

Abstract
Background/Aims:
Data regarding the outcomes of primary percutaneous coronary intervention (PCI) for ST-segment elevation myocardial infarction (STEMI) in nonagenarians are very limited. The aim of the present study was to evaluate the temporal trends and in-hospital outcomes of primary PCI in nonagenarian STEMI patients.
Methods:
We retrospectively reviewed data from the Korea Acute Myocardial Infarction Registry (KAMIR) from November 2005 to January 2008, and from the Korea Working Group on Myocardial Infarction (KorMI) from February 2008 to May 2010.
Results:
During this period, the proportion of nonagenarians among STEMI patients more than doubled (0.59% in KAMIR vs. 1.35% in KorMI), and the rate of use of primary PCI also increased (from 62.5% in KAMIR to 81.0% in KorMI). We identified 84 eligible study patients for which the overall in-hospital mortality rate was 21.4% (25.0% in KAMIR vs. 20.3% in KorMI, p = 0.919). Multivariate analysis identified two independent predictors of in-hospital mortality, namely a final Thrombolysis in Myocardial Infarction (TIMI) flow < 3 (odds ratio [OR], 13.7; 95% confidence interval [CI], 3.2 to 59.0; p < 0.001) and cardiogenic shock during hospitalization (OR, 6.7; 95% CI, 1.5 to 30.3; p = 0.013).
Conclusions:
The number of nonagenarian STEMI patients who have undergone primary PCI has increased. Although a final TIMI flow < 3 and cardiogenic shock are independent predictors of in-hospital mortality, primary PCI can be performed with a high success rate and an acceptable in-hospital mortality rate.
Keywords: In-hospital outcomes; Aged, 90 and over; Myocardial infarction; Percutaneous coronary intervention
INTRODUCTION
The very elderly (those ≥ 85 years of age) are the most rapidly growing population in Western countries. The mortality rate of this group increases markedly following ST-segment elevation myocardial infarction (STEMI) [1,2]. However, limited data are available regarding the outcomes of primary percutaneous coronary intervention (PCI) in this age group, especially in nonagenarians, who are generally excluded from clinical trials [3]. In the present study, we evaluated the temporal trends and in-hospital outcomes of primary PCI in nonagenarian STEMI patients using the Korea Acute Myocardial Infarction Registry (KAMIR) and Korea Working Group on Myocardial Infarction (KorMI) databases.
METHODS
Patient population
This study was conducted using data from the KAMIR and KorMI databases. The KAMIR is an online database from a Korean prospective multicenter registry. The purpose and methods used to register patients in the KAMIR have been described previously [4]. KorMI is an ongoing registry that began as a subsequent study to KAMIR. Patients were diagnosed with STEMI when they had a new ST-segment elevation ≥ 1 mm visible in any location, or a new left bundle branch block on the index or subsequent electrocardiogram, with ≥ 1 positive cardiac biochemical marker of necrosis (including creatine kinase-MB, troponin I, and troponin T). From November 2005 to May 2010, a total of 15,426 patients were diagnosed with STEMI. In the present study, we retrospectively analyzed STEMI patients aged ≥ 90 years who had undergone primary PCI within 12 hours of symptom onset. Comorbidity index scores were calculated using the Charlson comorbidity index [5].
PCI procedure
Loading doses of aspirin (200 to 300 mg) and clopidogrel (300 to 600 mg) were administered after obtaining written informed consent. Diagnostic angiography and PCI were performed after unfractionated heparin (50 to 70 U/kg) was administered through femoral or radial access. During the procedure, patients received additional doses of unfractionated heparin to obtain an activated clotting time > 250 seconds. The choice of stents, use of glycoprotein IIb/IIIa receptor inhibitors, and intra-aortic balloon pump were decided upon by individual surgeons. A successful PCI procedure was defined as the achievement of a Thrombolysis in Myocardial Infarction (TIMI) grade 3 flow and residual stenosis < 30% on the final angiography.
