

Abstract
Background
Orthopaedic surgeons often work under the assumption that patients over 60 are low-demand individuals. This study addressed the primary null hypothesis that older age does not correlate with the enjoyment of physical activities in patients with upper extremity illness. Secondary analyses sought factors associated with enjoyment of physical activity, activity level and magnitude of disability.
Methods
A cohort of 98 new and follow-up outpatients with upper extremity illnesses completed a measure of enjoyment of physical activity (Physical Activity Enjoyment Scale (PACES)), were categorized into one of three levels of activity after interview, and completed measures of general disability (Patient-Reported Outcomes Measurement Information System (PROMIS) Physical Function CAT), upper extremity-specific disability (Quick Disability of the Arm, Shoulder and Hand (QuickDASH) score), coping responses to pain (PROMIS Pain Interference CAT), and symptoms of depression (PROMIS Depression CAT).
Results
Greater enjoyment of physical activity correlated with older age (r = 0.29, p = 0.0039) but not with other explanatory variables. The final multivariable model of factors associated with greater physical activity included older age and male sex. The final multivariable model of factors associated with diminished PROMIS Physical Function included greater PROMIS Pain Interference, male sex, other pain conditions, and separated/divorced and single marital status and accounted for 34 % of the variance.
Conclusions
Enjoyment of physical activity does not decrease with age. Patient-specific expectations, goals and preferences for physical activity should be assessed prior to decision-making on treatment.
Level of Evidence: Level IV, Prognostic Study case series
Keywords: Ageing, Enjoyment, Activity, Upper, Extremity, Illness
Introduction
Orthopaedic surgeons have conventionally worked on the assumption that many people over age 60 tend to be content with a low-demand lifestyle. Age alone is shown to be a poor predictor of activity level with a high degree of individual variability [12, 22]. In the USA, people are increasingly active at older ages [23, 26]. Conversely, rising levels of obesity may be associated with lower activity levels amongst younger people on average [5, 14]. Perhaps surgeons should consider each individual’s enjoyment of physical activity and desired activity level [6, 20, 22].
Older patients are more disabled on average [1, 9, 18], but the relationship between age and enjoyment of physical activities is not as well studied [17]. It is our impression that enjoyment of physical activities may not correlate with chronological age.
The objective of this study was to determine the relationship between age and the enjoyment of physical activity, activity level and disability, taking demographic and psychosocial factors into consideration amongst patients suffering conditions involving the upper limb.
This study addresses the null hypothesis that older age does not correlate with the enjoyment of physical activities in patients with upper extremity illness. In secondary analyses, we looked for correlation of enjoyment of physical activities with other factors including categorical level of activity and Patient-Reported Outcomes Measurement Information System (PROMIS) physical function and factors associated with categorical activity level and PROMIS Physical Function accounting for demographic, diagnostic and psychosocial factors.
Materials and Methods
Between August 2013 and September 2013, new and follow-up outpatients presenting to the hand surgery outpatient clinic of three orthopaedic hand surgeons were invited to participate. Pregnant women, patients younger than 18 years and subjects unable to communicate in English were excluded. This observational cross-sectional study was approved by an institutional review board and verbal informed consent was obtained from all individual participants.
Amongst the 105 invited patients who fulfilled our eligibility criteria, 7 patients declined participation, resulting in a final sample of 98 patients. There were 47 men and 51 women with an average age of 50 ± 18 years (range 20–90 years) Table 1.
Table 1.
