

Abstract
Musculoskeletal health benefits from flexibility training and maintaining a functional, or sport specific, range of motion is important to one’s overall fitness. Commercial foam rollers are commonly used in gyms, therapy clinics and homes, yet data are lacking on the optimal rolling duration and effect on range of motion.
Purpose :
The purpose of this study was to examine the effect of varied durations of a commercial foam roller treatment on hamstring range of motion.
Methods :
The knee extension range of motion of 33 college aged men and women (age= 20±1.5y, mass= 72.2±10.8 kg) was assessed after a short (2 sets of 10s) and long (4 sets of 30s) duration of hamstring self-administered myofascial release using a commercial foam roller. A one way ANOVA was performed to compare the mean knee extension angle for each condition to baseline measures.
Results :
Results indicated that neither the short duration (67.30 ± 10.60 deg) nor long duration (67.41 ± 10.81 deg) rolling condition produced significant increases in knee extension compared to baseline (67.70 ± 9.90 deg).
Conclusion :
Self-administered foam rolling for a total duration of up to 2 minutes is not adequate to induce improvements in knee joint flexibility. Contributing factors may include the amount of pressure imparted by the commercial roller as well as duration of treatment.
Keywords: Commercial foam rollers, foam rolling, myofascial release, hamstring flexibility, knee extension, range of motion.
INTRODUCTION
Musculoskeletal health benefits from flexibility training and maintaining a functional, or sport specific, range of motion (ROM) is important to one’s overall fitness [1, 2]. The most common methods employed to increase ROM are various forms of stretching including static, ballistic, and dynamic stretching as well as proprioceptive neuromuscular facilitation. It is common practice to implement one or a combination of these methods as warm-up prior to exercise or after activity. Among stretching methods, static stretching is most commonly utilized; however when utilized as part of a warm up, it has been shown to decrease power and performance [1]. Because of possible performance deficits associated with static stretching, alternative methods for increasing ROM have been investigated.
The relative tightness of the soft tissue structures in the body, joint capsules, muscles and their fascia can affect flexibility [3]. Found surrounding the muscle, myofascia is a connective tissue that can restrict ROM and decrease strength and endurance if injured, inactive, or inflamed [4]. Clinicians use manual pressure over the tissue to effect therapeutic change in this tissue using a variety of techniques including osteopathic soft-tissue manipulations, structural integration, various forms of massage, muscle energy techniques, and Graston [5]. Alternatively, a technique to treat fascia independent of a practitioner, self-induced myofascial release (SMR), can be facilitated with a foam roller or roller massager. Foam rollers are cylinders made of varying densities and textures of foam and roller massagers are plastic rollers held in the hands. These tools utilize the same mechanism of treatment as traditional myofascial release, but pressure is applied by the individual externally or using body weight.
Research surrounding SMR is new and forth coming. Studies have investigated the effects of SMR on athletic performance and, to date, the majority of research shows no effect on performance measures, though it does not seem to decrease performance [6-9]. SMR has also been shown to reduce the pain associated with delayed onset muscle soreness [10-12] and possibly decrease arteriole stiffness [13]. SMR is highly regarded in the rehabilitation and strength and conditioning fields to aid recovery and increase joint ROM, sparking an area of recent research. Of four published studies, three have found chronic SMR to increase range of motion measures [14-16]. However, if used as a replacement for static stretching in a warm-up or treatment in a therapy session, the acute effects of SMR on ROM are also important.
Studies have found that SMR, utilizing various tools, times, and techniques, increases acute ROM [4, 6, 8, 12, 17]. Current literature supporting SMR’s ability to increase acute ROM utilized a roller massager as the tool of choice [4, 6, 8, 12] with the exception of MacDonald et al. [18], who utilized a homemade roller from PVC pipe and 1cm foam. These studies saw ROM increases ranging from 4.3% [4] to 16% [17]. Additionally, it is noteworthy that Sullivan [4] and Bradbury-Squires [17] employed the use of a specially designed constant pressure roller apparatus to apply the external force to the muscle.