Study outcomes and definitions
The following outcomes were evaluated during hospitalization: death, cardiogenic shock, recurrent myocardial infarction, stroke, acute renal failure, and major bleeding. Recurrent myocardial infarction was defined as recurrent symptoms with new ST-segment elevation or re-elevation of cardiac markers to at least twice the upper limit. A stroke was defined as the presence of a new focal neurologic deficit believed to be vascular in origin, with signs or symptoms lasting more than 24 hours and confirmation using computed tomography or magnetic resonance imaging of the brain. Acute renal failure was defined as an increase in serum creatinine levels of 0.5 mg/dL. Major bleeding was defined as any intracranial bleeding, significant gastrointestinal bleeding, retroperitoneal bleeding, bleeding associated with the need for blood transfusion, or any other clinically relevant bleeding, as judged by the investigator.
Statistical analysis
Statistical analysis was performed using SPSS version 19.0 (IBM Co., Armonk, NY, USA). Continuous variables are presented as the mean ± standard deviation, and were compared using the Student t test. Categorical variables are presented as the number and percentage, and were compared using the chi-square test. Logistic regression analysis was used to determine independent predictors of in-hospital mortality. A p < 0.05 was considered statistically significant.
RESULTS
From November 2005 to May 2010, 84 patients aged ≥ 90 years who presented within 12 hours of symptom onset and underwent primary PCI for STEMI were enrolled in this study (Fig. 1). Although the total number of participants was small, the proportion of nonagenarians among STEMI patients more than doubled during the study period (0.59% in KAMIR vs. 1.35% in KorMI). Therefore, the growth rate was the highest in this age group (Fig. 2A). According to this trend, the rate of use of primary PCI in nonagenarians also increased to the level of the average rate of use for each different age group (from 62.5% in KAMIR to 81.0% in KorMI) (Fig. 2B).
Figure 1.
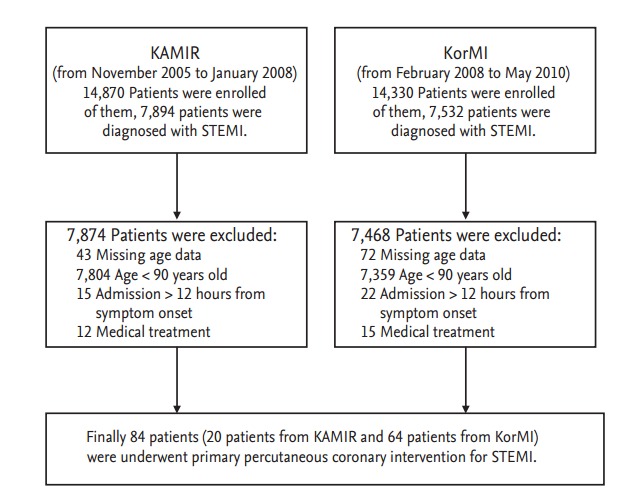
Study flow chart. KAMIR, Korea Acute Myocardial Infarction Registry; KorMI, Korea Working Group on Myocardial Infarction; STEMI, ST-segment elevation myocardial infarction.
Figure 2.

(A) The proportion of different age groups among patients with ST-segment elevation myocardial infarction (STEMI) during the study period. (B) The rate of use of primary percutaneous coronary intervention (PCI) in different age groups during the study period. KAMIR, Korea Acute Myocardial Infarction Registry; KorMI, Korea Working Group on Myocardial Infarction.
Baseline characteristics are presented in Table 1. The mean age was 92.3 ± 3.4 years and 63.1% of patients were women. Hypertension, diabetes mellitus, hyperlipidemia, and current smoking were present in 51.2%, 14.3%, 2.4%, and 8.3% of patients, respectively. Only a few patients suffered from coronary artery disease and 3.6% had received PCI. Comorbidity index score was generally low and 69.0% of patients had no comorbid conditions. On admission, 28.4% patients were in Killip class ≥ 3 and 17.9% patients were in cardiogenic shock. Mean pre-hospital delay time was 232 ± 132 minutes and 84.5% patients arrived at the hospital within 6 hours of symptom onset. Mean left ventricular ejection fraction was 50.8% ± 12.8%. Overall, the baseline characteristics of patients did not change over time.
