

Abstract
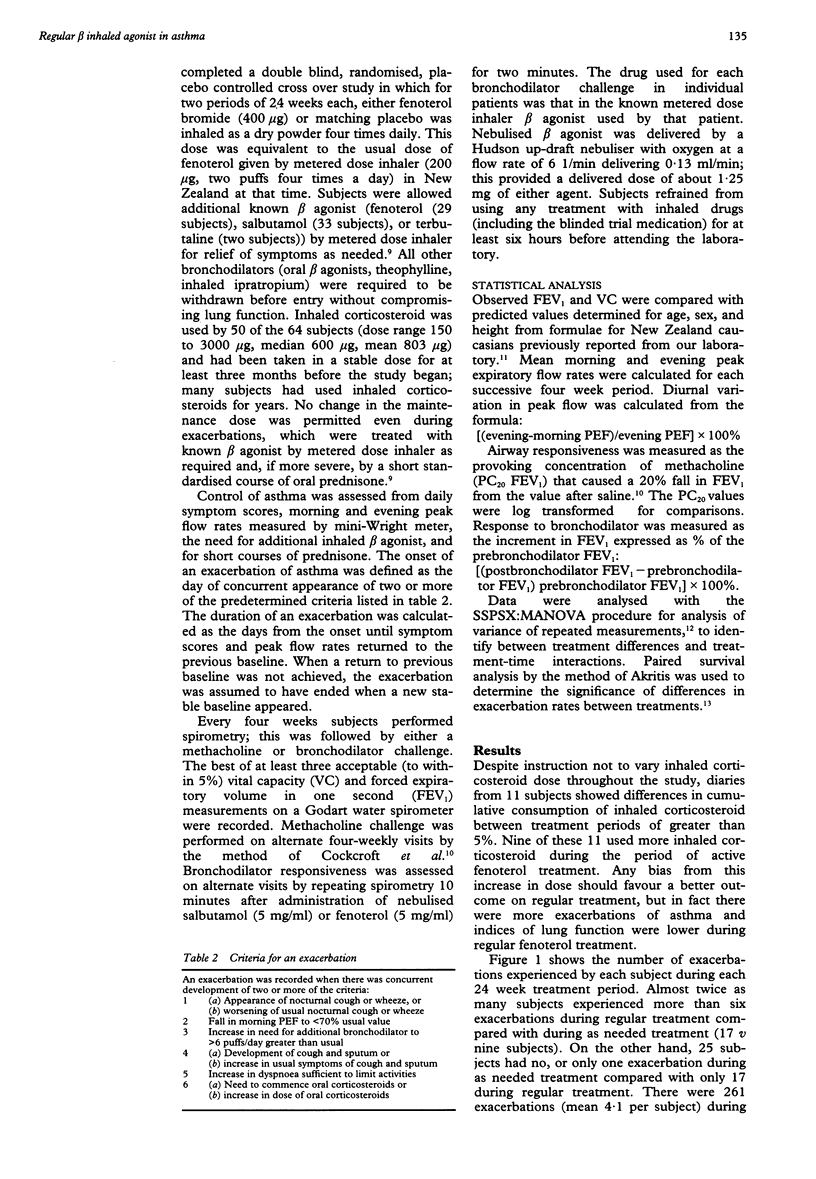
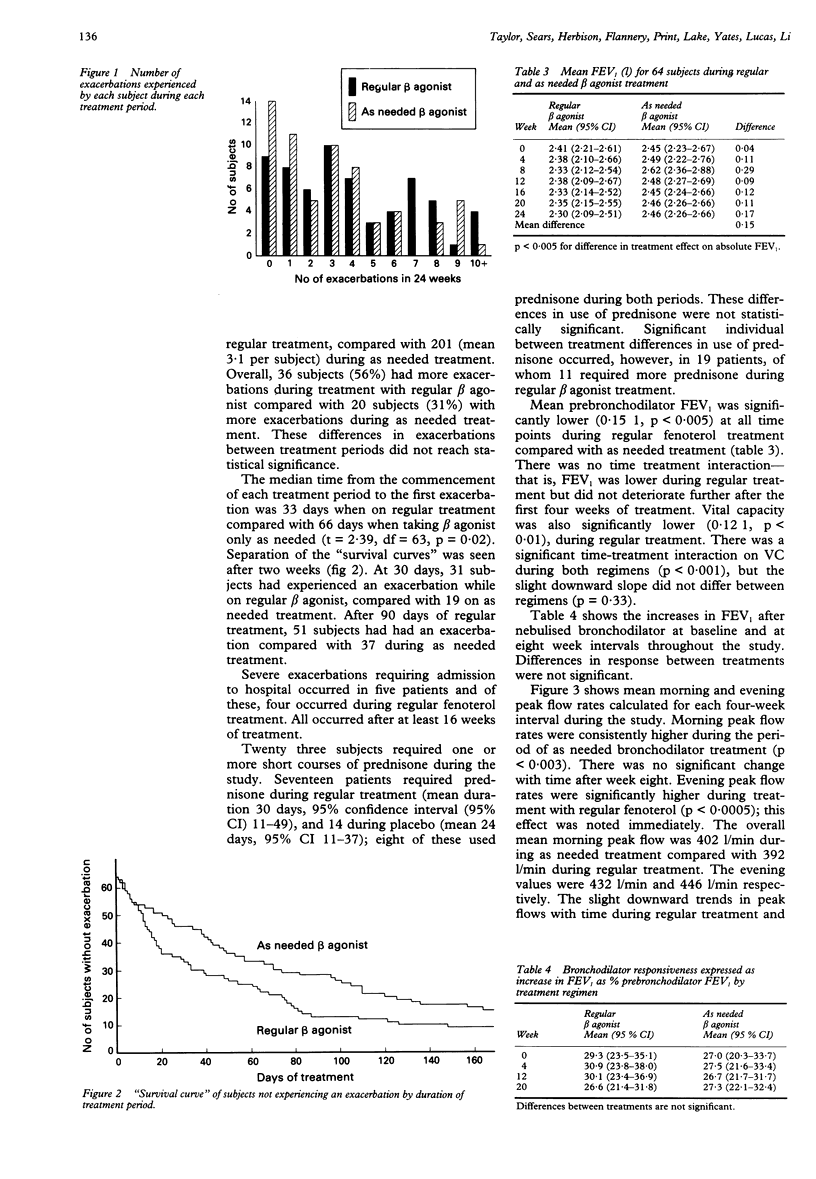
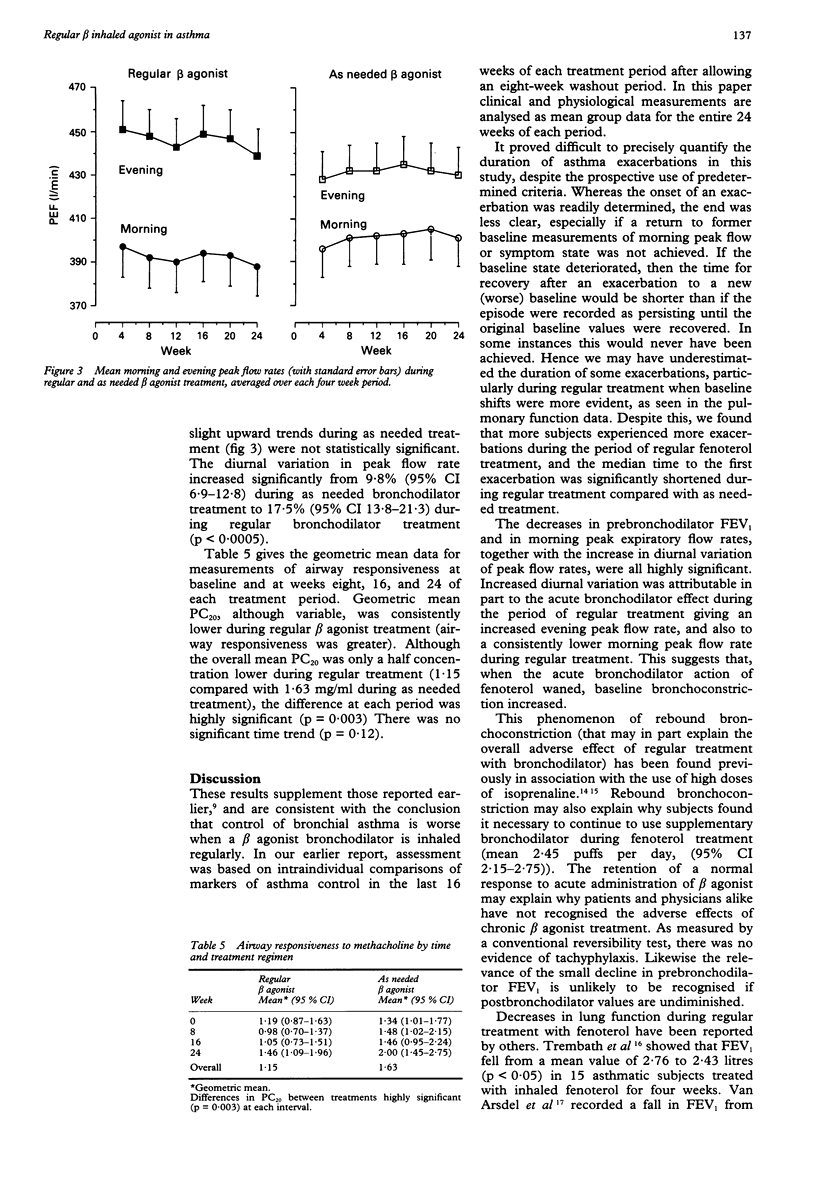
BACKGROUND: A comparison of the effects of regular upsilon as needed inhaled beta agonist treatment on the control of asthma in the last 16 weeks of each of two 24 week treatment periods has been reported. This paper presents additional information on exacerbations of asthma and trends in lung function, airways hyperresponsiveness to methacholine, and bronchodilator responsiveness during the entire 24 week periods of regular or as needed beta agonist treatment. METHODS: Subjects undertook a year long randomised, double blind crossover study of regular upsilon as needed inhaled beta agonist treatment. Fenoterol (400 micrograms) or matching placebo was inhaled as a dry powder four times daily for 24 weeks, then subjects crossed over to the alternative regimen. Treatment with inhaled corticosteroids was used by 50 of the 64 subjects in constant doses throughout the study. Symptoms, peak expiratory flow rates, and drug use were recorded daily, spirometry was performed every four weeks, and methacholine and bronchodilator responsiveness were measured every eight weeks. RESULTS: Exacerbations of asthma symptoms occurred earlier and more often during regular treatment with fenoterol and four of five severe exacerbations requiring admission to hospital occurred during the period of regular treatment. Prebronchodilator forced expiratory volume in one second (FEV1) was on average 0.15 litres lower (95% confidence interval (95% CI) 0.11-0.19) and vital capacity (VC) 0.12 litres lower (95% CI 0.08-0.16) than during the placebo period. Morning peak flow rates were significantly lower and