Patients demographics(n = 98)
| Mean | SD | Range | |
| Age, years | 50 | 18 | 20–90 |
| Education, years | 16 | 2.6 | 12–25 |
| n | % | ||
| Sex | |||
| Women | 51 | 52 | |
| Men | 47 | 48 | |
| Work status | |||
| Working full time | 63 | 64 | |
| Working part time | 9 | 9.2 | |
| Homemaker | 1 | 1.0 | |
| Retired | 18 | 18 | |
| Unemployed, able to work | 0 | 0.0 | |
| Unemployed, unable to work | 4 | 4.1 | |
| Workers compensation | 1 | 1.0 | |
| Currently on sick leave | 2 | 2.0 | |
| Marital status | |||
| Single | 33 | 34 | |
| Living with partner | 1 | 1.0 | |
| Married | 51 | 52 | |
| Separated/divorced | 10 | 10 | |
| Widowed | 3 | 3.1 | |
| Other pain conditions | |||
| Yes | 24 | 24 | |
| No | 74 | 76 | |
| Mean | SD | Range | |
| Health-related outcomes | |||
| PACES | 5.9 | 0.91 | 3.6–7 |
| PROMIS Physical Function | 53 | 8.9 | 20–73 |
| PROMIS Depression | 46 | 11 | 34–78 |
| PROMIS Pain Interference | 52 | 10 | 39–84 |
| Activity level | 2.2 | 0.78 | 1–3 |
| QuickDASH | 23 | 20 | 0–89 |
Patients completed the Physical Activity Enjoyment Scale (PACES); PROMIS Physical Function; Quick Disability of the Arm, Shoulder and Hand (QuickDASH) score; PROMIS Pain Interference (CAT); and the PROMIS Depression (CAT) instruments. Patients also completed a demographic survey and were asked to describe the physical activities they were involved in.
The PACES is an 18-item measure of enjoyment of physical activities. Respondents are asked “Please rate how you feel at the moment about the physical activity you have been doing” using a 7-point ordinal rating scale anchored at each end by opposing statements, e.g. “It’s very exhilarating” versus “It’s not at all exhilarating”. Eleven items are negatively worded and in these items lower scores reflect greater levels of enjoyment. The scores of these items were reversed in the statistical analysis. Higher PACES scores reflect greater levels of enjoyment of physical activity (range 18 to 126) [15]. It was originally developed using young adults but has been modified to provide a validated measure of activity in older patients [17].
Physical activity levels were based on the patient’s verbal responses to the question: “Which physical activities are you involved in?” Responses were recorded verbatim and subsequently categorized by two independent assessors according to a three-part activity level classification established by the US Department of Health and Human Services Center for Disease Control and Prevention (CDC) and the US Department of Health and Human Services [23, 24, 25].
The PROMIS CAT instrument scores range from 0 to 100, with an average score of 50 points in the general US population. The PROMIS Pain Interference and Depression instruments assess negatively worded items, with higher scores reflecting higher levels of pain interference and depression, respectively. For positively worded questionnaires, such as the PROMIS Physical Function, a high score indicates a high level of physical function [4, 20]. All PROMIS items employ five responses, i.e. 1 = Not at all, 2 = A little bit, 3 = Somewhat, 4 = Quite a bit, or 5 = Very much.
The PROMIS Physical Function questionnaire assesses one’s ability to perform physical activities, ranging from low-impact tasks (e.g. bathing and dressing) to vigorous physical activities (e.g. running, strenuous sports). The questions do not refer to a particular recall period but involve the participant’s status at the time of completion [4, 11, 21].
The PROMIS Depression questionnaire addresses the presence and severity of depressive symptoms in the past 7 days. The PROMIS Depression item bank is constructed from the full 28-item question bank [7, 19].
The PROMIS Pain Interference assesses the consequences of pain on common aspects of daily life. This incorporates social, cognitive, emotional, physical and recreational aspects. An automatically generated selection of subsequent items is made from the full 41-item question bank [2].
Upper extremity-specific disability is measured with the QuickDASH, an 11-item questionnaire where items are answered on a 5-point Likert scale [3]. The overall score ranges from 0 (no disability) to 100 (most severe disability) with a score of 11 points reflecting the mean score for the general US population [3, 8, 10].
Statistical Analysis
An a priori power analysis for the primary null hypothesis indicated that a minimum sample size of 98 patients would provide 80 % power to detect a 0.3 correlation between age and PACES (alpha 0.05).
Bivariable and multivariable analyses were conducted to test our hypotheses. The Pearson and Spearman’s rank correlation tests were conducted to assess normally and non-normally distributed quantitative variables, respectively. The association between continuous variables and dichotomous variables was analyzed using the Wilcoxon rank-sum test for non-normally distributed data and with the Student’s t test for normally distributed data. The association between continuous variables and categorical variables (e.g. marital status, work status) was analyzed using the Kruskal-Wallis test in case of non-normally distributed and the one-way ANOVA test in case of normally distributed data.