Although SMR has been shown effective with a roller massager, there is currently no research investigating the effect of foam roller application on a specific joint ROM. Current research utilizing a foam roller treated multiple muscle groups and investigated ROM changes with a sit and reach assessment. Roylance [19] had subjects independently roll using body weight and a traditional foam roller on the low back, upper back, buttocks, posterior thigh, and calf for two minutes on each area and saw no increase in sit and reach. Similarly, Peacock [20] used a whole body rolling protocol at five strokes over 30s for each muscle group and saw no increase in sit and reach.
Duration of roller application has varied as well. It is recommended that myofascial release occur for 60-90s up to five minutes, or until a release is felt [21] and the cumulative time of all studies fall within this range. Halperin et al. [6] utilized a roller massager for three repetitions of 30s and 10s rest in between and saw a 4% increase in ankle ROM. Macdonald et al. [18] used a PVC pipe covered in foam on the quadriceps and tested two one minute sessions with one minute rest and saw a 12.7% increase in quadriceps ROM 2 min post rolling. Sullivan et al. [4] used four different timed bouts of rolling with a roller massager on the hamstring. They investigated 1 set for 5s, 1 set for 10s, 2 sets for 5s, and 2 sets for 10s. Rolling increased ROM from pre to post-test 4.3% and there was an increase of 2.3% between 10s and 5s. While the above studies showed increases in ROM with as little as 5s of roller application, Mikesky [8] had athletes self-administer a roller massager to their hamstring for 2 min and saw no increase in ROM.
Currently, there is discrepancy and lack of evidence-based practice concerning the optimal duration of rolling and the type of roller that can be used for the most beneficial outcomes. Commercial foam rollers are sold for home use, and suggested for use as a means of enhancing flexibility, yet available studies utilize roller massagers or solid rollers and data therefore may not be applicable to the home-based population. Therefore, the purpose of this study was to investigate the effect of varied durations of foam rolling treatment on range of motion of the hamstring using a commercial foam roller commonly seen in gyms, therapy clinics and homes.
MATERIALS AND METHODOLOGY
Reliability Testing
The present study involved repeated measures of range of motion (ROM) at the knee following foam rolling. Reliability of investigators was established prior to subject sampling. Ten subjects outside the sample pool, (seven male and 3 female, age= 20± 1.3y, mass=160.7± 30.0kg), were recruited from a University population to establish Intra and Inter-tester reliability. Subjects were free from lower limb injury in the past 12 months and had a knee extension angle less than 85 degrees. Subjects provided signed consent in accordance with the University Institutional Review Board, who approved the study. Each subject was measured three times by three individuals, two investigators and a certified athletic trainer, using the ROM protocol described below. The certified athletic trainer functioned as a gold standard measure. The inter-tester ICC (3,2) was 0.947, while intra-tester ICC (1,2) values were 0.951, 0.955, and 0.921 for each of the testers. Sullivan et al. [4] investigated the effect of foam rolling duration on ROM and demonstrated an effect size of 0.65. They showed significant main effect for time (men and women combined) with an increase in ROM from pre (31.32 ± 2.10 cm) to post rolling (32.68 ± 2.06 cm) of 4.3%. Based on a power of 0.80, significance of p=0.05, and effect size (Cohen’s d) of 0.65, a sample size of 34 was calculated to be necessary to reject the null hypothesis.
Subjects
For the present study 33 subjects (19 female, 14 male, age= 20±1.5 y, mass= 72.2±10.8 kg) were recruited from a university population. Subjects were healthy, recreationally active, and voluntarily consented to testing procedures and provided written consent. Subjects had not experienced any lower leg injury or surgical procedures in the previous 12 months. While enrolled in the study subjects were asked to maintain their usual workout routine, but to refrain from exercising 12 hours prior to testing and not to perform foam rolling 48 hours before testing. Previous rolling experience was not an exclusionary or inclusionary criterion, but as stated previously any current rolling practice was suspended for 48 hours prior to participation. Additionally, correct rolling form was taught to all participants during a familiarization session on the first day of testing. Testing sessions were separated by a minimum of 48 hours and a maximum of 120 hours in order to avoid any effect of a prior treatment session. Testing occurred between the hours of 1 and 4pm, and subjects were scheduled at the same time for all three testing days.