evening peak flow rates significantly higher, with an increase in diurnal variation from 9.8% (95% CI 6.9-12.8) to 17.5% (95% CI 13.8-21.3) during regular treatment. Geometric mean concentration of methacholine causing a 20% fall in FEV1 from the value after saline (PC20) decreased significantly from 1.63 to 1.15 mg/ml, indicating increased bronchial hyperresponsiveness during regular treatment. Response to bronchodilator, as measured by the % increase in postbronchodilator FEV1 related to prebronchodilator FEV1, was maintained with no evidence for tachyphylaxis. CONCLUSION: Chronic use of inhaled fenoterol resulted in more exacerbations, a significant decline in baseline lung function, and an increase in airway responsiveness to methacholine in asthmatic subjects, but did not alter bronchodilator responsiveness. These findings support the previous report that regular inhaled beta agonist treatment is deleterious in the long term control of asthma.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Anderson H. R. Increase in hospital admissions for childhood asthma: trends in referral, severity, and readmissions from 1970 to 1985 in a health region of the United Kingdom. Thorax. 1989 Aug;44(8):614–619. doi: 10.1136/thx.44.8.614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cockcroft D. W., Killian D. N., Mellon J. J., Hargreave F. E. Bronchial reactivity to inhaled histamine: a method and clinical survey. Clin Allergy. 1977 May;7(3):235–243. doi: 10.1111/j.1365-2222.1977.tb01448.x. [DOI] [PubMed] [Google Scholar]
- Dutoit J. I., Salome C. M., Woolcock A. J. Inhaled corticosteroids reduce the severity of bronchial hyperresponsiveness in asthma but oral theophylline does not. Am Rev Respir Dis. 1987 Nov;136(5):1174–1178. doi: 10.1164/ajrccm/136.5.1174. [DOI] [PubMed] [Google Scholar]
