomplished by traction of the proper ovarian ligament
The articulating grasper was straightened within the abdomen and the left uterine horn was grasped. Subsequently the grasper was articulated with the tip deflecting towards the uterine horn. The uterine horn was suspended and the broad and round ligaments were sealed and transected with the 5-mm sealing device, reaching the body of the uterus (Fig 4).
FIG 4:
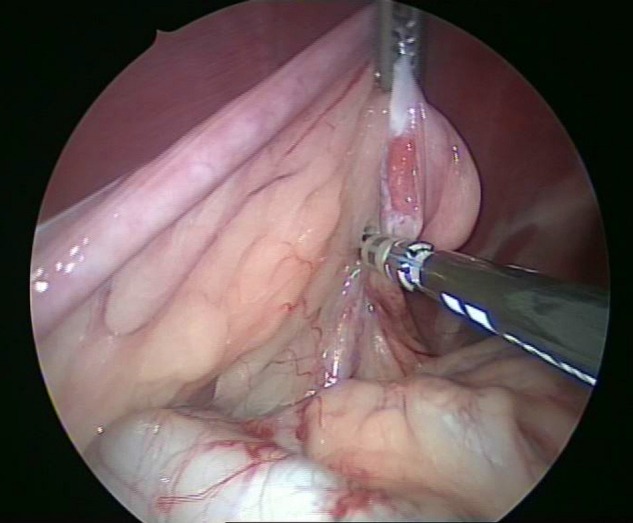
Exposure of the uterine horn and transection of the broad ligament until reaching the body of the uterus
The articulating grasper was then straightened within the abdominal cavity, and the camera, grasper and sealing device were removed. Insufflation was stopped and the patient was tilted in the opposite direction. The surgeon then moved to the right side of the dog and the video tower was repositioned on the left side.
Once the right ovary and uterine horn were dissected, the manoeuvres and surgical steps described herein were repeated on the opposite side. Uterine arteries were individually coagulated proximal to the cervix, and the uterine body was coagulated and severed alongside the cervix using a 5-mm sealing device and placing the animal in horizontal dorsal recumbency.
In one case related with an ovarian tumour, the authors have modified the technique and the single-incision device was inserted 8 cm caudal to the umbilicus. An additional 5-mm trocar was inserted in the umbilical area in order to dissect the granulose cell tumour in the right ovary. The articulating grasping forceps was inserted in the single-incision device and the sealing device was inserted through the additional 5-mm trocar. Both ovaries and uterine horns were released from their ligaments as far as the uterine body was reached. The removal of the ovarian tumour was enabled by extending the original 3-cm umbilical incision up to an 8 cm incision and the ovarian tumour was placed in a specimen retrieval bag. The left ovary and the associated uterine horn were also exposed through the abdominal 8 cm incision. The body of the uterus was externally ligated, transfixed and divided in a standard fashion and the uterine stump was reintroduced into the abdominal cavity through the caudal incision.
The uterine stump and ovarian vascular remnant pedicles of the animals were assessed for bleeding under laparoscopic vision, and the abdominal cavity was examined to identify any blood or iatrogenic injuries during the procedure. The device and the laparoscopic grasper (which grasped one of the ovaries by the proper ligament) were pulled outside the abdominal cavity. The ovaries and uterus were extracted by directly removing the single incision access device. External confirmation of total removal of ovarian and uterine tissues was then accomplished (Fig 5). Once the OVH was completed, the abdomen was examined.
FIG 5:

Ovaries and uterus after laparoendoscopic excision. Right ovarian granulosa cell tumour
The pneumoperitoneum was completely deflated by manual external compression of the abdomen. The abdominal incision was closed in a three layer routine manner. Cardiorespiratory parameters including heart and respiratory rate, pulse oxymetry, end tidal CO2, tidal volume per minute, inhaled and exhaled anaesthetic agent and airway peak pressure were monitored during surgery. Mean operative time, complications and incision scores were registered after surgery and data were summarised as mean±sd and range. The dogs were re-evaluated at 7 days, 15 days, one month and two months after surgical intervention. All dogs were administered 0.01 mg/kg intravenous buprenorphine at 4–6 hour intervals. Dogs were discharged with a four-day course of an NSAID (2 mg/kg/8 hours carprofen).
