

Abstract
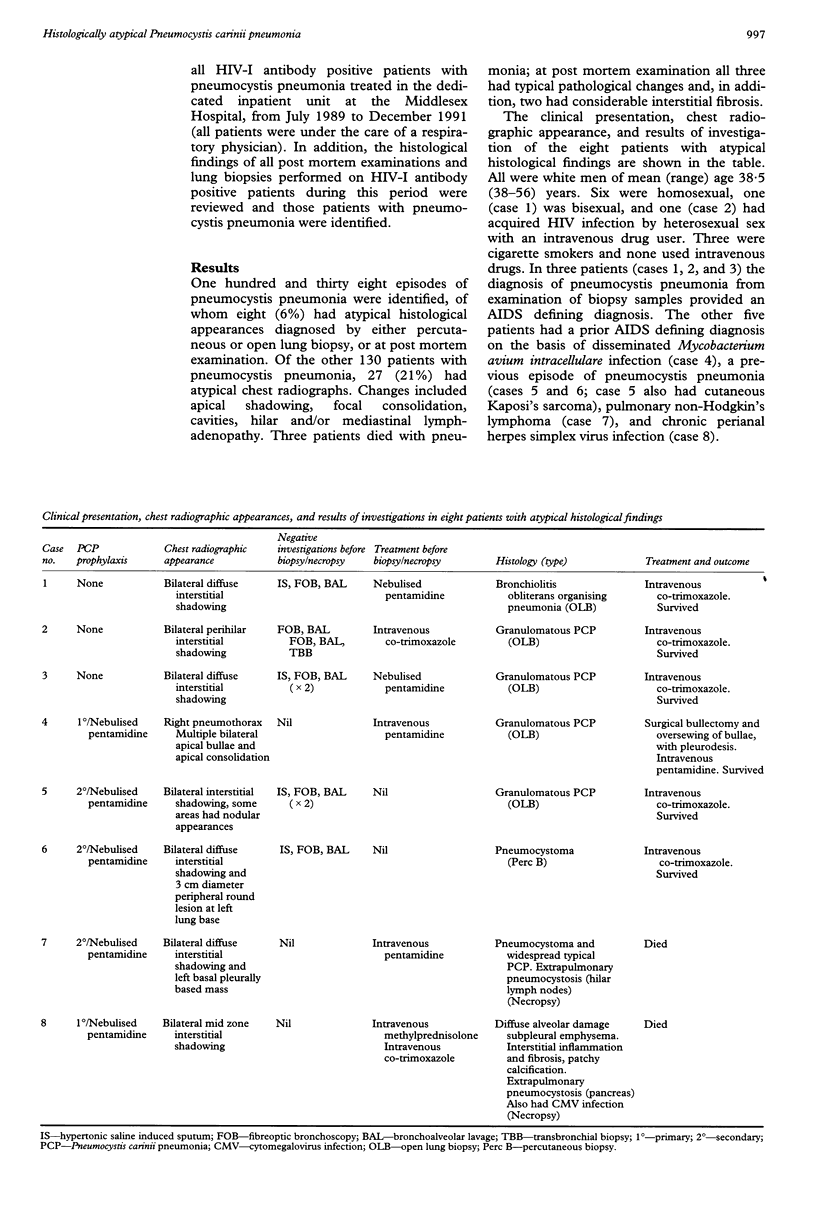
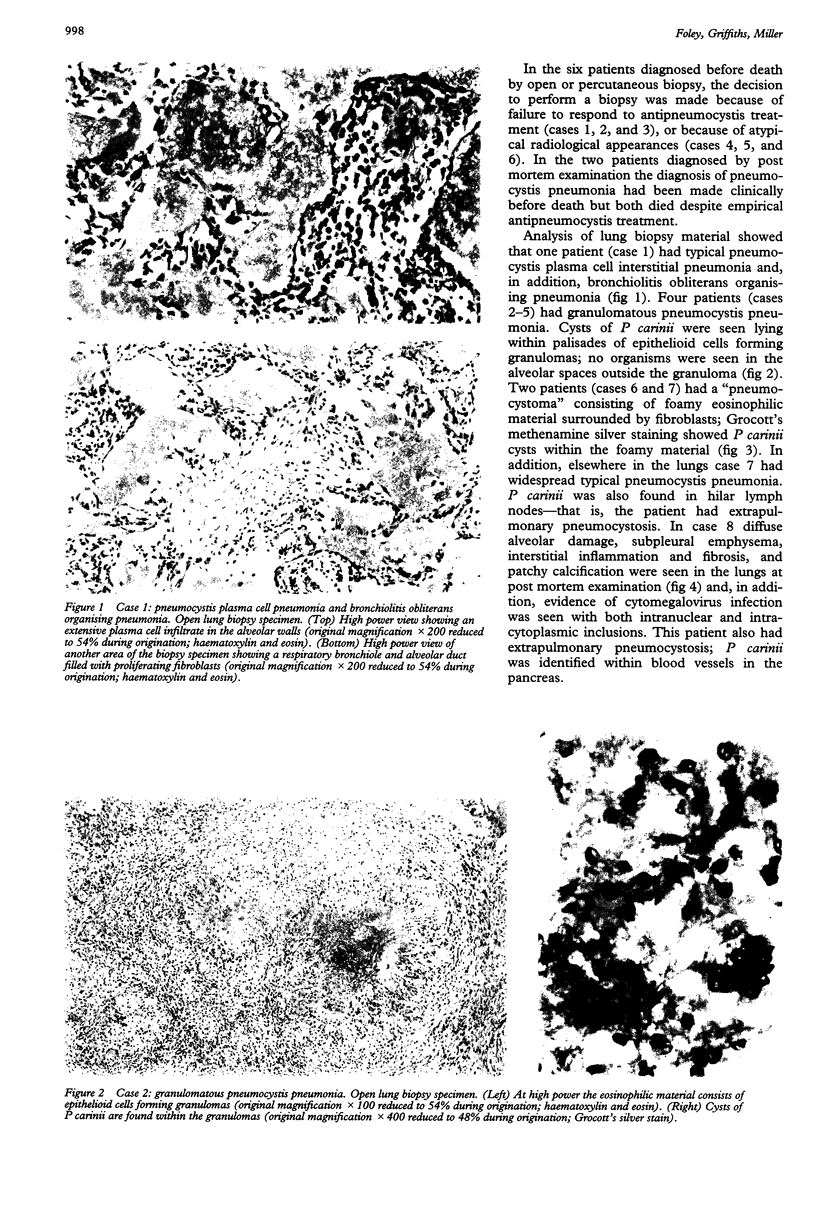
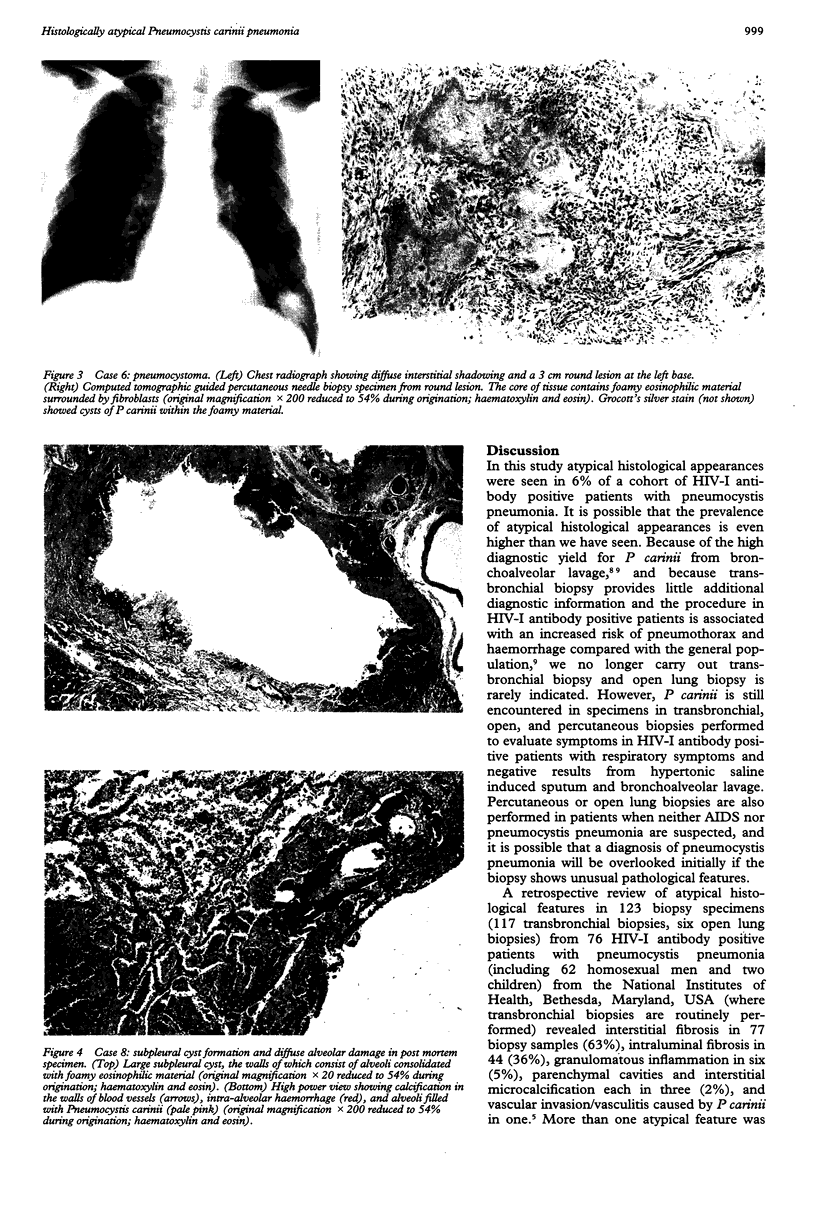
BACKGROUND--Infection with Pneumocystis carinii typically results in a pneumonia which histologically is seen to consist of an eosinophilic foamy alveolar exudate associated with a mild plasma cell interstitial infiltrate. Special stains show that cysts of P carinii lie within the alveolar exudate. Atypical histological appearances may occasionally be seen, including a granulomatous pneumonia and diffuse alveolar damage. In these patients the clinical presentation may be atypical and results of investigations negative unless lung biopsies are performed and tissue obtained for histological examination. METHODS--The incidence and mode of presentation of histologically atypical pneumocystis pneumonia was studied in a cohort of HIV-I antibody positive patients. RESULTS--Over a 30 month period 138 patients had pneumocystis pneumonia, of whom eight (6%) had atypical histological appearances which were diagnosed (after negative bronchoalveolar lavage) by open lung biopsy in five, percutaneous biopsy in one, and at post mortem examination in two. Atypical appearances included granulomatous inflammation in four patients, "pneumocystoma" in two (one also had extrapulmonary pneumocystosis), bronchiolitis obliterans organising pneumonia in one patient, diffuse alveolar damage and subpleural cysts in one (who also had intrapulmonary cytomegalovirus infection), and extrapulmonary pneumocystosis in two patients. CONCLUSIONS--Various atypical histological appearances may be seen in pneumocystis