Table 1.
Baseline characteristics
| Variable | Total (n = 84) | KAMIR (n = 20) | KorMI (n = 64) | p value |
|---|---|---|---|---|
| Age, yr | 92.3 ± 3.4 | 92.8 ± 5.2 | 92.2 ± 2.6 | 0.629 |
| Female sex | 53 (63.1) | 11 (55.0) | 42 (65.6) | 0.818 |
| Body mass index, kg/m2 | 22.2 ± 2.5 | 21.6 ± 2.8 | 22.3 ± 2.4 | 0.374 |
| History of | ||||
| Hypertension | 43 (51.2) | 7 (35.0) | 36 (56.2) | 0.197 |
| Diabetes mellitus | 12 (14.3) | 1 (5.0) | 11 (17.2) | 0.173 |
| Hyperlipidemia | 2 (2.4) | 1 (5.0) | 1 (1.5) | 0.421 |
| Current smoker | 7 (8.3) | 2 (10.0) | 5 (7.8) | 0.539 |
| Percutaneous coronary intervention | 3 (3.6) | 1 (5.0) | 2 (3.1) | 0.563 |
| Coronary artery bypass grafting | 0 | 0 | 0 | 1.000 |
| Myocardial infarction | 0 | 0 | 0 | 1.000 |
| Comorbidity index score | 0.640 | |||
| 0 | 58 (69.0) | 15 (75.0) | 43 (67.2) | |
| 1–2 | 22 (26.2) | 4 (20.0) | 18 (28.1) | |
| ≥ 3 | 4 (4.8) | 1 (5.0) | 3 (4.7) | |
| Killip class at admission | 0.672 | |||
| I | 42 (50.0) | 10 (50.0) | 32 (50.0) | |
| II | 19 (22.6) | 4 (20.0) | 15 (23.4) | |
| III | 8 (9.5) | 3 (15.0) | 5 (7.8) | |
| IV | 15 (17.9) | 3 (15.0) | 12 (18.8) | |
| Prehospital delay, min | 232 ± 132 | 237 ± 135 | 231 ± 132 | 0.858 |
| Prehospital delay < 6 hr | 71 (84.5) | 16 (80.0) | 55 (85.9) | 0.774 |
| Creatinine at admission, mg/dL | 1.23 ± 0.56 | 1.13 ± 0.54 | 1.26 ± 0.57 | 0.366 |
| Left ventricular ejection fraction on admission, % | 50.8 ± 12.8 | 48.0 ± 16.2 | 51.8 ± 11.3 | 0.362 |
| Peak creatinine kinase-MB, ng/mL | 161.7 ± 146.0 | 174.8 ± 166.9 | 159.5 ± 140.9 | 0.831 |
| Peak troponin I, ng/mL | 63.1 ± 75.6 | 70.8 ± 107.5 | 71.1 ± 88.4 | 0.074 |
| High-sensitivity C-reactive protein, mg/dL | 5.4 ± 13.5 | 3.9 ± 4.9 | 5.9 ± 15.3 | 0.434 |
Values are presented as mean ± SD or number (%).
KAMIR, Korea Acute Myocardial Infarction Registry; KorMI, Korea Working Group on Myocardial Infarction.
Angiographic findings and procedural results are presented in Table 2. The mean time from symptom onset to PCI was 311 ± 162 minutes, and was shortened compared to the KAMIR data (377 ± 146 minutes in KAMIR vs. 290 ± 161 minutes in KorMI, p = 0.030). The mean door-to-balloon time was 100 ± 79 minutes, and was also shortened compared to the KAMIR data (140 ± 131 minutes in KAMIR vs. 87 ± 45 minutes in KorMI, p = 0.087). Multi-vessel disease was present in 73.8% of patients. The left anterior descending artery and right coronary artery accounted for the majority of the infarct-related arteries, which were observed in 51.2% and 41.6% of patients, respectively. Coronary stents were implanted in 90.5% of patients, 67.9% of which were drug-eluting stents. A final TIMI grade 3 flow was obtained in 84.5% of patients (75.0% in KAMIR vs. 87.5% in KorMI, p = 0.320). The overall rate of use of glycoprotein IIb/IIIa receptor inhibitors was low; it was administered to only 7.1% of patients.