The influence of weight over surgical operative time was analysed by statistical software (IBM SPSS Statistics V.21, Amos Development Corporation, Meadville, Pennsylvania, USA). A P value of ≤0.05 will be considered statistically significant.
Tissue samples collected during ovariohysterectomy procedure were fixed in 10 per cent neutral buffered formalin. Routine microscopic evaluation with haematoxylin and eosin was performed.
Results
The mean (sd) age and weight was 4.55 (2.24) years (1–7 years) and 11.28 (4.63) kg (7.5–23 kg), respectively. The preoperative studies showed preoperative values within normal range. Physical examination and preoperative studies were found to be within reference ranges.
The mean total operative time was 52.66 (15.20) minutes (27–73 minutes) including incision performance and abdominal wall suturing manoeuvres. Surgical operative time was not statistically influenced either by the weight or age. Surgical procedures were performed through an initial 3.09 (0.20) cm (2.8 cm to 3.4 cm) skin incision. In one animal the final incision was enlarged until 8 cm in order to facilitate the extraction of an ovarian tumour.
The transumbilical approach was performed without difficulty, the abdominal cavity was successfully explored and the surgical procedures were completed without complications. Abnormalities of the ovaries and uterus were observed in three animals during laparoscopic surgery. Two animals showed ovarian cysts on the left side and in one case the right ovary and the left uterine horn showed different cysts. Emptying of the cysts before surgery was not necessary. One animal showed an ovarian granulose cell tumour. Single-incision laparoscopic ovariohysterectomies were performed combining straight and articulated laparoscopic instruments without major technical limitations. In one dog, technical difficulties were encountered for the mobilisation of the ovarian neoplasia and an additional 5-mm trocar was used in order to mobilise the ovary during the laparoscopic surgery converting the single-incision procedure in a multitrocar approach. No lesions or haemorrhages were observed during the laparoscopic procedure and ovaries and uteri were extracted without any tissue rupture. No relevant haemodynamic changes were observed as a consequence of pneumoperitoneum or surgery. All dogs recovered uneventfully from anaesthesia within 30 minutes after switching off sevoflurane vaporiser. No postoperative complications were encountered during follow-up and at 15 days after surgery all animals were behaviourally normal and no vaginal discharge, urinary incontinence, signs of infection, fever or anorexia was encountered in any case. Temperature, pulse, respiratory rate, and complete blood count remained, in all the dogs, within normal limits after surgery. On re-evaluation at one month and two months, all incisions were completely healed with no evidence of incisional or another complication.
Histological analysis confirmed the presence uterine cysts in four animals and a granulose cell tumour in one.
Discussion
Ovariohysterectomy is one of the most common surgical procedures in veterinary medicine including the elective sterilisation and the treatment for most uterine diseases (Bloomberg 1996, Hedlund 1997, Fingland 1998). Multiple techniques have been described in the literature and laparoscopic techniques have been progressively introduced and described as an alternative to conventional OVH in female dogs (Austin and others 2003, Davidson and others 2004, Howe 2006, Freeman and MacFarlane 2007, Gower and Mayhew 2008, Kim and others 2012) and laparoscopic ovariohysterectomy in dogs is associated with reduced postoperative pain and surgical stress compared with conventional open procedures (Davidson and others 2004, Devitt and others 2005, Hancock and others 2005).
In recent years, different single-port access techniques have proven useful in the therapy of different pathologies as an alternative approach to conventional laparoscopic surgery in an effort to reduce morbidity and improve the cosmetics, focused on human surgery (Mittermair and others 2014). The reduction in portal number combined with the instrument arrangement is called ‘reduced port surgery’. After different experiences in veterinary medicine (Khalajand others 2012, Manassero and others 2012, Runge and Holt 2012, Case and Ellison 2013, Emerson and others 2013, Mittermair and others 2014, Runge and others 2012, 2014, Runge and Mayhew 2013), this emerging technique is expected to offer benefits such as avoiding the need for multiple abdominal wall incisions or reducing them as much as possible, diminishing the risks of wound infection, reducing postoperative pain and morbidity, together with facilitating earlier recovery.
