

Abstract
Background
Web-based computer-tailored interventions have shown to be effective in improving health behavior; however, high dropout attrition is a major issue in these interventions.
Objective
The aim of this study is to assess whether people with a lower educational level drop out from studies more frequently compared to people with a higher educational level and to what extent this depends on evaluation of these interventions.
Methods
Data from 7 randomized controlled trials of Web-based computer-tailored interventions were used to investigate dropout rates among participants with different educational levels. To be able to compare higher and lower educated participants, intervention evaluation was assessed by pooling data from these studies. Logistic regression analysis was used to assess whether intervention evaluation predicted dropout at follow-up measurements.
Results
In 3 studies, we found a higher study dropout attrition rate among participants with a lower educational level, whereas in 2 studies we found that middle educated participants had a higher dropout attrition rate compared to highly educated participants. In 4 studies, no such significant difference was found. Three of 7 studies showed that participants with a lower or middle educational level evaluated the interventions significantly better than highly educated participants (“Alcohol-Everything within the Limit”: F 2,376=5.97, P=.003; “My Healthy Behavior”: F 2,359=5.52, P=.004; “Master Your Breath”: F 2,317=3.17, P=.04). One study found lower intervention evaluation by lower educated participants compared to participants with a middle educational level (“Weight in Balance”: F 2,37=3.17, P=.05). Low evaluation of the interventions was not a significant predictor of dropout at a later follow-up measurement in any of the studies.
Conclusions
Dropout attrition rates were higher among participants with a lower or middle educational level compared with highly educated participants. Although lower educated participants evaluated the interventions better in approximately half of the studies, evaluation did not predict dropout attrition. Further research is needed to find other explanations for high dropout rates among lower educated participants.
Keywords: dropout, attrition, educational level, computer tailoring, Web-based intervention, eHealth, evaluation, meta-analysis
Introduction
Previous studies have demonstrated that Web-based computer-tailored interventions can be effective in motivating individuals to adopt different health behaviors [1-3], such as increasing physical activity [4-10], improving healthy nutrition [11-14], smoking cessation [15-18], and reducing alcohol intake [19-21], and they have been successfully applied to multiple health behaviors [22,23]. In addition, these interventions have been found to be more cost-effective than usual care or nontailored information [24-27].
According to Eysenbach [28], dropout, either not completing the study or missing follow-up measurements, is a “fundamental characteristic” of Internet interventions and a problematic issue. The loss of participants to follow-up, dropout attrition, makes analyses and statements of the effectiveness of these interventions more complicated and less valid [28] because most outcome measures are assessed during follow-up and dropout from the intervention seems to be related to dropout attrition [29]. Therefore, it is important to find out why participants do not complete Web-based studies to ultimately understand and reduce this problem.
Acquiring follow-up measurements from at-risk groups, such as people with a lower educational level, is important because unhealthy lifestyle behaviors are most common among people with a lower educational level [30-32]. Lower educated people are known to eat less fruits and vegetables [33,34], are less physically active [30,35], consume alcohol more often in unhealthy quantities [36], use more tobacco [37-39], and have a higher likelihood of being obese [40] compared to highly educated people. It is not only important to reach this group with Web-based computer-tailored interventions, but also to prevent lower educated participants from dropping out of the follow-up measurements to be able to collect information about the effectiveness of the intervention [29].
Christensen and Mackinnon [41] already raised the issue of insufficient research regarding study dropout in 2006. Since then, findings about dropout among participants with different educational levels are still rarely reported and show ambiguous results. Although some studies revealed that people with a lower educational level have higher dropout rates in Web-based computer-tailored interventions than highly educated people [42-46], other studies did not find educational differences in terms of dropout [46-49]. To the best of our knowledge, no study indicates a significantly higher dropout among highly educated participants, but there remains a need to obtain more insight into dropout among people with different educational levels to be able to reduce dropout.
The reason for dropout among lower educated people is discussed rarely in the literature. Possible reasons for dropout can be intervention characteristics (eg, workload, content), personal characteristics such as educational level, or it can be related to participants’ perceptions of the interventions, such as a lack of perceived benefit, which may result in dissatisfaction [50]. Dissatisfaction with the intervention can be reflected in the evaluation of the intervention. It has been shown that participants who do evaluate the intervention as less positive are more likely to drop out [51] and, therefore, might not be interested in attending follow-up measurements. In other words, evaluation might be a predictor of dropout attrition in Web-based computer-tailored interventions, but little thought has been given to this aspect, which makes it difficult to draw valid conclusions [52].
Therefore, the aim of this study is first to examine if the dropout attrition rates in our 7 randomized controlled trials (RCTs) of Web-based computer-tailored interventions were higher for people with a lower educational level than people with a middle or high educational level. Second, we assessed whether people with different educational levels evaluated these interventions differently. Finally, we analyzed whether participations’ evaluation of the interventions predicted dropout at subsequent follow-up measurements.
Methods
Studies
To examine differences in dropout attrition and evaluation between participants with different educational levels, we used a convenience sample of participants from 7 Web-based computer-tailored intervention studies that were conducted in the past years (2010-2014) at the Department of Health Promotion of Maastricht University in the Netherlands.
The studies were RCTs to evaluate interventions that used computer-tailored techniques to improve diverse health behaviors. The study “Master Your Breath” (MYB) focused on increasing physical activity and smoking cessation among chronic obstructive pulmonary disease (COPD) patients and people at risk for COPD. The 3 studies “Stay Quit for You” (SQ4U), “Support to Quit” (STQ), and “Personal Advice in Stopping smoking” (PAS) focused on smoking cessation. “Weight in Balance” (WIB) aimed to prevent obesity by targeting physical activity and energy intake. The study “My Healthy Behavior” (MHB) targeted the following health behaviors: physical activity, fruit and vegetable consumption, alcohol intake, and smoking. The study “Alcohol-Everything within the Limits” (AEL) focused on moderate alcohol intake and is the only study that was not carried out in the Netherlands but in Germany.
All selected studies made use of the I-Change model [53,54], which postulates that the behavior change process has at least 3 phases: awareness, motivation, and action. The first factor is determined by factors such as behavioral awareness, knowledge, and risk perceptions. The second phase is determined by attitudes, social influence beliefs, and self-efficacy expectations, and results in a certain intention to perform a particular behavior. The third factor is determined by self-efficacy, action planning, skills, and barriers. The tailored feedback messages of the studies included in this paper have a strong focus on inter alia these determinants. A detailed description of these RCTs and the related publications can be found in Table 1.
Table 1.
Summary of the Web-based computer-tailored interventions.
| Study | Reference | Participants | Study groups | Intervention | Follow-up |
| AEL | Design and effects: [20] | German general population aged 18-69 years | Two intervention groups that differed in the computer-tailored feedback strategies (alternating vs summative) compared to 1 control group that received no computer-tailored feedback. | A 3-session, Web-based computer-tailored intervention aiming to reduce alcohol intake in high-risk adult drinkers. | T1=3 months; T2=6 months |
| MHB | Study protocol: [55]; effects: [20,26] | Dutch general population aged 19-65 years | Two experimental groups (ie, a sequential behavior tailoring condition and a simultaneous behavior tailoring condition) and 1 control group that that received only a tailored health risk appraisal but no motivational computer-tailored feedback. | Five lifestyle behaviors of smoking, alcohol intake, fruit consumption, vegetable consumption, and physical activity addressing computer-tailored feedback at several times. | T1=12 months; T2=24 months |
| MYB | Study protocol: [56]; effects: [57] | People with or at risk for COPD in the Netherlands | One intervention group received Web-based computer-tailored self-management intervention; the control group received usual care. | Web-based, computer-tailored self-management intervention with the aim to increase physical activity and support smoking cessation. | T1=6 months |
| PAS | Study protocol: [58]; effects: [18,25,59] | Adult Dutch smokers with intention to stop smoking within 6 months | Intervention group with computer-tailored information to quit smoking compared to control group that received no computer-tailored feedback. | A Web-based computer-tailored smoking cessation intervention. | T1=6 weeks; T2=6 months; T3=12 months |
| STQ | Study protocol: [60]; effects: [61,62] | Dutch smokers who were motivated to stop smoking and aged ≥18 years | Intervention groups 2 (video/text) × (low/middle/high socioeconomic status). Respondents were assigned to 1 of the intervention groups (text- vs video-tailored feedback) or to the control group (nontailored generic advice). | Comparing Web-based text and a Web-based video-driven computer-tailored approach for low and high SES smokers, this incorporates multiple computer-tailored feedback moments with the aim to support smoking cessation. | T1=6 months; T2=12 months |
| SQ4U | Study protocol: [63]; effects: [15] | Dutch daily smokers aged 18-65 years who were motivated to stop smoking | Two intervention groups (Action Plan, Action Plan+), 1 control group that received no computer-tailored feedback. | Two computer-tailored interventions to prevent smoking relapse. Provides tailored feedback in the Action Plan+ group after stop smoking attempts, in the Action Plan group after T0 measurement. | T1=6 months; T2=12 months |
| WIB | Study protocol: [64]; effects: [65] | Normal and overweight adults from the Netherlands | Two intervention groups (video and text) and 1 waiting list control group. | Computer-tailored feedback via text or video to prevent weight gain or support modest weight loss by targeting physical activity and energy intake. | T1=6 months |
Measurement
In all 7 studies, educational level was assessed by asking participants about their highest completed level of education. In-line with national guidelines, educational level was categorized into 3 groups: lower (1=no education, primary or lower vocational school), middle (2=secondary vocational school or high school), and higher (3=higher professional education or university) educational level [66].