The extent to which variables were responsible for the variance in PACES, activity levels and physical function was determined with a backwards, stepwise, multivariable linear regression analysis. Factors included in the multivariable linear regression were explanatory variables that met the p < 0.10 significance criteria in bivariable factor analysis.
In order to be able to use all patients for the multivariable analysis, mean imputation was used for one missing PACES score.
Results
Greater enjoyment of physical activity (as measured by the PACES instrument) correlated with older age (r = 0.29, p = 0.0039) (Fig. 1).
Fig. 1.
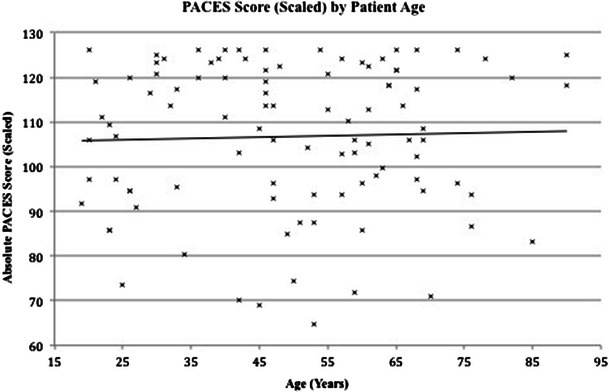
Correlation of patient age and enjoyment of physical activity (PACES)
PACES had no other correlations with demographic, diagnostic or psychosocial factors. PACES demonstrated positive correlation with both higher categorical activity level and PROMIS Physical Function (Table 2).
Table 2.
Bivariate analysis of PACES, activity level and PROMIS Physical Function against demographic, diagnostic and psychosocial factors
| PACES | Activity level | PROMIS Physical Function | ||||
|---|---|---|---|---|---|---|
| Sex | Mean (SD) | p value | Mean (SD) | p value | Mean (SD) | p value |
| Men | 6.0 (0.93) | 0.67 | 2.5 (0.72) | 0.0024 | 56 (8.1) | 0.0068 |
| Women | 5.9 (0.91) | 2.0 (0.77) | 51 (9.0) | |||
| Marital status | ||||||
| Single | 5.9 (0.82) | 0.55 | 2.3 (0.76) | 0.74 | 51 (6.9) | 0.018 |
| Living with partner | 6.7 (0) | 3.0 (0) | 64 (0) | |||
| Married | 5.8 (1.0) | 2.2 (0.76) | 54 (10) | |||
| Separated/divorced | 6.3 (0.60) | 2.0 (0.94) | 59 (6.7) | |||
| Widowed | 6.3 (0.82) | 2.3 (1.2) | 56 (4.3) | |||
| Work status | ||||||
| Working full time | 5.8 (0.95) | 0.26 | 2.3 (0.78) | 0.76 | 55 (8.2) | 0.12 |
| Working part time | 5.9 (0.90) | 2.1 (0.93) | 55 (8.0) | |||
| Homemaker | 5.2 (0) | 2.0 (0) | 50 (0) | |||
| Retired | 6.3 (0.84) | 2.2 (0.79) | 53 (6.9) | |||
| Unemployed, unable to work | 6.3 (0.75) | 2.0 (0.82) | 49 (10) | |||
| Workers’ compensation | 6.1 (0) | 2.0 (0) | 36 (0) | |||
| Currently on sick leave | 5.7 (0.82) | 1.5 (0.71) | 28 (12) | |||
| Acute/chronic | ||||||
| Acute new patient | 5.8 (0.94) | 0.3 | 2.4 (0.72) | 0.27 | 54 (6.5) | 0.93 |
| Acute operative patient | 5.9 (0.87) | 2.4 (0.84) | 52 (11) | |||
| Acute non-operative patient | 5.9 (1.0) | 2.2 (0.79) | 54 (9.7) | |||
| Chronic new patient | 6.3 (0.83) | 2.0 (0.79) | 55 (5.8) | |||
| Chronic operative patient | 5.8 (1.0) | 1.5 (1.0) | 45 (18) | |||
| Chronic non-operative patient | 5.7 (0.79) | 2.3 (0.65) | 54 (8.1) | |||
| Trauma/non-trauma | ||||||
| Trauma | 5.9 (0.97) | 0.51 | 2.3 (0.77) | 0.44 | 53 (8.6) | 0.58 |
| Non-trauma | 6.0 (0.82) | 2.2 (0.80) | 54 (9.4) | |||
| Other pain condition | ||||||
| Yes | 5.7 (1.1) | 0.25 | 2.1 (0.80) | 0.46 | 49 (10) | 0.039 |
| No | 6.0 (0.84) | 2.3 (0.78) | 55 (8.1) | |||
| Continuous measures | Coef. | p value | Coef. | p value | Coef. | p value |
| Age | 0.29 | 0.0039 | −0.17 | 0.095 | 0.094 | 0.36 |
| Years of education | −0.0031 | 0.98 | 0.15 | 0.14 | 0.24 | 0.016 |
| PACES | N/A | N/A | 0.22 | 0.027 | 0.31 | 0.0018 |