Currently there is a trend related with the reduced portal surgery (reduction in cannula number and size) for laparoscopic sterilisation in animals facilitating a reduction in morbidity and postoperative discomfort (Van Nimwegen and Kirpensteijn 2007, Dupre and others 2009, Case and others 2011, Wilson & Monnet 2012). Although the technique of single port ovariohysterectomy has not yet been standardised in veterinary medicine, in this preliminary study the authors describe the potential advantage related with the minimal access to the abdominal cavity and the possibility of the organ removal through this minimal access.
In the present case no transabdominal sutures were used and in one case, related with the presence of a 7 cm ovarian tumour, the authors decided to introduce a new trocar and convert the procedure in a multitrocar approach for the assistance of the surgeon. In all cases the single incision approach allows the use of two laparoscopic instruments at a time achieving excellent exposure of the ovaries and uterus, as well as optimal viewing during dissection and transection manoeuvres like during previous experiences in single incision ovariectomy (Manassero and others 2012).
During single incision ovariohysterectomy the combination of angulated and straight instruments avoid collisions between them maintaining the tip of the instruments placed in the surgical area compensating the triangulation limitations. Furthermore, the available flexible single-port devices can be bent in all directions which compensates for the triangulation limitations (Manassero and others 2012).
Despite the limited use of the single-port surgery in veterinary medicine, the global results seem favourable (Manassero and others 2012, Wilson and Monnet 2012). The single incision surgery offers certain advantages over laparoscopic procedures. First, is the use of a single 3 cm incision and in eight cases the ovaries and uterus were removed without needing incision enlargement. In the case of the ovarian tumour, the authors' retracted the uterus out of the portal for exteriorisation of the uterine horns and ovaries in order to carry out an extracorporeal transfixion, ligation and division of the uterine body further simplify the procedure. The authors agree with previous experiences (Dupre and others 2009, Khalaj and others 2012) that the use of a sealing device facilitates a sealant tissue effect and improves the feasibility of this technique. Another possible benefit of this technique is the ability to place the ovarian tissue in a specimen retrieval bag before removal from the abdomen (Emerson and others 2013).
However this novel approach is not without its limitations. In the SILS Port device the instruments are introduced parallel to each other and the manoeuvrability has been more complex than in traditional laparoscopic procedures even using angulated instruments (Manassero and others 2012). Moreover, in the authors’ opinion this novel minimally invasive approach presents additional drawbacks: a surgeon’s inadequate experience and the difficulty of some intracorporeal manoeuvres, collision of the instruments and telescope (Manassero and others 2012, Runge and others 2012) even with specifically bent or articulated instruments (Saber and others 2008, Santos and others 2011). In the previous experiences with laparoscopic ovariectomy, it seems less technically demanding than laparoscopic ovariohysterectomy and the triangulation is not mandatory (Dupre and others 2009) explaining why no technical difficulties were observed during single-port surgery in some studies (Manassero and others 2012).
Considering the positive operative and postoperative outcomes in ovariectomy, it seemed attractive to apply the single-port approach in the OVH procedure also. Although the technique of single incision ovariohysterectomy has not yet been standardised in veterinary medicine, in the authors’ opinion this approach could be available in clinical practice since no intraoperative complications, haemorrhages or lesions were encountered during the procedures. Accessing the abdominal cavity by means of small incisions and the organ removal through this access, provides a clear advantage as regards the recovery time after surgery.
During the procedures some previous recommendations regarding the introduction of the cannulae, lubrication of the cannulae and traction of the muscular edges were taken into consideration during the cannulae introduction in order to minimise the presence of lesions (Manassero and others 2012). Special protection measures include introduction of the multitrocar device bluntly, and the authors tried to establish the single incision technique using an intrabdominal pressure of 10 mm Hg. Correct exposure of the ovary and uterus is allowed by changing the position from dorsal recumbency to lateral recumbency and the authors used a 5-mm sealing device looking for a sealant tissue effect with a reduced risk of tissue burning (Dupre and others 2009). Displacement of the abdominal organs is facilitated by rotation of the patient to lateral recumbency, identifying the left or right ovary and uterine horn. Initially every ovary was grasped using an articulated grasper and the suspensory ligament and ovarian vasculature were sealed and divided. The uterine horns were retracted successfully using an angulated grasper and the broad ligaments were sealed and divided until reaching the cervix. Finally, the cervix is sectioned with a 5 mm sealing device and the uterus was removed through the single-port incision.