All studies included a process evaluation assessment to evaluate the intervention among participants within the intervention group. Participants were asked to evaluate the tailored feedback and the intervention. The process evaluation assessments of the 7 studies included had one item in common that asked participants to grade the intervention that they participated in: “Please evaluate the intervention with a school grade from 1 to 10” (10=highest grade, 1=lowest grade according to the Dutch school grading system; AEL: 15=highest grade, 1=lowest grade, which is in-line with the German school grading system).
To assess dropout attrition, participants who completed the baseline measurement but did not complete the follow-up measurement were characterized as dropouts (1=dropout; 0=completed follow-up). We assessed dropout attrition within differently educated participants for each follow-up measurement separately. Furthermore, we used the last available evaluation moment as predictor of dropout for the following measurement. Table 1 gives an overview of the specific follow-up moments per study.
Statistical Analysis
All analyses were performed with SPSS 20.0 (IBM Corp, Armonk, NY, USA). Descriptive statistics were used to describe sample characteristics. Per study, a logistic regression analysis was conducted to examine if dropout rates differed for each educational level. To control for multiple testing, the Benjamini and Hochberg linear step-up method was used for each study [67,68]. With the use of an Excel template, the adjusted significance levels were calculated [69].
Differences between the educational levels with regard to evaluation of the Web-based computer-tailored interventions were analyzed by means of ANOVAs and Tukey honestly significant difference (HSD) tests. Control groups were excluded from analysis with regard to evaluation of the intervention because they could not evaluate it.
To be able to give a more general picture of whether lower and higher educated participants from the intervention groups evaluated Web-based computer-tailored interventions differently, the Exploratory Software for Confidence Intervals (ESCI) Excel template [70] was used for pooling the data by means of a meta-analysis (Table 1). The meta-analysis used a random effect model and gave an impression of the overall differences for intervention evaluation between lower and higher educated participants (ie, by subtracting the evaluation of the most different groups, the lower educated participants from the higher educated participants). In one study (MHB), the evaluation item was assessed at multiple follow-up measurements; in this case, we included only the last follow-up measurement [71].
Finally, logistic regression analyses were conducted to examine if dropout was predicted by evaluation in 4 of the 7 interventions among participants with different educational levels. We excluded the studies WIB, PAS, and MYB from this analysis because their evaluation assessment took place during the last follow-up measurement; therefore, it was not possible to assess evaluation as a predictor of dropout in these studies. To identify possible interaction effects, an interaction term of educational level and evaluation was used in the regression model. If this interaction term was significant, then analyses were conducted separately per educational level. Analyses were corrected for age and gender. A P value of .05 was used as the significance level for all analysis.
Results
Participants
Table 2 shows the educational level, mean age, and gender distribution of the participants within the 7 selected studies at baseline.
Table 2.
Baseline sample characteristics of the participants in the Web-based computer-tailored interventions.
| Study | N | Educational level, n (%)a | Age (years), mean (SD) | Gender (male), n (%) | ||
|
|
|
Low | Middle | High |
|
|
| AEL | 1149 | 483 (44.8) | 256 (23.8) | 338 (31.4) | 43.82 (15.51) | 550 (47.9) |
| MHB | 5055 | 515 (10.4) | 2334 (47.1) | 2112 (42.6) | 44.15 (12.67) | 2661 (52.6) |
| MYB | 1307 | 386 (29.5) | 427 (32.7) | 494 (37.8) | 57.64 (7.22) | 627 (47.9) |
| PAS | 1123 | 238 (21.2) | 513 (45.7) | 372 (33.1) | 49.47 (32.55) | 535 (47.6) |
| STQ | 2099 | 707 (33.6) | 782 (37.3) | 612 (29.2) | 45.33 (13.21) | 821 (39.1) |
| SQ4U | 2031 | 207 (10.2) | 1130 (55.6) | 694 (34.2) | 40.88 (11.80) | 766 (37.7) |
| WIB | 1419 | 214 (15.1) | 436 (30.7) | 769 (54.2) | 48.13 (11.52) | 588 (41.4) |
Dropout
Table 3 shows the results of the dropout analyses with regard to the educational level for each study, each follow-up measurement including the dropout rates, and study group in detail with high education as the reference group.
Table 3.
Results of a logistic regression examine dropout attrition among different educational groups.
| Study, follow-up, and group | Dropout, n (%) | Educational levela | |||||
|
|
|
Low | Middle | ||||
|
|
|
OR (95% CI) | P | OR (95% CI) | P | ||
| AEL |
|
|
|
|
|
||
|
|
T1 | 398 (34.6) |
|
|
|
|
|
|
|
|
Sequential |
|
0.61 (0.10-3.59) | .58 | 1.03 (0.15-7.18) | .97 |
|
|
|
Simultaneously |
|
1.65 (0.61-4.58) | .32 | —c | .99 |
|
|
|
Control |
|
—c | .99 | —c | .99 |
|
|
T2 | 436 (37.9) |
|
|
|
|
|
|
|
|
Sequential |
|
1.16 (0.24-5.52) | .89 | 1.90 (0.18-19.37) | .58 |
|
|
|
Simultaneously |
|
1.15 (0.34-3.84) | .81 | 1.23 (0.21-7.13) | .81 |
|
|
|
Control |
|
0.90 (0.11-7.06) | .92 | 0.51 (0.37-7.09) | .61 |
| MHB |
|
|
|
|
|
||
|
|
T1 | 3317 (65.6) |
|
|
|
|
|
|
|
|
Sequential |
|
1.52 (1.14-2.01) | .004b | 1.05 (0.83-1.32) | .68 |
|
|
|
Simultaneously |
|
1.57 (1.18-2.08) | .002b | 1.39 (1.09-1.78) | .007b |
|
|
|
Control |
|
1.32 (1.00-1.73) | .04 | 1.27 (1.00-1.61) | .04 |
|
|
T2 | 3602 (71.3) |
|
|
|
|
|
|
|
|
Sequential |
|
1.43 (1.06-1.94) | .01b | 0.95 (0.74-1.23) | .73 |
|
|
|
Simultaneously |
|
1.51 (1.12-2.04) | .006b | 1.50 (1.16-1.94) | .002b |
|
|
|
Control |
|
1.23 (0.93-1.62) | .14 | 0.97 (0.76-1.23) | .81 |
| MYB |
|
|
|
|
|
||
|
|