| PROMIS Physical Function | 0.31 | 0.0018 | 0.3 | 0.0031 | N/A | N/A |
| PROMIS Depression | −0.094 | 0.36 | −0.042 | 0.68 | −0.18 | 0.085 |
| PROMIS Pain Interference | −0.15 | 0.14 | 0.059 | 0.56 | −0.39 | <0.001 |
| Activity level | 0.22 | 0.027 | N/A | N/A | 0.3 | 0.0031 |
| QuickDASH | −0.094 | 0.36 | −0.025 | 0.81 | −0.5 | <0.001 |
Categorical activity level did not correlate with age, but men were more active (Table 2). The only significant contributor to the final multivariable model of factors associated with activity level was sex accounting for 8.1 % of the variance (Table 3).
Table 3.
Multivariable analysis of predictive factors for activity level
| Activity level | Coef. | Part. R-squared | SE | p value | Adj. R-squared | 95 % CI | ||
|---|---|---|---|---|---|---|---|---|
| Sex | 0.47 | 0.091 | 0.15 | 0.0030 | 0.081 | 0.17 | 0.77 | |
In model: sex, age
Disability (PROMIS Physical Function) did not correlate with age but was associated with male sex, PROMIS Pain Interference, marital status, presence of other pain conditions, and years of education (Table 2). Male sex and separated/divorced marital status demonstrated positive correlation with PROMIS Physical Function. The final multivariable model of factors associated with PROMIS Physical Function included PROMIS Pain Interference (by far the strongest factor, beta = −0.31, partial R-squared = 0.14, p < 0.001) and combined with male sex, presence of other pain conditions and separated/divorced and single marital status, accounted for 34 % of the variance (Table 4).
Table 4.
Multivariable analysis of predictive factors for disability (PROMIS Physical Function)
| PROMIS Physical Function | Coef. | Part. R-squared | SE | p value | Adj. R-squared | 95 % CI | |
|---|---|---|---|---|---|---|---|
| PROMIS Pain Interference | −0.31 | 0.14 | 0.078 | <0.001 | −0.46 | −0.15 | |
| Sex | 4.1 | 0.074 | 1.5 | 0.0080 | 1.1 | 7.0 | |
| Other pain conditions | −4.5 | 0.059 | 1.9 | 0.019 | 0.34 | −8.2 | −0.76 |
| Marital status: separated/divorced | 7.1 | 0.079 | 2.5 | 0.0060 | 2.1 | 12 | |
| Marital status: single | −3.3 | 0.040 | 1.7 | 0.052 | −6.7 | 0.0 |
In model: sex, marital status, other pain conditions, education, PROMIS Pain Interference, PROMIS depression
Discussion
Ageing is associated with a wide spectrum of physiological changes and gradual overall decline in physical performance [16] that may or may not correspond with decreasing enjoyment of physical activity. Indeed, our data suggests that older patients enjoyed performing physical activities more than younger adults.
The reader should consider the following limitations to this study. The PACES instrument was validated with respect to specific activities such as fitness-orientated aerobic activity and may not apply to physical activities in general. The relationship between age and enjoyment of physical activity may vary by geographical, socioeconomic and cultural factors. Finally, we accidently scored the items on the PACES instrument on 8-point rather than 7-point ordinal scales. This was easily addressed by scaling the resulting scores and probably had little impact on the results.