Table 2.
Angiographic findings and procedural characteristics
| Variable | Total (n = 84) | KAMIR (n = 20) | KorMI (n = 64) | p value |
|---|---|---|---|---|
| Time from symptom onset to PCI, min | 311 ± 162 | 377 ± 146 | 290 ± 161 | 0.030 |
| Door-to-balloon time, min | 100 ± 79 | 140 ± 131 | 87 ± 45 | 0.087 |
| Multi-vessel coronary artery disease | 62 (73.8) | 14 (70.0) | 48 (75.0) | 0.710 |
| Infarct-related coronary artery | 0.554 | |||
| Left anterior descending | 43 (51.2) | 11 (55.0) | 32 (50.0) | |
| Left circumflex | 4 (4.8) | 0 | 4 (6.3) | |
| Right | 35 (41.6) | 8 (40.0) | 27 (42.1) | |
| Left main | 2 (2.4) | 1 (5.0) | 1 (1.6) | |
| TIMI flow, 0 or 1 before procedure | 60 (71.4) | 15 (75.0) | 45 (70.3) | 1.000 |
| Lesion complexity B2/C | 57 (67.9) | 16 (80.0) | 41 (64.1) | 0.854 |
| PCI with stent | 76 (90.5) | 19 (95.0) | 57 (89.1) | 0.371 |
| Drug eluting stent use | 57 (67.9) | 14 (70.0) | 43 (67.2) | 0.932 |
| Total no. of stent | 1.3 ± 0.6 | 1.4 ± 0.5 | 1.3 ± 0.6 | 0.465 |
| TIMI flow after procedure | 0.616 | |||
| 0 | 3 (3.6) | 1 (5.0) | 2 (3.1) | |
| 1 | 2 (2.4) | 1 (5.0) | 1 (1.6) | |
| 2 | 8 (9.5) | 3 (15.0) | 5 (7.8) | |
| 3 | 71 (84.5) | 15 (75.0) | 56 (87.5) | |
| Glycoprotein IIb/IIIa receptor inhibitor | 6 (7.1) | 0 | 6 (9.4) | 0.171 |
| Intra-aortic balloon pumping | 9 (10.7) | 3 (15.0) | 6 (9.4) | 0.364 |
Values are presented as mean ± SD or number (%).
KAMIR, Korea Acute Myocardial Infarction Registry; KorMI, Korea Working Group on Myocardial Infarction; PCI, percutaneous coronary intervention; TIMI, Thrombolysis in Myocardial Infarction.
In-hospital outcomes are presented in Table 3. Cardiogenic shock was present in 25% of patients. Incidences of recurrent myocardial infarction, stroke and acute renal failure were low, and occurred in 1.2%, 1.2%, and 8.3% of patients, respectively. Remarkably, there were no cases of major bleeding during hospitalization.
Table 3.
In-hospital outcomes
| Variable | Total (n = 84) | KAMIR (n = 20) | KorMI (n = 64) | p value |
|---|---|---|---|---|
| Death | 18 (21.4) | 5 (25.0) | 13 (20.3) | 0.919 |
| Cardiac | 15 (17.8) | 4 (20.0) | 11 (17.2) | |
| Non-cardiac | 3 (3.6) | 1 (5.0) | 2 (3.1) | |
| Cardiogenic shock | 21 (25.0) | 4 (20.0) | 17 (26.5) | 0.868 |
| Recurrent myocardial infarction | 1 (1.2) | 1 (5.0) | 0 | 0.238 |
| Stroke | 1 (1.2) | 1 (5.0) | 0 | 0.238 |
| Acute renal failure | 7 (8.3) | 2 (10.0) | 5 (7.8) | 0.762 |
| Major bleeding | 0 | 0 | 0 | 1.000 |
Values are presented as number (%).