T1 | 254 (19.4) |
|
|
|
|
|
|
|
|
Intervention |
|
1.33 (0.84-2.12) | .21 | 1.40 (0.89-2.20) | .13 |
|
|
|
Control |
|
1.14 (0.67-1.95) | .61 | 1.17 (0.70-1.96) | .53 |
| PAS |
|
|
|
|
|
||
|
|
T1 | 674 (60.0) |
|
|
|
|
|
|
|
|
Control |
|
0.93 (0.58-1.49) | .77 | 0.88 (0.59-1.31) | .55 |
|
|
|
Tailoring only |
|
2.02 (1.23-3.33) | .005 | 1.37 (0.93-2.01) | .10 |
|
|
T2 | 831 (74.0) |
|
|
|
|
|
|
|
|
Control |
|
0.93 (0.54-1.56) | .77 | 0.89 (0.57-1.39) | .61 |
|
|
|
Tailoring only |
|
2.04 (1.15-3.60) | .01 | 1.41 (0.93-2.15) | .10 |
|
|
T3 | 967 (86.1) |
|
|
|
|
|
|
|
|
Control |
|
1.42 (0.71-2.86) | .32 | 0.89 (0.52-1.52) | .67 |
|
|
|
Tailoring only |
|
1.41 (0.67-2.97) | .35 | 1.03 (0.60-1.78) | .90 |
| STQ |
|
|
|
|
|
||
|
|
T1 | 1306 (62.2) |
|
|
|
|
|
|
|
|
Video |
|
1.90 (1.24-2.90) | .003b | 1.39 (0.93-2.09) | 10 |
|
|
|
Text |
|
1.29 (0.87-1.91) | .19 | 1.22 (0.83-1.78) | .29 |
|
|
|
Control |
|
0.98 (0.67-1.47) | .98 | 0.71 (0.49-1.05) | .09 |
|
|
T2 | 1437 (68.5) |
|
|
|
|
|
|
|
|
Video |
|
1.95 (1.26-3.02) | .003b | 1.39 (0.92-2.09) | .11 |
|
|
|
Text |
|
2.31 (1.52-3.51) | .<001b | 1.29 (0.88-1.89) | .18 |
|
|
|
Control |
|
1.36 (0.90-2.04) | .13 | 1.24 (0.84-1.84) | .66 |
| SQ4U |
|
|
|
|
|
||
|
|
T1 | 1251 (61.9) |
|
|
|
|
|
|
|
|
Action Plan |
|
1.26 (0.75-2.12) | .36 | 1.03 (0.74-1.44) | .83 |
|
|
|
Action Plan + |
|
1.71 (0.92-3.18) | .08 | 1.14 (0.81-1.60) | .44 |
|
|
|
Control |
|
1.73 (0.91-3.27) | .09 | 0.90 (0.63-1.28) | .57 |
|
|
T2 | 1465 (72.1) |
|
|
|
|
|
|
|
|
Action Plan |
|
2.33 (1.24-4.35) | .01 | 1.30 (0.91-1.86) | .14 |
|
|
|
Action Plan + |
|
2.25 (1-11-4.52) | .02 | 1.55 (1.07-2.24) | .01 |
|
|
|
Control |
|
2.00 (1.02-3.92) | .04 | 1.35 (0.94-1.94) | .09 |
| WIB |
|
|
|
|
|
||
|
|
T1 | 404 (28.5) |
|
|
|
|
|
|
|
|
Video |
|
1.50 (0.87-2.59) | .15 | 1.23 (0.81-2.01) | .29 |
|
|
|
Text |
|
2.29 (1.33-3.95) | .003b | 1.12 (0.74-1.69) | .60 |
|
|
|
Control |
|
1.57 (0.81-3.04) | .18 | 2.01 (1.22-3.32) | .006b |
a All analysis are corrected for age and gender. High education is the reference group.
b Significant P values after correction for multiple comparisons according to Benjamini-Hochberg.
c Odds ratios are not reported due to low cell count.
After correction for multiple testing, significantly higher dropout rates were found within 3 studies (MHB, STQ, WIB) among lower educated participants compared to higher educated ones. Furthermore, in these 3 studies, dropout attrition was also significantly higher among middle educated participants in comparison with higher educated participants. In 4 of 7 studies (AEL, MYB, PAS, SQ4U), no difference in dropout with regard to educational level was found.
Evaluation
Table 4 presents differences between the educational groups with regard to evaluation of the Web-based computer-tailored interventions in detail. In 3 of 7 studies (AEL, MHB, MYB), lower educated participants evaluated the intervention significantly higher compared to their counterparts. In one study (WIB), lower educated participants evaluated the intervention less positively compared to middle educated participants.
Table 4.
Evaluation of the 7 Web-based computer-tailored interventions by different educational levels.
| Study and groupa | Level of education, mean (SD) | F (df1,df2) | P | Tukey HSD, P | ||||||
|
|
Low | Middle | High |
|
|
L-Mb | L-H | M-H | ||
| AEL |
|
|
|
|
|
|
|
|
||
|
|
T0 |
|
|
|
|
|
|
|
|
|
|
|
|
Sequential | 11.20 (3.48) | 11.12 (3.00) | 10.72 (3.62) | 0.71 (2,340) | .56 | .97 | .47 | .70 |
|
|
|
Simultaneously | 11.75 (3.37) | 11.49 (2.85) | 10.40 (3.61) | 5.97 (2,376) | .003 | .82 | .002 | .05 |
|
|
T2 |
|
|
|
|
|
|
|
|
|
|
|
|
Sequential | 11.32 (4.27) | 11.27 (3.69) | 10.39 (4.33) | 0.58 (2,229) | .56 | .77 | .89 | .53 |
|
|
|
Simultaneously | 11.09 (4.28) | 11.53 (3.30) | 10.81 (3.89) | 1.26 (2,246) | .56 | .99 | .29 | .48 |
| MHB |
|
|
|
|
|
|
|
|
||
|
|
T1 |
|
|
|
|
|
|
|
|
|
|
|
|
Sequential | 7.43 (1.08) | 7.14 (1.79) | 7.03 (1.13) | 2.12 (2,201) | .12 | .98 | .48 | .11 |
|
|
|
Simultaneously | 7.80 (0.91) | 6.94 (1.70) | 6.56 (2.41) | 1.30 (2,178) | .27 | .60 | .27 | .62 |
|
|
T2 |
|
|
|
|
|
|
|
|
|
|
|
|
Sequential | 7.78 (1.27) | 7.59 (0.94) | 7.53 (0.91) | 1.04 (2,367) | .35 | .64 | .37 | .71 |
|
|
|
Simultaneously | 7.94 (0.89) | 7.68 (0.92) | 7.43 (1.02) | 5.52 (2,359) | .004 | .30 | .01 | .05 |
| MYB |
|
|
|
|
|
|
|
|
||
|
|
T1 |
|
|
|
|
|
|
|
|
|
|
|
|
Intervention | 7.07 (1.50) | 6.93 (1.23) | 6.60 (1.77) | 3.17 (2,317) | .04 | .77 | .05 | .17 |
| PAS |
|
|
|
|
|
|
|
|
||
|
|
T3 |
|
|
|
|
|
|
|
|
|
|
|
|
Tailoring only | 6.09 (1.70) | 6.72 (1.25) | 7.03 (1.20) | 2.42 (2,81) | .09 | .92 | .96 | .63 |
| STQ |
|
|
|
|
|
|
|
|
||
|
|
T2 |
|
|
|
|
|
|
|
|
|
|
|
|
Video | 6.48 (1.97) | 6.18 (2.17) | 6.28 (1.64) | 0.38 (2,193) | .69 | .67 | .83 | .95 |
|
|
|
Text | 6.53 (1.84) | 6.51 (1.23) | 5.96 (1.72) | 3.29 (2,234) | .04 | .99 | .08 | .07 |
| SQ4U |
|
|
|
|
|
|
|
|
||
|
|
T1 |
|
|
|
|
|
|
|
|
|
|
|
|
Action Plan | 6.56 (1.74) | 6.63 (1.41) | 6.20 (1.60) | 1.29 (2,134) | .28 | .98 | .79 | .25 |
|
|
|
Action Plan+ | 6.27 (2.10) | 6.49 (1.69) | 6.51 (1.27) | 0.10 (2,108) | .90 | .97 | .85 | .99 |
| WIB |
|
|
|
|
|
|
|
|
||
|
|
T1 |
|
|
|
|
|
|
|
|
|
|
|
|
Video | 6.99 (1.23) | 7.56 (0.78) | 7.36 (1.08) | 3.17 (2,37) | .05 | .05 | .27 | .21 |
|
|
|
Text | 6.79 (0.92) | 7.32 (0.82) | 7.11 (1.24) | 0.66 (2,51) | .52 | .49 | .67 | .88 |
a T specifies the time of the evaluation measurement.
b Level of education: L=low, M=middle, H=high.
Furthermore, the meta-analysis of the 7 studies comparing evaluation of lower and higher educated participants indicated that participants with a lower educational level evaluated the interventions significantly more positively compared to highly educated participants (OR 0.28, 95% CI –0.54 to 0.04, P<.001) (see Figure 1). Nevertheless, the meta-analysis revealed presence of a moderate level of heterogeneity (I 2=66.10%) [74,75], which indicates variation across the studies.
