

Abstract
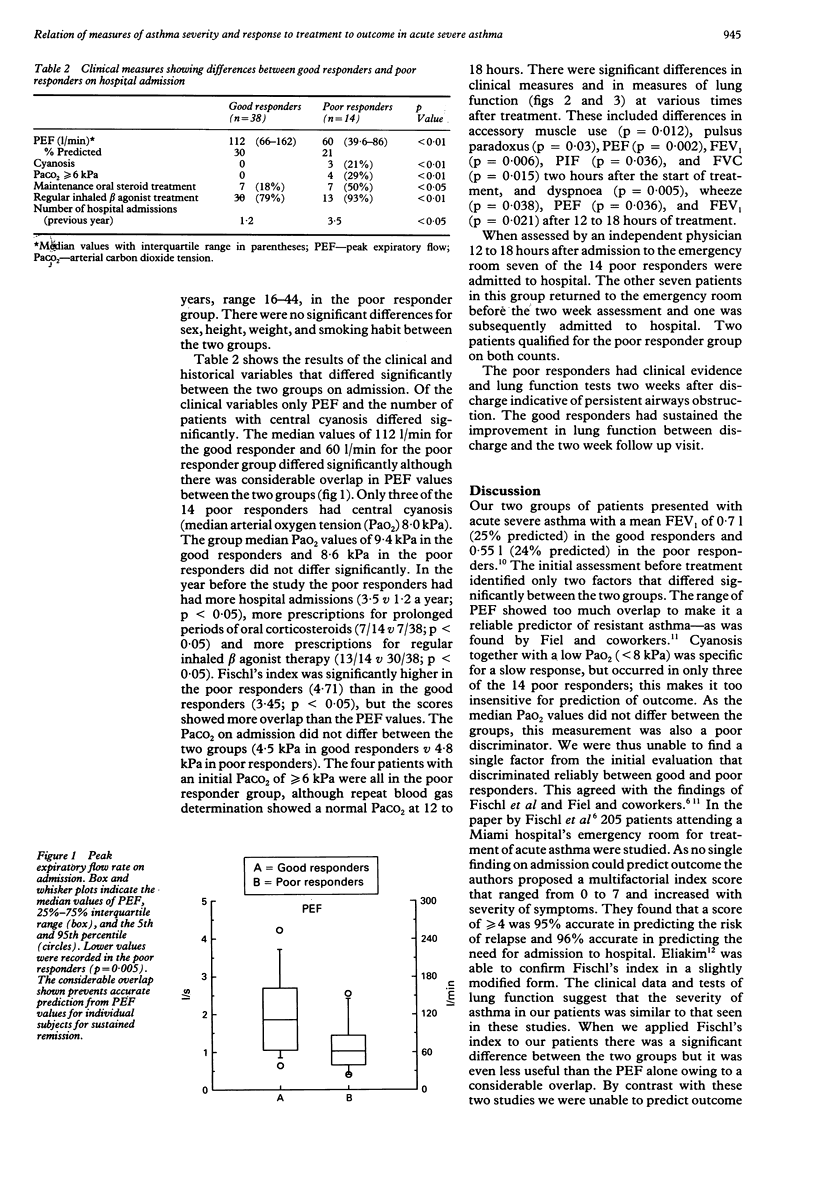
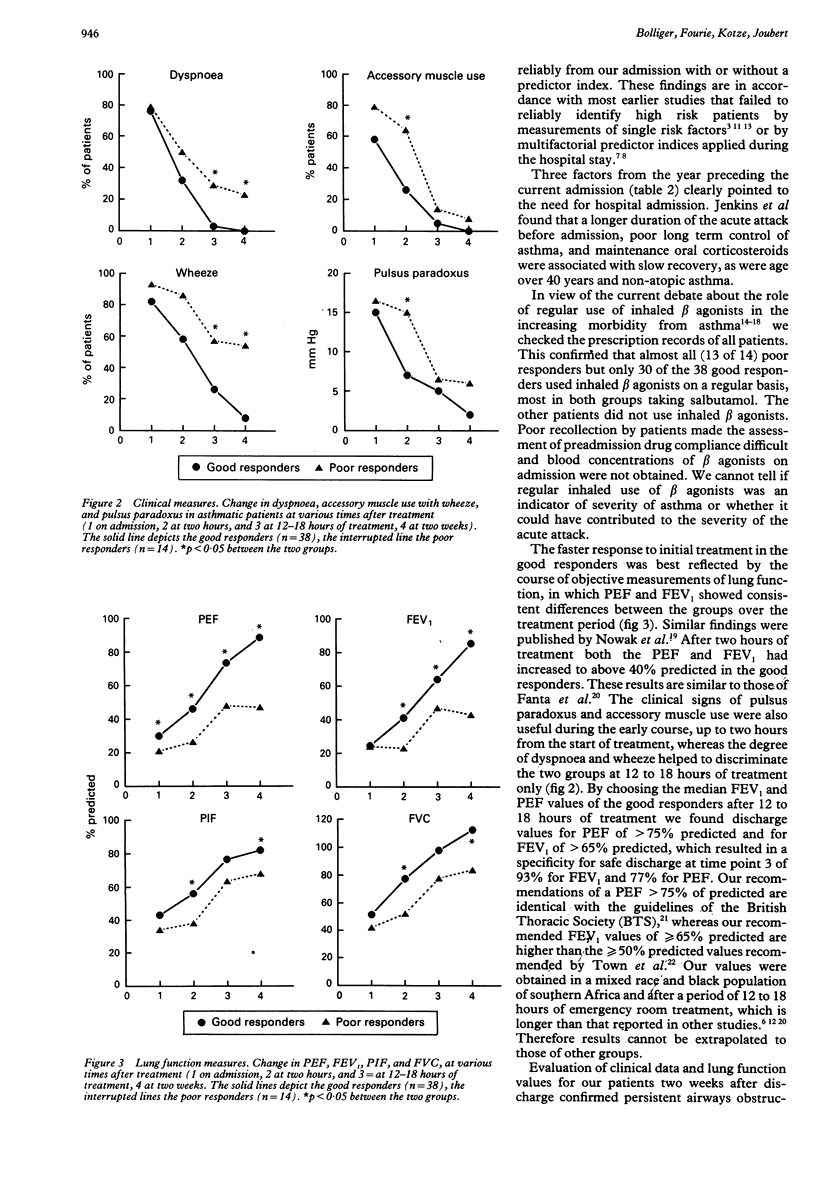
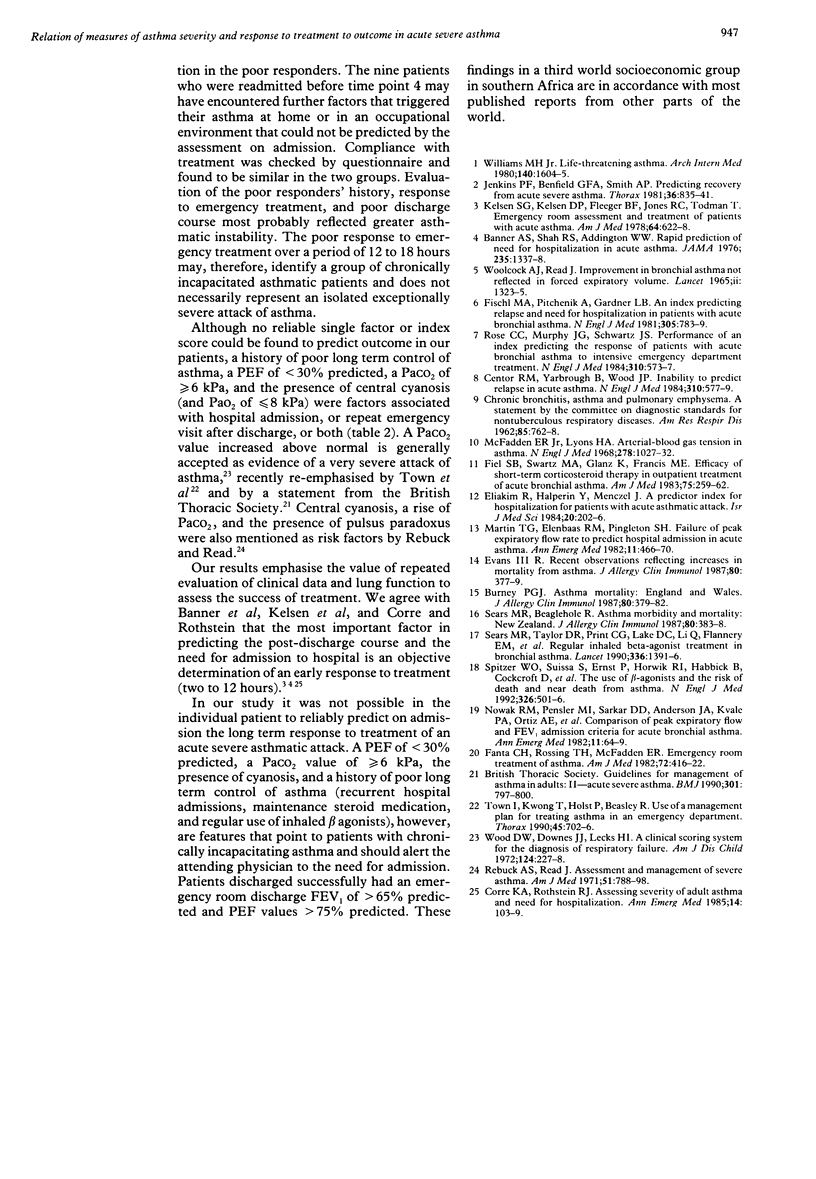
BACKGROUND: It would be helpful if patients with asthma who require admission to hospital for an acute attack could be identified. METHODS: The relation between the severity of an attack of asthma as determined by admission assessment and the eventual outcome was studied in 52 asthmatic patients aged 14 to 44 years and admitted to an asthma emergency room. The patient's history, including medication and previous admissions to hospital, was recorded and a clinical assessment, including a full inspiratory and expiratory flow-volume loop, was performed on four occasions: on admission, at two hours and at 12-18 hours after the start of a standardised treatment, and two weeks later on an outpatient basis. Patients who were discharged and who had an uneventful follow up at the two week assessment were defined as good responders. Patients who had to be admitted to hospital after 12 to 18 hours or were readmitted during the two weeks, or both, were defined as poor responders. RESULTS: Thirty eight patients were good responders and 14 were poor responders (seven admitted at 12 to 18 hours, seven returned to hospital). All four patients with a raised arterial carbon dioxide tension (PaCO2) (> or = 6 kPa) and the three with cyanosis were in the poor responder group, and this group had lower peak expiratory flow (PEF) values (21% v 30% predicted) on admission. There was, however, considerable overlap in PEF between the two groups and no clinical measure was able to distinguish between the good and the poor responders reliably. Poor responders had a history of more chronic systemic steroid administration, regular use of inhaled beta agonists, and asthma related