KAMIR, Korea Acute Myocardial Infarction Registry; KorMI, Korea Working Group on Myocardial Infarction.
The overall in-hospital mortality rate was 21.4%, which is four times higher than that of STEMI patients who underwent primary PCI within 12 hours of symptom onset (5.04%). The in-hospital mortality rate did not improve significantly during the study period (25.0% in KAMIR vs. 20.0% in KorMI, p = 0.919), and this trend was the same for other age groups (Fig. 3).
Figure 3.
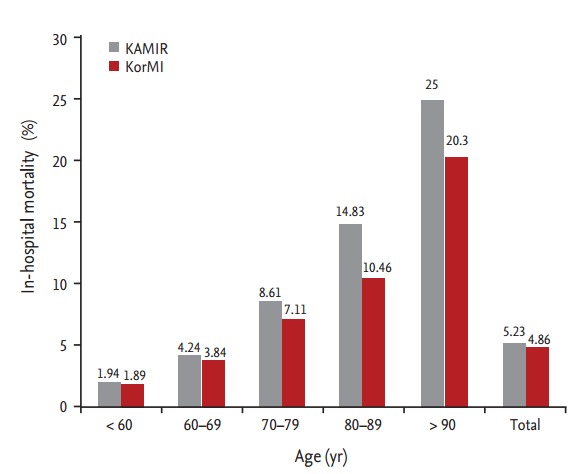
In-hospital mortality rate for different age groups during the study period. KAMIR, Korea Acute Myocardial Infarction Registry; KorMI, Korea Working Group on Myocardial Infarction.
Stepwise logistic regression analysis identified two independent predictors of in-hospital mortality, namely a final TIMI flow grade < 3 (odds ratio [OR], 13.7; 95% confidence interval [CI], 3.2 to 59.0; p < 0.001) and cardiogenic shock during hospitalization (OR, 6.7; 95% CI, 1.5 to 30.3; p = 0.013) (Table 4).
Table 4.
Multivariate analysis of in-hospital mortality
| Variable | Odds ratio | 95% Confidence interval | p value |
|---|---|---|---|
| Final TIMI flow < 3 | 13.7 | 3.2–59.0 | < 0.001 |
| Cardiogenic shock during hospitalization | 6.7 | 1.5–30.3 | 0.013 |
TIMI, Thrombolysis in Myocardial Infarction.
DISCUSSION
Acute myocardial infarction (AMI) is the leading cause of death in elderly patients [6], and age is an important predictor of death after myocardial infarction. Thus, very elderly patients such as nonagenarians represent a high-risk population. Although nonagenarians constitute a small proportion of AMI patients, more nonagenarian STEMI patients may be encountered in daily practice in the near future as the population ages. In our study, the total number of STEMI patients remained unchanged, but the proportion of nonagenarian STEMI patients more than doubled during the study period, and their growth rate increased most rapidly compared to other age groups. This increase contributes to the reason why evidence-based data are necessary to guide proper management in this population.
There is evidence supporting the use of reperfusion therapy in elderly patients up to the age of 85 years [7]. However, in the current guidelines for the treatment of STEMI patients [8,9], there is no age limit for reperfusion therapy, and the recent TRIANA (TRatamiento del Infarto Agudo de miocardio eN Ancianos) trial proposed primary PCI as the optimal reperfusion strategy for old patients [10]. Thus, there is a general acceptance in daily practice for nonagenarian STEMI patients to undergo primary PCI. Several studies have reported the outcomes of primary PCI in nonagenarian STEMI patients [11-14]; these showed that achievement of a TIMI grade 3 flow rate after the procedure ranges from 74.1% to 82%, and in-hospital mortality rate ranges from 18.5% to 34.2%. As a result, the authors concluded that primary PCI can be performed with a high success rate and an acceptable in-hospital mortality rate. Our results also support these previous studies, as achievement of a TIMI grade 3 flow rate after the procedure was 84.5%, while in-hospital mortality was 21.4%.