Figure 1.
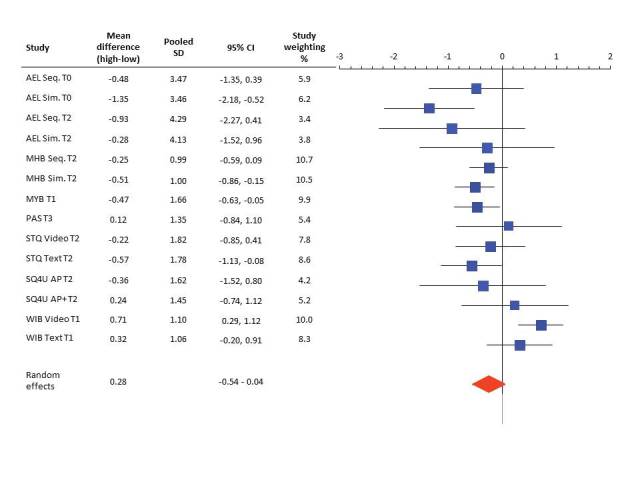
Forest plot of mean differences by random effect model of evaluation of Web-based computer-tailored interventions between highly and lower educated participants. Random effects represent the combined effect.
Association of Education and Evaluation with Dropout Attrition
For the 4 studies that evaluated the intervention before the follow-up measurements, a significant interaction between education and evaluation regarding dropout at follow-up was not found (Table 5). Only within the MHB study was a positive association found between the intervention evaluation and educational level. Participants with a middle educational level were more likely to dropout than participants with a higher educational level.
Table 5.
Association of education and evaluation with dropout attrition at follow-up.
| Study and variablesa | β | P | OR (95% CI) | χ2 7 | R 2 | |
| AEL T1 |
|
|
|
9.0 | .054 | |
|
|
Education low | –1.02 | .35 | 0.35 (0.04-3.14) |
|
|
|
|
Education middle | –0.08 | .96 | 0.92 (0.02-37.18) |
|
|
|
|
Evaluation T0 | 0.03 | .69 | 1.03 (0.88-1.19) |
|
|
|
|
Education × evaluation |
|
.48 |
|
|
|
| MHB T1 |
|
|
|
96.9 | .053 | |
|
|
Education low | 1.90 | .05 | 6.71 (0.97-46.43) |
|
|
|
|
Education middle | 0.93 | .07 | 2.55 (0.89-7.27) |
|
|
|
|
Evaluation T0 | –0.01 | .84 | 0.99 (0.90-1.08) |
|
|
|
|
Education × evaluation |
|
.18 |
|
|
|
| STQ T2 |
|
|
|
16.6 | .033 | |
|
|
Education low | 0.62 | .29 | 1.86 (0.57-6.00) |
|
|
|
|
Education middle | 0.28 | .64 | 1.32 (0.40-4.35) |
|
|
|
|
Evaluation T1 | –0.49 | .52 | 0.95 (0.81-1.10) |
|
|
|
|
Education × evaluation |
|
.99 |
|
|
|
| SQ4U T2 |
|
|
|
5.6 | .051 | |
|
|
Education low | 4.33 | .11 | 76.36 (0.34-16.713.27) |
|
|
|
|
Education middle | 1.32 | .55 | 3.75 (0.46-303.55) |
|
|
|
|
Evaluation T1 | 0.11 | .69 | 1.11 (0.64-1.92) |
|
|
|
|
Education × evaluation |
|
.40 |
|
|
|
a T indicates follow-up; high education is reference group. All analyses are corrected for age and gender.
Discussion
Dropout Attrition
The first aim of this study was to evaluate whether participants with a lower educational level have higher dropout attrition from Web-based computer-tailored studies than participants with a medium or high educational level. In 3 of these studies, lower and middle educated participants dropped out more frequently compared to higher educated participants.
A possible explanation for the higher dropout rates may be that lower educated participants tend to use written health information more often [76] and spend less time online seeking health information [77,78]. It could be possible that they lose interest in the intervention sooner, which causes them to drop out of the study.
Also, the fact that lower educated people have an unhealthier lifestyle [30-32] might play a role in dropout. Due to tailoring, participants with an unhealthier lifestyle in multiple health behavior interventions received more recommendations to change their health behavior(s) and this has been found to decrease participants’ motivation to change [79]. It might be possible that lower educated participants started the intervention with the aim to change their health behavior, but that receiving information about extensive required changes decreased their self-efficacy to be able to change [80] and could subsequently have decreased their motivation to participate. Another explanation could be that lower educated participants might have been less likely to change their behavior and, thus, may have perceived the recommendations as less feasible, which caused them to drop out of the study [28,81,82]. This could have caused not only usage and nonusage attrition, but also dropout attrition because these 2 kinds of attrition seem to be related [46].
Moreover, lower educated people might be less familiar with Web-based computer-tailored interventions [83,84] and that might result in lower confidence in the effectiveness of those interventions (ie, lower perceived efficacy) and, in turn, could cause an increase in dropout [85,86]. Although these are reasons for nonusage attrition (not using the intervention), it seems convincing that this correlates with dropout attrition because participants who did not evaluate the intervention positively might have little interest in completing follow-up measurements [51].
All participants were asked to complete long questionnaires and received tailored feedback, which must be cognitively processed and requires intensive cognitive performance. Lower educated adults have been shown to have a lower level of health literacy [84,87,88]. They have more difficulties processing new information and this could cause ego depletion [89,90]. Ego depletion may, in turn, reduce the willingness to participate any longer within the study.
Some studies found that dropout attrition could be increased by sending reminders and prompts [78,91-93]. Further research is necessary to evaluate if this is also effective for people with different educational levels.
Evaluation
Against our initial expectation that lower educated participants might evaluate the interventions less positively, we found that lower educated participants evaluated the intervention in 3 of 7 studies more positively compared to their higher educated counterparts. This might be explained by the finding that highly educated people make more use of the Internet as health information resource, whereas these interventions might be newer and more interesting for lower educated people. A review supported this assumption because it shows that people with a high educational level may make more intensive use of several sources (eg, people form their social network, mass media, health professionals) to gain health-related information compared to lower educated people and they might read the received information more superficially [94]. This might result in less elaboration of the messages and a lower evaluation regarding the novelty of the messages. Due to the use of several resources, highly educated participants also rely less on online information and have lower levels of trust in them, which may negatively influence their evaluation of the intervention [95].
Evaluation was not a significant predictor of dropout at follow-up in any of our studies. This suggests that other factors must be important in explaining why participants did not return to the study for follow-up questionnaires. Dropout analysis performed within these studies has shown that a lower educational level, unhealthy lifestyle, low intention to change the behavior, and low self-efficacy were predictors of dropout [20,96,97].
Limitations and Strengths
First, the only item all studies had in common concerning the evaluation of the interventions was an overall grade participants assigned to the intervention. Although we can assume that this item gives an overall impression of participants’ evaluation, it might be that participants with different educational levels liked and disliked different aspects of the intervention (eg, layout, provided information, or personal relevance), which was not reflected in this overall grade. However, the evaluation of these different aspects was not equally assessed in all 7 studies. Furthermore, it is possible that participants who did not like the intervention dropped out before completing the evaluation item. In this study, we included only those participants that completed the evaluation item and assessed follow-up at the subsequent measurement.
Second, all interventions were based on the I-Change model and targeted the same social cognitive determinants to change behavior, which allows for comparing the 7 studies. However, a generalization of the results for other interventions must be done with caution because some interventions also used other theories, such as self-regulation theories, as a framework for the educational content.
Although the restricted number of studies is a limitation, including other Web-based tailored interventions might have resulted in even higher program heterogeneity and would have made comparisons even more difficult and results (partly) dependent on program characteristics. Also Wienert and Kuhlmann [98] have determined that tailored interventions are difficult to compare, whereas the interventions included in this study were comparable because they all were based on the same theoretical background (the I-Change model), all 7 studies provided tailored feedback on social cognitive determinants from this model and provided feedback, and all 7 studies included the same program evaluation item. The comparison of interventions using other tailoring techniques than the interventions described in this study is difficult and access to the original data at the individual level would be necessary for further research and adequate analysis [99].