hospital admissions. Nearly all the subjects showing a good response to standardised treatment had a PEF > 75% predicted and an FEV1 > 65% predicted 12 to 18 hours after the start of treatment. CONCLUSION: Prediction of outcome at admission was not possible in individual patients. A history of poor long term control of asthma, a PEF < 30% of predicted, a PaCO2 > or = 6 kPa, the presence of cyanosis, and lack of early response to treatment indicated a group of asthmatic patients who are less likely to respond to conventional emergency treatment over a short period.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Banner A. S., Shah R. S., Addington W. W. Rapid prediction of need for hospitalization in acute asthma. JAMA. 1976 Mar 29;235(13):1337–1338. [PubMed] [Google Scholar]
- Burney P. G. Asthma mortality: England and Wales. J Allergy Clin Immunol. 1987 Sep;80(3 Pt 2):379–382. doi: 10.1016/0091-6749(87)90054-6. [DOI] [PubMed] [Google Scholar]
- Centor R. M., Yarbrough B., Wood J. P. Inability to predict relapse in acute asthma. N Engl J Med. 1984 Mar 1;310(9):577–580. doi: 10.1056/NEJM198403013100907. [DOI] [PubMed] [Google Scholar]
- Eliakim R., Halperin Y., Menczel J. A predictor index for hospitalization for patients with acute asthmatic attack. Isr J Med Sci. 1984 Mar;20(3):202–206. [PubMed] [Google Scholar]
- Evans R., 3rd Recent observations reflecting increases in mortality from asthma. J Allergy Clin Immunol. 1987 Sep;80(3 Pt 2):377–379. doi: 10.1016/0091-6749(87)90053-4. [DOI] [PubMed] [Google Scholar]
- Fanta C. H., Rossing T. H., McFadden E. R., Jr Emergency room of treatment of asthma. Relationships among therapeutic combinations, severity of obstruction and time course of response. Am J Med. 1982 Mar;72(3):416–422. doi: 10.1016/0002-9343(82)90498-3. [DOI] [PubMed] [Google Scholar]