- Harvey J. E., Tattersfield A. E. Airway response to salbutamol: effect of regular salbutamol inhalations in normal, atopic, and asthmatic subjects. Thorax. 1982 Apr;37(4):280–287. doi: 10.1136/thx.37.4.280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jackson R., Sears M. R., Beaglehole R., Rea H. H. International trends in asthma mortality: 1970 to 1985. Chest. 1988 Nov;94(5):914–918. doi: 10.1378/chest.94.5.914. [DOI] [PubMed] [Google Scholar]
- Juniper E. F., Kline P. A., Vanzieleghem M. A., Hargreave F. E. Reduction of budesonide after a year of increased use: a randomized controlled trial to evaluate whether improvements in airway responsiveness and clinical asthma are maintained. J Allergy Clin Immunol. 1991 Feb;87(2):483–489. doi: 10.1016/0091-6749(91)90006-a. [DOI] [PubMed] [Google Scholar]
- Keighley J. F. Iatrogenic asthma associated with adrenergic aerosols. Ann Intern Med. 1966 Nov;65(5):985–995. doi: 10.7326/0003-4819-65-5-985. [DOI] [PubMed] [Google Scholar]
- Kerrebijn K. F., van Essen-Zandvliet E. E., Neijens H. J. Effect of long-term treatment with inhaled corticosteroids and beta-agonists on the bronchial responsiveness in children with asthma. J Allergy Clin Immunol. 1987 Apr;79(4):653–659. doi: 10.1016/s0091-6749(87)80163-x. [DOI] [PubMed] [Google Scholar]
- Kraan J., Koëter G. H., vd Mark T. W., Sluiter H. J., de Vries K. Changes in bronchial hyperreactivity induced by 4 weeks of treatment with antiasthmatic drugs in patients with allergic asthma: a comparison between budesonide and terbutaline. J Allergy Clin Immunol. 1985 Oct;76(4):628–636. doi: 10.1016/0091-6749(85)90786-9. [DOI] [PubMed] [Google Scholar]