One of the strengths of this study is the access to 7 datasets (at participant level), which allowed us to conduct the analysis with the original data. Second, all studies used at least one identical item to assess the study evaluation which enables us to compare these studies. Finally, all studies had a large number of participants ranging from 1149 to 5055, which makes our results meaningful.
Conclusion
This study showed that for 3 of 7 studies on computer-tailored interventions, participants with a lower educational level dropped out more often from follow-up measurements and tended to evaluate the interventions better compared to participants with a middle and higher educational level. However, the evaluation of the intervention did not predict participation or nonparticipation at follow-up. Based on our results, it is hard to say what other factors may play a role in dropout attrition from Web-based computer-tailored interventions. Further studies might evaluate different aspects of the intervention, besides only the participants’ grades, to find more relevant aspects of intervention evaluation.
Future studies should take high dropout among lower educated participants into consideration when developing strategies to decrease high dropout from Web-based computer-tailored interventions.
Acknowledgments
We would like to thank all doctoral advisors who supported the development of the mentioned Web-based computer-tailored interventions: Catherine Bolman, Stef Kremers, Lilian Lechner, Anke Oenema, Liesbeth van Osch, Jean Muris, and Trudy van der Weijden.
Abbreviations
- AEL
Alcohol-Everything within the Limit
- COPD
chronic obstructive pulmonary disease
- HSD
honestly significant difference
- MHB
My Healthy Behavior
- MYB
Master Your Breath
- PAS
Personal Advice in Stopping smoking
- RCT
randomized controlled trial
- SQ4U
Stay Quit for You
- STQ
Support to Quit
- WIB
Weight in Balance
Footnotes
Authors' Contributions: All authors contributed to this paper. DR conducted the analyses and drafted the paper. HdV and RC contributed to the design of the paper. All authors contributed to the interpretation of the data and to the writing of the paper. All authors revised the manuscript critically for important intellectual content and read and approved the final manuscript.
Conflicts of Interest: HdV is the scientific director of Vision2Health, a company that licenses evidence-based innovative computer-tailored health communication tools. The other authors declare that they have no competing interests.
References
- 1.Noar SM, Harrington NG, editors. eHealth Applications: Promising Strategies for Behavior Change (Routledge Communication Series) New York: Routledge; 2012. [Google Scholar]
- 2.Noar S, Grant Harrington N, Van Stee SK, Shemanski Aldrich R. Tailored health communication to change lifestyle behaviors. American Journal of Lifestyle Medicine. 2010 Nov 19;5(2):112–122. doi: 10.1177/1559827610387255. [DOI] [Google Scholar]
- 3.Wantland D, Portillo C, Holzemer W, Slaughter R, McGhee E. The effectiveness of Web-based vs. non-Web-based interventions: a meta-analysis of behavioral change outcomes. J Med Internet Res. 2004 Nov 10;6(4):e40. doi: 10.2196/jmir.6.4.e40. http://www.jmir.org/2004/4/e40/ v6e40 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ammann R, Vandelanotte C, de Vries H, Mummery W. Can a website-delivered computer-tailored physical activity intervention be acceptable, usable, and effective for older people? Health Educ Behav. 2013 Apr;40(2):160–70. doi: 10.1177/1090198112461791.1090198112461791 [DOI] [PubMed] [Google Scholar]
- 5.van 't Riet J, Ruiter RA, Werrij M, de Vries H. Investigating message-framing effects in the context of a tailored intervention promoting physical activity. Health Educ Res. 2010 Apr;25(2):343–54. doi: 10.1093/her/cyp061. http://her.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=19841041 .cyp061 [DOI] [PubMed] [Google Scholar]
- 6.Zuercher A. A look at the latest AIDS projections for the United States. Health Aff (Millwood) 1990;9(2):163–70. doi: 10.1377/hlthaff.9.2.163. http://content.healthaffairs.org/cgi/pmidlookup?view=long&pmid=2163963 . [DOI] [PubMed] [Google Scholar]
- 7.Norman G, Zabinski M, Adams M, Rosenberg D, Yaroch A, Atienza A. A review of eHealth interventions for physical activity and dietary behavior change. Am J Prev Med. 2007 Oct;33(4):336–345. doi: 10.1016/j.amepre.2007.05.007. http://europepmc.org/abstract/MED/17888860 .S0749-3797(07)00363-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Compernolle S, Vandelanotte C, Cardon G, De Bourdeaudhuij I, De Cocker K. Effectiveness of a web-based, computer-tailored, pedometer-based physical activity intervention for adults: a cluster randomized controlled trial. J Med Internet Res. 2015;17(2):e38. doi: 10.2196/jmir.3402. http://www.jmir.org/2015/2/e38/ v17i2e38 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Peels D, van Stralen MM, Bolman C, Golsteijn RH, de Vries H, Mudde A, Lechner L. The differentiated effectiveness of a printed versus a Web-based tailored physical activity intervention among adults aged over 50. Health Educ Res. 2014 Oct;29(5):870–82. doi: 10.1093/her/cyu039. http://her.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=24980023 .cyu039 [DOI] [PubMed] [Google Scholar]
- 10.Konstantinidis E, Billis A, Mouzakidis C, Zilidou V, Antoniou P, Bamidis P. Design, implementation and wide pilot deployment of FitForAll: an easy to use exergaming platform improving physical fitness and life quality of senior citizens. IEEE J. Biomed. Health Inform. 2014 Dec 09;PP(99):1–1. doi: 10.1109/JBHI.2014.2378814. http://ieeexplore.ieee.org/xpl/articleDetails.jsp?reload=true&arnumber=6980053 . [DOI] [PubMed] [Google Scholar]
- 11.Brug J, Campbell M, van Assema P. The application and impact of computer-generated personalized nutrition education: a review of the literature. Patient Educ Couns. 1999 Feb;36(2):145–56. doi: 10.1016/s0738-3991(98)00131-1.S0738-3991(98)00131-1 [DOI] [PubMed] [Google Scholar]
- 12.Krebs P, Prochaska J, Rossi J. A meta-analysis of computer-tailored interventions for health behavior change. Prev Med. 2010;51(3-4):214–21. doi: 10.1016/j.ypmed.2010.06.004. http://europepmc.org/abstract/MED/20558196 .S0091-7435(10)00231-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hamel L, Robbins L. Computer- and web-based interventions to promote healthy eating among children and adolescents: a systematic review. J Adv Nurs. 2013 Jan;69(1):16–30. doi: 10.1111/j.1365-2648.2012.06086.x. [DOI] [PubMed] [Google Scholar]
- 14.Broekhuizen K, Kroeze W, van Poppel MN, Oenema A, Brug J. A systematic review of randomized controlled trials on the effectiveness of computer-tailored physical activity and dietary behavior promotion programs: an update. Ann Behav Med. 2012 Oct;44(2):259–86. doi: 10.1007/s12160-012-9384-3. http://europepmc.org/abstract/MED/22767052 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Elfeddali I, Bolman C, Candel Math JJ, Wiers R, de Vries H. Preventing smoking relapse via Web-based computer-tailored feedback: a randomized controlled trial. J Med Internet Res. 2012;14(4):e109. doi: 10.2196/jmir.2057. http://www.jmir.org/2012/4/e109/ v14i4e109 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Smit E, de Vries H, Hoving C. Effectiveness of a Web-based multiple tailored smoking cessation program: a randomized controlled trial among Dutch adult smokers. J Med Internet Res. 2012;14(3):e82. doi: 10.2196/jmir.1812. http://www.jmir.org/2012/3/e82/ v14i3e82 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.McClure J, Shortreed S, Bogart A, Derry H, Riggs K, St John J, Nair V, An L. The effect of program design on engagement with an internet-based smoking intervention: randomized factorial trial. J Med Internet Res. 2013;15(3):e69. doi: 10.2196/jmir.2508. http://www.jmir.org/2013/3/e69/ v15i3e69 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Smit E, de Vries H, Hoving C. Effectiveness of a Web-based multiple tailored smoking cessation program: a randomized