pneumonia. Lung biopsy (either percutaneous or open) should be considered when bronchoalveolar lavage is repeatedly negative and evidence of P carinii should be sought, by use of special stains, in all lung biopsy material from HIV-I antibody positive patients.
Full text
PDF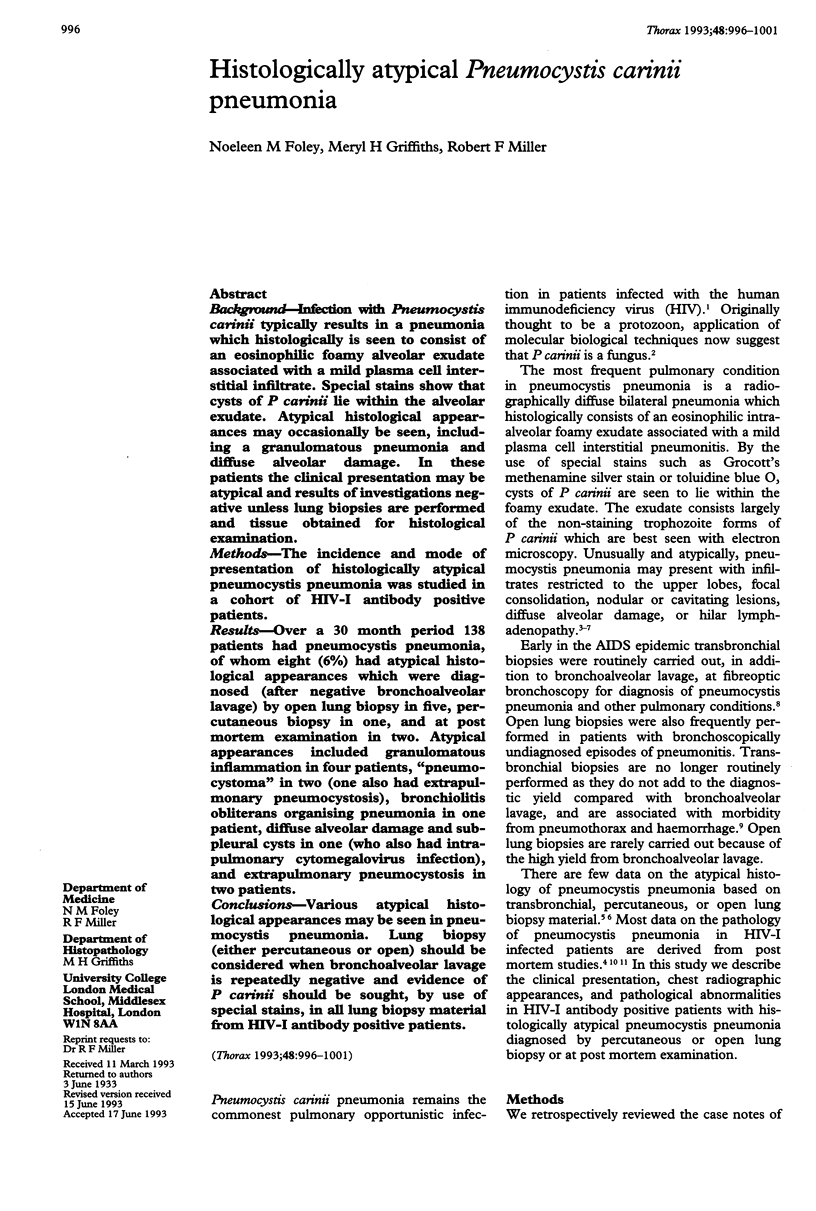

Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Askin F. B., Katzenstein A. L. Pneumocystis infection masquerading as diffuse alveolar damage: a potential source of diagnostic error. Chest. 1981 Apr;79(4):420–422. doi: 10.1378/chest.79.4.420. [DOI] [PubMed] [Google Scholar]
- Barrio J. L., Suarez M., Rodriguez J. L., Saldana M. J., Pitchenik A. E. Pneumocystis carinii pneumonia presenting as cavitating and noncavitating solitary pulmonary nodules in patients with the acquired immunodeficiency syndrome. Am Rev Respir Dis. 1986 Nov;134(5):1094–1096. doi: 10.1164/arrd.1986.134.5.1094. [DOI] [PubMed] [Google Scholar]
- Birley H. D., Buscombe J. R., Griffiths M. H., Semple S. J., Miller R. F. Granulomatous Pneumocystis carinii pneumonia in a patient with the acquired immunodeficiency syndrome. Thorax. 1990 Oct;45(10):769–771. doi: 10.1136/thx.45.10.769. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blumenfeld W., Basgoz N., Owen W. F., Jr, Schmidt D. M. Granulomatous pulmonary lesions in patients with the acquired immunodeficiency syndrome (AIDS) and Pneumocystis carinii infection. Ann Intern Med. 1988 Sep 15;109(6):505–507. doi: 10.7326/0003-4819-109-6-505. [DOI] [PubMed] [Google Scholar]