Procedures
On orientation day subjects arrived and completed a health history questionnaire and informed consent. After a five minute warm-up on a cycle at 74 Watts (1.5kg, 50rpm Monark cycle), baseline hamstring range of motion (ROM) was measured, and subjects were instructed on the foam rolling technique and provided time to practice the rolling pace. The baseline ROM measures were used as the control, or pre-treatment values. Day two and three of testing involved a five minute cycle warm-up, the assigned rolling duration, and measurement of hamstring ROM. There was a 2-4 minute transition time between the completion of rolling and commencement of ROM measurements.
The rolling durations tested were four sets of 30s (“Long”), each separated by 30s of rest and two sets of ten seconds (“Short”), each separated by 30s of rest. The test days were counterbalanced between subjects. The roller used was a 6”x12” EPE Black High Density Foam Roller, 1.9 lbs per cubic foot density.
Foam Rolling Technique
Subjects were read a standardized foam rolling procedure based on accepted rolling technique [22] and an investigator also demonstrated. The procedures required the subject to roll the right leg from the ischial tuberosity to the back of the knee. The hands were set on the floor and did not move during the rolling motion. The body shifted back and forth to a metronome cadence, with the left leg acting as a stabilizer (Figs. 1, 2). Subjects were instructed to keep maximum weight over the right leg. Pilot testing established a rolling cadence of 40 bpm. Rolling from ischial tuberosity to knee was considered one beat.
Fig. (1).

Foam roller placement under knee.
Fig. (2).

Foam roller placement under hip.
Range of Motion Measures
Hamstring ROM was measured using a passive knee extension test, as described by Berryman Reece and Bandy [23], on a board specially designed to maintain 90° hip flexion. The subject laid supine on the table with the right hip flexed to 90°; if needed a bolster was added behind the knee. The left leg was extended flat on the table with the knee fully extended (Fig. 3). The angle of the hip was confirmed at 90° with a goniometer. The length from the fibular head to the bottom edge of the lateral malleolus was measured and a mark was made at 60.6% of this length. This point was the placement position of the manual muscle tester (MMT, Lafayette Instrument, Lafayette, IN). Weight of the leg was measured using the MMT with the knee bent at 90° and the leg relaxed. An inclinometer (The Sauders Group Inc. Chaska, MN) was strapped to the middle of the right tibia while the knee was passively extended using a standardized force.
Fig. (3).

Subject set up for knee extension ROM measurement.
In order, to account for passive lower leg weight and gravity [24], a 7kg force was applied to determine an initial knee extension angle (Fig. 4). Using the equation F = (cos α)W, where F was force, α was degrees of initial knee extension above horizontal, and W the passive lower leg weight, which was measured at the horizontal using the MMT, the amount of force to be applied was calculated. (F) in addition to the 7kg (F+7kg) was the force applied to the leg during ROM measurement trials.
Fig. (4).

Knee extension measurement.
The knee was passively extended to a second time using the new force (7kg + F) and held at this point for 20-30s to activate the golgi tendon and reduce ROM measurement error. Using the same force, the leg was extended 3 times and angles were recorded. The mean of 3 measures was used as the final knee extension angle. Results were analyzed using a one-way repeated measures ANOVA. Significance was determined based on an alpha level of p<0.05.
Loading Relative to Body Weight
Previous studies investigating foam rolling reported the force applied to the body by the roller because it was a controlled factor in the study [4, 17]. In order to better compare the results of the studies, a subset of 7 subjects were placed on a digital scale (SECA, Chino, CA) and the weight was recorded at three points in the rolling sequence, knee, mid-thigh, and hip. Recorded values from the scale in the three positions and the previously obtained body weight were used to approximate the percent of body weight applied by the roller.