controlled trial among Dutch adult smokers. J Med Internet Res. 2012;14(3):e82. doi: 10.2196/jmir.1812. http://www.jmir.org/2012/3/e82/ v14i3e82 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.van der Wulp NY, Hoving C, Eijmael K, Candel Math JJ, van Dalen W, De Vries H. Reducing alcohol use during pregnancy via health counseling by midwives and internet-based computer-tailored feedback: a cluster randomized trial. J Med Internet Res. 2014;16(12):e274. doi: 10.2196/jmir.3493. http://www.jmir.org/2014/12/e274/ v16i12e274 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Schulz D, Candel M, Kremers S, Reinwand D, Jander A, de Vries H. Effects of a Web-based tailored intervention to reduce alcohol consumption in adults: randomized controlled trial. J Med Internet Res. 2013;15(9):e206. doi: 10.2196/jmir.2568. http://www.jmir.org/2013/9/e206/ v15i9e206 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Boon B, Risselada A, Huiberts A, Riper H, Smit F. Curbing alcohol use in male adults through computer generated personalized advice: randomized controlled trial. J Med Internet Res. 2011;13(2):e43. doi: 10.2196/jmir.1695. http://www.jmir.org/2011/2/e43/ v13i2e43 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.van Keulen HM, Mesters I, Ausems M, van Breukelen G, Campbell M, Resnicow K, Brug J, de Vries H. Tailored print communication and telephone motivational interviewing are equally successful in improving multiple lifestyle behaviors in a randomized controlled trial. Ann Behav Med. 2011 Feb;41(1):104–18. doi: 10.1007/s12160-010-9231-3. http://europepmc.org/abstract/MED/20878293 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Smeets T, Kremers SP, Brug J, de Vries H. Effects of tailored feedback on multiple health behaviors. Ann Behav Med. 2007 Apr;33(2):117–23. doi: 10.1080/08836610701307801. [DOI] [PubMed] [Google Scholar]
- 24.van Keulen HM, Bosmans J, van Tulder MW, Severens J, de Vries H, Brug J, Mesters I. Cost-effectiveness of tailored print communication, telephone motivational interviewing, and a combination of the two: results of an economic evaluation alongside the Vitalum randomized controlled trial. Int J Behav Nutr Phys Act. 2010;7:64. doi: 10.1186/1479-5868-7-64. http://www.ijbnpa.org/content/7//64 .1479-5868-7-64 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Smit E, Evers SM, de Vries H, Hoving C. Cost-effectiveness and cost-utility of Internet-based computer tailoring for smoking cessation. J Med Internet Res. 2013;15(3):e57. doi: 10.2196/jmir.2059. http://www.jmir.org/2013/3/e57/ v15i3e57 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Schulz D, Smit E, Stanczyk N, Kremers SP, de Vries VH, Evers SM. Economic evaluation of a web-based tailored lifestyle intervention for adults: findings regarding cost-effectiveness and cost-utility from a randomized controlled trial. J Med Internet Res. 2014;16(3):e91. doi: 10.2196/jmir.3159. http://www.jmir.org/2014/3/e91/ v16i3e91 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Stanczyk N, Bolman C, Smit E, Candel MJ, Muris JW, de Vries H. How to encourage smokers to participate in web-based computer-tailored smoking cessation programs: a comparison of different recruitment strategies. Health Educ Res. 2014 Feb;29(1):23–40. doi: 10.1093/her/cyt104. http://her.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=24287402 .cyt104 [DOI] [PubMed] [Google Scholar]
- 28.Eysenbach G. The law of attrition. J Med Internet Res. 2005;7(1):e11. doi: 10.2196/jmir.7.1.e11. http://www.jmir.org/2005/1/e11/ v7e11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Cunningham A. Intervention adherence is related to participant retention: implications for research. J Med Internet Res. 2014;16(5):e133. doi: 10.2196/jmir.2948. http://www.jmir.org/2014/5/e133/ v16i5e133 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Vlismas K, Stavrinos V, Panagiotakos D. Socio-economic status, dietary habits and health-related outcomes in various parts of the world: a review. Cent Eur J Public Health. 2009 Jun;17(2):55–63. doi: 10.21101/cejph.a3475. [DOI] [PubMed] [Google Scholar]
- 31.Margolis R. Educational differences in healthy behavior changes and adherence among middle-aged Americans. J Health Soc Behav. 2013;54(3):353–68. doi: 10.1177/0022146513489312. http://europepmc.org/abstract/MED/23988727 .0022146513489312 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Cowell A. The relationship between education and health behavior: some empirical evidence. Health Econ. 2006 Feb;15(2):125–46. doi: 10.1002/hec.1019. [DOI] [PubMed] [Google Scholar]
- 33.De Irala-Estévez J, Groth M, Johansson L, Oltersdorf U, Prättälä R, Martínez-González MA. A systematic review of socio-economic differences in food habits in Europe: consumption of fruit and vegetables. Eur J Clin Nutr. 2000 Sep;54(9):706–14. doi: 10.1038/sj.ejcn.1601080. [DOI] [PubMed] [Google Scholar]
- 34.Hulshof KF, Brussaard J, Kruizinga A, Telman J, Löwik MR. Socio-economic status, dietary intake and 10 y trends: the Dutch National Food Consumption Survey. Eur J Clin Nutr. 2003 Jan;57(1):128–37. doi: 10.1038/sj.ejcn.1601503.1601503 [DOI] [PubMed] [Google Scholar]
- 35.Gidlow C, Johnston L, Crone D, Ellis N, James D. A systematic review of the relationship between socio-economic position and physical activity. Health Education Journal. 2006 Dec 01;65(4):338–367. doi: 10.1177/0017896906069378. [DOI] [Google Scholar]
- 36.Groot W, Maassen van den Brink M. What does education do to our health?. Measuring the Effects of Education on Health and Civic Engagement: Proceedings of the Copenhagen Symposium; Copenhagen Symposium on measuring the effects of education on health and civic engagement; Mar 2006; Copenhagen. 2006. pp. 355–364. http://www.oecd.org/edu/innovation-education/37437718.pdf . [Google Scholar]
- 37.Hiscock R, Bauld L, Amos A, Fidler J, Munafò M. Socioeconomic status and smoking: a review. Ann N Y Acad Sci. 2012 Feb;1248:107–23. doi: 10.1111/j.1749-6632.2011.06202.x. [DOI] [PubMed] [Google Scholar]
- 38.Savage C. Alcohol and tobacco related health inequity: a population health perspective. J Addict Nurs. 2012 Feb;23(1):72–4. doi: 10.3109/10884602.2011.648739. [DOI] [PubMed] [Google Scholar]
- 39.Grittner U, Kuntsche S, Gmel G, Bloomfield K. Alcohol consumption and social inequality at the individual and country levels--results from an international study. Eur J Public Health. 2013 Apr;23(2):332–9. doi: 10.1093/eurpub/cks044. http://eurpub.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=22562712 .cks044 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Cutler D, Lleras-Muney A. Understanding differences in health behaviors by education. J Health Econ. 2010 Jan;29(1):1–28. doi: 10.1016/j.jhealeco.2009.10.003. http://europepmc.org/abstract/MED/19963292 .S0167-6296(09)00114-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Christensen H, Mackinnon A. The law of attrition revisited. J Med Internet Res. 2006;8(3):e20; author reply e21. doi: 10.2196/jmir.8.3.e20. http://www.jmir.org/2006/3/e20/ v8i3e20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Strecher V, McClure J, Alexander G, Chakraborty B, Nair V, Konkel J, Greene S, Couper M, Carlier C, Wiese C, Little R, Pomerleau C, Pomerleau O. The role of engagement in a tailored web-based smoking cessation program: randomized controlled trial. J Med Internet Res. 2008;10(5):e36. doi: 10.2196/jmir.1002. http://www.jmir.org/2008/5/e36/ v10i5e36 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Geraghty AW, Torres L, Leykin Y, Pérez-Stable EJ, Muñoz RF. Understanding attrition from international Internet health interventions: a step towards global eHealth. Health Promot Int. 2013 Sep;28(3):442–52. doi: 10.1093/heapro/das029. http://heapro.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=22786673 .das029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Rogers E. Diffusion of Innovations. New York: Free Press; 2003. [Google Scholar]