Consistent with prior studies, (1) men were more active than women and had less disability [27] and (2) coping strategies were the most important contributor to disability. The findings of this study further the increasing understanding that disability relates less upon physical impairment, including age-related impairment, than to adaptation and resilience. Optimizing resilience and minimizing depression are shown to have significant associations with self-rated successful ageing [13]. This is particularly important in the context of the growing public health initiatives to understand and promote health and wellbeing in the elderly.
Given that age does not correlate with categorical activity level, and has inconsistent and small correlations with disability, we recommend that chronological age no longer be considered when making treatment decisions. With an increased emphasis on greater patient involvement in decision-making, we anticipate that demographic factors will have less influence on treatment choices than patient preferences and values.
Acknowledgments
Conflict of Interest
Prakash Jayakumar is a paid consultant for Johnson and Johnson Surgical Innovation/Janssen Healthcare Innovation. Celeste L. Overbeek has no conflicts of interest. David C. Ring is a paid consultant for Wright Medical and Skeletal Dynamics; has provided paid expert testimony for multiple malpractice and personal injury lawsuits; has received grants for the institution from Biomet and Skeletal Dynamics; has received payment for lectures as honoraria and per diem from AO North America, AO International and Several universities; has received paid royalties by Wright Medical and non-paid contracted work from Skeletal Dynamics, Medartis and Biomet; has stock with Illuminos; and is a paid deputy editor of the Journal of Hand Surgery, and Clinical Orthopaedics and Related Research, and non-paid deputy editor of Journal of Orthopaedic Trauma and Associate Editor of the Journal of Shoulder and Elbow Surgery.
Each author certifies that there were no grants or commercial associations (e.g. consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent
Informed consent was obtained from all patients for being included in the study.
Contributor Information
Prakash Jayakumar, Email: prakash.jayakumar@balliol.ox.ac.uk.
Celeste L. Overbeek, Email: coverbeek2706@gmail.com
David C. Ring, Phone: 617-726-4700, Email: dring@partners.org
References
- 1.Adamo DE, et al. The influence of age and physical activity on upper limb proprioceptive ability. J Aging Phys Act. 2009;17(3):272–293. doi: 10.1123/japa.17.3.272. [DOI] [PubMed] [Google Scholar]
- 2.Amtmann D, Cook KF, Jensen MP, et al. Development of a PROMIS item bank to measure pain interference. Pain. 2010;150(1):173–182. doi: 10.1016/j.pain.2010.04.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Beaton DE, Wright JG, Katz JN. Upper extremity collaborative group. Development of the QuickDASH: comparison of three item-reduction approaches. J Bone Joint Surg Am. 2005;87(5):1038–1046. doi: 10.2106/JBJS.D.02060. [DOI] [PubMed] [Google Scholar]
- 4.Cella D, Riley W, Stone A, et al. The patient-reported outcomes measurement information system (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005–2008. J Clin Epidemiol. 2010;63(11):1179–1194. doi: 10.1016/j.jclinepi.2010.04.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Deforche BI, De Bourdeaudhuij IM, Tanghe AP. Attitude toward physical activity in normal-weight, overweight and obese adolescents. J Adolesc Health. 2006;38(5):560–568. doi: 10.1016/j.jadohealth.2005.01.015. [DOI] [PubMed] [Google Scholar]
- 6.Dishman RK, Sallis JF, Orenstein DR. The determinants of physical activity and exercise. Public Health Rep. 1985;100:158–170. [PMC free article] [PubMed] [Google Scholar]
- 7.Gibbons LE, Feldman BJ, Crane HM, et al. Migrating from a legacy fixed-format measure to CAT administration: calibrating the PHQ-9 to the PROMIS depression measures. Qual Life Res. 2011;20(9):1349–1357. doi: 10.1007/s11136-011-9882-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gummesson C, Ward MM, Atroshi I. The shortened disabilities of the arm, shoulder and hand questionnaire (QuickDASH): validity and reliability based on responses within the full-length DASH. BMC Musculoskelet Disord. 2006;7:44. doi: 10.1186/1471-2474-7-44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hillsdon MM, Brunner EJ, Guralnik JM, et al. Prospective study of physical activity and physical function in early old age. Am J Prev Med. 2005;28(3):245–250. doi: 10.1016/j.amepre.2004.12.008. [DOI] [PubMed] [Google Scholar]