RESULTS
The mean ± SD for baseline knee extension was 67.70 ± 9.90 degrees, short duration was 67.30 ± 10.60 degrees, and long duration was 67.41 ± 10.81 degrees. There were no significant differences (p=0.986) across conditions (Fig. 5). ANOVA comparisons were also run between genders by treatment and did not show any significant differences. Therefore genders were combined for the overall analysis.
Fig. (5).
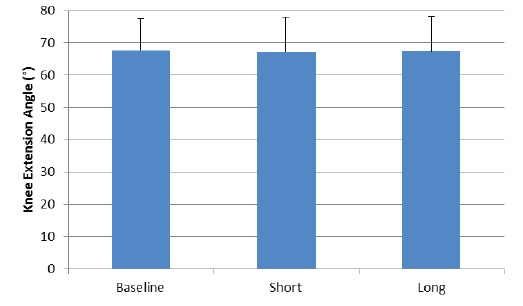
Mean and SD of knee extension angles across the three conditions.
In order to determine the relative loading on the hamstring by the foam roller, a subset of 7 subjects performed foam rolling with the roller placed on a digital scale. Percent of body weight applied varied across knee (25.44± 3.86%), mid-thigh (35.33 ± 5.59%) and hip (46.44± 4.7%). The data are shown in Fig. (6).
Fig. (6).
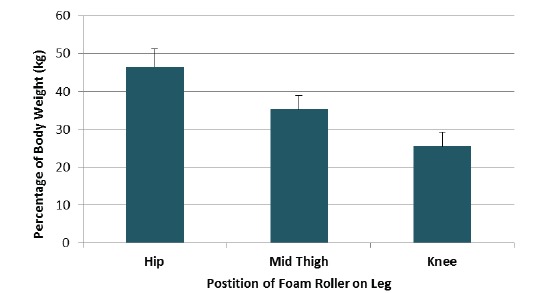
Force applied by the roller to the hamstring. This does not account for surface area of contact or density of the roller.
DISCUSSION
Commercial foam rollers are commonly used for both clinical and home therapy. Often self-administered using body weight as loading, little information is available as to the therapeutic effectiveness The results of the present study showed no significant differences between baseline knee extension ROM and the ROM present after foam rolling for either a short (2 sets of 10s) or long (4 sets of 30s) duration. While the rolling times used in this study were comparable to previous research showing an increase in ROM, we did not see similar increases. Differing results may be attributable to the type of roller and rolling method used, the ROM assessment methodology, or variations in rolling time and cadence.
The design of the foam roller may significantly influence treating the deep tissue and inducing a therapeutic effect. Curran [25] showed that a denser roller exerted more pressure per square inch than a less dense foam roller. Pressure is dependent on force exerted by the roller and area of contact with the roller. The rollers used in studies showing an increase in ROM were denser than the foam roller used in this study. Bradbury-Squires et al. [17], Halperin et al. [6], and Sullivan et al. [4] all utilized roller massagers made of a rigged thermoplastic and saw up to 16%, 4.4%, and 4.3% increases in ROM respectively. MacDonald et al. [18] employed a PVC pipe wrapped in a 1 cm thick layer of foam and saw up to a 12.7% increase in ROM. These rollers had higher densities and smaller diameters compared to the commercial roller used in the present study. These factors contribute to increasing the applied force and reducing the area of roller contact, therefore increasing the pressure applied directly to the tissue. Increased roller densities also limit deformation of the roller by body weight. This deformation occurs with conventional rollers, and decreases the pressure applied to the tissue. These findings support earlier conclusions that myofascial release should start superficially but needs to work into the deep tissue to have a therapeutic impact [26].
Additionally, it is noteworthy that Sullivan et al. [4] and Bradbury-Squires et al. [17] employed the use of a specially designed constant pressure roller apparatus to apply the external force on the tissue at roughly 20% and 25% body weight respectively. This method does allow for a controlled application of pressure, but does not reflect the actual dispersion of forces when an individual is independently using the roller, reflecting treatment conditions in a clinic or the home. In the present study, using a small subset of the subject pool (n=7) we found an average of 36% of body weight directed through the roller at the hip, with decreasing load as the roller moved distally (Fig. 4). Though there was a greater average percent body weight applied to the tissue in the present study, the increased diameter and decreased density of the commercial foam roller compared to a roller massager most likely negated impact of the higher load.