- Coker R. J., Clark D., Claydon E. L., Gompels M., Ainsworth J. G., Lucas S. B., Miller R., Goldin R. D., Pinching A. J., Harris J. R. Disseminated pneumocystis carinii infection in AIDS. J Clin Pathol. 1991 Oct;44(10):820–823. doi: 10.1136/jcp.44.10.820. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eng R. H., Bishburg E., Smith S. M. Evidence for destruction of lung tissues during Pneumocystis carinii infection. Arch Intern Med. 1987 Apr;147(4):746–749. [PubMed] [Google Scholar]
- Feurestein I. M., Archer A., Pluda J. M., Francis P. S., Falloon J., Masur H., Pass H. I., Travis W. D. Thin-walled cavities, cysts, and pneumothorax in Pneumocystis carinii pneumonia: further observations with histopathologic correlation. Radiology. 1990 Mar;174(3 Pt 1):697–702. doi: 10.1148/radiology.174.3.2305052. [DOI] [PubMed] [Google Scholar]
- Griffiths M. H., Kocjan G., Miller R. F., Godfrey-Faussett P. Diagnosis of pulmonary disease in human immunodeficiency virus infection: role of transbronchial biopsy and bronchoalveolar lavage. Thorax. 1989 Jul;44(7):554–558. doi: 10.1136/thx.44.7.554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hartz J. W., Geisinger K. R., Scharyj M., Muss H. B. Granulomatous pneumocystosis presenting as a solitary pulmonary nodule. Arch Pathol Lab Med. 1985 May;109(5):466–469. [PubMed] [Google Scholar]
- Hughes-Davies L., Kocjan G., Spittle M. F., Miller R. F. Occult alveolar haemorrhage in bronchopulmonary Kaposi's sarcoma. J Clin Pathol. 1992 Jun;45(6):536–537. doi: 10.1136/jcp.45.6.536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klein J. S., Warnock M., Webb W. R., Gamsu G. Cavitating and noncavitating granulomas in AIDS patients with Pneumocystis pneumonitis. AJR Am J Roentgenol. 1989 Apr;152(4):753–754. doi: 10.2214/ajr.152.4.753. [DOI] [PubMed] [Google Scholar]
