

Highlights
-
•
THA in patients with developmental dysplasia of the hip can be a complex procedure due to acetabular and proximal femoral deformities.
-
•
An adequate fixation of an acetabular roof reinforcement ring to the pelvis with cancellous bone screws is crucial for the stability of the prosthesis.
-
•
The conical femoral stem is an efficient implant. Optimum anteversion of the stem is possible with no technical difficulties.
Keywords: Developmental dysplasia of the hip, Total hip arthroplasty, Roof reinforcement ring, Conical stem
Abstract
Introduction
Total hip arthroplasty in patients with developmental dysplasia of the hip can be a complex procedure due to acetabular and proximal femoral deformities.
Presentation of case
A 59-year-old male patient underwent a total hip arthroplasty for the treatment of end-stage dysplastic osteoarthritis. A roof reinforcement ring, a cemented polyethylene cup, and a cementless stem were used. A portion of the superior rim of the ring was uncovered by the host bone. Morsellized autogenous femoral-head graft was impacted to fill the space between the superior rim of the ring and the superior part of the dysplastic acetabulum. At the follow-up after 5-years, the patient had no complaints and was very satisfied with the operation result. The hip radiograph revealed no signs of instability of the acetabular component, and no bone graft resorption.
Discussion
Favorable results were described using metal rings and conical femoral stems for the treatment of the developmental dysplasia of the hip. The superior rim of the metal ring should be against host bone for 60% of its support. Despite the suboptimal implantation of the ring compromising, apparently, mechanical stability of the arthroplasty, the outcome was favorable.
Conclusion
This result can be supported by the good fixation of the metal ring to the pelvis with screws, the adequate orientation of both components of the total hip arthroplasty, and the bone graft incorporation.
1. Introduction
The outcomes of maltreated or neglected developmental dysplasia of the hip are highly detrimental. Degree of subluxation and time left untreated are the two main factors that contribute to severity of the sequelae of this disorder [1].
Total hip arthroplasty (THA) is the procedure of choice for most patients with symptomatic end-stage osteoarthritis secondary to hip dysplasia [2]. Ideally, the acetabular cup is covered completely by host bone and should span the distance between the teardrop and the superolateral margin of the acetabulum [3].
Standard cementless femoral stems with a rectangular cross-section can be difficult to use for the treatment of dysplastic osteoarthritis, due to the femoral proximal deformities. A cementless stem with a conical shape can be indicated [4].
In this report a THA was performed for the treatment of a hip osteoarthritis secondary to developmental dysplasia. An acetabular roof reinforcement ring with a cemented polyethylene cup, and a conical stem were implanted. A superolateral portion of the metal ring was uncovered by host-bone, due to an inadequate operative technique.
The purpose of this paper was to show the outcome of the THA at 5-years follow-up, namely the mechanical behavior of the acetabular component.
2. Case report
A 59-year-old male patient underwent a total hip arthroplasty for the treatment of end-stage dysplastic osteoarthritis, in 2010. He presented a severe hip pain, functional impairment, the limb-length discrepancy was 30 mm, and was Thendelenburg-type gait. The pelvic radiograph revealed dysplasia of the right acetabulum according Hartofilakidis classification [5], coxa valga, and pelvic obliquity (Fig. 1). The right femoral head presented marginal osteophytes and was large and flattened in shape. Using a standard posterior approach, a roof reinforcement ring and a cemented polyethylene cup were implanted. The femur was reconstructed with a cementless femoral stem with conical shape.
Fig. 1.

Preoperative anteroposterior radiograph of the pelvis showing advanced right hip osteoarthritis, dysplasia of the acetabulum and coxa valga, and pelvic obliquity.
An appropriate size ring was inserted with a slight press-fit into the acetabulum, and secured using cancellous bone screws in order to achieve satisfactory mechanical fixation to the pelvis. A polyethylene cup was then secured with cement in the desired position. Thus, optimum anteversion and inclination is possible, regardless of the position of the ring.
However, a portion of the rim of the metal ring was uncovered by host bone. Then, the removed femoral head was morsellized (using a rongeur) on table, and bone graft was carefully impacted to fill the space between the uncovered border of the ring, and the superolateral margin of the native acetabulum. A conical stem was easily implanted with a correct femoral anteversion.
The postoperative course showed no problems with respect to the hip. Daily activity was quickly resumed. At 6-months after surgery the patient presented an asymptomatic hip with no limping, and approximation of equalization of limb-length. At 1-years follow-up the hip radiograph revealed a satisfactory orientation of the prosthesis, a small medialization of hip’s center of rotation, and some heterotopic ossifications. The bone autograft was incorporated (Fig. 2).