- Fiel S. B., Swartz M. A., Glanz K., Francis M. E. Efficacy of short-term corticosteroid therapy in outpatient treatment of acute bronchial asthma. Am J Med. 1983 Aug;75(2):259–262. doi: 10.1016/0002-9343(83)91202-0. [DOI] [PubMed] [Google Scholar]
- Fischl M. A., Pitchenik A., Gardner L. B. An index predicting relapse and need for hospitalization in patients with acute bronchial asthma. N Engl J Med. 1981 Oct 1;305(14):783–789. doi: 10.1056/NEJM198110013051402. [DOI] [PubMed] [Google Scholar]
- Jenkins P. F., Benfield G. F., Smith A. P. Predicting recovery from acute severe asthma. Thorax. 1981 Nov;36(11):835–841. doi: 10.1136/thx.36.11.835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kelsen S. G., Kelsen D. P., Fleeger B. F., Jones R. C., Rodman T. Emergency room assessment and treatment of patients with acute asthma. Adequacy of the conventional approach. Am J Med. 1978 Apr;64(4):622–628. doi: 10.1016/0002-9343(78)90582-x. [DOI] [PubMed] [Google Scholar]
- Martin T. G., Elenbaas R. M., Pingleton S. H. Failure of peak expiratory flow rate to predict hospital admission in acute asthma. Ann Emerg Med. 1982 Sep;11(9):466–470. doi: 10.1016/s0196-0644(82)80063-2. [DOI] [PubMed] [Google Scholar]
- McFadden E. R., Jr, Lyons H. A. Arterial-blood gas tension in asthma. N Engl J Med. 1968 May 9;278(19):1027–1032. doi: 10.1056/NEJM196805092781901. [DOI] [PubMed] [Google Scholar]
- Nowak R. M., Pensler M. I., Sarkar D. D., Anderson J. A., Kvale P. A., Ortiz A. E., Tomlanovich M. C. Comparison of peak expiratory flow and FEV1 admission criteria for acute bronchial asthma. Ann Emerg Med. 1982 Feb;11(2):64–69. doi: 10.1016/s0196-0644(82)80298-9. [DOI] [PubMed] [Google Scholar]