- Kuhlman J. E., Kavuru M., Fishman E. K., Siegelman S. S. Pneumocystis carinii pneumonia: spectrum of parenchymal CT findings. Radiology. 1990 Jun;175(3):711–714. doi: 10.1148/radiology.175.3.2343118. [DOI] [PubMed] [Google Scholar]
- Liu Y. C., Tomashefski J. F., Jr, Tomford J. W., Green H. Necrotizing Pneumocystis carinii vasculitis associated with lung necrosis and cavitation in a patient with acquired immunodeficiency syndrome. Arch Pathol Lab Med. 1989 May;113(5):494–497. [PubMed] [Google Scholar]
- McGowan I., Potter M., George R. J., Michaels L., Sinclair E., Scaravilli F., Miller R. F. HIV encephalopathy presenting as hypomania. Genitourin Med. 1991 Oct;67(5):420–424. doi: 10.1136/sti.67.5.420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller R. F., Mitchell D. M. AIDS and the lung: update 1992. 1. Pneumocystis carinii pneumonia. Thorax. 1992 Apr;47(4):305–314. doi: 10.1136/thx.47.4.305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moskovic E., Miller R., Pearson M. High resolution computed tomography of Pneumocystis carinii pneumonia in AIDS. Clin Radiol. 1990 Oct;42(4):239–243. doi: 10.1016/s0009-9260(05)82110-5. [DOI] [PubMed] [Google Scholar]
- Murry C. E., Schmidt R. A. Tissue invasion by Pneumocystis carinii: a possible cause of cavitary pneumonia and pneumothorax. Hum Pathol. 1992 Dec;23(12):1380–1387. doi: 10.1016/0046-8177(92)90058-b. [DOI] [PubMed] [Google Scholar]
