

Highlights
-
•
Femoral neck stress fractures are not uncommon.
-
•
Osteomalacia is a common cause of insufficiency fractures.
-
•
Coxa vara is a rare cause of femoral neck stress fractures.
-
•
Co-existence of osteomalacia and coxa vara is a rare condition.
Abstract
Introduction
Femoral neck stress fractures are not uncommon. Several causes exist about these fractures. Osteomalacia is one of the most common cause of insufficiency fractures and coxa vara can produce a focal concentration of mechanical stress in the femoral neck and may cause stress fractures. This case study is about the co-existence of these two pathologies in a patient with bilateral femoral neck stress fracture.
Presentation of case
A 26-year-old woman admitted to our department with a complaint of bilateral groin pain and diagnosed as bilateral coxa vara and osteomalacia. Medical treatment for osteomalacia and staged bilateral Pauwels’ osteotomy was performed. After 2 years of follow-up, good result was obtained.
Discussion
There are several risk factors for stress fractures and osteomalacia and coxa vara are two of the causes. Osteomalacia results in softening of the bones and coxa vara can produce a focal concentration of stresses in the femoral neck.
Conclusion
Joint and bone pain without any trauma should be investigated and bone metabolism disorders should be kept in mind. There might be co-existing factors related with stress fractures, and they must be treated simultaneously.
1. Introduction
Stress fractures of the femoral neck can be classified as insufficiency and fatigue fractures. The distinction of these pathologies is important because the underlying pathology and treatment is different. Insufficiency fractures result with normal stresses on a bone with reduced strength and associated with different conditions [1]. Conversely, fatigue fractures occur in normal bone of a healthy individual who exercise and do repetitive activity [2].
Osteomalacia is one of the most common cause of insufficiency fractures. It is a bone methabolism disorder associated with defective bone mineralization. The causes of osteomalacia are varied, but ultimately result in a vitamin D deficiency [3].
Coxa vara is a hip deformity, which the femoral neck–shaft angle is less than 120°. This deformity can produce a focal concentration of mechanical stress in the femoral neck and may cause stress fractures [4].
In this paper, we present a case of bilateral femoral neck stress fracture due to osteomalacia and coxa vara treated by bilateral Pauwels osteotomy.
2. Presentation of case
A 26 year-old woman was referred to our department with a complaint of bilateral groin pain for 7 months and difficulty in walking. She denied any trauma. On examination, both hips had normal range of motions but painful in flexion-internal rotation. She was otherwise healthy and she had no medication or drug history.
Anteroposterior view of both hips was taken and a fracture line on the right femoral neck was seen. Also bilateral coxa vara was observed and bilateral neck–shaft angle was measured 113° (Fig. 1). Whereon, magnetic resonance imaging (MRI) of both hips were taken. In T2 weighted images, edema and a clear fracture line were seen in the right femoral neck, and a slight edema was seen in the left femoral neck (Fig. 2).
Fig. 1.
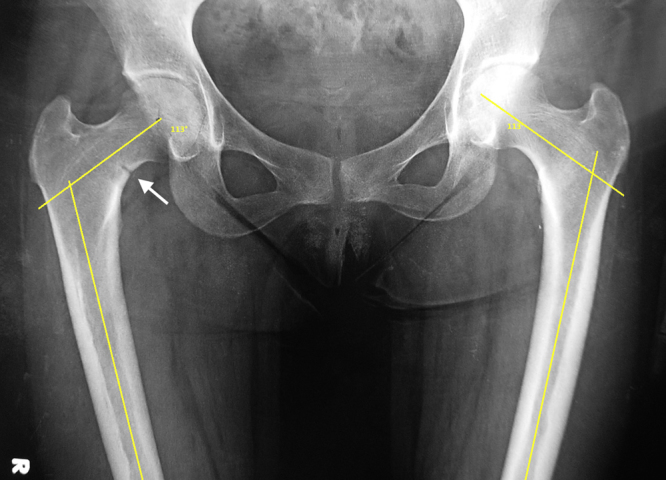
Preoperative AP view of both hips. A fracture line is seen in the inferomedial order of the right femoral neck. Both femoral neck–shaft angle is 113°.
Fig. 2.

Preoperative T2-weighted MRI images of both hips (A) coronal view (B) axial view. White arrow shows clear edema in the right femoral neck and black arrow shows a slight edema in the left femoral neck.