The present study also used a controlled procedure to standardize the force applied to the leg when measuring knee extension. This level of control may also explain some differences among the literature, as other published studies did not use this level of control. Sullivan et al. [4] rolled the hamstring and measured ROM changes using a sit and reach measure. Sit and reach is not specific for hamstring ROM, as it accounts for lumbar ROM as well. Studies have shown the sit-and-reach to have a low-to-moderate correlation coefficient of criterion-related validity for participants with limited hamstring flexibility and moderate-to-high for individuals with high hamstring flexibility [27]. Sit-and-reach values, though compared across the same subject, may not provide the best measure of hamstring extensibility as the measure relies on the movement of many other joints as well. Additionally, MacDonald et al. [18] and Bradbury-Squires et al. [17] measured passive knee flexion ROM changes using a kneeling lunge. The knee was flexed during each session until a point of discomfort and then an angle measure was collected. Using pain or discomfort as a termination point can induce error of measurement. Pearcey et al. [11] showed that subjects who performed foam rolling following delayed onset muscle soreness experienced reduced pain levels 24 and 48 hours after exercise. Similar findings were seen by Jay et al. [10], who induced soreness and 48 hours later had an examiner for applying a roller massager to the hamstrings for 10 minutes. The leg that received the roller massager had significantly lower levels of perceived soreness and higher pain pressure thresholds compared to the opposite, non-treated leg. Since rolling has been shown to increase pain pressure threshold, studies that have examined ROM with point of discomfort as an endpoint may therefore see improvements in ROM due to the increased torque applied as a result of reduced discomfort, and not a therapeutic effect to the muscle or fascia. ROM changes can occur due to decreases in muscle stiffness, seen as a decrease in a torque/angle curve, increase in muscle length, a right shift of a torque angle curve, or increase in applied torque [28]. The present study controlled for force applied to the limb, making end range of motion objective, rather than pain subjective, and saw no change in ROM. Weppler and Magnusson [28] highlighted the lack of support for mechanical mechanisms to increase muscle extensibility and advocated the sensory theory. The sensory theory states that changes in sensation, not physical alterations of the muscle, allow for a greater joint ROM after acute bouts of stretching. MacDonald et al. [18] saw a 12.7% increase in ROM 2 minutes after 2, 1 minute bouts of rolling and Bradbury-Squires et al. [17] saw a 16% increase after 5, 1 minute bouts of rolling. These two studies using discomfort as a stopping point for measurement saw greater increases than those that used sit and reach (4.3% (4) or measured immediately after rolling using an ankle dorsiflexion lunge (3.6% [6]). It is possible that SMR with a roller may produce small therapeutic effects in the fascia or muscle if enough force is applied as seen in the small ROM increases from Sullivan et al. [4] and Halperin et al. [6]. Though, using an assessment that allows possible changes in sensation caused by the treatment to be measured, as used by MacDonald et al. [18] and Bradbury-Squires et al. [17], may account for the greater ROM increase. The present study, using a less dense roller than the above cited studies, may not have exerted enough pressure to affect the soft tissue. Also, the knee extension test was not pain limited and therefore the measure was uninfluenced by any possible changes in pain pressure threshold that would have resulted in a greater ROM.
Rolling time and cadence are also a factor in the effectiveness of SMR treatments. These factors are confounded in current research due to the use of different rollers, on different muscles, with different SMR techniques and currently no conclusions can be drawn. This study, in finding no statistical differences between the tested times, showed a range of rolling times using a commercial foam roller was ineffective for increasing ROM. This presents an area for future research.