- Lipworth B. J., Clark R. A., Dhillon D. P., McDevitt D. G. Subsensitivity of beta-adrenoceptor responses in asthmatic patients taking regular low dose inhaled salbutamol. Eur J Clin Pharmacol. 1990;38(2):203–205. doi: 10.1007/BF00265986. [DOI] [PubMed] [Google Scholar]
- Mitchell E. A. Is current treatment increasing asthma mortality and morbidity? Thorax. 1989 Feb;44(2):81–84. doi: 10.1136/thx.44.2.81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reisman R. E. Asthma induced by adrenergic aerosols. J Allergy. 1970 Sep;46(3):162–177. doi: 10.1016/0021-8707(70)90095-x. [DOI] [PubMed] [Google Scholar]
- Sears M. R., Taylor D. R., Print C. G., Lake D. C., Li Q. Q., Flannery E. M., Yates D. M., Lucas M. K., Herbison G. P. Regular inhaled beta-agonist treatment in bronchial asthma. Lancet. 1990 Dec 8;336(8728):1391–1396. doi: 10.1016/0140-6736(90)93098-a. [DOI] [PubMed] [Google Scholar]
- Sinclair S. W., Avery S. F., Brady D. M., Smith D. A., Holst P. E., O'Donnell T. V. Prediction formulae for normal pulmonary function values in New Zealand European subjects. N Z Med J. 1980 Jan 9;91(651):1–5. [PubMed] [Google Scholar]
- Tashkin D. P., Conolly M. E., Deutsch R. I., Hui K. K., Littner M., Scarpace P., Abrass I. Subsensitization of beta-adrenoceptors in airways and lymphocytes of healthy and asthmatic subjects. Am Rev Respir Dis. 1982 Feb;125(2):185–193. doi: 10.1164/arrd.1982.125.2.185. [DOI] [PubMed] [Google Scholar]
- Trembath P. W., Greenacre J. K., Anderson M., Dimmock S., Mansfield L., Wadsworth J., Green M. Comparison of four weeks' treatment with fenoterol and terbutaline aerosols in adult asthmatics. A double-blind crossover study. J Allergy Clin Immunol. 1979 Jun;63(6):395–400. doi: 10.1016/0091-6749(79)90212-4. [DOI] [PubMed] [Google Scholar]