Fig. 2.

Postoperative THA radiograph at follow-up period of 1-year. The superolateral portion of the roof reinforcement ring is not covered by the native acetabulum. It is possible to observe the incorporation of impacted morsellized autograft placed between the rim of the metal ring and the superior part of the dysplastic acetabulum.
At 5-years follow-up, the patient continued to present a stable and asymptomatic hip and expressed high degree of satisfaction with surgery result. The hip radiograph showed unchanged and stable seating of the acetabular component, and stable fixation of the femoral stem by bone ingrowth, no measurable subsidence or radiolucent lines around the stem (Fig. 3). Heterotopic ossifications can be observed and were classified as stage I according to the classification of Brooker [6]. The autograft presented no signs of bone resorption.
Fig. 3.
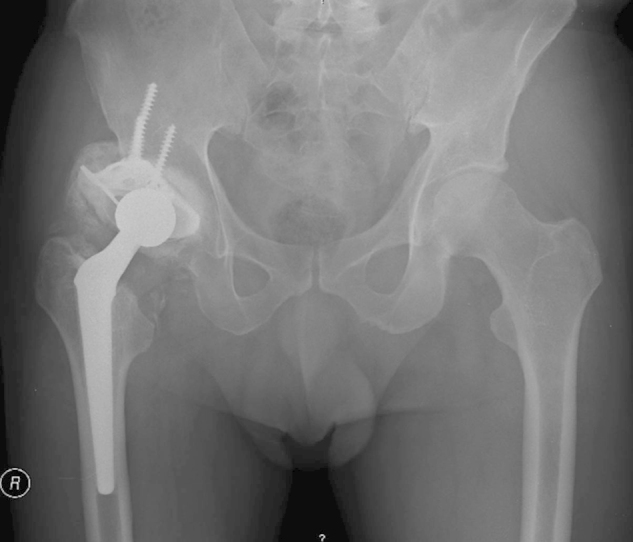
Postoperative THA radiograph at follow-up period of 5-years showing no signs of implant instability, no signs of bone graft resorption, and approximation of the leg lengths equality.
3. Discussion
Pain and severe functional impairment with limping in end-stage osteoarthritis of the hip, secondary to developmental dysplasia, are a clear indication for THA [5].
Due to femoral proximal deformities and excessive anteversion of the femur in hip dysplasia, we preferred the use of a cementless femoral stem with conical shape, and with a rounded cross-section. The conical fixation of the stem ensure excellent primary stability [7]. It is possible to produce correct femoral anteversion with no technical difficulties.
In dysplastic hip the acetabular component can usually be placed in the true acetabulum. Restoration of the hiṕs center of rotation and the femoral lateral offset, and limb-length equality are important goals to achieve. [5].
In our case the acetabular reconstruction was done using a roof reinforcement ring with the polyethylene cup cemented to the ring. The metal ring can be optimally adapted to the shape of the acetabulum since the polyethylene cup is anchored using cement and, thus, may be freely positioned. Favorable results were described using metal rings in congenital dysplasia of the hip, and in complex primary or revision hip arthroplasty [8].
Nevertheless, a significant portion of the superolateral margin of the metal ring was uncovered by the host bone, because the osteophytes on the bottom of the acetabulum, the so-called double floor, were not sufficiently reamed down to the depth of the original acetabular fossa. This condition led to incomplete bony coverage of the ring and suboptimal stability. The superior rim of the metal ring should be against host bone for 60% of its support [9]. Insufficient acetabular bone coverage may affect the durability of acetabular cup fixation [10].
In order to obtain augmentation of the acetabular ring a biological technique was used. After the cementation of the polyethylene cup, morsellized cancellous bone autograft was impacted between the lateral border of the metal ring and the superior part of the dysplastic acetabulum.
Incorporation and remodeling of the impacted morsellized bone graft was found. At 1-years of follow-up, the hip radiograph showed continuation of the trabecular lines from the host bone into the graft. The value of this technique was demonstrated in dysplastic hip [11].
At the follow-up after 5-years, the patient had no complaints regarding the right hip and regarded the outcome of the operation as very satisfactory. The hip radiograph showed no signs of instability of the roof reinforcement ring and of the femoral stem, and no signs of resorption of autograft.