In her laboratory tests, blood count test was normal. Calcium level was 9.1 mg/dl (range 8.6–10.2), phosphor level was 3.7 mg/dl (range 2.6–4.5), parathyroid hormone (PTH) level was 187.1 pg/ml (range 15–65) and 25-hidroxyvitamin D level was 21.7 ng/ml (range 25–80). Subsequently, the patient was consulted with internal medicine department and vitamin D therapy started immediately. She underwent colonoscopy and the pathologic result was non-specific colitis.
After that surgery was planned. Under general anesthesia, with the patient on supine position, right hip Pauwels valgus osteotomy was performed with a 135°-angled plate (Fig. 3). Weight bearing was restricted for 3 months, and after 3 months, she underwent surgery for her left hip and same surgery was performed. After 3 months of non-weight bearing for left limb, she was able to walk without crutches and she had normal range of motions in both hips. After 2 years of follow up, she had no complaint and osteosynthesis was good (Fig. 4). In the laboratory tests, calcium, phosphor, PTH and 25-hidroxyvitamin D level became normal.
Fig. 3.
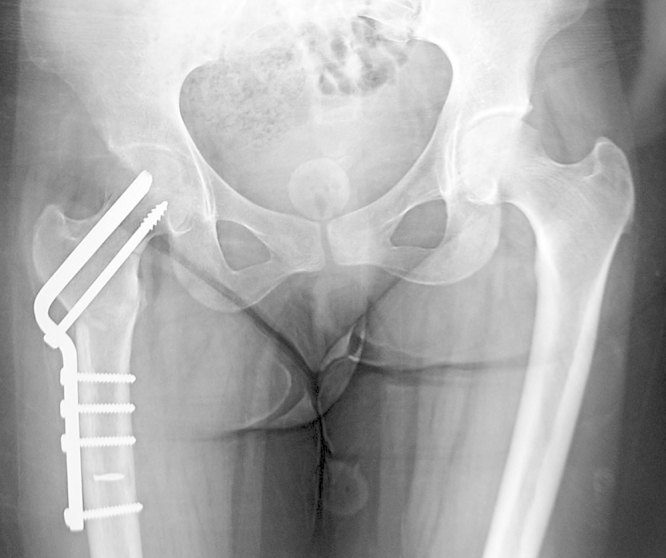
Postoperative AP view of both hips after right hip surgery.
Fig. 4.
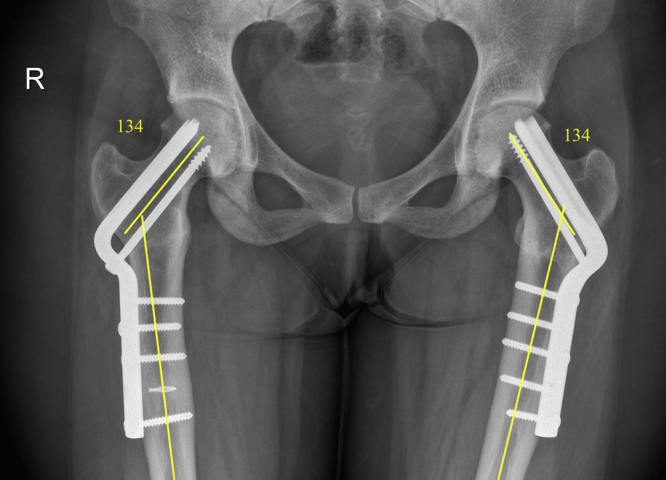
AP view of both hips after 2 years follow-up. Both femoral neck–shaft angle is 134°.
3. Discussion
Insufficiency fractures occur in weak bone under normal loading. There are several risk factors for these fractures and osteoporosis, osteomalacia, long-term corticosteroid and anticonvulsant treatment, renal osteodystrophy, amenorrhea, fluoride treatment and pelvic irradiation are some of the causes [1]. Fatigue fractures, on the other hand, occurs in normal bone of a healthy individual as a result of excessive and repetitive loading. These fractures are common in athletes, dancers and military personnel and also can result from normal forces on abnormal anatomy [2].
In this case report, there are two factors causing bilateral femoral neck stress fracture. One of them is osteomalasia, which is a common cause of insufficiency fractures, and the other one is, coxa vara, a rare cause of fatigue fractures.