CONCLUSION
We conclude that there are no significant differences between baseline knee extension ROM and the ROM present after foam rolling for either a short (2 sets of 10s) or long (4 sets of 30s) duration in healthy, active, college-aged men and women. A major factor influencing the results was the pressure per unit area exerted by the roller onto the tissue, which is influenced by the roller density and diameter. Future studies should address the impact of time, cadence, pressure, and the ROM assessment methodology to identify whether foam rolling has a therapeutic impact on ROM.
ACKNOWLEDGEMENTS
Declared none.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
REFERENCES
- 1.Behm D.G., Chaouachi A. A review of the acute effects of static and dynamic stretching on performance. Eur. J. Appl. Physiol. 2011;111(11):2633–2651. doi: 10.1007/s00421-011-1879-2. [DOI] [PubMed] [Google Scholar]
- 2.Corbin C.B., Noble L. Flexibility: a major component of physical fitness. J Phys Educ Recreat. 1980;51(6):23–60. [Google Scholar]
- 3.Heyward V. Advanced Fitness Assessment and Exercise Prescription. 6th ed. IL, USA: Human Kinetics Publishers; 2010. Assessing Flexibility. p. 266. [Google Scholar]
- 4.Sullivan K.M., Silvey D.B., Button D.C., Behm D.G. Roller-massager application to the hamstrings increases sit-and-reach range of motion within five to ten seconds without performance impairments. Int. J. Sports Phys. Ther. 2013;8(3):228–236. [PMC free article] [PubMed] [Google Scholar]
- 5.Simmonds N., Miller P., Gemmell H. A theoretical framework for the role of fascia in manual therapy. J. Bodyw. Mov. Ther. 2012;16(1):83–93. doi: 10.1016/j.jbmt.2010.08.001. [DOI] [PubMed] [Google Scholar]
- 6.Halperin I., Aboodarda S.J., Button D.C., Andersen L.L., Behm D.G. Roller massager improves range of motion of plantar flexor muscles without subsequent decreases in force parameters. Int. J. Sports Phys. Ther. 2014;9(1):92–102. [PMC free article] [PubMed] [Google Scholar]
- 7.Healey K.C., Hatfield D.L., Blanpied P., Dorfman L.R., Riebe D. The effects of myofascial release with foam rolling on performance. J. Strength Cond. Res. 2014;28(1):61–68. doi: 10.1519/JSC.0b013e3182956569. [DOI] [PubMed] [Google Scholar]
- 8.Mikesky A.E., Bahamonde R.E., Stanton K., Alvey T., Fitton T. Acute effects of The Stick on strength, power, and flexibility. J. Strength Cond. Res. 2002;16(3):446–450. [PubMed] [Google Scholar]
- 9.Schroeder A.N., Best T.M. Is self myofascial release an effective preexercise and recovery strategy? A literature review. Curr. Sports Med. Rep. 2015;14(3):200–208. doi: 10.1249/JSR.0000000000000148. [DOI] [PubMed] [Google Scholar]
- 10.Jay K., Sundstrup E., Søndergaard S.D., Behm D., Brandt M., Særvoll C.A., Jakobsen M.D., Andersen L.L. Specific and cross over effects of massage for muscle soreness: randomized controlled trial. Int. J. Sports Phys. Ther. 2014;9(1):82–91. [PMC free article] [PubMed] [Google Scholar]
- 11.Pearcey G.E., Bradbury-Squires D.J., Kawamoto J.E., Drinkwater E.J., Behm D.G., Button D.C. Foam rolling for delayed-onset muscle soreness and recovery of dynamic performance measures. J. Athl. Train. 2015;50(1):5–13. doi: 10.4085/1062-6050-50.1.01. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Macdonald G.Z., Button D.C., Drinkwater E.J., Behm D.G. Foam rolling as a recovery tool after an intense bout of physical activity. Med. Sci. Sports Exerc. 2014;46(1):131–142. doi: 10.1249/MSS.0b013e3182a123db. [DOI] [PubMed] [Google Scholar]