In the present study, we enrolled nonagenarian STEMI patients who arrived at the hospital within 12 hours of symptom onset. The overall rate of use of primary PCI in these patients was 75.7%, and this rate eventually reached the average of other age groups (from 62.5% in KAMIR to 81.0% in KorMI). A previous single-center study in nonagenarian STEMI patients reported a primary PCI rate of use of 54% and an associated in-hospital mortality rate of 23% [15]. Considering results from the GRACE registry, in which 30% of STEMI patients who presented within 12 hours of symptom onset did not receive reperfusion therapy [16], the primary PCI rate of use was considered high in our study. This result is due to the fact that the included patients were relatively healthy nonagenarians and many patients presented with a short pre-hospital delay. Thus, the responsible physicians may have attempted to perform primary PCI actively. Contrary to the previous study in which PCI use rate increased over time and resulted in reduced in-hospital mortality rate after STEMI in nonagenarians [17], our study did not result in a reduction in mortality despite the increased primary PCI use rate over time. This could be due to three reasons. The first is the different inclusion criteria used for patient selection. Secondly, as mentioned earlier, primary PCI use rate was sufficiently high in our study to determine an acceptable in-hospital mortality rate. Lastly, the use rate of glycoprotein IIb/IIIa receptor inhibitors, which have favorable effects on mortality in this population, was low [11].
In our study, a final TIMI grade < 3 and cardiogenic shock were identified as independent predictors of in-hospital mortality. Final TIMI flow grade is an important determinant of in-hospital and long-term adverse events following primary PCI, but elderly patients are less likely to achieve a final TIMI grade of 3 after PCI [18]. Although high bleeding risk and complex coronary anatomy are common in elderly patients, judicious use of glycoprotein IIb/IIIa receptor inhibitors and thrombosuction devices can represent meaningful approaches to improve myocardial perfusion in elderly STEMI patients. Cardiogenic shock was present in 17.9% of patients at the time of admission and eventually developed in 7.1% of patients after admission, for a total of 25% of patients. Similar to other studies [11,19,20], our in-hospital mortality rate was very high in patients with cardiogenic shock (42.9%), indicating that the presence of cardiogenic shock in nonagenarian STEMI patients requires more careful consideration when determining treatment strategy. In one notable study [19], the in-hospital mortality rate was 90% in patients with cardiogenic shock, and the authors concluded that primary PCI is unable to affect the poor prognosis of very old patients with cardiogenic shock.
We are aware of several limitations in the present study. This is a retrospective multicenter analysis and is subject to the inherent limitations of such studies. Although two registries were combined, the number of enrolled patients was small, as nonagenarian STEMI patients account for only 0.9% of total STEMI patients. Therefore, it can be assumed that many nonagenarian STEMI patients were not referred to primary PCI. The total mortality rate was too small to perform multivariate analysis, which should be taken into account when interpreting our results. Lastly, we were unable to assess long-term mortality rate and quality of life.
KEY MESSAGE
1. There has been a rapid increase in nonagenarian ST-segment elevation myocardial infarction (STEMI) patients; the rate of use of primary percutaneous coronary intervention (PCI) in these patients has also increased.
2. Primary PCI for nonagenarian STEMI patients can be performed safely with an acceptable in-hospital mortality rate.
3. To improve outcomes, future research is necessary to determine which patients would benefit from primary PCI through proper risk stratification.