Vitamin D deficiency is a global health problem [5] and can result from inadequate nutritional intake and/or inadequate sunlight exposure, limited vitamin D absorption and conditions effecting vitamin D catabolism including liver and kidney disorders. Deficiency effects bone mineralization and causes softening of the bones. It is called as rickets in children and osteomalacia in adults. In the literature, there are several reports of femoral neck stress fracture due to vitamin D deficiency [6], [7], [8]. In some countries these insufficiency fractures also known as Looser’s zones or Milkman’s lines. One of the common cause of osteomalacia is the inadequate sun exposure. Over 90% of vitamin D is derived from ultraviolet B light and the rest is obtained from the diet. In a fair-skinned person, 20–30 min of sunlight exposure on the face and forearms at midday are estimated to generate the equivalent of around 2000 IU of vitamin D. A recent survey in the UK showed that more than 50% of the adult population have insufficient levels of vitamin D and that 16% have severe deficiency during winter and spring. The highest rates were found in Scotland, Northern England and Northern Ireland [9].
Abnormal hip biomechanics can cause stress fractures. In the presence of implants in the femoral neck, gonarthrosis or total knee arthroplasty may lead to secondary stress fractures while the hip anatomy is normal [10], [11], [12], [13], [14], [15]. On the other hand, in the presence of abnormal hip anatomy, as in coxa vara, the deformity can produce a focal concentration of stresses in the femoral neck according to Pawels’ laws [4]. In a cohort study, Carpintero et al. analyzed 22 femoral neck stress fractures and found that coxa vara predisposes to femoral neck stress fracture [16].
Femoral neck stress fractures can be classified as compression and tension fractures [17], [18]. Compression fractures are seen in the inferomedial border of the femoral neck and mechanically stable. Tension fractures are seen in the superior border, can rapidly progress and can lead to displacement [17], [18], [19]. Treatment of femoral neck stress fractures are challenging. Compression type fractures can be treated conservatively because they are mechanically stable. However, tension type fractures need surgical fixation due to mechanical instability. In this case, the patient had compression type femoral neck fracture but we operated her because another factor exist, coxa vara, leading to mechanical abnormality.
Surgical treatment of femoral neck stress fractures include cannulated screws, dynamic hip screw, proximal femoral nail, angled or anatomic plates and arthroplasty. Proximal femoral valgus osteotomy with an angled plate is a good surgical option to align the hip mechanical axis. Intertrochanteric osteotomy was first introduced by Pauwels [20]. It was used to treat many hip problems such as, infantile coxa vara (ICV) and femoral neck nonunions [21], [22], [23], [24], [25]. This osteotomy converts shearing forces into compression forces. This osteotomy can be used in femoral neck stress fractures with coxa vara. Carpintero et al., treated 3 femoral neck stress fracture patients who had coxa vara with valgus osteotomy and obtained good results [16].
The distinctive features of this case include bilateral stress fractures with a co-existence of osteomalasia and coxa vara.
4. Conclusion
Femoral neck stress fractures is not uncommon and needs detailed intervention. In these conditions, the accurate history of the patient, sufficient imaging and laboratory tests for bone metabolism must be considered, and adequate treatment should be performed according to the results. Coxa vara can be co-existing pathology and must be kept in mind and must be treated.
Contributor Information
Kerim Sariyilmaz, Email: ksariyilmaz@gmail.com, ksariyilmaz@yahoo.com.
Okan Ozkunt, Email: drdeto@gmail.com.
Mustafa Sungur, Email: drmsungur@gmail.com.
Fatih Dikici, Email: fatihdikici71@hotmail.com.
Onder Yazicioglu, Email: onderyazicioglu@gmail.com.
References
- 1.Egol K.A. Stress fractures of the femoral neck. Clin. Orthop. Relat. Res. 1998;348:72–78. [PubMed] [Google Scholar]