- Rose C. C., Murphy J. G., Schwartz J. S. Performance of an index predicting the response of patients with acute bronchial asthma to intensive emergency department treatment. N Engl J Med. 1984 Mar 1;310(9):573–577. doi: 10.1056/NEJM198403013100906. [DOI] [PubMed] [Google Scholar]
- Sears M. R., Beaglehole R. Asthma morbidity and mortality: New Zealand. J Allergy Clin Immunol. 1987 Sep;80(3 Pt 2):383–388. doi: 10.1016/0091-6749(87)90055-8. [DOI] [PubMed] [Google Scholar]
- Sears M. R., Taylor D. R., Print C. G., Lake D. C., Li Q. Q., Flannery E. M., Yates D. M., Lucas M. K., Herbison G. P. Regular inhaled beta-agonist treatment in bronchial asthma. Lancet. 1990 Dec 8;336(8728):1391–1396. doi: 10.1016/0140-6736(90)93098-a. [DOI] [PubMed] [Google Scholar]
- Spitzer W. O., Suissa S., Ernst P., Horwitz R. I., Habbick B., Cockcroft D., Boivin J. F., McNutt M., Buist A. S., Rebuck A. S. The use of beta-agonists and the risk of death and near death from asthma. N Engl J Med. 1992 Feb 20;326(8):501–506. doi: 10.1056/NEJM199202203260801. [DOI] [PubMed] [Google Scholar]
- Town I., Kwong T., Holst P., Beasley R. Use of a management plan for treating asthma in an emergency department. Thorax. 1990 Sep;45(9):702–706. doi: 10.1136/thx.45.9.702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams M. H., Jr Life-threatening asthma. Arch Intern Med. 1980 Dec;140(12):1604–1605. [PubMed] [Google Scholar]
- Wood D. W., Downes J. J., Lecks H. I. A clinical scoring system for the diagnosis of respiratory failure. Preliminary report on childhood status asthmaticus. Am J Dis Child. 1972 Mar;123(3):227–228. doi: 10.1001/archpedi.1972.02110090097011. [DOI] [PubMed] [Google Scholar]
- Woolcock A. J., Read J. Improvement in bronchial asthma not reflected in forced expiratory volume. Lancet. 1965 Dec 25;2(7426):1323–1325. doi: 10.1016/s0140-6736(65)92343-3. [DOI] [PubMed] [Google Scholar]