THA in patients with developmental dysplasia of the hip can be a complex procedure due to acetabular and proximal femoral deformities. The main problems continue to be the restoration of the normal anatomy, and the fixation of the acetabular component, requiring meticulous preoperative patient evaluation and surgical planning. In this report, bone insufficiency coverage of the acetabular component was well tolerated.
Despite cementless acetabular reconstruction without acetabular augmentation is now the standard of care in dysplastic hips, we believe that the favorable outcome of our case can be supported by the solid fixation of the metal ring to the pelvis with cancellous bone screws, the osseointegration of the blasted pure titanium surface of the metal ring, the correct inclination angle of the cemented acetabular cup, the correct orientation of femoral stem, and the bone graft incorporation. It is possible that the autograft has played some role in mechanical stability of the acetabular prosthesis.
Nevertheless, further follow-up is required to determine the mechanical behavior of the implants in long-term.
Conflict of interest
The authors declare that they have no competing interests.
Funding
None.
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal upon request.
Author contribution
All authors contributed to the writing and collection of data, and they have participated in the surgery.
All authors read and approved the final manuscript for submission.
Contributor Information
Fernando M. Judas, Email: fernandojudas@gmail.com, fernandojudas@iol.pt.
Francisco M. Lucas, Email: francisco.m.lucas@gmail.com.
Ruben L. Fonseca, Email: ruben_fonseca@msn.com.
References
- 1.Rosenstein A.D., Diaz R.J. Challenges and solutions for total hip arthroplasty in treatment of patients with symptomatic sequelae of developmental dysplasia of the hip. Am. J. Orthop. 2011;40:87–91. [PubMed] [Google Scholar]
- 2.Sanchez-Sotelo J., Berry D.J., Trousdale R.T., Cabanela M.E. Surgical treatment of developmental dysplasia of the hip in adults: II. Arthroplasty options. J. Am. Acad. Orthop. Surg. 2002;10:334–344. doi: 10.5435/00124635-200209000-00005. [DOI] [PubMed] [Google Scholar]
- 3.Pulido W.J. Surgical principles of total hip arthroplasty. In: Parvizi J., Klatt B.A., editors. Essentials in Total Hip Arthroplasty. Slack Incorporated; 2013. pp. 147–152. (Chapter 8) [Google Scholar]
- 4.Castelli C.C., D'angelo F., Molina M., Ferrario A., Cherubino P. Radiographic evaluation of the conus uncemented stem. Hip Int. 1999;9:133–138. [Google Scholar]
- 5.Hartofilakidis G., Karachalios T. Surgical Techniques in Orthopaedics and Traumatology. Elsevier; Paris: 2000. Total hip replacement in congenital hip disease. 55-440-E-10. [Google Scholar]
- 6.Brooker A.F., Bowerman J.W., Robinson R.A., Riley L.H., Jr. Ectopic ossification following total hip replacement: incidence and a method of classification. J. Bone Joint Surg. Am. 1973;55:1629–1632. [PubMed] [Google Scholar]
- 7.Wagner H., Wagner M. Cone prosthesis for the hip joint. Arch. Orthop. Trauma Surg. 2000;120:88–95. doi: 10.1007/pl00021223. [DOI] [PubMed] [Google Scholar]
- 8.Krishnan K.M., Longstaff L., Partington P. Acetabular reconstruction using morcellised bone with ring support—medium-term results at three to nine years. Acta Orthop. Belg. 2011;77(1):61–67. [PubMed] [Google Scholar]
- 9.Udomkiat P., Dorr L.D., Won Y.Y., Longjohn D., Wan Z. Technical factors for success with metal ring acetabular reconstruction. J. Arthroplasty. 2001;16(8):961–969. doi: 10.1054/arth.2001.27669. [DOI] [PubMed] [Google Scholar]
- 10.Dorr L.D., Tawakkol S., Moorthy M., Long W., Wan Z. Medial protrusio technique for placement of a porous-coated: hemispherical acetabular component without cement in a total hip arthroplasty in patients who have acetabular dysplasia. J. Bone Joint Surg. Am. 1999;81:83–92. doi: 10.2106/00004623-199901000-00012. [DOI] [PubMed] [Google Scholar]
- 11.Kaneuji A., Sugimori T., Ichiseki T., Yamada K., Fukui K., Matsumoto T. Minimum ten-year results of a porous acetabular component for Crowe I to III hip dysplasia using an elevated hip center. J. Arthroplasty. 2009;24:187–194. doi: 10.1016/j.arth.2007.08.004. [DOI] [PubMed] [Google Scholar]