- Pitkin A. D., Grant A. D., Foley N. M., Miller R. F. Changing patterns of respiratory disease in HIV positive patients in a referral centre in the United Kingdom between 1986-7 and 1990-1. Thorax. 1993 Mar;48(3):204–207. doi: 10.1136/thx.48.3.204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sandhu J. S., Goodman P. C. Pulmonary cysts associated with Pneumocystis carinii pneumonia in patients with AIDS. Radiology. 1989 Oct;173(1):33–35. doi: 10.1148/radiology.173.1.2789413. [DOI] [PubMed] [Google Scholar]
- Stover D. E., White D. A., Romano P. A., Gellene R. A. Diagnosis of pulmonary disease in acquired immune deficiency syndrome (AIDS). Role of bronchoscopy and bronchoalveolar lavage. Am Rev Respir Dis. 1984 Oct;130(4):659–662. doi: 10.1164/arrd.1984.130.4.659. [DOI] [PubMed] [Google Scholar]
- Travis W. D., Pittaluga S., Lipschik G. Y., Ognibene F. P., Suffredini A. F., Masur H., Feuerstein I., Kovacs J., Pass H. I., Condron K. S. Atypical pathologic manifestations of Pneumocystis carinii pneumonia in the acquired immune deficiency syndrome. Review of 123 lung biopsies from 76 patients with emphasis on cysts, vascular invasion, vasculitis, and granulomas. Am J Surg Pathol. 1990 Jul;14(7):615–625. doi: 10.1097/00000478-199007000-00002. [DOI] [PubMed] [Google Scholar]
- Yoneda K., Walzer P. D. Mechanism of pulmonary alveolar injury in experimental Pneumocystis carinii pneumonia in the rat. Br J Exp Pathol. 1981 Aug;62(4):339–346. [PMC free article] [PubMed] [Google Scholar]
- deRuiter A., Webb A., Mindel A., Scaravilli F., Michaels L., Miller R. F. Intensive care for advanced HIV disease. Genitourin Med. 1992 Jun;68(3):154–158. doi: 10.1136/sti.68.3.154. [DOI] [PMC free article] [PubMed] [Google Scholar]