

Highlights
-
•
Sarcoidosis is a multisystemic, idiopathic disease.
-
•
Thyroid cancer is rarely reported in the literature.
-
•
We present a case with sarcoidosis mimicking metastatic papillary thyroid cancer.
Keywords: Sarcoidosis, Metastatic papillary thyroid cancer, Neck mass
Abstract
Introduction
Sarcoidosis is a multisystemic, idiopathic disease. It has a highly variable clinical course. It has been reported to present in association with malignancy. Coexistence of sarcoidosis and thyroid cancer is rarely reported in the literature.
Presentatioin of the case
We present a case with neck swelling for 3 months, and symmetrical painless thyroid enlargement without fixation to deep tissues of the neck. Multiple nodules on the both thyroid lobes, hard irregular, grade two goiter with lymphadenopathy all over anterior neck compartments. Fine needle aspiration cytology was done under ultrasound guide from right thyroid nodule and showed papillary thyroid carcinoma. Excisional biopsy of the neck lymphnode showed picture typical for sarcoidosis.
Discussion
Most researchers believe that patients with pulmonary sarcoidosis are predisposed to develop malignancies, less than a dozen of cases are reported in the literature to be associated with PTC with a very wide range of presentations and clincal coarses. An interesting finding of our case is that in contrast to what is reported, both diseases were not known by the physician until the time of presentation.
Conclusion
Cervical lymphadenopathy in association with goiter could be metastasis, sarcoidosis or mixed, therefore should be seperately biopsied.
1. Introduction
Sarcoidosis (SA) (flesh-like process) is a multisystemic, idiopathic disease which is characterized by non-caseating epithelioid granulomas mainly involving the lungs (90%), lymph nodes, eyes, and skin [1]. It has a highly variable clinical course [2]. Sarcoidosis has been reported to present in association with malignancy, either preceding, during, or after chemotherapy [3]. The development of cervical lymphadenopathy in a patient with both (SA) and (PTC) can create a diagnostic dilemma. Occasionally, lymph nodes with PTC metastasis and SA may coexist in the neck [4].
It is very important to obtain a tissue diagnosis of suspicious metastatic lesions. We report a case of papillary thyroid cancer presenting with multiple sarcoid lesion (cervical and hilar limphadenopathy) mimicking metastatic lesions.
2. Case report
A 48-year-old female presented with neck swelling for 3 months without significant associated symptoms. On examination, there was symmetrical painless thyroid enlargement without fixation to deep tissues of the neck. Multiple nodules on the both thyroid lobes, hard irregular, grade two goiter with lymphadenopathy all over anterior neck compartments. There was also clubbing of the fingers. Ultrasound of the neck showed three small nodules with 5 mm and less in diameter, 2 of them are solid other is cystic, neither calcification no abnormal vasculature is seen. Also there was complex solid nodule of about 25 × 17 mm in size in right lobe with spots of calcification and marked internal vascularity. There was bilateral cervical enlarged lymph nodes along the jugular chein, largist one reaching the size of 12 mm with abnormal architecture. T3 = 1.85 (nmol/L), T4 = 121 (nmol/L), TSH = 1.4 IU/mL. Chest X-ray showed bilateral hilar masses (Fig. 1). Fine needle aspiration cytology was done under ultrasound guide from right thyroid nodule and showed papillary thyroid carcinoma. Patient underwent total thyroidectomy with modified radical neck lymph nodes dissection for Level; II, III, IV and VI.
Fig. 1.
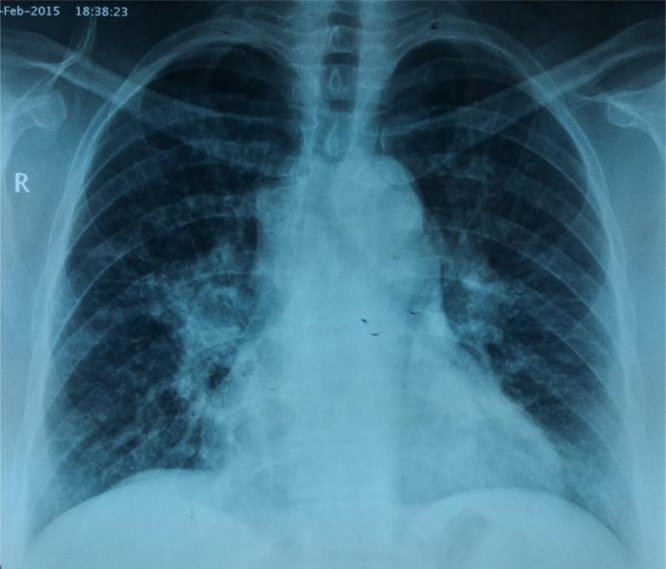
Showing bilateral hilar shadow.
