

Introduction
Metastatic spread towards the carpalia is very rare [5], especially when the metastasis presents earlier then the primary tumor [4]. Malignant tumors rather disseminate to the lungs, liver or larger skeletal bones (e.g., the spine, pelvic or ribs) before metastasis might present in the carpal bones. The hand is affected in approximately 0.1 % of all metastatic spread, and even then, it most often occurs in the distal phalanges, followed by the metacarpal bones or proximal phalanges [5, 6].
We present a rare case of a patient whose painful wrist was the first clinical symptom of a pulmonary malignancy. The first plain X-ray of the hand revealed a radiolucency in the lunate and mild degenerative arthritis. The radiolucent lesion was initially not labeled as suspect for metastasis.
Case Presentation
An 83 year old man presented with a painful wrist to the rheumatologist. The pain might have started after lifting a large bucket of water. He had no history of trauma to the hand nor complaints of other joints. Apart from a single episode of hematuria, he had no other complaints or significant medical history. Plain radiography of the wrist (Fig. 1) showed some osteoarthritis in the radiocarpal and scaphotrapeziotrapezoid (STT) joints, which was considered to be in conformity with the patient’s age. Furthermore, a round radiolucency in the ulnar part of the lunate was seen, which was erroneously classified as an intraosseous cyst. An ultrasound of the wrist was performed and showed no signs of tenosynovitis or other abnormalities. The rheumatologist suspected an osteoarthritis after mild trauma and injected a triamcinolone solution (Kenacort®-A40) in the wrist. The pain did not resolve and a Magnetic Resonance Imaging (MRI) scan was performed (Figs. 2 and 3). The MRI revealed a completely pathological high intensity signal in the lunate that expanded following lunate-triquetral interosseous ligament into the triquetral bone with extensive reactive synovitis. So basically a bone disease with secondary synovial reactive change. The results were interpreted as suggestive for osteomyelitis, but a malignancy could not be ruled out. Subsequently, the patient was referred to the Handsurgery department. At that time, the patient had a swollen hand, which was kept in an antalgic neutral position. All active and passive movement of the wrist was extremely painful. Still, the only clinical symptoms were the painful swollen wrist and a single episode of hematuria. Revision of the plain X-ray made it obvious that cytologic aspiration puncture was needed immediately. Cytology revealed atypical cells, suggestive for malignancy (Fig. 4). Histological diagnosis was required. The search for a primary tumor started at the bladder, given the hematuria episode. Abdominal ultrasound was suspect for a tumor in the bladder. Two days later a cystoscopy and a proximal row carpectomy were performed simultaneously. Surprisingly, the cystoscopy revealed no tumors nor any suspicion of bladder pathology. The lunate, scaphoïd and triquetrum were sent to pathology and revealed a diagnosis consistent with large cell carcinoma (Fig. 5). The pain in the wrist subsided after surgery. Based on the immunohistochemistry, the primary tumor should either be a renal cell carcinoma or a pulmonary carcinoma. Computed Tomography scans were performed and a tumor at the superior sulcus on the right side was identified (Fig. 6). The patient was now without any symptoms and was referred to oncology. Two months after the initial consultation, the patient died.
Fig. 1.

PA view of the wrist shows an ill defined radiolucent ulnar aspect of the lunate. Ill defined margins are a sign of malignant disease
Fig. 2.
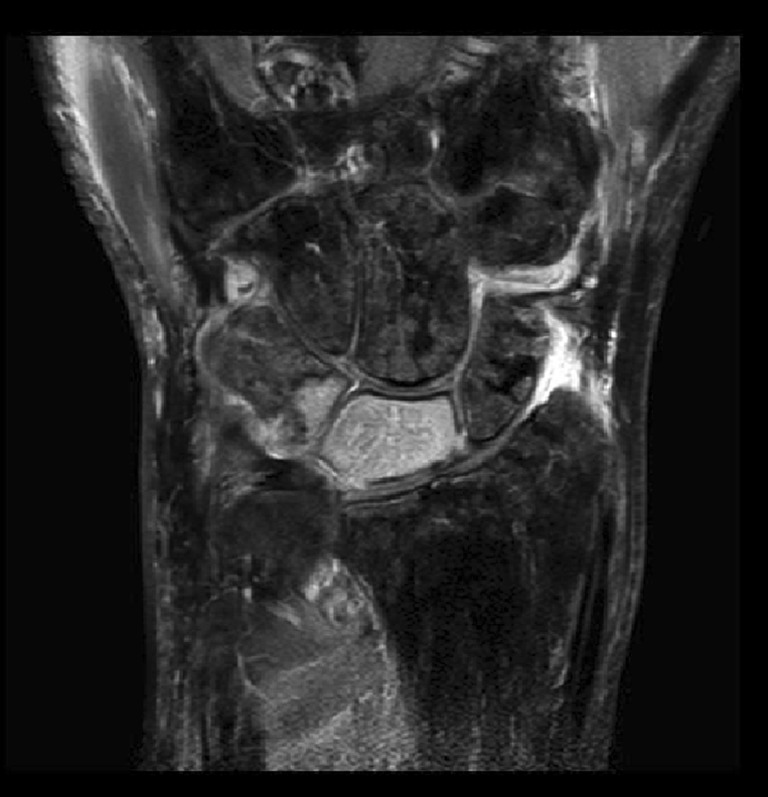
Coronal fat suppressed T2 weighted MR image shows the whole lunate bone with a high signal intensity, suggestive of complete infiltration
Fig. 3.