- 13.Okamoto T., Masuhara M., Ikuta K. Acute effects of self-myofascial release using a foam roller on arterial function. J. Strength Cond. Res. 2014;28(1):69–73. doi: 10.1519/JSC.0b013e31829480f5. [DOI] [PubMed] [Google Scholar]
- 14.Ebrahim A., Abd Elghany A. The effect of foam roller exercise and Nanoparticle in speeding of healing of sport injuries. J Am Sci. 2013;9(6):450–458. [Google Scholar]
- 15.Mohr A.R., Long B.C., Goad C.L. Effect of foam rolling and static stretching on passive hip-flexion range of motion. J. Sport Rehabil. 2014;23(4):296–299. doi: 10.1123/jsr.2013-0025. [DOI] [PubMed] [Google Scholar]
- 16.Junker D., Stöggl T. The foam roll as a tool to improve hamstring flexibility. J. Strength Cond. Res. 2015 doi: 10.1519/JSC.0000000000001007. [Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- 17.Bradbury-Squires D.J., Noftall J.C., Sullivan K.M., Behm D.G., Power K.E., Button D.C. Roller-massager application to the quadriceps and knee-joint range of motion and neuromuscular efficiency during a lunge. J. Athl. Train. 2015;50(2):133–140. doi: 10.4085/1062-6050-49.5.03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.MacDonald G.Z., Penney M.D., Mullaley M.E., Cuconato A.L., Drake C.D., Behm D.G., Button D.C. An acute bout of self-myofascial release increases range of motion without a subsequent decrease in muscle activation or force. J. Strength Cond. Res. 2013;27(3):812–821. doi: 10.1519/JSC.0b013e31825c2bc1. [DOI] [PubMed] [Google Scholar]
- 19.Roylance D.S., George J.D., Hammer A.M., et al. Evaluating acute changes in joint range-of-motion using self-myofascial release, postural alignment exercises, and static stretches. Int. J. Exerc. Sci. 2013;6(4):310–319. [Google Scholar]
- 20.Peacock C.A., Krein D.D., Silver T.A., Sanders G.J., Von Carlowitz K.A. An acute bout of self-myofascial release in the form of foam rolling improves performance testing. Int. J. Exerc. Sci. 2014;7(3):202–211. doi: 10.70252/DTPM9041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Paolini J. Review of myofascial release as an effective massage therapy technique. Athl. Ther. Today. 2009;14(5):30–34. [Google Scholar]
- 22.Sports Medicine Institute A guide to the foam roller.
- 23.Reese N., Bandy W. Muscle length testing of the lower extremity. Joint range of motion and muscle length testing. 2nd ed. USA: Saunders Elselvier; 2014. pp. 390–391. [Google Scholar]
- 24.Guex K., Fourchet F., Loepelt H., Millet G.P. Passive knee-extension test to measure hamstring tightness: influence of gravity correction. J. Sport Rehabil. 2012;21(3):231–234. doi: 10.1123/jsr.21.3.231. [DOI] [PubMed] [Google Scholar]
- 25.Curran PF, Fiore RD, Crisco JJ. A comparison of the pressure exerted on soft tissue by 2 myofascial rollers. J Sport Rehabil. 2008;11; 17(4):432–42. doi: 10.1123/jsr.17.4.432. [DOI] [PubMed] [Google Scholar]
- 26.Comerford M.J., Mottram S.L. Functional stability re-training: principles and strategies for managing mechanical dysfunction. Man. Ther. 2001;6(1):3–14. doi: 10.1054/math.2000.0389. [DOI] [PubMed] [Google Scholar]
- 27.Mayorga-Vega D., Merino-Marban R., Viciana J. Criterion-related validity of sit-and-reach tests for estimating hamstring and lumbar extensibility: a meta-analysis. J. Sports Sci. Med. 2014;13(1):1–14. [PMC free article] [PubMed] [Google Scholar]
- 28.Weppler C.H., Magnusson S.P. Increasing muscle extensibility: a matter of increasing length or modifying sensation? Phys. Ther. 2010;90(3):438–449. doi: 10.2522/ptj.20090012. [DOI] [PubMed] [Google Scholar]