(23 lymphnodes from each side) results of tissue biopsy confirmed PCT and metastasis to a right upper cervical lymphnode and other lymphnodes showed non-caseating granuloma, typical picture of sarcoidosis confirmed by multiple examinations. Post operatively patient was put on daily 125 μg of l-thyroxine, I-131 and steroid. Patient refused to do more invasive diagnostic workup for the hilar mass as facility for transbronchial biopsy are absent in our country. Three months after medication patient was free of symptoms and her chest X-ray showed decrease size of hilar shadow.
3. Discussion
Although there have been many theories on the link between sarcoidosis and malignancy, the association remains unproven [5]. Most researchers believe that patients with pulmonary sarcoidosis are predisposed to develop malignancies, but others presume that malignancies lead to sarcoidosis [6]. according to two retrospective case series, 4–14% of all patients with malignancy can exhibit some histopathological evidence of sarcoidosis [7], [8]. Although sarcoid reaction has been reported to be associated with various malignancies, less than a dozen of cases are reported in the literature to be associated with PTC with a very wide range of presentations and clincal coarses [4]. PTC are the most common thyroid malignancy, accounts for 80% of the all thyroid cancers. Management of co-existing PTC and SA can be challenging because both of diseases can affect the same organs and the incidences are very similar [4]. An interesting finding of our case is that both diseases were not known by the physician until the time of presentation while in other cases patients are known to have at least one of the disease before cosultation [1], [2], [5]. and this make more cofusion for diagnostic workup and need special attension.
4. Conclusion
Physician should think widely when facing neck mass, cervical lymphadenopathy in association with goiter could be metastasis or sarcoidosis or mixed, therefore should be seperately biopsied. Proper examination and and investigation of respiratory system are mandatory when a patient presented with neck mass to exclude co-existence diseases.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on reques.
Conflict of interest
There is no conflict of interest.
Funding
There is no sources of funding.
Ethical approval
Approval has been givenby ethics committee of bioscience center.
Author contribution
AbdulWahid M. Salih; performed operation. Data collection. Fahmi Kakamad; writing the manuscript. Salah M. Fatih; Data collection,examination and follow up.
Registration of research studies
Researchregistry559.
Guarantor
Fahmi H. Kakamad.
Contributor Information
Abdulwahid M. Salih, Email: awahidms@yahoo.com.
Salah M. Fatih, Email: Salahkalary@yahoo.com.
F.H. Kakamad, Email: fahmi.hussein@univsul.edu.iq.
Referrences
- 1.Viswanath Lokesh. Darier–Roussy sarcoidosis mimicking metastatic breast cancer. Case Rep. Oncol. 2009;2:251–254. doi: 10.1159/000262412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Shetty A., Carter J.D. Sarcoidosis mimicking lymphoma on FDG-PET imaging. Radiol. Case Rep. 2011;6:409. doi: 10.2484/rcr.v6i2.409. (Online) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Myint Zin W., Chow Robert D. J. Community Hosp. Intern. Med. Perspect. 2015;5:26360. doi: 10.3402/jchimp.v5.26360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ergin Ahmet Bahadir, Nas Christian E. Sarcoidosis and thyroid cancer. Sarcoidosis Vasc. Diffuse Lung Dis. 2014;31:240–243. [PubMed] [Google Scholar]
- 5.Mingins C., Williams M.R. Cox NH: subcutaneous sarcoidosis mimicking breast carcinoma. Br. J. Dermatol. 2002;146:924–925. doi: 10.1046/j.1365-2133.2002.04705.x. [DOI] [PubMed] [Google Scholar]
- 6.Krawczyk B.P., Gryglicka B., Kieszko R., Korobowicz E., Sojczuk S. Malignant neoplasms and pulmonary sarcoidosis—a case report. New Med. 2004;7:94–96. [Google Scholar]
- 7.Brincker H. Sarcoid reactions in malignanttumors. Cancer Treat. Rev. 1986;13:147–156. doi: 10.1016/0305-7372(86)90002-2. [DOI] [PubMed] [Google Scholar]
- 8.Llombart L., Jr, Escudero J.M. The incidence andsignificance of epithelioid and sarcoid-like cellular reaction in the stromata of malignant tumours: a morphological and experimental study. Eur. J. Cancer. 1970;6:545–551. doi: 10.1016/0014-2964(70)90076-9. [DOI] [PubMed] [Google Scholar]