Acknowledgments
The Korea Acute Myocardial Infarction Registry (KAMIR) Study Group of the Korean Circulation Society was as follows: Myung Ho Jeong, MD, Young Keun Ahn, MD, Shung Chull Chae, MD, Jong Hyun Kim, MD, Seung Ho Hur, MD, Young Jo Kim, MD, In Whan Seong, MD, Dong Hoon Choi, MD, Jei Keon Chae, MD, Taek Jong Hong, MD, Jae Young Rhew, MD, Doo Il Kim, MD, In Ho Chae, MD, Jung Han Yoon, MD, Bon Kwon Koo, MD, Byung Ok Kim, MD, Myoung Yong Lee, MD, Kee Sik Kim, MD, Jin Yong Hwang, MD, Myeong Chan Cho, MD, Seok Kyu Oh, MD, Nae Hee Lee, MD, Kyoung Tae Jeong, MD, Seung Jea Tahk, MD, Jang Ho Bae, MD, Seung-Woon Rha, MD, Keum Soo Park, MD, Chong Jin Kim, MD, Kyoo Rok Han, MD, Tae Hoon Ahn, MD, Moo Hyun Kim, MD, Ki Bae Seung, MD, Wook Sung Chung, MD, Ju Young Yang, MD, Chong Yun Rhim, MD, Hyeon Cheol Gwon, MD, Seong Wook Park, MD, Young Youp Koh, MD, Seung Jae Joo, MD, Soo Joong Kim, MD, Dong Kyu Jin, MD, Jin Man Cho, MD, Yang Soo Jang, MD, Jeong Gwan Cho, MD, and Seung Jung Park, MD. This work was supported by a grant from the National Research Foundation of Korea Grant funded by the Korean Government (MEST), Republic of Korea (2010-0020261), and the Korea Healthcare Technology R&D Project, Ministry for Health, Welfare and Family Affairs, and Korea National Institute of Health, Republic of Korea (A084869).
Footnotes
No potential conflict of interest relevant to this article was reported.
REFERENCES
- 1.White HD, Barbash GI, Califf RM, et al. Age and outcome with contemporary thrombolytic therapy: results from the GUSTO-I trial. Global Utilization of Streptokinase and TPA for Occluded coronary arteries trial. Circulation. 1996;94:1826–1833. doi: 10.1161/01.cir.94.8.1826. [DOI] [PubMed] [Google Scholar]
- 2.Showkathali R, Boston-Griffiths E, Parker M, et al. Should primary percutaneous coronary intervention be the routine reperfusion strategy in octogenarians presenting with ST elevation myocardial infarction? J Cardiovasc Med (Hagerstown) 2014;15:53–59. doi: 10.2459/JCM.0b013e3283649978. [DOI] [PubMed] [Google Scholar]
- 3.Lee PY, Alexander KP, Hammill BG, Pasquali SK, Peterson ED. Representation of elderly persons and women in published randomized trials of acute coronary syndromes. JAMA. 2001;286:708–713. doi: 10.1001/jama.286.6.708. [DOI] [PubMed] [Google Scholar]
- 4.Korea Acute Myocardial Infarction Registry (KAMIR) Investigators. Lee KH, Jeong MH, et al. Gender differences of success rate of percutaneous coronary intervention and short term cardiac events in Korea Acute Myocardial Infarction Registry. Int J Cardiol. 2008;130:227–234. doi: 10.1016/j.ijcard.2007.08.044. [DOI] [PubMed] [Google Scholar]
- 5.Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47:1245–1251. doi: 10.1016/0895-4356(94)90129-5. [DOI] [PubMed] [Google Scholar]
- 6.Hovanesyan A, Rich MW. Outcomes of acute myocardial infarction in nonagenarians. Am J Cardiol. 2008;101:1379–1383. doi: 10.1016/j.amjcard.2008.01.012. [DOI] [PubMed] [Google Scholar]
- 7.Alexander KP, Newby LK, Armstrong PW, et al. Acute coronary care in the elderly, part II: ST-segment-elevation myocardial infarction: a scientific statement for health-care professionals from the American Heart Association Council on Clinical Cardiology: in collaboration with the Society of Geriatric Cardiology. Circulation. 2007;115:2570–2589. doi: 10.1161/CIRCULATIONAHA.107.182616. [DOI] [PubMed] [Google Scholar]
- 8.Smith SC, Jr, Feldman TE, Hirshfeld JW, Jr, et al. ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/SCAI Writing Committee to Update 2001 Guidelines for Percutaneous Coronary Intervention) Circulation. 2006;113: doi: 10.1161/CIRCULATIONAHA.106.173220. [DOI] [PubMed] [Google Scholar]