- VanArsdel P. P., Jr, Schaffrin R. M., Rosenblatt J., Sprenkle A. C., Altman L. C. Evaluation of oral fenoterol in chronic asthmatic patients. Chest. 1978 Jun;73(6 Suppl):997–998. doi: 10.1378/chest.73.6_supplement.997. [DOI] [PubMed] [Google Scholar]
- Vathenen A. S., Knox A. J., Higgins B. G., Britton J. R., Tattersfield A. E. Rebound increase in bronchial responsiveness after treatment with inhaled terbutaline. Lancet. 1988 Mar 12;1(8585):554–558. doi: 10.1016/s0140-6736(88)91352-9. [DOI] [PubMed] [Google Scholar]
- Weber R. W., Smith J. A., Nelson H. S. Aerosolized terbutaline in asthmatics: development of subsensitivity with long-term administration. J Allergy Clin Immunol. 1982 Dec;70(6):417–422. doi: 10.1016/0091-6749(82)90003-3. [DOI] [PubMed] [Google Scholar]
- Woolson R. F., O'Gorman T. W. A comparison of several tests for censored paired data. Stat Med. 1992 Jan 30;11(2):193–208. doi: 10.1002/sim.4780110206. [DOI] [PubMed] [Google Scholar]
- van Schayck C. P., Dompeling E., van Herwaarden C. L., Folgering H., Verbeek A. L., van der Hoogen H. J., van Weel C. Bronchodilator treatment in moderate asthma or chronic bronchitis: continuous or on demand? A randomised controlled study. BMJ. 1991 Dec 7;303(6815):1426–1431. doi: 10.1136/bmj.303.6815.1426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Schayck C. P., Graafsma S. J., Visch M. B., Dompeling E., van Weel C., van Herwaarden C. L. Increased bronchial hyperresponsiveness after inhaling salbutamol during 1 year is not caused by subsensitization to salbutamol. J Allergy Clin Immunol. 1990 Nov;86(5):793–800. doi: 10.1016/s0091-6749(05)80185-x. [DOI] [PubMed] [Google Scholar]