- 2.Rome K., Handoll H.H., Ashford R. Interventions for preventing and treating stress fractures and stress reactions of bone of the lower limbs in young adults. Cochrane Database Syst. Rev. 2005;2:CD000450. doi: 10.1002/14651858.CD000450.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Aaron J.E. Frequency of osteomalacia and osteoporosis in fractures of the proximal femur. Lancet. 1974;1(7851):229–233. doi: 10.1016/s0140-6736(74)92545-8. [DOI] [PubMed] [Google Scholar]
- 4.Pauwels F. Springer-Verlag; New York: 1976. Biomechanics of the Normal and Diseased Hip. [Google Scholar]
- 5.Holick M.F., Chen T.C. Vitamin D deficiency: a worldwide problem with health consequences. Am. J. Clin. Nutr. 2008;87(4):1080S–1086S. doi: 10.1093/ajcn/87.4.1080S. [DOI] [PubMed] [Google Scholar]
- 6.Chadha M. Spontaneous bilateral displaced femoral neck fractures in nutritional osteomalacia—a case report. Acta Orthop. Scand. 2001;72(1):94–96. doi: 10.1080/000164701753606770. [DOI] [PubMed] [Google Scholar]
- 7.Faraj A.A. Bilateral simultaneous combined intra- and extracapsular femoral neck fracture secondary to nutritional osteomalacia: a case report. Acta Orthop. Belg. 2003;69(2):201–203. [PubMed] [Google Scholar]
- 8.Nagao S., Ito K., Nakamura I. Spontaneous bilateral femoral neck fractures associated with a low serum level of vitamin D in a young adult. J. Arthroplasty. 2009;24(2):322e1–322e4. doi: 10.1016/j.arth.2008.01.309. [DOI] [PubMed] [Google Scholar]
- 9.Pearce S.H., Cheetham T.D. Diagnosis and management of vitamin D deficiency. BMJ. 2010;340:b5664. doi: 10.1136/bmj.b5664. [DOI] [PubMed] [Google Scholar]
- 10.Baker D.M. Fractures of the femoral neck after healed intertrochanteric fractures: a complication of too short a nail plate fixation. Report of three cases. J. Trauma. 1975;15(1):73–81. [PubMed] [Google Scholar]
- 11.Dorne H.L., Lander P.H. Spontaneous stress fractures of the femoral neck. Am. J. Roentgenol. 1985;144(2):343–347. doi: 10.2214/ajr.144.2.343. [DOI] [PubMed] [Google Scholar]
- 12.Hardy D. [Subcapital fracture of the femoral neck: a rare complication of a pertrochanteric fracture healed in coxa vara position] Acta Orthop. Belg. 1990;56(2):507–511. [PubMed] [Google Scholar]
- 13.Hardy D.C. Stress fracture of the hip. An unusual complication of total knee arthroplasty. Clin. Orthop. Relat. Res. 1992;281:140–144. [PubMed] [Google Scholar]
- 14.Lesniewski P.J., Testa N.N. Stress fracture of the hip as a complication of total knee replacement. Case report. J. Bone Joint Surg. Am. 1982;64(2):304–306. [PubMed] [Google Scholar]
- 15.Satku K., Kumar V.P., Pho R.W. Stress fractures of the tibia in osteoarthritis of the knee. J. Bone Joint Surg. Br. 1987;69(2):309–311. doi: 10.1302/0301-620X.69B2.3818767. [DOI] [PubMed] [Google Scholar]
- 16.Carpintero P. Stress fractures of the femoral neck and coxa vara. Arch. Orthop. Trauma Surg. 2003;123(6):273–277. doi: 10.1007/s00402-003-0514-z. [DOI] [PubMed] [Google Scholar]
- 17.Fullerton L.R., Jr., Snowdy H.A. Femoral neck stress fractures. Am. J. Sports Med. 1988;16(4):365–377. doi: 10.1177/036354658801600411. [DOI] [PubMed] [Google Scholar]
- 18.Devas M.B. Stress fractures of the femoral neck. J. Bone Joint Surg. Br. 1965;47(4):728–738. [PubMed] [Google Scholar]
- 19.Diwanji S.R. Displaced stress fracture of the femoral neck treated by valgus subtrochanteric osteotomy: 2 case studies. Am. J. Sports Med. 2007;35(9):1567–1570. doi: 10.1177/0363546507299241. [DOI] [PubMed] [Google Scholar]
- 20.Pauwels F. [Biomechanics of bone grafts] Acta Orthop. Belg. 1971;37(6):701–725. [PubMed] [Google Scholar]
- 21.Anglen J.O. Intertrochanteric osteotomy for failed internal fixation of femoral neck fracture. Clin. Orthop. Relat. Res. 1997;341:175–182. [PubMed] [Google Scholar]
- 22.Said G.Z., Farouk O., Said H.G. Valgus intertrochanteric osteotomy with single-angled 130° plate fixation for fractures and non-unions of the femoral neck. Int. Orthop. 2010;34(8):1291–1295. doi: 10.1007/s00264-009-0885-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Magu N.K. Modified Pauwels’ intertrochanteric osteotomy in neglected femoral neck fracture. Clin. Orthop. Relat. Res. 2009;467(4):1064–1073. doi: 10.1007/s11999-008-0695-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Desai S.S., Johnson L.O. Long-term results of valgus osteotomy for congenital coxa vara. Clin. Orthop. Relat. Res. 1993;294:204–210. [PubMed] [Google Scholar]
- 25.Carroll K., Coleman S., Stevens P.M. Coxa vara: surgical outcomes of valgus osteotomies. J. Pediatr. Orthop. 1997;17(2):220–224. doi: 10.1097/00004694-199703000-00016. [DOI] [PubMed] [Google Scholar]