The surgical time ranged from 27 minutes to 73 minutes (mean, 52 minutes) and the authors can perceive a progressive surgeon’s skills acquisition and a reduction of the learning curve associated with this approach. The surgical times detailed here are shorter than other reported laparoscopic ovariohysterectomies in dogs. Several factors were related to the duration of the resection of the ovaries and uterine horns. One of these was the amount of fat encountered around the ovarian pedicle (Dupre and others 2009) and the mesometrium. The ovarian pedicle and broad ligament fat score could be associated with obesity and the increased surgical time. The presence of fat significantly influenced operative time because of the tissue thickness and because of making vessels difficult to be recognised (Dupre and others 2009). This fact prolonged the duration of surgery and also the resection of both ovaries and uteri independent from the technique. In the authors’ experience, the use of the left-hand tip articulated laparoscopic instruments and straight right-hand laparoscopic instruments allowed us to accomplish this intervention safely in all cases in reasonable operative time.
In one dog the procedure was converted to a multitrocar technique by inserting an additional 5-mm trocar in the abdominal midline in order to mobilise and expose an ovarian tumour during the surgical procedure. Finally, in this dog the original 3-cm incision of the single port device was enlarged to 8 cm in order to facilitate the extraction of the ovarian tumour and uterus. Histological analysis confirmed the presence of uterine cysts in four animals and a granulose cell tumour.
In conclusion, the present results suggest that the combination of a multitrocar device, a 30° laparoscope, the sealing device and a tip-articulated laparoscopic instrument allowed excellent anatomical and surgical visualisation, adequate manoeuvrability and safety during sealing and cutting of anatomical structures and finally, the organ removal. In addition, all the procedures were completed in a reasonable total surgical time and conversion to open surgery was not necessary. In one case the procedure was converted to a multitrocar laparoscopic technique adding an additional 5-mm trocar to handle an ovarian tumour. Dogs were discharged few hours after surgery and no wound complications, swelling or hernias were observed during two months follow-up. However, the authors consider that single incision ovariohysterectomy is technically more demanding than the same laparoscopic procedure and probably the highest limitation could be the expensive access device (Coisman and others 2013) and surgical instrumentation required (Runge and others 2012).
Initial clinical experience and results with this novel approach are promising, in spite of the short-term follow-up and moderately small study population. Although the authors have not found operative lesions or postoperative complications in this preliminary study, more studies are necessary in order to evaluate accurately the possibilities of this novel approach.
Footnotes
Twitter: Follow Francisco Sanchez Margallo at @sanchezmargallo
Contributors: FMS-M has participated in the design, development and the analysis of the results. ATA has participated in the development of the study. ID-G has participated in the analysis of the results.
Competing interests: None declared.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data sharing statement: No additional data are available.
References
- Adamovich-Rippe K. N., Mayhew P. D., Runge J. J., Culp W. T., Steffey M. A., Mayhew K. N., Hunt G. B. (2013) Evaluation of laparoscopic-assisted ovariohysterectomy for treatment of canine pyometra. Veterinary Surgery 42, 572–578 doi:10.1111/j.1532-950X.2013.12012.x [DOI] [PubMed] [Google Scholar]
- Austin B., Lanz O. I., Hamilton S. M., Broadstone R. V., Martin R. A. (2003) Laparoscopic ovariohysterectomy in nine dogs. Journal of the American Animal Hospital Association 39, 391–396 doi:10.5326/0390391 [DOI] [PubMed] [Google Scholar]