Sagittal proton density MR image clearly shows diffuse infiltration of the whole lunate bone
Fig. 4.
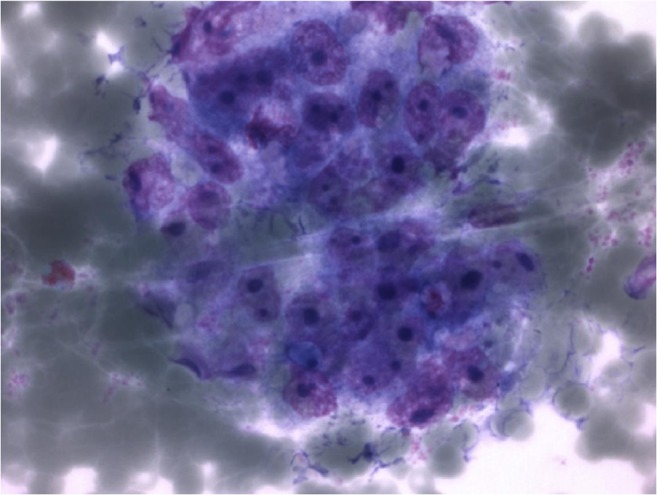
Cytology. Atypical cells suggestive for malignancy
Fig. 5.
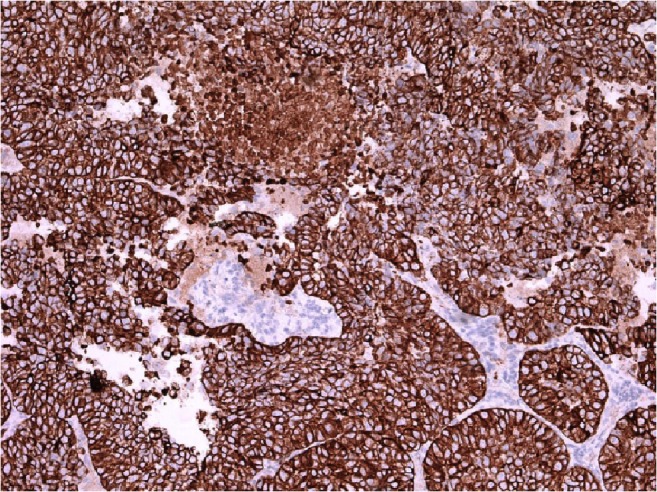
Immunohistochemistry. CKAE1/3, positive in case of carcinoma
Fig. 6.
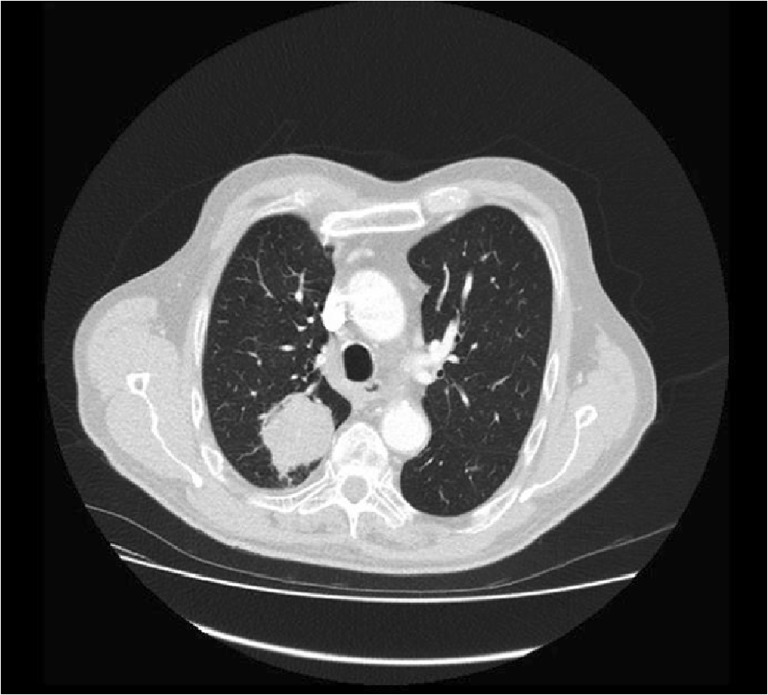
Axial Lung window CT scan shows tumor mass in the posterior paravertebral region in the right lung
Discussion
We present a case where a painful wrist and an osteolytic leasion on X-ray were the first signs of pulmonary malignancy. Initially erroneously classified as an intraosseous cyst histologic examination, after proximal row carpectomy, revealed a pulmonary metastasis.