- 10.Hudak PL, Amadio PC, Bombardier C. Development of an upper extremity outcome measure: the DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collaborative Group (UECG) Am J Ind Med. 1996;29(6):602–608. doi: 10.1002/(SICI)1097-0274(199606)29:6<602::AID-AJIM4>3.0.CO;2-L. [DOI] [PubMed] [Google Scholar]
- 11.Hung M, Clegg DO, Greene T, et al. Evaluation of the PROMIS physical function item bank in orthopaedic patients. J Orthop Res. 2011;29(6):947–953. doi: 10.1002/jor.21308. [DOI] [PubMed] [Google Scholar]
- 12.Iorio R, Healy WL, Appleby D. Preoperative demand matching is a valid indicator of patient activity after total hip arthroplasty. J Arthroplasty. 2004;19(7):825–828. doi: 10.1016/j.arth.2004.03.014. [DOI] [PubMed] [Google Scholar]
- 13.Jeste DV, Savla GN, Thompson WK, et al. Association between older age and more successful aging: critical role of resilience and depression. Am J Psychiatry. 2013;170(2):188–196. doi: 10.1176/appi.ajp.2012.12030386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kelly AS, Barlow SE, Rao G, et al. Severe obesity in children and adolescents: identification, associated health risks, and treatment approaches: a scientific statement from the American Heart Association. Circulation. 2013;128(15):1689–1712. doi: 10.1161/CIR.0b013e3182a5cfb3. [DOI] [PubMed] [Google Scholar]
- 15.Kendzierski D, DeCarlo K. Physical activity enjoyment scale: two validation studies. J Sports Exerc Psychol. 1991;13:50–64. [Google Scholar]
- 16.Mahler DA, Cunningham LN, Curfman GD. Aging and exercise performance. Clin Geriatr Med. 1986;2(2):433–452. [PubMed] [Google Scholar]
- 17.Mullen SP, Olson EA, Phillips SM, et al. Measuring enjoyment of physical activity in older adults: invariance of the physical activity enjoyment scale (paces) across groups and time. Int J Behav Nutr Phys Act. 2011;8:103. doi: 10.1186/1479-5868-8-103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Paz SH, Spritzer KL, Morales LS, et al. Age-related differential item functioning for the patient-reported outcomes information system (PROMIS®) physical functioning items. Prim Health Care. 2013;3:131. doi: 10.4172/2167-1079.1000131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Pilkonis PA, Choi SW, Reise SP, et al. Item banks for measuring emotional distress from the patient-reported outcomes measurement information system (PROMIS(R)): depression, anxiety, and anger. Assessment. 2011;18(3):263–283. doi: 10.1177/1073191111411667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Rennemark M, Lindwall M, Halling A, et al. Relationships between physical activity and perceived qualities of life in old age. Results of the SNAC study. Aging Ment Health. 2009;13(1):1–8. doi: 10.1080/13607860802154416. [DOI] [PubMed] [Google Scholar]
- 21.Rose M, Bjorner JB, Becker J, et al. Evaluation of a preliminary physical function item bank supported the expected advantages of the patient-reported outcomes measurement information system (PROMIS) J Clin Epidemiol. 2008;61(1):17–33. doi: 10.1016/j.jclinepi.2006.06.025. [DOI] [PubMed] [Google Scholar]
- 22.Schmalzried TP, Szuszczewicz ES, Northfield MR, et al. Quantitative assessment of walking activity after total hip or knee replacement. J Bone Joint Surg Am. 1998;80:54. doi: 10.1302/0301-620X.80B1.7739. [DOI] [PubMed] [Google Scholar]
- 23.Wankel LM, Berger BG. The psychological and social benefits of sport and physical activity. J Leis Res. 1990;22(2):167–182. [Google Scholar]
- 24.Website: Available at: http://www.cdc.gov/nccdphp/dnpa/physical/pdf/PA_Intensity_table_2_1.pdf. Accessed January 1st 2014
- 25.Website: Available at: http://www.census.gov/prod/cen2010/briefs/c2010br-03.pdf. Accessed January 1st 2014.
- 26.Website: Available at: http://www.health.gov/paguidelines/pdf/paguide.pdf. Accessed January 1st 2014.
- 27.Website: Available at: http://www.who.int/gho/ncd/risk_factors/physical_activity_text/en/ Accessed January 1st 2014