- Bloomberg M. S. (1996) Surgical neutering and nonsurgical alternatives. Journal of the American Veterinary Medical Association 208, 517–519 [PubMed] [Google Scholar]
- Case J. B., Marvel S. J., Boscan P., Monnet E. L. (2011) Surgical time and severity of postoperative pain in dogs undergoing laparoscopic ovariectomy with one, two, or three instrument cannulas. J Am Vet Med Assoc 239, 203–208 [DOI] [PubMed] [Google Scholar]
- Case J. B., Ellison G. (2013) Single incision laparoscopic-assisted intestinal surgery (SILAIS) in 7 dogs and 1 cat. Veterinary Surgery 42, 629–634 doi:10.1111/j.1532-950X.2013.12017.x [DOI] [PubMed] [Google Scholar]
- Coisman J. G., Case J. B., Clark N. D., Wellehan J. F., Ellison G. W. (2013) Efficacy of decontamination and sterilization of a single-use single-incision laparoscopic surgery port. American Journal of Veterinary Research 74, 934–938 doi:10.2460/ajvr.74.6.934 [DOI] [PubMed] [Google Scholar]
- Coisman J. G., Case J. B., Shih A., Harrison K., Isaza N., Ellison G. (2014) Comparison of surgical variables in cats undergoing single-incision laparoscopic ovariectomy using a LigaSure or extracorporeal suture versus open ovariectomy. Veterinary Surgery 43, 38–44 doi:10.1111/j.1532-950X.2013.12073.x [DOI] [PubMed] [Google Scholar]
- Davidson E. B., Moll H. D., Payton M. E. (2004) Comparison of laparoscopic ovariohysterectomy and ovariohysterectomy in dogs. Veterinary Surgery 33, 62–69 doi:10.1111/j.1532-950X.2004.04003.x [DOI] [PubMed] [Google Scholar]
- Devitt C. M., Cox R. E., Hailey J. J. (2005) Duration, complications, stress, and pain of open ovariohysterectomy versus a simple method of laparoscopic-assisted ovariohysterectomy in dogs. Journal of the American Veterinary Medical Association 227, 921–927 doi:10.2460/javma.2005.227.921 [DOI] [PubMed] [Google Scholar]
- Dupre G., Fiorbianco V., Skalicky M., Gultiken N., Ay S. S., Findik M. (2009) Laparoscopic ovariectomy in dogs: comparison between single portal and two-portal access. Veterinary Surgery 38, 818–824 doi:10.1111/j.1532-950X.2009.00601.x [DOI] [PubMed] [Google Scholar]
- Emerson J. A., Case J. B., Brock A. P., Vigani A., Graham D. R., Isaza R. (2013) Single-incision, multicannulated, laparoscopic ovariectomy in two tigers (Panthera tigris). Veterinary Quarterly 33, 108–111 doi:10.1080/01652176.2013.783951 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fingland R. B. (1998) Ovariohysterectomy. In: Current Techniques in Small Animal Surgery. Ed. Bojrab M. J. Baltimore: Williams & Wilkins; pp 489–496 [Google Scholar]
- Freeman A., MacFarlane P. (2007) Laparoscopic ovariohysterectomy in dogs. The Veterinary Record 160, 812 doi:10.1136/vr.160.23.812-a [DOI] [PubMed] [Google Scholar]
- Gower S., Mayhew P. (2008) Canine laparoscopic and laparoscopic-assisted ovariohysterectomy and ovariectomy. Compendium 30, 430–432, 434, 436, 438, 440 [PubMed] [Google Scholar]
- Hancock R. B., Lanz O. I., Waldron D. R., Duncan R. B., Broadstone R. V., Hendrix P. K. (2005) Comparison of postoperative pain after ovariohysterectomy by harmonic scalpel-assisted laparoscopy compared with median celiotomy and ligation in dogs. Veterinary Surgery 34, 273–282 doi:10.1111/j.1532-950x.2005.00041.x [DOI] [PubMed] [Google Scholar]
- Hedlund C. S. (1997) Surgery of the reproductive and genital systems. In Small Animal Surgery. Ed. Fossum T. W. St. Louis: Mosby-Year Book Inc; pp 523–524. 536–537 [Google Scholar]
- Howe L. M. (2006) Surgical methods of contraception and sterilization. Theriogenology 66, 500–509 doi:10.1016/j.theriogenology.2006.04.005 [DOI] [PubMed] [Google Scholar]