Patients suffering from a superior sulcus (Pancoast) tumor usually present with shoulder or upper arm pain, Horner’s syndrome, muscle weakness and/or atrophy. Most superior sulcus tumors are non-small-cell lung carcinomas, e.g., squamous cell carcinoma or adenocarcinoma. The most frequent site of distant metastasis from a superior sulcus tumor is the brain, followed by bone.
Afshar et al. analyzed 221 cases of metastasis to the hand and wrist [3]. Lung, gastrointestinal tract and kidney were the most common locations of primary tumors. In 30 % of all cases the metastasis was the first presentation of occult malignant disease [3]. Only three reports of metastatic spread to the lunate were found [1, 8, 11]. All cases were from a primary lung carcinoma. None from other origins.
Due to its rarity, malignant disease in the carpalia is often initially not considered. Conservative therapy was not effective in our patient, and the X-ray findings were not initially interpreted as malignant. Apart from infectious conditions, the differential diagnosis of osteolytic lesions in the carpalia should include giant cell reparative granuloma [10], intraosseous epidermoid cyst [9], chondroblastoma [7], sarcoidosis [2], chrondosarcoma [12] and of course, metastatic spread from an occult primary tumor or multiple myeloma.
This case emphasizes the importance of initial radiological recognition of an infrequent presentation of metastatic disease, in the absence of clinical symptoms suspect for malignant disease. Uncommon combinations of clinical presentation and radiological findings should raise suspicion for more rare infectious or malignant pathological conditions. Metastasis should be considered in a patient with wrist pain and an osteolytic radiolucency on the plain X-ray. In addition, Afshar et al. argue that metastatic spread to the hand may be underreported, due to subclinical presentation, selection and reporting bias and missed cases and should therefore no longer be considered a rare finding in malignant disease [3]. Early recognition of metastasis in the hand may prevent delay of proper oncologic diagnosis treatment.
Footnotes
Each author certifies that he has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
Contributor Information
J. A. Strooker, Email: jooststrooker@gmail.com
M. Maas, Email: m.maas@amc.uva.nl
N. Bulkmans, Email: n.bulkmans@kg.nl
M. Kreulen, Email: kreulen@me.com
References
- 1.Abrahams T. Occult malignancy presenting as metastatic disease to hand and wrist. Skelet Radiol. 1995;24(2):135–137. doi: 10.1007/BF00198077. [DOI] [PubMed] [Google Scholar]
- 2.Adelaar R. Sarcoidosis of the upper extremity: case presentation and literature review. J Hand Surg [Am] 1983;8(4):492–496. doi: 10.1016/S0363-5023(83)80214-7. [DOI] [PubMed] [Google Scholar]
- 3.Afshar A, Farhadnia P, Khalkhali H. Metastases to the hand and wrist: an analysis of 221 cases. J Hand Surg [Am] 2014;39(5):923–932. doi: 10.1016/j.jhsa.2014.01.016. [DOI] [PubMed] [Google Scholar]
- 4.Flynn C, Danjoux C, Wong J et al (2008) Two cases of acrometastasis to the hands and review of the literature. Curr Oncol 51–58 [DOI] [PMC free article] [PubMed]
- 5.Kerin R. The hand in metastatic disease. J Hand Surg [Am] 1987;12(1):77–83. doi: 10.1016/S0363-5023(87)80164-8. [DOI] [PubMed] [Google Scholar]
- 6.Kerin R. Metastatic tumors of the hand: a review of the literature. J Bone Joint Surg Am. 1984;65:1331–1335. [PubMed] [Google Scholar]
- 7.Kudo T, Okada K, Hirano Y, Sageshima M. Chondroblastoma of the metacarpal bone mimicking an aneurysmal bone cyst: a case report and a review of the literature. Tohoku J Exp Med. 2001;194(4):251–257. doi: 10.1620/tjem.194.251. [DOI] [PubMed] [Google Scholar]
- 8.Lochonovsky J, Pavlansky R. Metastasis in the os lunatum as the 1st symptom of bronchogenic carcinoma. Acta Chir Orthop Traumatol Cech. 1966;33(5):387–390. [PubMed] [Google Scholar]
- 9.Mattiassich G, Ensat F, Hager M, Wechselberger G (2012) A suspected malignancy in osteolytic bone tumour of the thumb. BMJ Case Rep [DOI] [PMC free article] [PubMed]
- 10.Monacelli G, Rizzo M, Monarca C. Multicentric osteolytic lesion of the middle finger of the hand. Case report. G Chir. 2012;33(4):136–138. [PubMed] [Google Scholar]
- 11.Roncaglio C, Arena B. Metastasi alla mano da carcinoma broncopolmonare. Minerva Ortop Traumatol. 1993;44:37–43. [Google Scholar]
- 12.Tos P, Artiaco S, Linari A, Battiston B. Chondrosarcoma in the distal phalanx of the index finger: clinical report and literature review. Chir Main. 2009;28:265–269. doi: 10.1016/j.main.2009.02.002. [DOI] [PubMed] [Google Scholar]