- 45.Price M, Gros D, McCauley J, Gros K, Ruggiero K. Nonuse and dropout attrition for a web-based mental health intervention delivered in a post-disaster context. Psychiatry. 2012;75(3):267–84. doi: 10.1521/psyc.2012.75.3.267. http://europepmc.org/abstract/MED/22913502 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Murray E, White I, Varagunam M, Godfrey C, Khadjesari Z, McCambridge J. Attrition revisited: adherence and retention in a web-based alcohol trial. J Med Internet Res. 2013;15(8):e162. doi: 10.2196/jmir.2336. http://www.jmir.org/2013/8/e162/ v15i8e162 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Peels D, Bolman C, Golsteijn RH, de Vries H, Mudde A, van Stralen MM, Lechner Lilian. Differences in reach and attrition between Web-based and print-delivered tailored interventions among adults over 50 years of age: clustered randomized trial. J Med Internet Res. 2012;14(6):e179. doi: 10.2196/jmir.2229. http://www.jmir.org/2012/6/e179/ v14i6e179 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Ezendam Nicole P M. Brug Johannes, Burg Johannes, Borsboom Gerard, van Empelen Pepijn, Oenema Anke. Differential effects of the computer-tailored FATaintPHAT programme on dietary behaviours according to sociodemographic, cognitive and home environmental factors. Public Health Nutr. 2014 Feb;17(2):431–9. doi: 10.1017/S1368980012005344.S1368980012005344 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Habibović M, Cuijpers P, Alings M, van der Voort P, Theuns D, Bouwels L, Herrman J, Valk S, Pedersen S. Attrition and adherence in a WEB-Based Distress Management Program for Implantable Cardioverter defibrillator Patients (WEBCARE): randomized controlled trial. J Med Internet Res. 2014;16(2):e52. doi: 10.2196/jmir.2809. http://www.jmir.org/2014/2/e52/ v16i2e52 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Kelders S, Kok R, Ossebaard H, Van Gemert-Pijnen JE. Persuasive system design does matter: a systematic review of adherence to web-based interventions. J Med Internet Res. 2012;14(6):e152. doi: 10.2196/jmir.2104. http://www.jmir.org/2012/6/e152/ v14i6e152 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Postel G, de Haan HA, ter Huurne ED, van der Palen J, Becker S, de Jong CA. Attrition in web-based treatment for problem drinkers. J Med Internet Res. 2011;13(4):e117. doi: 10.2196/jmir.1811. http://www.jmir.org/2011/4/e117/ v13i4e117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Skelton J, Irby M, Geiger A. A systematic review of satisfaction and pediatric obesity treatment: new avenues for addressing attrition. J Healthc Qual. 2014;36(4):5–22. doi: 10.1111/jhq.12003. http://europepmc.org/abstract/MED/23414547 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.van der Wulp NY, Hoving C, de Vries H. A qualitative investigation of alcohol use advice during pregnancy: experiences of Dutch midwives, pregnant women and their partners. Midwifery. 2013 Nov;29(11):e89–98. doi: 10.1016/j.midw.2012.11.014.S0266-6138(12)00221-5 [DOI] [PubMed] [Google Scholar]
- 54.de Vries H, Mudde A, Leijs I, Charlton A, Vartiainen E, Buijs G, Clemente MP, Storm H, González NA, Nebot M, Prins T, Kremers S. The European Smoking Prevention Framework Approach (EFSA): an example of integral prevention. Health Educ Res. 2003 Oct;18(5):611–26. doi: 10.1093/her/cyg031. http://her.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=14572020 . [DOI] [PubMed] [Google Scholar]
- 55.Schulz D, Kremers S, van Osch LA, Schneider F, van Adrichem MJ, de Vries H. Testing a Dutch web-based tailored lifestyle programme among adults: a study protocol. BMC Public Health. 2011;11:108. doi: 10.1186/1471-2458-11-108. http://www.biomedcentral.com/1471-2458/11/108 .1471-2458-11-108 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Voncken-Brewster V, Tange H, de Vries H, Nagykaldi Z, Winkens B, van der Weijden T. A randomised controlled trial testing a web-based, computer-tailored self-management intervention for people with or at risk for chronic obstructive pulmonary disease: a study protocol. BMC Public Health. 2013;13:557. doi: 10.1186/1471-2458-13-557. http://www.biomedcentral.com/1471-2458/13/557 .1471-2458-13-557 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Voncken-Brewster V, Tange H, de Vries H, Nagykaldi Z, Winkens B, van der Weijden T. A randomized controlled trial evaluating the effectiveness of a web-based, computer-tailored self-management intervention for people with or at risk for COPD. Int J Chron Obstruct Pulmon Dis. 2015;10:1061–73. doi: 10.2147/COPD.S81295. doi: 10.2147/COPD.S81295.copd-10-1061 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Smit E, de Vries H, Hoving C. The PAS study: a randomized controlled trial evaluating the effectiveness of a web-based multiple tailored smoking cessation programme and tailored counselling by practice nurses. Contemp Clin Trials. 2010 May;31(3):251–8. doi: 10.1016/j.cct.2010.03.001.S1551-7144(10)00031-5 [DOI] [PubMed] [Google Scholar]
- 59.Smit E, de Vries H, Hoving C. The PAS study: a randomized controlled trial evaluating the effectiveness of a web-based multiple tailored smoking cessation programme and tailored counselling by practice nurses. Contemp Clin Trials. 2010 May;31(3):251–8. doi: 10.1016/j.cct.2010.03.001.S1551-7144(10)00031-5 [DOI] [PubMed] [Google Scholar]
- 60.Stanczyk N, Bolman C, Michel JL Walthouwer. de Vries H. Study protocol of a Dutch smoking cessation e-health program. BMC Public Health. 2011;11:847. doi: 10.1186/1471-2458-11-847. http://www.biomedcentral.com/1471-2458/11/847 .1471-2458-11-847 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Stanczyk N, Smit E, Schulz DN, de Vries H, Bolman C, Muris JW, Evers SM. An economic evaluation of a video- and text-based computer-tailored intervention for smoking cessation: a cost-effectiveness and cost-utility analysis of a randomized controlled trial. PLoS One. 2014;9(10):e110117. doi: 10.1371/journal.pone.0110117. http://dx.plos.org/10.1371/journal.pone.0110117 .PONE-D-13-48690 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Stanczyk N, Bolman C, van Adrichem M, Candel M, Muris J, de Vries H. Comparison of text and video computer-tailored interventions for smoking cessation: randomized controlled trial. J Med Internet Res. 2014;16(3):e69. doi: 10.2196/jmir.3016. http://www.jmir.org/2014/3/e69/ v16i3e69 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Elfeddali I, Bolman C, de Vries H. SQ4U - a computer tailored smoking relapse prevention program incorporating planning strategy assignments and multiple feedback time points after the quit-attempt: development and design protocol. Contemp Clin Trials. 2012 Jan;33(1):151–8. doi: 10.1016/j.cct.2011.09.008.S1551-7144(11)00244-8 [DOI] [PubMed] [Google Scholar]
- 64.Walthouwer MJ, Oenema A, Soetens K, Lechner L, de Vries H. Systematic development of a text-driven and a video-driven web-based computer-tailored obesity prevention intervention. BMC Public Health. 2013;13:978. doi: 10.1186/1471-2458-13-978. http://www.biomedcentral.com/1471-2458/13/978 .1471-2458-13-978 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Walthouwer MJ, Oenema A, Soetens K, Lechner L, de Vries H. Are clusters of dietary patterns and cluster membership stable over time? Results of a longitudinal cluster analysis study. Appetite. 2014 Nov;82:154–9. doi: 10.1016/j.appet.2014.07.025.S0195-6663(14)00382-1 [DOI] [PubMed] [Google Scholar]
- 66.Luijkx R, de Heus M. The International Standard Classification of Education. Mannheim: Mannheimer Zentrum für Europäische Sozialforschung (MZES); 2008. The educational system of the Netherlands; pp. 47–75. [Google Scholar]
- 67.Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. Journal of the Royal Statistical Society Series B (Methodological) 1995;57:289–300. doi: 10.2307/2346101. [DOI] [Google Scholar]
- 68.Yekutieli D, Benjamini Y. The dontrol of the false discovery rate in multiple testing under dependency. The Annals of Statistics. 2001 Aug;29(4):1165–1188. doi: 10.1214/aos/1013699998. [DOI] [Google Scholar]
- 69.Weinkauf M. marum. [2015-10-03]. Software and programs https://marum.de/Software_and_Programs.html .