- Khalaj A., Bakhtiari J., Niasari-Naslaji A. (2012) Comparison between single and three portal laparoscopic splenectomy in dogs. BMC Veterinary Research 8, 161 doi:10.1186/1746-6148-8-161 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kilkenny C., Browne W. J., Cuthill I. C., Emerson M., Altman D. G. (2010) Improving bioscience research reporting: the ARRIVE guidelines for reporting animal research. PLoS Biol 8, e1000412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim Y. K., Lee S. S., Suh E. H., Lee L., Lee H. C., Lee H. J., Yeon S. C. (2012) Sprayed intraperitoneal bupivacaine reduces early postoperative pain behavior and biochemical stress response after laparoscopic ovariohysterectomy in dogs. Veterinary Journal 191, 188–192 doi:10.1016/j.tvjl.2011.02.013 [DOI] [PubMed] [Google Scholar]
- Manassero M., Leperlier D., Vallefuoco R., Viateau V. (2012) Laparoscopic ovariectomy in dogs using a single-port multiple-access device. The Veterinary Record 171, 69 doi:10.1136/vr.100060 [DOI] [PubMed] [Google Scholar]
- Mayhew P. D. (2014) Recent advances in soft tissue minimally invasive surgery. The Journal of Small Animal Practice 55, 75–83 doi:10.1111/jsap.12164 [DOI] [PubMed] [Google Scholar]
- Mayhew P. D., Brown D. C. (2007) Comparison of three techniques for ovarian pedicle hemostasis during laparoscopic-assisted ovariohysterectomy. Veterinary Surgery 36, 541–547 doi:10.1111/j.1532-950X.2007.00280.x [DOI] [PubMed] [Google Scholar]
- Mittermair C., Schirnhofer J., Brunner E., Pimpl K., Obrist C., Weiss M., Weiss H. G. (2014) Single port laparoscopy in gastroenterology and hepatology: a fine step forward. World J Gastroenterol 20, 15599–15607 doi:10.3748/wjg.v20.i42.15599 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Runge J. J., Curcillo P. G. II, King S. A., Podolsky E. R., Holt D. E., Davidson J., Agnello K. A. (2012) Initial application of reduced port surgery using the single port access technique for laparoscopic canine ovariectomy. Veterinary Surgery 41, 803–806 doi:10.1111/j.1532-950X.2012.01012.x [DOI] [PubMed] [Google Scholar]
- Runge J. J., Holt D. E. (2012) Initial experience with laparoendoscopic single site (LESS) cryptorchidectomy using the Triport+ and a articulating telescope in dogs and cats. Proceedings of the Veterinary Endoscopy Society 9th Annual Meeting Park City, Utah [Google Scholar]
- Runge J. J., Mayhew P. D. (2013) Evaluation of single port access gastropexy and ovariectomy using articulating instruments and angled telescopes in dogs. Veterinary Surgery 42, 807–813 doi:10.1111/j.1532-950X.2013.12036.x [DOI] [PubMed] [Google Scholar]
- Runge J. J., Mayhew P. D., Case J. B., Singh A., Mayhew K. N., Culp W. T. (2014) Single-port laparoscopic cryptorchidectomy in dogs and cats: 25 cases (2009–2014). Journal of the American Veterinary Medical Association 245, 1258–1265 doi:10.2460/javma.245.11.1258 [DOI] [PubMed] [Google Scholar]
- Saber A. A., Elgamal M. H., Itawi E. A., Rao A. J. (2008) Single incision laparoscopic sleeve gastrectomy (SILS): a novel technique. Obesity Surgery 18,1338–1342 [DOI] [PubMed] [Google Scholar]
- Sanchez-Margallo F. M., Matos-Azevedo A. M., Perez-Duarte F. J., Enciso S., Martin-Portugues I. D. (2014) Performance analysis on physical simulator of four different instrument setups in laparo-endoscopic single-site (LESS) surgery. Surgical Endoscopy 28, 1479–1488 doi:10.1007/s00464-013-3337-1 [DOI] [PubMed] [Google Scholar]
- Santos B. F., Enter D., Soper N. J., Hungness E. S. (2011) Single-incision laparoscopic surgery (SILS) versus standard laparoscopic surgery: a comparison of performance using a surgical simulator. Surg Endosc 25, 483–490 [DOI] [PubMed] [Google Scholar]
- Van Nimwegen S. A., Kirpenstein J. (2007) Comparison of Nd:YAG surgical laser and Remorgida bipolar electrosurgery forceps for canine laparoscopic ovariectomy. Veterinary Surgery 36, 533–540 [DOI] [PubMed] [Google Scholar]
- Wilson D. M., Monnet E. L. (2012) The use of single incision laparoscopic surgery (SILS Port) in dogs: description of the technique and initial impressions after 22 consecutive cases. Proceedings of the 9th annual meeting of the Veterinary Endoscopy Society, Park City, UT, March 22-24. [Google Scholar]