- 9.King SB, 3rd, Smith SC, Jr, Hirshfeld JW, Jr, et al. 2007 Focused update of the ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association task force on practice guidelines: 2007 writing group to review new evidence and update the ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention, writing on behalf of the 2005 Writing Committee. Circulation. 2008;117:261–295. doi: 10.1161/CIRCULATIONAHA.107.188208. [DOI] [PubMed] [Google Scholar]
- 10.Bueno H, Betriu A, Heras M, et al. Primary angioplasty vs. fibrinolysis in very old patients with acute myocardial infarction: TRIANA (TRatamiento del Infarto Agudo de miocardio eN Ancianos) randomized trial and pooled analysis with previous studies. Eur Heart J. 2011;32:51–60. doi: 10.1093/eurheartj/ehq375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Danzi GB, Centola M, Pomidossi GA, et al. Usefulness of primary angioplasty in nonagenarians with acute myocardial infarction. Am J Cardiol. 2010;106:770–773. doi: 10.1016/j.amjcard.2010.04.041. [DOI] [PubMed] [Google Scholar]
- 12.Koutouzis M, Grip L, Matejka G, Albertsson P. Primary percutaneous coronary interventions in nonagenarians. Clin Cardiol. 2010;33:157–161. doi: 10.1002/clc.20720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Salinas P, Galeote G, Martin-Reyes R, et al. Primary percutaneous coronary intervention for ST-segment elevation acute myocardial infarction in nonagenarian patients: results from a Spanish multicentre registry. EuroIntervention. 2011;6:1080–1084. doi: 10.4244/EIJV6I9A188. [DOI] [PubMed] [Google Scholar]
- 14.Rigattieri S, Cera M, Sciahbasi A, et al. Primary percutaneous coronary intervention in nonagenarians: six-month outcomes from a single-center registry. J Invasive Cardiol. 2013;25:242–245. [PubMed] [Google Scholar]
- 15.Ionescu CN, Amuchastegui M, Ionescu S, Marcu CB, Donohue T. Treatment and outcomes of nonagenarians with ST-elevation myocardial infarction. J Invasive Cardiol. 2010;22:474–478. [PubMed] [Google Scholar]
- 16.Eagle KA, Goodman SG, Avezum A, et al. Practice variation and missed opportunities for reperfusion in ST-segment-elevation myocardial infarction: findings from the Global Registry of Acute Coronary Events (GRACE) Lancet. 2002;359:373–377. doi: 10.1016/S0140-6736(02)07595-5. [DOI] [PubMed] [Google Scholar]
- 17.Mandawat A, Mandawat A, Mandawat MK. Percutaneous coronary intervention after ST-segment elevation myocardial infarction in nonagenarians: use rates and in-hospital mortality. J Am Coll Cardiol. 2013;61:1207–1208. doi: 10.1016/j.jacc.2012.12.019. [DOI] [PubMed] [Google Scholar]
- 18.Dziewierz A, Siudak Z, Rakowski T, Dubiel JS, Dudek D. Age-related differences in treatment strategies and clinical outcomes in unselected cohort of patients with ST-segment elevation myocardial infarction transferred for primary angioplasty. J Thromb Thrombolysis. 2012;34:214–221. doi: 10.1007/s11239-012-0713-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Valente S, Lazzeri C, Salvadori C, et al. Effectiveness and safety of routine primary angioplasty in patients aged > or =85 years with acute myocardial infarction. Circ J. 2008;72:67–70. doi: 10.1253/circj.72.67. [DOI] [PubMed] [Google Scholar]
- 20.Shah P, Najafi AH, Panza JA, Cooper HA. Outcomes and quality of life in patients>or=85 years of age with ST-elevation myocardial infarction. Am J Cardiol. 2009;103:170–174. doi: 10.1016/j.amjcard.2008.08.051. [DOI] [PubMed] [Google Scholar]