- 70.Cumming G. Understanding the New Statistics: Effect Sizes, Confidence Intervals, and Meta-Analysis (Multivariate Applications Series) New York: Routledge Academic; 2012. [Google Scholar]
- 71.Borenstein M, Hedges LV, Rothstein H. Introduction to Meta-Analysis. Oxford: Wiley; 2009. [Google Scholar]
- 72.Statistisches Bundesamt. 2013. [2015-10-03]. Bildungsstand https://www.destatis.de/DE/ZahlenFakten/GesellschaftStaat/BildungForschungKultur/Bildungsstand/Tabellen/Bildungsabschluss.html;jsessionid=7E781B5507CB5855D3AF5C8D883FB9B3.cae3 .
- 73.Bierings H. Centraal Bureau voor de Statistiek. 2013. Oct 03, [2015-10-03]. Onderwijsniveau bevolking gestegen http://www.cbs.nl/nl-NL/menu/themas/onderwijs/publicaties/artikelen/archief/2013/2013-3905-wm.htm .
- 74.Huedo-Medina T, Sánchez-Meca J, Marín-Martínez F, Botella J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol Methods. 2006 Jun;11(2):193–206. doi: 10.1037/1082-989X.11.2.193.2006-07641-005 [DOI] [PubMed] [Google Scholar]
- 75.Higgins JP, Thompson S. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002 Jun 15;21(11):1539–58. doi: 10.1002/sim.1186. [DOI] [PubMed] [Google Scholar]
- 76.Cutrona SL, Mazor KM, Vieux SN, Luger TM, Volkman JE, Finney Rutten LJ. Health information-seeking on behalf of others: characteristics of "surrogate seekers". J Cancer Educ. 2015 Mar;30(1):12–9. doi: 10.1007/s13187-014-0701-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Jensen J, King A, Davis L, Guntzviller L. Utilization of internet technology by low-income adults: the role of health literacy, health numeracy, and computer assistance. J Aging Health. 2010 Sep;22(6):804–26. doi: 10.1177/0898264310366161.0898264310366161 [DOI] [PubMed] [Google Scholar]
- 78.Wangberg S, Andreassen H, Prokosch H, Santana SM, Sørensen T, Chronaki C. Relations between Internet use, socio-economic status (SES), social support and subjective health. Health Promot Int. 2008 Mar;23(1):70–7. doi: 10.1093/heapro/dam039. http://heapro.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=18083686 .dam039 [DOI] [PubMed] [Google Scholar]
- 79.Wilson K, Senay I, Durantini M, Sánchez F, Hennessy M, Spring B, Albarracín D. When it comes to lifestyle recommendations, more is sometimes less: a meta-analysis of theoretical assumptions underlying the effectiveness of interventions promoting multiple behavior domain change. Psychol Bull. 2015 Mar;141(2):474–509. doi: 10.1037/a0038295.2014-56564-001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Crutzen R, Ruiter R. Interest in behavior change interventions: a conceptual model. Eur Health Psychol. 2015;17:6–11. http://www.crutzen.net/interest.pdf . [Google Scholar]
- 81.Postel M, de Haan HA, ter Huurne ED, Becker E, de Jong CA. Effectiveness of a web-based intervention for problem drinkers and reasons for dropout: randomized controlled trial. J Med Internet Res. 2010;12(4):e68. doi: 10.2196/jmir.1642. http://www.jmir.org/2010/4/e68/ v12i4e68 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Christensen H, Griffiths K, Farrer L. Adherence in internet interventions for anxiety and depression. J Med Internet Res. 2009;11(2):e13. doi: 10.2196/jmir.1194. http://www.jmir.org/2009/2/e13/ v11i2e13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Kraft P, Yardley L. Current issues and new directions in Psychology and Health: What is the future of digital interventions for health behaviour change? Psychol Health. 2009 Jul;24(6):615–8. doi: 10.1080/08870440903068581.912857109 [DOI] [PubMed] [Google Scholar]
- 84.Neter E, Brainin E. eHealth literacy: extending the digital divide to the realm of health information. J Med Internet Res. 2012;14(1):e19. doi: 10.2196/jmir.1619. http://www.jmir.org/2012/1/e19/ v14i1e19 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.McKay H, Danaher B, Seeley J, Lichtenstein E, Gau J. Comparing two web-based smoking cessation programs: randomized controlled trial. J Med Internet Res. 2008;10(5):e40. doi: 10.2196/jmir.993. http://www.jmir.org/2008/5/e40/ v10i5e40 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Geraghty AW, Wood A, Hyland M. Attrition from self-directed interventions: investigating the relationship between psychological predictors, intervention content and dropout from a body dissatisfaction intervention. Soc Sci Med. 2010 Jul;71(1):30–7. doi: 10.1016/j.socscimed.2010.03.007.S0277-9536(10)00232-7 [DOI] [PubMed] [Google Scholar]
- 87.Kickbusch I. Health literacy: addressing the health and education divide. Health Promot Int. 2001 Sep;16(3):289–97. doi: 10.1093/heapro/16.3.289. http://heapro.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=11509466 . [DOI] [PubMed] [Google Scholar]
- 88.Paasche-Orlow M, Parker R, Gazmararian J, Nielsen-Bohlman L, Rudd R. The prevalence of limited health literacy. J Gen Intern Med. 2005 Feb;20(2):175–84. doi: 10.1111/j.1525-1497.2005.40245.x. http://europepmc.org/abstract/MED/15836552 .JGI40245 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Baumeister R, Heatherton T, Tice D. Losing Control: How and Why People Fail at Self-Regulation. San Diego: Academic Press; 1994. [Google Scholar]
- 90.Baumeister R, Muraven M, Tice D. Ego eepletion: a resource model of volition, self-regulation, and controlled processing. Social Cognition. 2000 Jun;18(2):130–150. doi: 10.1521/soco.2000.18.2.130. [DOI] [Google Scholar]
- 91.Murray E, White I, Varagunam M, Godfrey C, Khadjesari Z, McCambridge J. Attrition revisited: adherence and retention in a web-based alcohol trial. J Med Internet Res. 2013;15(8):e162. doi: 10.2196/jmir.2336. http://www.jmir.org/2013/8/e162/ v15i8e162 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.De Leon E, Fuentes L, Cohen J. Characterizing periodic messaging interventions across health behaviors and media: systematic review. J Med Internet Res. 2014;16(3):e93. doi: 10.2196/jmir.2837. http://www.jmir.org/2014/3/e93/ v16i3e93 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Fry J, Neff R. Periodic prompts and reminders in health promotion and health behavior interventions: systematic review. J Med Internet Res. 2009;11(2):e16. doi: 10.2196/jmir.1138. http://www.jmir.org/2009/2/e16/ v11i2e16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Bell A. "I think about Oprah": social class differences in sources of health information. Qual Health Res. 2014 Apr;24(4):506–16. doi: 10.1177/1049732314524637.1049732314524637 [DOI] [PubMed] [Google Scholar]
- 95.Diviani N, van den Putte B, Giani S, van Weert JC. Low health literacy and evaluation of online health information: a systematic review of the literature. J Med Internet Res. 2015;17(5):e112. doi: 10.2196/jmir.4018. http://www.jmir.org/2015/5/e112/ v17i5e112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Kalichman S, Cherry C, Cain D, Weinhardt L, Benotsch E, Pope H, Kalichman M. Health information on the Internet and people living with HIV/AIDS: information evaluation and coping styles. Health Psychol. 2006 Mar;25(2):205–10. doi: 10.1037/0278-6133.25.2.205.2006-03515-009 [DOI] [PubMed] [Google Scholar]
- 97.Elfeddali I, Bolman C, Candel Math JJ, Wiers W, de Vries H. Preventing smoking relapse via Web-based computer-tailored feedback: a randomized controlled trial. J Med Internet Res. 2012;14(4):e109. doi: 10.2196/jmir.2057. http://www.jmir.org/2012/4/e109/ v14i4e109 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Wienert J, Kuhlmann T. A stitch in time saves nine: things to consider when tailoring your online intervention. The Europeam Health Psychologist. 2015;17:12–7. http://openhealthpsychology.com/ehp/index.php/contents/issue/viewFile/ehp.v17.i1/pdf_43 . [Google Scholar]
- 99.Noguchi K, Albarracín D, Durantini M, Glasman L. Who participates in which health promotion programs? A meta-analysis of motivations underlying enrollment and retention in HIV-prevention interventions. Psychol Bull. 2007 Nov;133(6):955–75. doi: 10.1037/0033-2909.133.6.955.2007-15350-006 [DOI] [PMC free article] [PubMed] [Google Scholar]